Article Text

Abstract
Background Physical inactivity is common in older age, yet increased activity benefits older people in terms of preventing chronic disease and maximising independence. Health coaching is a behaviour change intervention that has been shown to increase physical activity in clinical populations. This systematic review and meta-analysis investigated the effect of health coaching on physical activity, mobility, quality of life and mood in older people.
Methods MEDLINE, EMBASE, CENTRAL, PsycINFO, PEDro, SPORTDiscus, LILACS and CINAHL databases were used to identify randomised controlled trials which evaluated the effect of health coaching on physical activity (primary outcome) among people aged 60+. Secondary outcomes were mobility, quality of life and mood. We calculated standardised mean differences (SMDs, Hedges’ g) with 95% CIs from random effects meta-analyses.
Results 27 eligible trials were included. Health coaching had a small, statistically significant effect on physical activity (27 studies; SMD = 0.27; 95% CI 0.18 to 0.37; p<0.001). There was no evidence of an effect of health coaching on mobility (eight studies; SMD = 0.10; 95% CI −0.03 to 0.23; p=0.13), quality of life (eight studies; SMD = 0.07; 95% CI −0.06 to 0.20; p<0.05) or mood (five studies; SMD = 0.02; 95% CI −0.12 to 0.16; p=0.83).
Conclusions Health coaching significantly increased physical activity in people aged 60+. There was no evidence of an effect of health coaching on quality of life, mobility and mood, so different approaches may be required to impact on these outcomes.
- Physical activity
- Elderly people
Statistics from Altmetric.com
Introduction
Physical inactivity is estimated to cause more than five million deaths worldwide each year and was reported to be among the 10 leading risk factors for global disease burden in the 2010 Global Burden of Disease Study.1 2 Physical inactivity contributes to between 6% and 10% of the world’s major non-communicable diseases, including cardiovascular disease, diabetes, cancer and depression,1 and was described as a pandemic in the 2012 special issue on physical activity in The Lancet.3 Inactivity has been documented to increase as age increases, with the most inactive segment of society being those aged 80 years and over.4 5 However, older people have the most to gain from maintaining an active lifestyle in terms of disease prevention and maximising functional independence.6
Faced with the substantial burden of inactivity,3 health services are exploring innovative strategies to reverse this trend and reduce its associated cost to society. One approach to addressing this health issue is by promoting patient-centred self-management strategies. These strategies aim to encourage health behaviour change in relation to physical activity participation in order to reduce the risk and impact of chronic conditions.7
Health coaching is one strategy that aims to encourage healthier lifestyle choices and promote better management of conditions with a potentially lower cost and greater convenience than traditional healthcare services.8 A recent systematic review9 identified an emerging consensus on the definition of health coaching, which is: ‘a patient-centred process that is based upon behaviour change theory and is delivered by health professionals with diverse backgrounds. The actual health coaching process entails goal setting determined by the patient, encourages self-discovery in addition to content education, and incorporates mechanisms for developing accountability in health behaviours.’ Although there are many different models or frameworks that can be used within a health coaching approach, it commonly includes motivational interviewing techniques and solution-focused goal setting as a strategy for effective intervention.7 10–12 Health coaching has recently emerged as a promising behavioural intervention for improving health outcomes and health behaviour for people with diabetes, obesity, low back pain and risk of cardiovascular disease.9 13 14
Given the recent rise in the use of health coaching, there has been an increase in the number of published trials examining the effect of health coaching to improve physical activity participation. The effectiveness of health coaching has been tested in randomised controlled trials (RCTs) involving clinical populations.15–18 However, there is a lack of published research that summarises the effect of health coaching on physical activity participation in general samples of community-dwelling older people. To address this current evidence gap, we conducted a systematic review and meta-analysis of randomised trials that evaluated the effect of health coaching on physical activity among people aged 60 years and older. The secondary aims were to examine the effect of health coaching on mobility, quality of life and mood among people aged 60 years and older.
Methods
Search strategy and selection criteria
The review protocol was registered with the PROSPERO database prior to commencement (#CRD42014013224). Reporting has been guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.19
A systematic literature search was conducted in MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), PsycINFO, the Physiotherapy Evidence Database (PEDro), SPORTDiscus, Lilacs and CINAHL databases from inception to May 2016. Keywords, Medical Subject Headings (MeSH) and other index terms, as well as combinations of these terms and appropriate synonyms were used to construct the search strategy, including health coaching, wellness coaching, physical activity counselling, older people, aged, randomised and controlled trial (see online supplementary appendix 1). The reference lists of relevant systematic reviews were also handsearched. There were no restrictions on language.
