Article Text

Abstract
Background A challenge for sports physicians is to estimate the risk of a hamstring re-injury, but the current evidence for MRI variables as a risk factor is unknown.
Objective To systematically review the literature on the prognostic value of MRI findings at index injury and/or return to play for acute hamstring re-injuries.
Data sources Databases of PubMed, Embase, MEDLINE, Scopus, CINAHL, Google Scholar, Web of Science, LILACS, SciELO, ScienceDirect, ProQuest, SPORTDiscus and Cochrane Library were searched until 20 June 2016.
Study eligibility criteria Studies evaluating MRI as a prognostic tool for determining the risk of re-injury for athletes with acute hamstring injuries were eligible for inclusion.
Data analysis Two authors independently screened the search results and assessed risk of bias using standardised criteria from a consensus statement. A best-evidence synthesis was used to identify the level of evidence. Post hoc analysis included correction for insufficient sample size.
Results Of the 11 studies included, 7 had a low and 4 had a high risk of bias. No strong evidence for any MRI finding as a risk factor for hamstring re-injury was found. There was moderate evidence that intratendinous injuries were associated with increased re-injury risk. Post hoc analysis showed moderate evidence that injury to the biceps femoris was a moderate to strong risk factor for re-injury.
Conclusion There is currently no strong evidence for any MRI finding in predicting hamstring re-injury risk. Intratendinous injuries and biceps femoris injuries showed moderate evidence for association with a higher re-injury risk.
Systematic review registration Registration in the PROSPERO International prospective register of systematic reviews was performed prior to study initiation (registration number CRD42015024620).
- Hamstring
- Recurrent
- MRI
- Risk factor
- Thigh
Statistics from Altmetric.com
Background
Hamstring injuries are a prevalent injury in sports with high-speed running or activities requiring substantial hamstring lengthening. These injuries are associated with significant time loss from sports and high re-injury rates, despite efforts in the prevention and management of these injuries.1–3 But what could be the meaning of specific MRI findings for these injuries?
In our previous systematic review,4 we evaluated the value of MRI for prognosis on the time to return to play (RTP), which is frequently used as the primary outcome following hamstring injury. No strong evidence for any MRI finding was reported. Nevertheless, moderate evidence was found that injuries without hyperintensity on fluid sensitive sequences are associated with a shorter time to RTP and that injuries involving the proximal free tendon are associated with a longer time to RTP.
Another clinically relevant outcome for muscle injuries is the re-injury rate. Predicting re-injury remains a clinical challenge and given the extended time loss after a re-injury, it is important to identify risk factors. Possibly MRI is a suitable tool to predict a hamstring re-injury after RTP.
Three previous systematic reviews on this topic,5–7 dating from 2011 to 2012, showed three MRI variables as risk factors for hamstring re-injury: larger volume size of the initial trauma,5 7 a grade 1 hamstring injury at initial trauma compared with grade 0 and grade 2 injuries (classification according to Peetrons)5 and greater length of the initial injury, seen as oedema (>6 cm long) on MRI.6 Conflicting evidence is present for cross-sectional area (CSA) as a risk factor.5 7
Since then new data on the prognosis of hamstring injuries have been published. The publication of new studies warranted an analysis whether MRI findings at baseline (=time of index injury) or at RTP, are associated with hamstring re-injury. The purpose of this study was to systematically review the literature on the value of MRI findings at baseline and/or RTP for predicting acute hamstring re-injuries.
Methods
Registration in the PROSPERO international prospective register of systematic reviews was performed prior to study initiation (registration number CRD42015024620).
Literature search
The following databases were searched for relevant reports of individual studies: PubMed, Embase, MEDLINE (Ovid), Scopus, CINAHL, Google Scholar, Web of Science, LILACS, SciELO, ScienceDirect, ProQuest, SPORTDiscus and Cochrane Library. Databases (regular and grey literature) were searched without time restrictions until 20 June 2016. Our sensitive search strategy was assisted by a biomedical information specialist (WM Bramer) and contained both controlled vocabulary and free-text terms (table 1).
Search strategy
Coauthors of our research group, with a specific interest in hamstring injuries, were asked about internationally known recently completed and/or submitted diagnostic trials up to 20 June 2016.
