Article Text

Abstract
Background Hamstring injuries remain prevalent across a number of professional sports. In football, the incidence has even increased by 4% per year at the Champions League level over the last decade. The role of muscle strength or strength ratios and their association with risk of hamstring injury remain restricted by small sample sizes and inconclusive results.
Purpose The purpose of this study is to identify risk factors for hamstring injury in professional football players in an adequately powered, prospective cohort study. Using both established (isokinetic) and novel (eccentric hamstring test device) measures of muscle strength, we aimed to investigate the relationship between these strength characteristics over the entire range of motion with risk of hamstring injury.
Methods All teams (n=18) eligible to compete in the premier football league in Qatar underwent a comprehensive strength assessment during their annual periodic health evaluation at Aspetar Orthopaedic and Sports Medicine Hospital in Doha, Qatar. Variables included isokinetic strength, Nordic hamstring exercise strength and dynamic hamstring: quadriceps ratios.
Results Of the 413 players included (68.2% of all league players), 66 suffered a hamstring injury over the two seasons. Only isokinetic quadriceps concentric at 300°/s (adjusted for bodyweight) was associated with risk of hamstring injury when considered categorically. Age, body mass and playing position were also associated with risk of hamstring injury. None of the other 23 strength variables examined were found to be associated with hamstring injury.
Conclusion The clinical value of isolated strength testing is limited, and its use in musculoskeletal screening to predict future hamstring injury is unfounded.
- hamstrings
- isokinetic
- risk factor
- injury prevention
Statistics from Altmetric.com
Introduction
Hamstring injuries have remained prevalent across a number of professional sports.1 In football, the incidence has even increased by 4% per year over the last decade at the Champions League level.2 Recently, the complexity involved with the occurrence of injury has been highlighted,3 but clinically meaningful risk factor identification remains an important part of the injury prevention model.4 The most recent meta-analysis identified age, previous hamstring injury and quadriceps strength as risk factors for a primary or recurrent hamstring injury.5 Isokinetic muscle strength in particular has received much attention in the literature.6–10 In addition, lower limb strength balance, typically expressed as hamstring-to-quadriceps (H:Q) strength ratio, has also been associated with an increased risk of hamstring injury, although the results have been inconsistent.8 10–12 Alternative measures of eccentric muscle strength have been suggested,13 and recently, a novel device was developed to objectively measure eccentric hamstring muscle strength when performing the Nordic hamstring exercise.14
The findings related to muscle strength or strength ratios and their association with risk of injury remain restricted by small sample sizes and inconclusive results.5 Further exploration of these strength ratios between hamstrings and quadriceps muscle groups has been suggested to include a more dynamic representation,15 as well as the ‘dynamic control ratio’ which represents the net joint torque at different angles over the entire range of motion.16 However, this approach has not been investigated prospectively. Although the need for adequately powered studies with appropriate design was called for more than a decade ago,17 few such prospective studies exist. Previous methodological limitations include inconsistency regarding injury surveillance, biased sampling of previous injury data and a lack of recorded exposure for the athletes included.18
The purpose of this study was to identify risk factors for hamstring injury in professional football players in an adequately powered, prospective cohort study. Using both established (isokinetic) and novel (eccentric hamstring test device) measures of muscle strength, we aimed to investigate the relationship between these strength characteristics over the entire range of motion with risk of hamstring injury.
Methods
Study design
All teams (n=18) eligible to compete in the Qatar Stars League (QSL), the premier football league in Qatar, agreed to participate in the study, which covered two football seasons (September 2013 to May 2015). Each player from the respective teams underwent an annual periodic health evaluation (PHE) at Aspetar Orthopaedic and Sports Medicine Hospital in Doha, Qatar. The PHE was performed from May to September, with the official start of the season in September of each year. If players performed PHE outside of this period and met the inclusion criteria, they were still included in the study.
All players over the age of 18 years and eligible to compete in the QSL, who had provided written consent and were able to perform the strength testing, were included. Players who were injured at the time of the PHE and therefore unable to perform the tests were excluded. If no isokinetic test was performed at the start of a season or no exposure or injury surveillance data were recorded over an entire season, players were also excluded. Figure 1 depicts the inclusion methodology during the two study seasons.