Supplementary file 1
Titles and abstracts were screened independently by two reviewers (JSO and ABA). The full report of potentially eligible articles was obtained and assessed using an electronic screening form designed to assess the predetermined eligibility criteria (Box 1). All disagreements regarding the selection of included studies were solved by discussion and, when necessary, arbitration occurred with a third reviewer (AT). We included a PRISMA study flow diagram to document the screening process.
Inclusion criteria
Design: Randomised and quasi-randomised controlled trials
Participants: Adults aged 60 years and over
Intervention: Health coaching with a clear focus on changing behaviour and attaining health promotion goals
Control: No intervention, usual care or wait-list control
Outcomes measured related to: Physical activity, mobility, quality of life and mood
Assessment of trial characteristics and risk of bias
Quality
The Physiotherapy Evidence Database (PEDro) Scale (1–10), which assesses the internal validity of a RCT,20 21 was used to rate the methodological quality of included trials. PEDro scores were extracted from the PEDro database (www.pedro.org.au).
Participants
Eligible studies were those that included only participants 60 years of age or older or trials in which participants had an average or median age of at least 60 years old. No restriction was placed on the source of the participants, that is, patients from primary care as well as community settings were eligible, and the source of recruitment was recorded.
Intervention
Trials were included if the intervention involved health coaching aimed at increasing physical activity participation with a clear focus on changing behaviour (ie, physical activity) and attaining health promotion goals. The term physical activity was defined according to the American College of Sports Medicine (ACSM) definition as: ‘any body movement that is produced by the contraction of skeletal muscles that increases energy expenditure’.22 Trials that included telephone-based health coaching, coaching supported by mobile technology, motivational interviewing, intervention via internet and face-to-face coaching were included. We did not consider trials to be eligible if the intervention only included provision of written advice about increasing physical activity without any individually tailored discussion from a health coach or similar.
Types of studies
Only RCTs and quasi-RCTs were included in this review. To be eligible, trials had to consist of one group that received the health coaching intervention and a comparison group that received usual care or wait-list control or included a no intervention control group. We did not include trials that compared health coaching with another intervention aimed at increasing physical activity levels (eg, provision of a pedometer).
Outcome measures
Trials were eligible for inclusion if they included physical activity as an outcome measure (primary outcome for this systematic review). Secondary outcome measures were mobility, quality of life and mood.
Outcome data were extracted for preintervention and postintervention time points. If baseline values were not reported, groups were compared at follow-up. If multiple follow-up data points were provided, the scores obtained as close to the completion of the intervention as possible were used.
Objectively measured (such as with accelerometers or pedometers) and self-reported (with validated questionnaires) physical activity measures were included. Secondary outcome measures of mobility included any validated methods measuring gait speed, sit to stand, functional tests or other mobility scales. Measures of quality of life included any validated questionnaire of health-related quality of life, health status and functional status. Validated measures of mood included self-reported questionnaires of depression and anxiety.
Data extraction
Two review authors (JSO and AA) independently extracted study characteristics (details of participants, settings, interventions and outcomes) from the included trials using pretested standardised data extraction forms. Outcome data collected at baseline and at first follow-up or only at first follow-up included physical activity, mobility, quality of life and mood.
Authors of the included studies were contacted via email if the study reports were incomplete or if data were missing. If the author did not reply within 2 weeks, a second email was sent as a reminder. If, at the end of the fourth week, a reply had not been received, available data were used.
Data analysis
Details of the setting, health coaching intervention components, intervention dose, outcomes measured and timing of measurements were summarised descriptively. We conducted random effects meta-analyses for each outcome (physical activity, mobility, quality of life and mood) using Comprehensive Meta-Analysis software (Version 2, Biostat, Englewood, New Jersey, USA).
The standardised mean difference (SMD) (Hedges’ g) was calculated for each meta-analysis, standardised by postscore SD (or its estimate) and calculated using the premean and postmean and SD or, when this was unavailable, the mean change score. Effect sizes were categorised as small (0.2), medium (0.5) or larger (0.8 or greater).23
Statistical heterogeneity was determined by visual inspection of the forest plots and with consideration of the I2 and χ2 tests. Clinical heterogeneity was determined by consensus between the investigators on the basis of collective experience in the field.