Study selection
Studies evaluating MRI performed at baseline and/or RTP as a prognostic tool for determining the risk of hamstring re-injury in athletes with acute hamstring injuries as an outcome measure, were eligible for inclusion if they met the following criteria:
Subjects with a clinical diagnosis of an acute hamstring injury.
MRI examination performed within 7 days of the acute injury and/or follow-up MRI within 7 days of RTP.
MRI findings as a prognostic tool for hamstring re-injury were studied.
The primary outcome was hamstring re-injury.
The study had to be an original published report.
Full text of the article had to be available.
The article was written in English, Dutch or German language.
All studies identified by our search strategy were imported into a citation database (Endnote 7.1, Thomson Reuters, New York, USA) and duplicates were removed. All titles and abstracts were screened by two reviewers (GR and MHM). Full-text articles considered eligible by at least one researcher were obtained and assessed independently, by the same two reviewers (GR and MM), using the inclusion criteria. When the assessors did not agree on inclusion of a study, a meeting was scheduled to seek consensus. When no consensus was met, a third reviewer (MvH) made the final decision on inclusion of the study.
Data extraction
One reviewer (MvH) extracted the data of all included studies using a standardised data extraction form to ensure a uniform data collection. From studies, written by the same (co-)author and using the same data set, we included only the data of the most recent study.
The following data were extracted: general study information, study population, study characteristics, details of the MRI (magnetic field strength, coil, sequences, time to repetition, time to echo, time to inversion, echo train length, flip angle, thickness sections/gap, field of view and matrix), MRI findings and outcome of the analysis of association between MRI findings and hamstring re-injury. Primary investigators of the reports included were contacted when information on data to be extracted was missing.
Risk of bias assessment
Two reviewers (R-JdV and JLT) independently assessed the potential risk of bias of the studies included, using the criteria of the consensus statement of Hayden et al.4 8 This risk of bias assessment tool assessed six potential bias domains, each consisting of specific items for opportunity of bias (see online supplement 1). If there was a difference in opinion on an item, a consensus was reached by the two reviewers. If no consensus was reached, the independent opinion of a third reviewer (MvH) was decisive.
Supplementary file
When at least one of the primary risk of bias assessors was involved as a coauthor, an independent experienced assessor (JO) evaluated the concerning article as third assessor to exclude bias as a result of detailed knowledge of these published studies by the authors. If there was a difference in outcome of the overall risk of bias categorisation (low risk or high risk of bias), a consensus was reached by the three assessors. If no consensus was reached, the independent opinion of the third assessor was decisive.
As shown on the risk of bias form each of the six potential bias domains consisted of two to five specific items. When ≥75% of these items within a domain were fulfilled, we considered the bias low in that domain. To have overall low risk of bias, a study should have low bias on at least five out of the six domains.
Data synthesis
We considered pooling data when studies were sufficiently statistically and clinically homogeneous. The process by which we planned to perform data pooling (calculating relative risks and performing a sensitivity analysis) is described in detail in the protocol registered (PROSPERO, registration number CRD42015024620). If data could not be pooled because of clinical and methodological heterogeneity, a qualitative analysis of the data was carried out using the five levels of evidence according to van Tulder et al.9
Strong evidence: provided by two or more studies with low risk of bias and by generally consistent findings in all studies (≥75% of the studies reported consistent findings).
Moderate evidence: provided by one study with low risk of bias and/or two or more studies with high risk of bias and by generally consistent findings in all studies (≥75% of the studies reported consistent findings).
Limited evidence: provided by only one study with high risk of bias.
Conflicting evidence: inconsistent findings in multiple studies (<75% of the studies reported consistent findings).
No evidence: when no studies could be found.