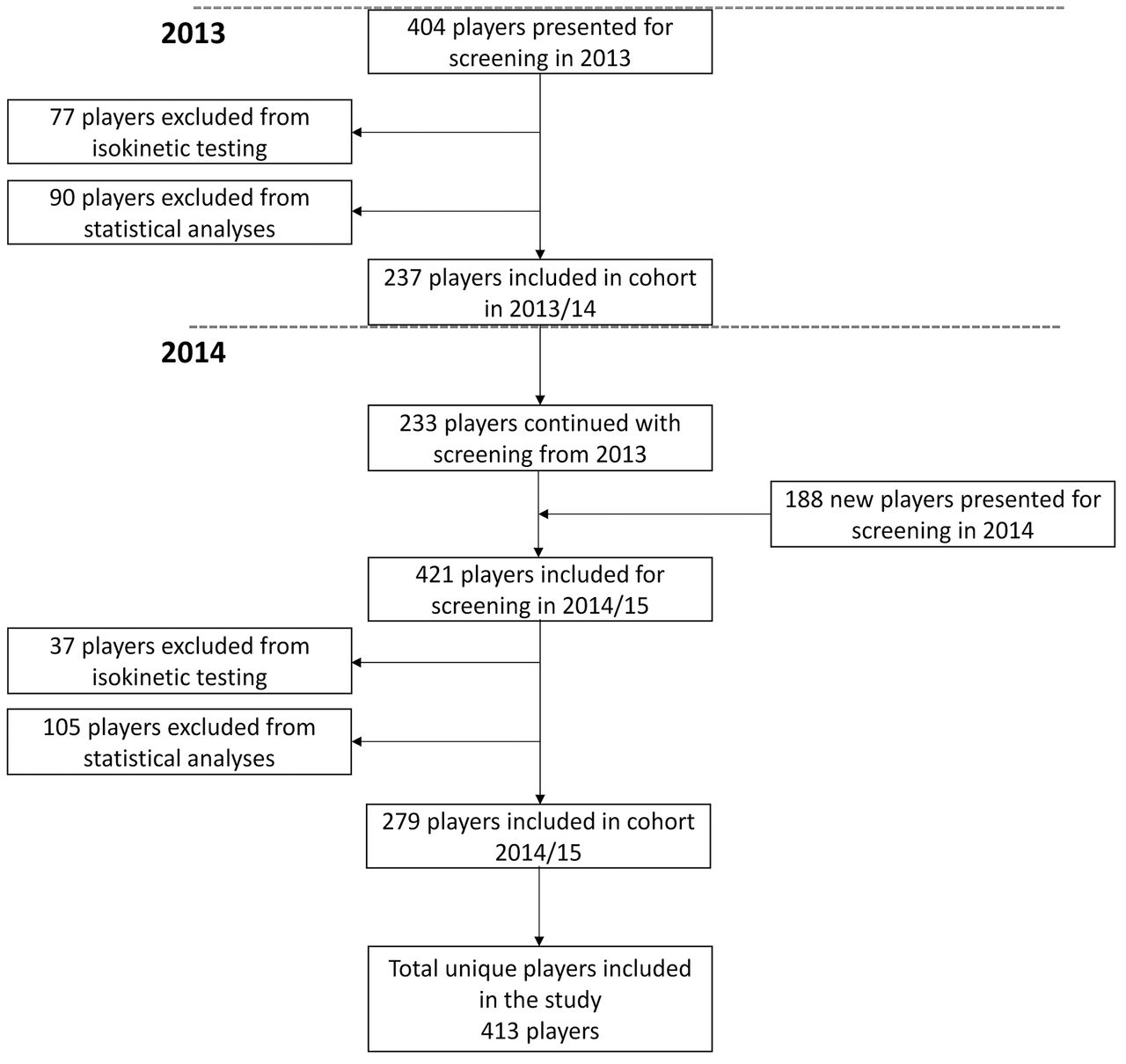
Flow chart demonstrating the movement of players and repeated measurements between different seasons.
Player information
All likely non-modifiable risk factors were considered. A history of previous hamstring injury in the past 12 months,19 20 season, team, leg dominance, position and ethnicity were recorded. Player height and weight were measured, and body mass index (BMI) was calculated during the PHE.
History of previous injury was self-reported at the time of screening and cross-checked with their hospital medical file for the entire cohort. To minimise recall bias and account for players not willing to reveal past injuries during screening, we also conducted a subgroup analysis including only players playing in the QSL during the previous seasons (2012–2014) and therefore were covered by our prospective injury surveillance.