Exploratory meta-regression analyses were undertaken to determine sources of between-study heterogeneity. Meta-regression was carried out for the primary outcome (ie, physical activity) to determine if there were significant differences in the intervention effect sizes between trials that included participants with clinical conditions and those that were recruited from the general older population. Meta-regression was also used to explore differences in effect sizes between trials in which health coaching was primarily delivered face to face and trials in which the intervention was primarily delivered by telephone. Further meta-regression was conducted to examine the effect of study methodological quality, as measured with the PEDro score, on the pooled effect size. We dichotomised PEDro scores into categories of ≥6 (indicating higher methodological quality) and <6 (indicating lower methodological quality). A meta-regression examining the impact of study sample size on the pooled effect of health coaching was also undertaken. Trials were dichotomised into two categories of small trials (n≤100 participants) and large trials (n>100 participants). Additionally, meta-regression analysis was conducted to examine if there were differences in the effect of health coaching on physical activity between trials that used objective measures of physical activity and those that used self-report questionnaires to measure physical activity.
Furthermore, we investigated publication bias by using a funnel plot of the effect estimates from included studies. The funnel plot was assessed by visual inspection and by using Egger’s test, with p<0.1 as evidence of publication bias.24
Results
Flow of trials through the review
A total of 1092 studies were identified through database searching after removing duplicates. Handsearching identified two additional records of which one was ineligible25 and one was eligible.26 After screening of 111 full-text papers, 27 original trials fulfilled the inclusion criteria and were included in the review.15–18 26–48 Figure 1 presents the flow of studies through the review.

Flow of studies through the review. RCT, randomised controlled trial.
All included trials were pooled in the primary meta-analysis evaluating the effect of health coaching on physical activity. For secondary analyses, eight trials were pooled reporting mobility outcomes,31 34 35 37 42 44 47 48 five trials were pooled reporting mood outcomes17 31 37 39 42 and eight trials were pooled reporting quality of life outcomes.16 18 31 34 37 38 40 48
Characteristics of included trials
The 27 trials included in the review were conducted in eight different countries: single trials were conducted in Canada46 and Italy,32 2 in Belgium,30 36 New Zealand38 40 and United Kingdom,29 42 4 in Australia,15 16 28 48 5 in The Netherlands,18 27 31 37 39 and 10 in the USA.17 26 33–35 41 43–45 47 Online supplementary appendix 2 summarises the characteristics of the included trials, including participant characteristics and summary of intervention and control group components.
Supplementary file 2
Quality
The methodological quality and the reporting of eligible trials are presented in online supplementary appendix 3. The total PEDro scores ranged from 3 to 8, with a mean of 6. For the primary outcome, 17 trials15 16 18 26 30 32 33 38–40 42–48 were of high methodological quality on the PEDro Scale and 10 were of low quality.17 27–29 31 34–37 41 For mobility outcome, four trials33 42 44 47 48 were of high methodological quality, while four were low.31 34 35 37 For quality of life outcome, five trials16 18 38 40 48 were of high methodological quality, while three were low,31 34 37 and for mood outcome, two of the five trials39 41 were of high methodological quality and three were low.17 31 37 Randomisation of participants and calculation of point estimates and variability were carried out in all 27 trials. Intention-to-treat analysis was infrequently undertaken (10/27 studies; 37%). As expected with this type of intervention, none of the trials included blinded participants or blinded therapists.
Supplementary file 3
Participants
A total pooled sample of 5803 participants was included in the primary analysis. Trials included in the mobility analysis involved 2051 participants, and trials pooled for the quality of life analysis involved 1923 participants. For mood, included trials involved 769 participants.