Results
Literature search
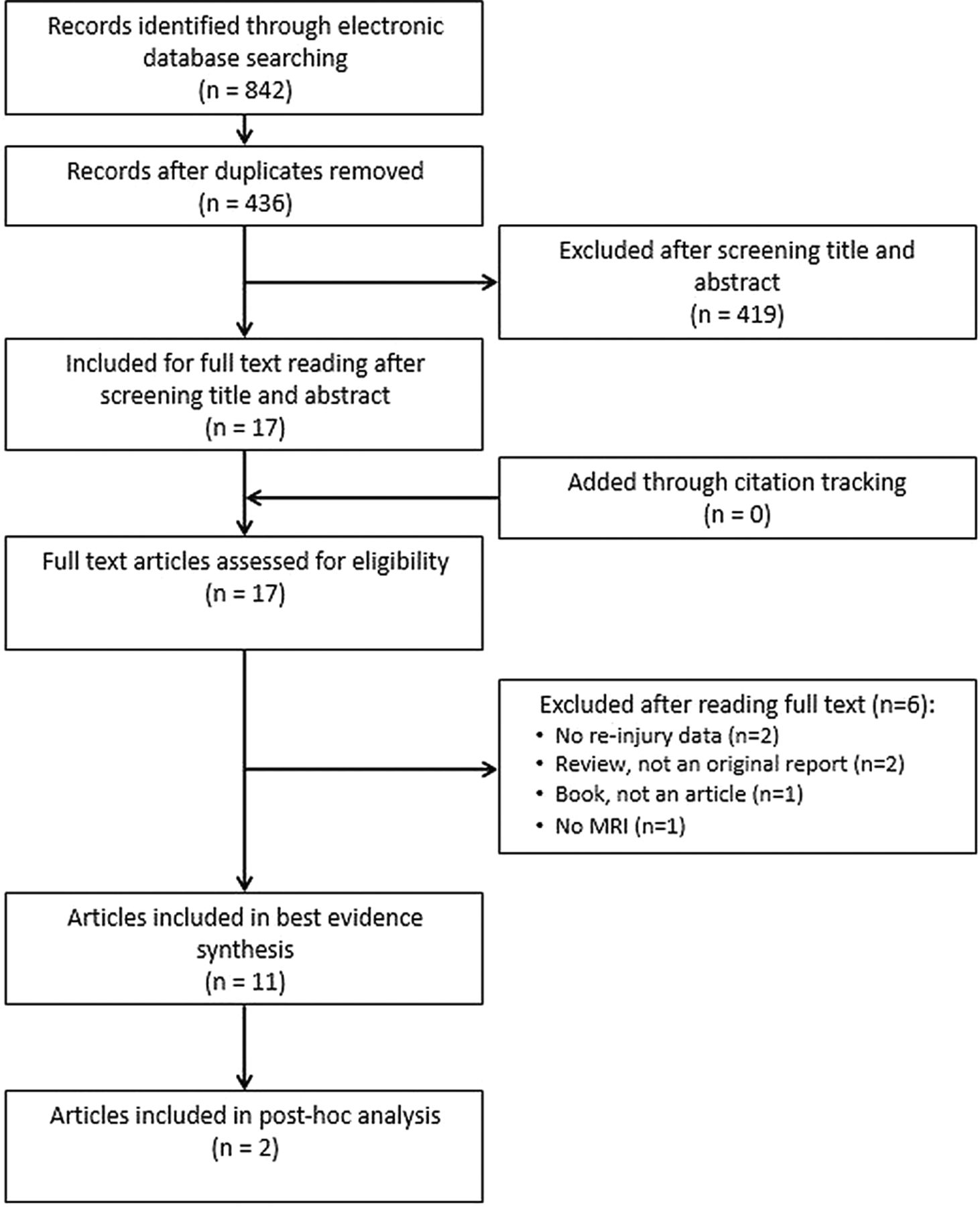
The initial search yielded 842 records. Eleven studies met the inclusion criteria and were included in this review10–20 (figure 1).
{kind=link}
Study selection flow diagram.
Description of included studies
Table 2 presents some of the characteristics of the included studies.10–20 An extended version of the characteristics is included in the appendix (see online supplement 2). A supplementary appendix provides an overview of the MRI protocols used in the included studies (see online supplement 3).
Supplementary file
Supplementary file
Table 2 Characteristics of included studies
Risk of bias assessment
Table 3 shows the scores on the potential risk of bias domains of the included studies. Seven studies had a low risk of bias11–15 17 20 and four studies had a high risk of bias.10 16 18 19 High risk of bias was frequently related to lack of adequate description or adjustment of the outcome of measurements, inappropriate adjustment for confounders and inappropriate statistical analysis.