Isokinetic strength testing
Knee flexion and extension muscle strength were tested using an isokinetic dynamometer (Biodex Multi-joint System 3, Biodex Medical Systems, New York, USA). After an explanation of the testing methodology, the player performed a 5–10 min warm up routine, cycling on a stationary exercise bike (Bike Forma, Technogym, Cesena, Italy).
The order (ie, left, right) was randomised and maintained for each of the three different testing modes and speeds for the each subject. All players completed the test procedure as previously described.18
First, the players were tested over five repetitions of concentric knee flexion and extension at 60°/s, followed by 10 repetitions of concentric knee flexion and extension at 300°/s. These test modes measures the concentric strength of the quadriceps (knee extension) and hamstring (knee flexion) muscles. Finally, players performed five repetitions of eccentric knee extension at 60°/s which measures the eccentric strength of the hamstring muscles. The highest peak torque value observed from all repetitions performed for each of the three different tests was recorded.
Dynamic control profile
The dynamic control profile represents the net joint torque (eccentric hamstrings to concentric quadriceps) over the entire range of motion during isokinetic testing.16 The specific knee flexion angle where the quadriceps torque was greater than the eccentric hamstring torque was identified, and the torque-angle plots for eccentric hamstrings and concentric quadriceps were determined using a custom algorithm created in Labview (V.7.0 National Instruments, Austin, Texas, USA) and exported in Microsoft Excel (Microsoft Office 2013, Redmond, Washington, USA).
The peak torque (Nm) measurements for concentric knee flexion and extension at 60°/s and eccentric knee extension at 60°/s were used to define the dynamic control profile. Concentric H:Q ratio (concentric hamstrings divided by concentric quadriceps) and dynamic control ratios (eccentric hamstrings was divided by the concentric quadriceps) were calculated at angles of 30°, 40° and 50°.
For each data point (angle), the torque value for concentric quadriceps was subtracted from the eccentric hamstrings. Consequently, the ‘angle of crossover’ was identified as the point where the net joint torque was equal to zero.
Nordic hamstring exercise testing
Before the start of season 2, players also performed one set of three maximal repetitions on a device specially designed to measure the Nordic hamstring exercise.14 After completion of the isokinetic test, the players were tested in a kneeling position on a padded board, with both ankles secured immediately above the lateral malleolus by individual ankle braces. These braces were attached to uniaxial load cells (Delphi Measurement, Gold Coast, Australia) with wireless data acquisition capabilities (Mantracourt Electronics, Farringdon, UK). The device has been described previously14 and allows for separate measurements of each limb. The player was instructed to progressively lean forward at the slowest possible speed resisting the movement with both limbs while keeping the trunk and hips in a neutral position and the hands held across the chest. If the force output reached a distinct peak (indicative of maximal eccentric strength), followed by a rapid decline in force that occurred when the player could no longer resist the effects of gravity, a trial was deemed acceptable.
Injury surveillance
All participating QSL teams are provided with medical services by the National Sports Medicine Programme, a department with the Aspetar Orthopaedic and Sports Medicine Hospital. This centralised system with a focal point for the medical care of each club competing in the QSL allowed for standardisation of the ongoing injury surveillance through the Aspetar Injury and Illness Surveillance Programme (AIISP).21
The AIISP includes prospective injury and exposure (minutes of training and match play) recording from all QSL teams. The injury data were collected monthly, with regular communication with the responsible team physician/physiotherapist to encourage timely and accurate reporting. Throughout the 2013 and 2014 season (July to May; 44 weeks), training and match exposure for each team were recorded by the team physician (or lead physiotherapist if no team physician was available). At the conclusion of each season, all the data from the individual clubs were collated into a central database, and discrepancies were identified and followed up at the different clubs to be resolved.
A hamstring injury was defined as acute pain in the posterior thigh that occurred during training or match play and resulted in immediate termination of play and inability to participate in the next training session or match.22 These injuries were confirmed through clinical examination (identifying pain on palpation, pain with isometric contraction and pain with muscle lengthening) by the club medical team. If indicated, the clinical diagnosis was supported by ultrasonography and MRI at the study centre. A recurrent injury was defined as a hamstring injury that occurred in the same limb and within 2 months of the initial injury.23
Statistical analyses
Univariate analyses (independent t-tests) were performed between the limbs of the injured and the uninjured players for the isokinetic strength test, Nordic hamstring exercise test and dynamic control profile. Injured limbs were compared with uninjured limbs among injured players and then to all uninjured limbs among the uninjured players.