The mean age of the participants in the included trials ranged from 60 to 79 years. Three trials included men only33 43 44 and all the other trials included both men and women. Fourteen trials recruited participants with a specific clinical condition. Of these, five trials recruited patients with chronic obstructive pulmonary disease27 30 31 36 37 and single trials recruited participants with metabolic syndrome,28 chronic heart failure,29 diabetes,32 colorectal cancer,16 multiple chronic illness,43 coronary artery disease,46 rheumatoid arthritis,39 stroke15 and Parkinson’s disease.18
Eight of 27 (32%) trials recruited participants from primary care,26 27 33 34 38 43–45 six trials (24%) recruited from community,17 26 35 42 47 48 five (20%) recruited from hospital,18 27 36 39 46 three (12%) recruited from outpatient clinic,15 32 37 two recruited from pulmonary rehabilitation30 31 and single trials recruited from a senior centre,41 a rural community28 and a cancer registry.16
Outcome measures
For the primary outcome of physical activity, the most commonly used measures were accelerometer-recorded activity (six studies),15 30 36 42 45 47 pedometer-recorded steps (four studies)27 31 37 46 and the self-reported Community Healthy Activities Model Program for Seniors (CHAMPS) Questionnaire (four studies),33 41 43 44 with the remaining studies using other self-report measures (see online supplementary appendix 2). Scores from the Timed Up and Go (TUG) test, Short Physical Performance Battery (SPPB), Chair-Stand test and The Tinetti Gait and Balance test were pooled for the mobility analysis.31 34 35 37 42 44 47 48 The Health Survey Short Form-36 (SF-36), The RAND 36-item Health Survey, Parkinson’s Disease Questionnaire (PDQ-39), the St. George’s Respiratory Questionnaire and the Quality of Life Questionnaire (AQoL) were pooled to investigate the impact of physical activity on quality of life.16 18 31 34 37 38 40 48 Scores from the Beck Depression Inventory (BDI), Brief Symptom Inventory (BSI), The Geriatric Depression Scale (GDS) and Hospital Anxiety and Depression Scale (HADS) were pooled for the mood analysis.17 31 37 39 42
Intervention
In all studies, the experimental group received a health coaching intervention that used behavioural change techniques and goal setting. Intervention dose ranged from 3 to 24 sessions with each session ranging from 10 to 60 min. The duration of the interventions ranged from short (ie, 4 weeks) to as long as 96 weeks, and the mean duration was 28 weeks.
Health coaching was delivered via telephone in 10 trials,16 28 34–36 40–43 48 face to face in 7 trials18 27 29–31 37 39 and via both face to face and telephone in 10 trials.15 17 26 32 33 38 44–47 The person who delivered the health coaching varied between studies and included exercise counsellor, physiotherapist, physician, nurse, psychologist, primary care provider, health educator, geriatrician and researcher.
The control groups of 13 studies17 18 27 28 30 31 37 38 40 42 44 46 48 received no intervention or wait-list control/usual care and in 12 studies15 16 26 29 32 33 35 36 39 41 43 45 written information or educational session/advice was provided. In single studies, control participants received individualised goals34 and walking plan with no follow-up counselling or provision of an activity tracker with no feedback.47
Adverse events
Nine included trials measured adverse events related to the physical activity intervention.15 18 26 33 34 38–40 42 Two trials reported that no adverse events occurred.39 42 Six of the trials reported falls and musculoskeletal injuries that occurred during the physical activity intervention; however, no major adverse events were directly attributed to the intervention.15 18 33 34 38 40 The remaining one trial reported minor adverse events as a result of the physical activity intervention such as mild muscular fatigue, strain or soreness during the initial months of intervention.26
Publication bias
The funnel plot did not display overt asymmetry and the Egger’s tests revealed no significant publication bias (p=0.21) (see online supplementary appendix 4).
Supplementary file 4
The effect of health coaching on physical activity levels
The pooled effect of health coaching on the primary outcomes indicates a small but statistically significant effect on physical activity levels in participants who received health coaching versus control participants (27 studies; SMD=0.27; 95% CI 0.18 to 0.37; p<0.001, I2=61%; figure 2).

Effect size (95% CI) of health coaching on physical activity by pooling data from 27 studies comparing health coaching versus control using random effects meta-analysis (n=5803).
In the 18 trials in which health coaching was primarily delivered via telephone, the impact on physical activity was small (SMD=0.21; 95% CI 0.11 to 0.32; p<0.001). For the nine trials in which the intervention was primarily delivered via face-to-face sessions, a larger pooled effect was found (SMD=0.41; 95% CI 0.25 to 0.58; p<0.001). The difference between the subgroups was statistically significant (p=0.047).
No significant difference in the effect of health coaching on physical activity levels was found between trials which recruited participants with a health condition and those that recruited general, healthy community-based people (p=0.32). In the 14 trials in which the participants had some clinical conditions, there was a small effect on physical activity levels (SMD=0.32; 95% CI 0.19 to 0.45; p<0.001), while in the 13 trials of general healthy participants, a smaller pooled effect on physical activity was found (SMD=0.23; 95% CI 0.10 to 0.36; p<0.001).