Risk of bias assessment
For the specific items for opportunity of bias there was disagreement in 22 out of the 242 assessed items (9%), for which consensus was reached by the two reviewers in two consensus meetings. A third reviewer (JO) assessed the three articles where at least one of the primary risk of bias assessors was involved as coauthor. For one article16 there was a difference in outcome of the overall risk of bias categorisation with the third independent assessor. Finally, consensus was reached by the three assessors on the risk of bias categorisation for this article.
Determinants related to re-injury
Owing to clinical and methodological heterogeneity (varying definitions of re-injury, length of follow-up and methodological quality), it was not possible to perform pooling of the data.21 A qualitative analysis of the data was carried out using the best evidence synthesis methodology.
Table 4 presents an overview of all the reported MRI findings, their association with re-injury and the corresponding level of evidence according to the best-evidence synthesis.
Overview of the studied MRI findings at baseline and at RTP. The risk of bias, the association with re-injury and the corresponding level of evidence are presented for each MRI finding according to the best-evidence synthesis and the corresponding level of evidence
Baseline MRI
Strong evidence
No strong evidence for any MRI finding as risk factor for hamstring re-injury was found.
Strong evidence for the absence of association with hamstring re-injury was found for five determinants.
Two studies with low risk of bias found that there was no association between grading (grade 0–III, according to Peetrons) and hamstring re-injury.11 20
The specific hamstring muscle involved (biceps femoris, semimembranosus or semitendinosus), identified on MRI, showed strong evidence for no association with hamstring re-injury. Ekstrand et al 11–13 found a positive association for the biceps femoris versus the semimembranosus and the semitendinosus, but four other studies, of which three studies with low risk of bias, found no significant association for this determinant.14 15 19 20
There is also strong evidence for no relationship of injury location on MRI with hamstring re-injury, as two studies with low risk of bias reported no association with injury location.14 15 Koulouris et al 14 compared athletes that sustained a re-injury with athletes that did not have a re-injury during the same competition period. There was no statistically significant difference in the number of lesions located at the musculotendinous junction, myofascial, mixed, tendon-bone and proximal tendon between these groups. Pollock et al 15 categorised the injury location as proximal, central and distal injuries and they did not find an association between this classification and re-injury.
Four studies, of which two studies were with low risk of bias, found that an increased length of the hyperintensity signal was not associated with higher re-injury risk, so there is strong evidence for no relationship with hamstring re-injury.10 14 18 20
The CSA of the hyperintensity signal was not associated with hamstring re-injury. Only a study with high risk of bias by Silder et al 18 found that the re-injured subjects had a significantly greater per cent area injured on initial MRI. However, three other studies (two with low risk of bias and one with high risk of bias) reported no difference.10 14 20
Moderate evidence
Two determinants with a positive association with hamstring re-injury were found in this systematic review. There is moderate evidence for intratendinous injuries identified on MRI and classification according to the British Muscle Injury Classification, both found by Pollock et al.15
Moderate evidence for no relationship with hamstring re-injury was found for distance of the lesion to the ischial tuberosity and hyperintensity signal volume of the lesion.19 20
Limited evidence
Limited evidence for no relationship with hamstring re-injury was found for the number of muscles involved and transverse size of the hyperintensity signal.17
MRI at RTP
Strong evidence
There is no strong evidence for an association between MRI parameters at RTP and hamstring re-injury.
Moderate evidence
Moderate evidence for no association with hamstring re-injury was found for the presence of intramuscular fibrosis, longitudinal length of fibrosis, length of fibrosis on axial view, width of fibrosis on axial view, volume of fibrosis and the involved muscle with fibrosis on MRI.17
Limited evidence
Limited evidence for no association with hamstring re-injury was found for the presence of a hyperintensity signal, a normalised T2-hyperintensity signal, length and CSA of the hyperintensity signal on MRI.16 18
Critical post hoc analysis
A not predefined project team consensus meeting on data interpretation revealed that despite the fact that the majority of included studies were at low risk of bias as assessed by the Hayden system, this system was not suitable to detect potentially underpowered studies. The studies included between 4 and 41 re-injuries. With relatively low numbers there was a high risk of a type 2 error (not finding an association when one was actually present). According to Bahr et al 22 20–50 re-injury cases were needed to detect moderate to strong associations, whereas small to moderate associations would need about 200 re-injured subjects. The assessment of these type 2 errors were not taken into account in our predefined research protocol, but would substantially affect the outcome of the systematic review. Therefore additional analysis was performed on the only two studies with ≥20 re-injuries (Ekstrand et al 13 and Reurink et al 17 (table 4)). The study of Ekstrand et al 13 showed a moderate to strong association of injury to the biceps femoris and hamstring re-injury compared with injury to the semimembranosus or semitendinosus muscle. No association with hamstring re-injury was found for grading according to Peetrons on baseline MRI. The study of Reurink et al 17 found that fibrosis on MRI at RTP is not associated with hamstring re-injury. The detection of determinants with a possible small to moderate association with re-injury was not possible, as this required larger sample sizes.