Due to the consistency in our sample, the repeated measures performed over the two seasons, as well as the fact that not every player had the same number of measurements (ie, some subjects would have test results including both limbs for both seasons, while other subjects might only have been tested once), SEs would have increased when using general estimating equations in a traditional Cox regression model. Therefore, we performed a univariate Cox regression analysis in STATA (V.11.0, College Station, Texas, USA) using the limb as the unit of analyses, adjusting for player identity as a cluster factor. Exposure was totalled as duration in hours for game and training combined from the start to the end of each season or time to first injury. Variables independently associated with hamstring strain injury were determined from the univariate analyses. A p value of ≤0.05 was considered statistically significant. Effect size, which is the quantitative measure of the strength of an observed occurrence, was calculated and interpreted as small (0.2–0.3), medium (0.5) or large (>0.8).24
Potential risk factors were treated as continuous and categorical variables. In the continuous analyses, all variables with p value ≤0.10 were considered further in a backward stepwise multivariate Cox regression analysis to evaluate potential predictor variables. HRs with 95% CIs are presented with exact p values, and p values of ≤0.05 were considered statistically significant.
For the categorical analyses, the limbs of players were grouped for isokinetic strength, Nordic hamstring exercise and dynamic control profile. The OR and 95% CI were calculated for the groups with the lowest (<1 SD below the mean) and the highest (>1 SD above the mean) values for each variable, respectively, with the intermediate group as the reference group.25
Results
Players
During the two-season study period, 592 elite male soccer players (age 25.8±4.8 years, height 177±7 cm, weight 72.4±9.3 kg, BMI 23.1±2) reported for screening and were considered for isokinetic testing. Players who were unable to perform the test due to injury, did not provide consent or had no exposure data recorded in either season (n=179, age 25.3±4.5 years, height 177±7 cm, weight 73.5±9.8 kg, BMI 23.4±1.8) were excluded from the final analyses. The remaining 413 players performed a total of 1087 isokinetic test procedures (considering both limbs) over the two seasons.
New hamstring strain injuries
Over the two seasons, 413 unique players (68.2% of all QSL players) competed for 544 player seasons (132 players competed both seasons) (figure 1). In total, 66 of the 413 players sustained 69 index hamstring injuries. The three players who had more than one injury were retained in the analyses (none of these injuries met the criteria for reinjury), and all injured players in season 1 had their previous injury status adjusted accordingly in season 2.
Non-strength-related risk factors
There were no differences in height, ethnicity, limb dominance and body composition between injured and uninjured groups (table 1). Previous hamstring injury was reported by 31% of the entire cohort (n=413) with no significant difference between injured and uninjured players. Also in the subgroup of players with injury history based on injury surveillance during the previous season (n=336), a history of previous injury did not represent an increased risk of new hamstring injury.
Characteristics of injured (n=66) and uninjured players (n=347)
Univariate analyses identified age and position as potential risk factors for hamstring injury (table 1). Goalkeepers were significantly less likely to sustain a hamstring injury than defenders, midfielders or forwards. When age was considered as a categorical variable, players in the younger age group (<1 SD below the mean, 18–21 years) had a lower risk of injury than the intermediate age group (table 2). Players who weighed more (>1 SD above the mean, 81.8–104.5 kg) were at lower risk for injury compared with the intermediate weight group (table 2).
Comparison between uninjured and injured players with potential risk factors treated as categorical variables using univariate Cox regression analyses
In the multivariate Cox regression analysis, age (HR 1.07 per 1-year increase in age, 95% CI 1.03 to 1.12) and position (HR 5.79 for outfield players vs goalkeepers, 95% CI 1.44 to 23.32) were retained from the univariate analyses and were significantly associated with hamstring injury risk.
The OR (95% CI) was calculated for the group of players with the lowest (>1 SD below the mean) and the highest (>1 SD above mean) values for each variable, respectively, with the intermediate group of players as reference group.
Strength measurements as potential risk factors
The results of the univariate analyses are shown tables 3 and 4 for isokinetic strength and Nordic hamstring exercise, respectively. Among injured players (n=66), there were no differences in strength between the injured and uninjured limbs.