The size of the effect of health coaching on physical activity did not appear to be influenced by the methodological quality or sample size of the included trials. The impact on physical activity levels in the 17 trials with a PEDro score of 6 or more (SMD=0.26; 95% CI 0.15 to 0.39; p<0.001) was similar to the effect in the 10 trials with PEDro scores less than 6 (SMD=0.29; 95% CI 0.12 to 0.45; p<0.01). The difference between these subgroups was not statistically significant (p for comparison=0.86). In the 10 trials with a sample size of 100 or less participants, the impact of the intervention (SMD=0.32, 95% CI 0.10 to 0.53; p<0.01) was also comparable with the result in the 17 trials with a sample size of more than 100 (SMD=0.26; 95% CI 0.16 to 0.37; p<0.001). The difference between the subgroups was not statistically significant (p=0.66).
No significant difference in the effect of health coaching on physical activity levels was found between trials that used objective measures of physical activity and those that used self-report questionnaires to assess physical activity levels (p=0.41). In the 10 trials that used objective measures, there was a small effect on physical activity levels (SMD=0.35; 95% CI 0.14 to 0.56; p<0.01), and in the 17 trials that used self-report questionnaires, a smaller pooled effect on physical activity was found (SMD=0.26; 95% CI 0.15 to 0.36; p<0.001).
The effect of health coaching on secondary outcome measures
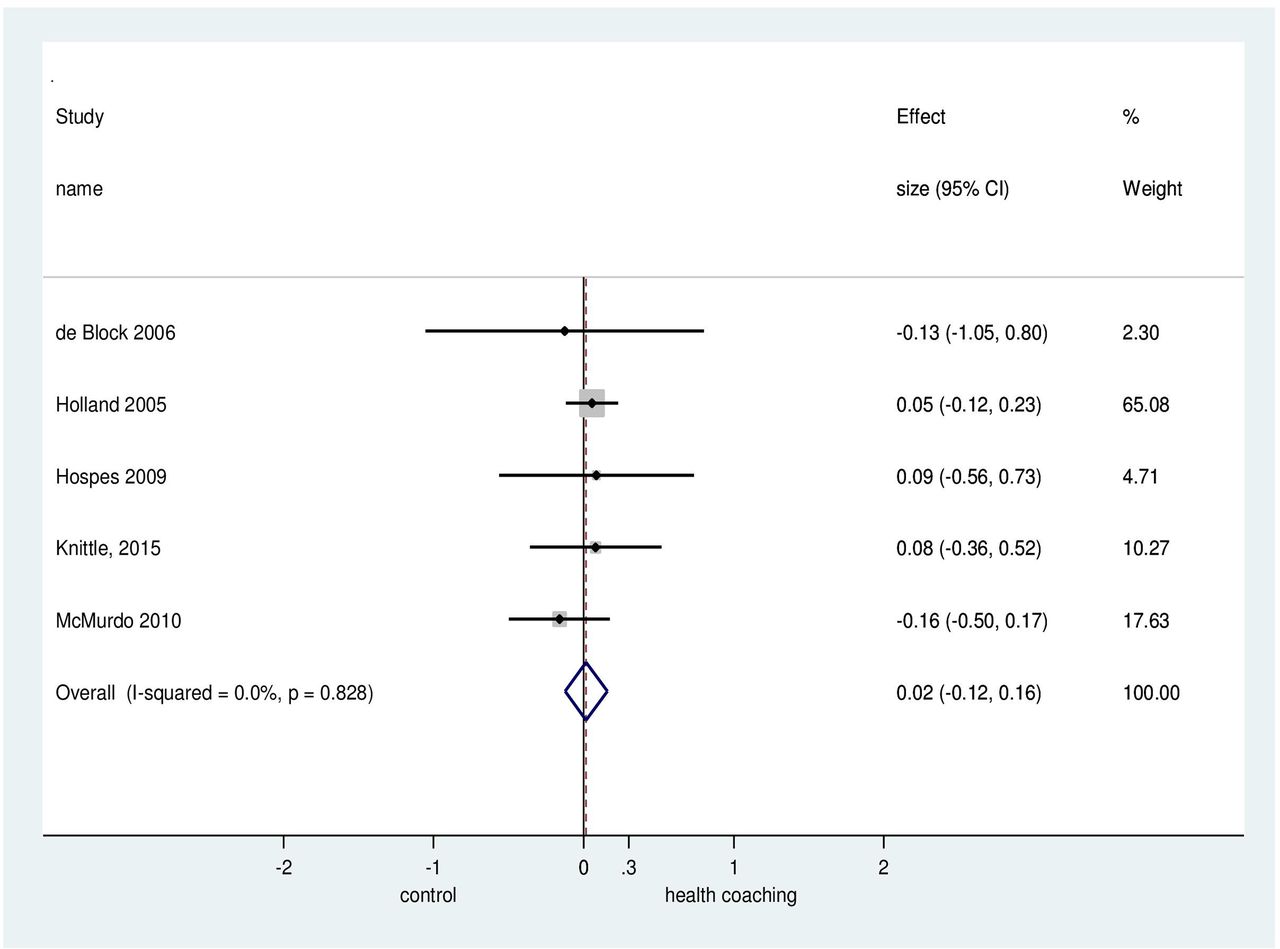
There was no evidence of a differential effect of health coaching compared with control in improving mobility (eight studies; SMD=0.10; 95% CI −0.03 to 0.20; p=0.23; I2=38%, figure 3), quality of life (eight studies; SMD=0.07; 95% CI −0.06 to 0.20; p<0.05; I2=54%, figure 4) or mood (five studies; SMD=0.02; 95% CI, −0.12 to 0.16; p=0.83; I2=0%, figure 5).
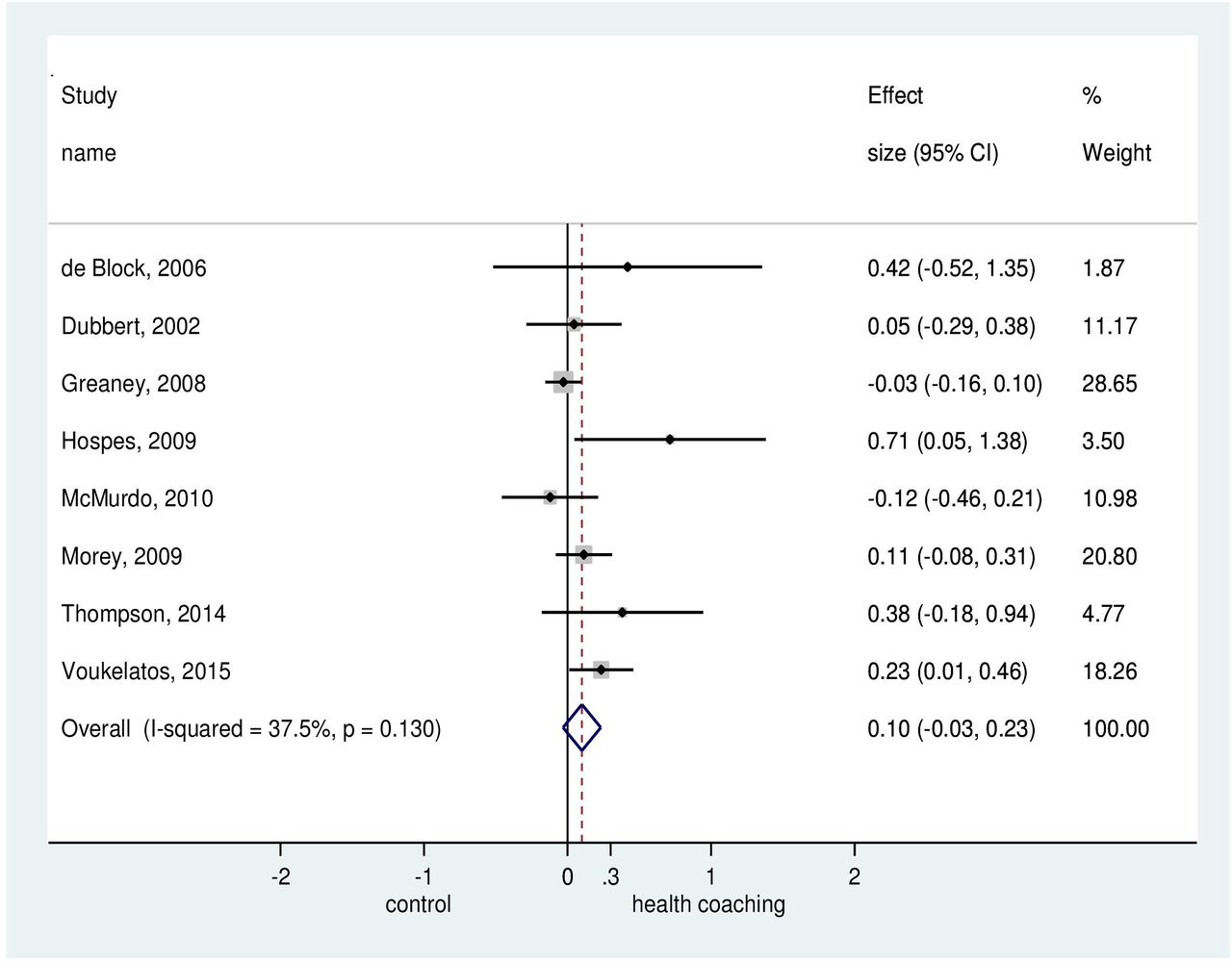
Effect size (95% CI) of health coaching on mobility by pooling data from eight studies comparing health coaching versus control using random effects meta-analysis (n=2051).