Qualitative analysis showed a moderate level of evidence for these three determinants (table 4). So there was moderate evidence for a moderate to strong association of injury to the biceps femoris and hamstring re-injury, moderate evidence for no association of grading according to Peetrons on baseline MRI and hamstring re-injury and moderate evidence for no association of the presence of fibrosis on MRI at RTP and hamstring re-injury.
Discussion
Main findings
This review showed no strong evidence for any MRI finding at the time of injury or RTP as a risk factor for hamstring re-injury. At baseline, there was moderate evidence that intratendinous injuries, identified on MRI and therefore grading according to the British Muscle Injury Classification, were associated with hamstring re-injury risk. At RTP there was moderate evidence that fibrosis on MRI was not associated with hamstring re-injury. However, this best evidence synthesis did not include correction for the (small) sample sizes. Our post hoc analysis, including two studies with sufficient sample size and a low risk of bias, showed moderate evidence for a moderate to strong association of injury to the biceps femoris and hamstring re-injury compared with injury to the semimembranosus or semitendinosus muscle. Moderate evidence for absence of an association with hamstring re-injury was found at baseline for grading (according to Peetrons) and at RTP for the presence of fibrosis on MRI. The determinants intratendinous injuries and grading according to the British Muscle Injury Classification were not analysed in these two studies.
De Visser et al,5 Rubin et al 6 and Freckleton et al 7 reported in their previous systematic reviews three MRI variables as a risk factor for hamstring re-injury: larger volume size of the initial trauma, a grade 1 hamstring injury at initial trauma compared with grade 0 and grade 2 injuries (classification according to Peetrons) and greater length of the initial injury, seen as oedema (>6 cm long) on MRI. For all three determinants this did not match our results, where we found moderate, strong and strong evidence, respectively, for an absence of association.
This difference could mainly be explained by the inclusion of new and qualitative better studies in our review. Of the five studies included by de Visser et al,5 three were also included in our review.10 14 19 In the other two studies they only performed clinical examination instead of MRI examination. In the review of Rubin et al 6 only 2 studies10 14 presented data about MRI findings as a risk factor for hamstring re-injury, and in the review of Freckleton7 3 of the 34 included studies.10 14 19 These studies were the same as presented by de Visser et al.
Another cause was the difference in re-injury definition; de Visser et al used data from another time frame from the study of Verrall et al than we did.
Re-injury definition
The reported incidence of hamstring re-injuries in this systematic review ranged from 9% to 40%. This wide range could be potentially explained by the different definitions of location, diagnosis and time frame used in the 11 included articles (table 2). Description of the injury location varied from ‘injury in the same limb’ to ‘injury to the same hamstring muscle’ or ‘injury of the same type and at the same site as an index injury’. There was currently no consensus on what constitutes a re-injury.
The diagnosis of any re-injury was confirmed by MRI in two studies, clinical examination in five studies and monitoring with telephone calls in three studies.
The time frame of re-injury definition differed among the studies (table 2). This time frame varied from ‘2 months after return to play (RTP)’, ‘during the same season/competition period’ to ‘1 year’. The exception was Verrall et al,19 who used both the same as well as the subsequent season and therefore showed two different data sets of results. We only used the data from the same season as the hamstring injury, not the data from the subsequent season, because in the data synthesis we used one data set per article and the follow-up of one season gave the best comparison with the length of follow-up of the other studies (follow-up varying from 2 months to a maximum of 1 year).
The heterogeneous follow-up time frames complicated comparing studies. For example, if the follow-up time was 2 months, less re-injuries were to be expected than with a 1-year follow-up.
The length of follow-up within a time frame also could vary a lot. If this length was a standard period, such as one playing season, every patient would have a different exposure time to hamstring re-injury, depending on when they get injured during the season. As a consequence the re-injury risk could vary substantially. Players who get injured at the end of the season, had a very short follow-up duration till the end of the playing season. In the analysis, appropriate adjustment for this exposure time is needed. For further studies standardisation of the follow-up should be defined.
Two studies also included an exacerbation of symptoms before RTP during rehabilitation as re-injuries.15 18 According to the definition of Fuller et al 23 a re-injury can only occur following RTP. Therefore it is questionable if these exacerbations of symptoms should be regarded as a re-injury or require another definition. Additional analysis by Pollock et al,15 after communication with them, and with exclusion of these cases with exacerbations of symptoms instead of a ‘real’ re-injury, still showed a statistically significant association for classification according to the British Muscle Injury Classification and intratendinous injuries with re-injury. In the study of Silder et al,18 only two of the four described re-injuries were ‘real’ re-injuries after RTP. For this study, we performed no additional analysis with exclusion of the exacerbations, because this study was already the most underpowered one and this would not have changed the results.
Finally, only four studies defined the clinical characteristics of a re-injury, such as worsening functional and clinical tests, modification of rehabilitation or training for greater than 48 hours and time loss from training or match play.15 18–20 In other studies, these characteristics had not been specified.
The above mentioned discrepancies on re-injury definition between the included studies, emphasises that there is a lack of consensus on this subject.
Confounding factors
As we were interested in the independent relationship between MRI determinants and hamstring re-injury we used the correction of confounders as an important quality criteria. Unfortunately, only three studies14 15 17 adequately described potential confounders and appropriately accounted for them in the study design or analysis to sufficiently limit the potential bias (table 3, domain 5).
Pollock et al 15 reported a statistically significant association with hamstring re-injury for both grading according to the British Muscle Injury Classification and intratendinous injuries identified on MRI. Involvement of the tendon, however, was a part of the above grading system, so hamstring injuries that extended into the tendon (grade ‘c’ in the grading system) were more prone to hamstring re-injury. In other words, high grading in the classification system also implied a high risk of tendon involvement. Thus the significance of intratendinous injuries ensured that grading according to the British Muscle Injury Classification also showed a significant difference.
In the study of Reurink et al 16 the majority of the participants received an intramuscular injection (with platelet rich plasma or normal saline). The effect of these injections on hamstring muscle healing and MRI appearance is still unknown and possibly postinjection changes of the needle and/or the injected fluid are visible on MRI weeks later. This might have influenced the findings of the MRI and makes it difficult to draw firm conclusions.
Most of the other remaining studies did not mention possible confounders.
Limitations
Our review had some potential limitations. The most important one was the relative low numbers of reported re-injuries of the majority of included articles of this review. Only two articles included ≥20 re-injuries (n=2617 and n=4113),which was generally considered to be sufficient to detect moderate to strong associations. With these potential underpowered studies we could not exclude a type 2 error, which would influence the results. For example, when we viewed the results of all studies together, the specific hamstring muscle involved on MRI showed strong evidence for no association with hamstring re-injury. While when we took the results of only the sufficiently powered studies (post hoc analysis), there was moderate evidence for a moderate to strong association of injury to the biceps femoris and hamstring re-injury.
We refrained from statistical pooling of the data, because of the clinical and methodological heterogeneity of the studies with regard to definitions, outcome measures, MRI findings and methodological quality. This limited the interpretation of the magnitude of the reported associations. However, the quality of a systematic review is not dependent on the presence of meta-analysis, but is dependent on the quality of the studies included. Pooling data from papers with a high risk of bias actually compounds the bias.24
Data extraction of the 11 included articles was suboptimal, as it was performed by just one person instead of two persons.
Finally, we conducted a thorough search using multiple databases, but our search was limited to English, Dutch or German language. We potentially excluded relevant studies published in other languages. There is also a possibility of publication bias, because we only included published literature.
Clinical relevance
The fact that there is moderate evidence that biceps femoris injuries and intratendinous injuries, both identified on baseline MRI, are associated with a higher hamstring re-injury risk might have consequences for interpreting baseline MRIs. Although biceps femoris injury can be established by clinical examination, detecting an intratendinous injury on clinical examination is probably difficult to achieve with confidence. MRI could be used to detect tendon involvement for estimating the re-injury risk. MRI at RTP shows no positive associations with re-injury, and thus seems to have little added value for predicting hamstring re-injury.