Effect size (95% CI) of health coaching on quality of life by pooling data from eight studies comparing health coaching versus control using random effects meta-analysis (n=1923).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect size (95% CI) of health coaching on mood by pooling data from four studies comparing health coaching versus control using random effects meta-analysis (n=769).
Discussion
Principal findings
In this systematic review and meta-analysis, we found that health coaching was effective in improving physical activity participation in older people. Our meta-regression results demonstrate that health coaching was equally as effective for older adults with clinical conditions and for apparently healthy older adults and that study quality or sample size did not influence the size of the effect of health coaching on physical activity. The meta-regression results also found that although both face-to-face and telephone-based health coaching were effective in increasing physical activity participation among older people, greater effects on physical activity levels were seen from interventions delivered face to face compared with telephone-based methods.
The average effects of health coaching on physical activity were relatively small (SMD=0.27), but we found wide variation in the health coaching methods, the target population, mode of delivery (ie, face to face or telephone coaching), who delivered the intervention, frequency and duration of the interventions in the included trials. There were too few trials to investigate whether these aspects impacted on the results and for this reason more research is needed to fully explore the potential of health coaching for increasing physical activity. Nonetheless, our findings are consistent with a previous systematic review11 that identified evidence of a substantial effect of health coaching on increasing physical activity levels in patients with chronic disease at follow-up.
We observed no effect of health coaching on quality of life, mobility and mood; however, data were limited to trials that included at least physical activity as an outcome, so other relevant studies that included measures of quality of life, mobility and mood may have been missed. Moreover, it is likely that the small impact of health coaching on physical activity levels was not sufficient to translate to changes in mobility, quality of life and mood outcomes. It is also possible that improvements in these outcomes may require different approaches to health coaching or other interventions.
Strengths and weaknesses of the study
To the best of our knowledge, this is the first systematic review and meta-analysis to evaluate the impact of health coaching on physical activity levels in a broad range of people aged 60 years and older. This systematic review was conducted in accordance with PRISMA guidelines, followed the prospectively registered protocol and was not restricted by publication, language or date. A key strength is that the 27 included trials involved a substantial and diverse sample of 5803 healthy and clinical participants. We undertook a comprehensive search to identify eligible trials. All included studies were RCTs and the majority (17/27) were of relatively high methodological quality (mean PEDro score of 6).
We acknowledge that this review also has certain limitations. One potential limitation is that we only included outcome data from the immediate postintervention time point, limiting our results to the short-term or immediate effect of health coaching on physical activity without consideration of the longer-term sustainability of effects.
Further potential sources of bias relate to methodological shortcomings of the included trials such as the lack of concealed allocation, blinding of therapists and patients. Moreover, most of the included trials did not use intention-to-treat analyses, which might have introduced risk of bias. Other potential sources of bias include the use of self-report measures of physical activity in most of the included studies. Self-report measures are susceptible to recall and response bias49 and can overestimate as well as underestimate the impact of interventions on physical activity levels. However, it is worth emphasising that the pooled analysis based on physical activity and the subgroup analysis revealed no significant difference in the effect of the intervention on physical activity levels between trials that used objective measures and those that used self-report questionnaires. Finally, it is possible that the results of some included trials were impacted by the Hawthorne effect, which may have increased physical activity levels in control group participants and hence lessened the between-group differences in these trials. Encouragingly, the funnel plot did not suggest publication bias.