At the time of acute injury (baseline), clinical examination might be of more added value than MRI. Clinical factors seem to be important for the estimation of re-injury risk; the number of previous hamstring injuries, active knee extension deficit, isometric knee flexion force deficit at 15°, and presence of localised discomfort on palpation just after RTP are all associated with a higher hamstring re-injury rate.20 Previous ipsilateral ACL reconstruction is also a risk factor for re-injury.5
Future directions
Given the identified limitations, we recommend for further research studies to have larger sample sizes: 20–50 re-injury cases are needed to detect moderate to strong associations, whereas small to moderate associations would need about 200 re-injured cases.22 Adequately describing and accounting for potential confounders and an appropriate statistical analysis will improve the study quality.
For standardising the quality assessment a uniform, reliable and validated risk of bias assessment tool for prognostic studies is indicated. Screening the sample size for power detection is recommended as a separate score.
The heterogeneity of the re-injury definition requires further delineation of the length of follow-up (preferably 2 months for the early and 1 year for the mid-term re-injuries), description of the precise location of the injury and confirmation of the diagnosis by at least clinical examination.
Conclusion
This review of seven low and four high risk of bias prospective studies found no strong evidence for association of any MRI finding at baseline and/or RTP with hamstring re-injury. For baseline MRI findings, there is moderate evidence that intratendinous injuries and therefore higher grading according to the British Muscle Injury Classification are associated with a hamstring re-injury. For all other determinants no association with hamstring re-injury was found.
Due to inclusion of potentially underpowered studies, additional analysis of the only two studies with a sufficient sample size (≥20 re-injuries) showed moderate evidence for a moderate to strong association of biceps femoris injury, identified on MRI, with hamstring re-injury.
What is already known?
Hamstring injuries are associated with high re-injury rates, despite efforts in the prevention and management of these injuries.
Clinical parameters that are associated with a higher hamstring re-injury rate are: active knee extension deficit, isometric knee flexion force deficit at 15° and presence of localised discomfort on palpation just after return to play (RTP). The number of previous hamstring injuries and previous ipsilateral ACL reconstruction are also risk factors for re-injury.
The best available evidence from three previous systematic reviews shows three MRI variables to be related to risk for hamstring re-injury: larger volume size of the initial trauma, a grade 1 hamstring injury at initial trauma compared with grade 0 and grade 2 injuries (classification according to Peetrons) and greater length of the initial injury, seen as oedema (>6 cm long) on MRI. These data date back from 2004, 2006 and 2007 and since then new data on the prognosis of hamstring injuries have been published.
What are the new findings?
Based on the current evidence, there is no strong evidence for any MRI finding at baseline and/or return to play in predicting hamstring re-injury risk.
At baseline MRI there is moderate evidence that intratendinous injuries are associated with a higher re-injury risk.
There is considerable risk of bias in the majority of current studies due to inclusion of potentially underpowered studies. Additional analysis of the only two studies with a sufficient sample size showed moderate evidence for a moderate to strong association of biceps femoris injury with re-injury.
How might it impact on clinical practice in the near future?
Biceps femoris injury can be established by clinical examination and other clinical factors seem to be important for the estimation of re-injury risk. Detecting an intratendinous injury on clinical examination is probably difficult to achieve with confidence, so MRI could be used to detect tendon involvement for estimating the re-injury risk.
MRI at RTP shows no positive associations with re-injury and thus seems to have little added value for predicting hamstring re-injury.
Acknowledgments
The authors thank WM Bramer (biomedical information specialist in the Erasmus University Medical Center, Rotterdam, the Netherlands) for assistance in the search strategy.
References
Footnotes
Contributors All authors have contributed to the development of the research question and study design. MvH and RdV developed the literature search, whilst GR and MHM performed the study selection. JLT, R-JdV and JO achieved the risk of bias assessment. MvH extracted the data and made a data synthesis of the included studies. MvH developed the first draft, all authors developed the subsequent drafts of the manuscript. All authors reviewed and approved the manuscript.
Funding JT's institute received funding from the Marti-Keuning-Eckhardt Foundation for the preparation of this review, but none of the authors was personally financially compensated.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.