In this review, we included any health coaching intervention which aimed to increase physical activity participation with a clear focus on changing behaviour and attaining health promotion goals. However, the term health coaching as an intervention strategy may not have been cited in the included papers since other terms are often used such as wellness coaching, physical activity counselling, exercise counselling, physical activity advice and behaviour change intervention. It is possible that relevant studies may have been missed due to the lack of clarity in terminology used for what might have been a similar approach. Likely, one major reason for this is the fact that there is a lack of standardisation in the concept of health coaching9; therefore, there is a critical need for a consistent and clear definition of health coaching as a specific intervention.
Implications for clinicians and policy makers
Given the well-known benefits of physical activity for healthy ageing, interventions that influence adoption of healthy lifestyle behaviours such as physical activity are needed. Health coaching is an effective and promising intervention strategy that could help to combat low physical activity participation rates in people aged 60 and older. Although this review identified only a small effect of health coaching on physical activity, this result needs to be considered in the context of the practicality and low cost of delivering such interventions in order to gain a significant public health impact. A previous review50 identified that behavioural physical activity interventions can improve physical activity at a relatively lower cost than other interventions, making health coaching likely to be a good investment for inclusion in clinical practice as part of a physical activity programme with demonstrable benefits for older people.
Since health coaching was effective in increasing physical activity among healthy older people and those with clinical conditions, it can be recommended as a physical activity promotion strategy for older people with a range of health states and abilities.
Both face-to-face and telephone-based health coaching were effective in improving physical activity participation among older people. However, although health coaching delivered via telephone is a more convenient and low-cost option of delivery, the interventions that included face-to-face sessions were more effective in increasing physical activity than telephone-based methods. Future studies can explore the relative cost effectiveness of the two approaches.
Unanswered questions
Clearly, further research is needed to obtain consensus on the precise definition of health coaching and what comprises this approach as a specific intervention. Research is therefore needed to establish the most effective mode of delivery for health coaching, and the optimal dose and length of the intervention for maximising the impact on physical activity participation among older people. In addition, economic evaluations are warranted to investigate the cost effectiveness of health coaching.
The sustainability of effect of health coaching on physical activity levels in older people remains unknown as our results were limited to the short-term effects. Hence, additional studies should examine the longer-term effects of health coaching among older people. Our findings also point to the need for future reviews that evaluate specifically the impact of health coaching on other measures of health such as mobility, quality of life and mood.
A better understanding of the role of health coaching for increasing physical activity participation will be enhanced by more methodologically rigorous clinical research using well-designed interventions with explicit definitions and methods of health coaching used to underpin their intervention.
Conclusion
Our results provide evidence that health coaching is an effective intervention for increasing physical activity participation among people aged 60 years and older. Our findings are widely generalisable to older adults with clinical conditions and to healthy older adults. Both face-to-face and telephone-based health coaching were effective in improving physical activity participation among older people. However, although health coaching delivered via telephone is a more convenient and low-cost option of delivery, the interventions that included face-to-face sessions were more effective in increasing physical activity than telephone-based methods. We found no evidence of an effect of health coaching on quality of life, mobility and mood, so different approaches to health coaching or other interventions may be required to impact on these outcomes. Further research is warranted to determine a consistent definition of health coaching as a specific behaviour change intervention and to identify the optimal intervention modality, frequency and dose. Future studies are also needed to explore the relative cost effectiveness of the face-to-face and telephone-delivered health coaching.
What are the new findings?
Health coaching is an effective intervention for increasing physical activity among people aged 60 years and older with a broad range of health states.
Health coaching was equally as effective for older adults with clinical conditions and for apparently healthy older adults.
Health coaching delivered face to face was more effective in increasing physical activity participation among older people than telephone-delivered health coaching.
There was no evidence of an effect of health coaching on quality of life, mobility and mood.
References
Footnotes
Contributors JSO, AT and CS conceived the study and contributed to study design and interpretation of the data. JSO coordinated the literature search and data collection with assistance from ABA and ABD. JSO, AT, ABD and CS contributed to data analysis and interpretation of the data. JSO drafted the manuscript and all authors contributed to revisions and approved the final manuscript. JSO is the guarantor for the study.
Funding This review received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. JSO, ABA and ABD are supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil. CS holds a fellowship from the National Health and Medical Research Council (NHMRC), Australia. AT holds a career development fellowship from the National Health and Medical Research Council (NHMRC), Australia.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data.