Univariate comparison of isokinetic strength tests between the injured and the uninjured limb in the injured players, all uninjured limbs in the uninjured players and Cox regression analysis demonstrating parameter estimates (95% CIs) for all isokinetic strength variables when comparing injured to uninjured limbs
Univariate comparison of Nordic hamstring exercise test results between the injured and the uninjured limb in the injured players, all uninjured limbs in the uninjured players and Cox regression analysis demonstrating parameter estimates (95% CIs) for all strength variables included when comparing injured to uninjured limbs. Absolute values and values adjusted for body weight (BW) are shown as mean force values in Newton(N) with SD
Comparing injured limbs (n=69) to the uninjured limbs (n=1018), the parameter estimates of the univariate Cox regression analyses of the isokinetic strength test variables are presented in table 3, expressed as HRs per one-unit (1 Nm/kg) strength change. In the continuous analyses, none of the 11 strength variables were found to be significantly associated with an increased risk of hamstring injury (table 3). The categorical analyses identified the greater strength group (>1 SD above mean, 2.2–3.7 Nm/kg) for quadriceps concentric torque at 300°/s (normalised to bodyweight) as being at increased risk for injury (table 2).
No significant differences were found for any of the Nordic hamstring exercise test variables between injured and uninjured limbs (table 4).
When profiling dynamic control, no difference was observed either in the angle of cross over between the injured limbs (n=56) and uninjured limbs (n=752) (injured limbs: 45°±8° (SD), uninjured limbs: 44°±7°) or in the dynamic control ratio (figure 2).

{kind=link}
{kind=link}
Dynamic control ratio at 30°, 40° and 50° for injured (closed symbols) and uninjured players (open symbols) throughout the test range of motion for the two test modes (concentric and eccentric). Data represent group means with SD.
Discussion
The main finding of this prospective two-season cohort study of 413 football players, the largest to date, was that none of the 24 strength variables examined differed between injured and healthy players. The only exception was that the group with the highest quadriceps concentric torque at 300°/s (>1 SD below the mean) had an increased risk of hamstring injury. Age, body mass and playing position (ie, being a goalkeeper) were associated with injury risk.
Modifiable risk factors
The comparison of the strength measures between the injured and uninjured groups (tables 3 and 4) clearly demonstrate that it is not possible to distinguish between the groups clinically. In the categorical analyses, the greater strength group for concentric quadriceps strength at 300°/s (adjusted for bodyweight) was found to be significant (see table 2). Although our finding of a weak association with quadriceps strength is supported by the meta-analyses performed by Freckleton and Pizzari,5 the small effect size of 0.2 and the fact that there was no group difference in strength indicates that this holds little clinical value. The smallest detectable difference for concentric quadriceps peak torque is reported between 11.9% and 20%,26 27 and therefore, the differences reported in this study are likely equivalent to test–retest variability. Comparison to previous findings is difficult, such as the testing protocol, inclusion criteria, duration of the follow-up period and injury definition. It is, however, more striking that only 1 out of 24 strength variables evaluated (11 isokinetic strength test, 5 Nordic hamstring exercise test and 8 dynamic control profile measures) was weakly associated with an increased risk of hamstring injury.
The Nordic hamstring exercise has received much attention in the literature, and its value as a preventative tool is well established.28 Further investigation has been done to examine the use of this exercise as a test to determine risk of hamstring injury, and initially, no significant association was found between a simple visual assessment of test performance and hamstring injury risk.13 Despite this, a novel device has recently been developed to accurately measure eccentric hamstring strength when performing this exercise.14 Subsequent studies positively identified players with inferior eccentric strength as being at increased risk for hamstring injury,29 30 while Bourne et al31 found no increased risk with lower eccentric strength in rugby union players. These previous studies determined best fit cut-off values for eccentric hamstring strength and assessed the risk of injury based on these in multivariate models. In the present study, we compared eccentric strength in the Nordic hamstring exercise test between injured and uninjured groups and also assessed risk in the group with inferior performance. However, none of the variables related to the Nordic hamstring exercise test were found to be significantly associated with an increased risk of hamstring injury. We do not dispute that the Nordic hamstring exercise may be a useful injury prevention tool.32 33 It may alter the influence of non-modifiable risk factors such as age or previous injury29 or lead to protective muscle architecture adaptations.30 34 However, the present findings urge caution if the clinician attempts to relate the results of a standalone Nordic hamstring exercise test to individual risk for injury.35
The H:Q ratio as conventional and dynamic entities of mixed isokinetic strength has been identified previously as risk factors for hamstring injury,7 8 11 36 with some debate over how these ratios are interpreted. Essentially, we should consider that scaling these data may not appropriately represent the lower and higher end of the range (ie, the slope of the relationship between the two variables is not equal to 1). Furthermore, when we divide two normally distributed variables, the resulting ratio is unlikely to be normally distributed itself.37 Two large previous investigations have reported contradicting results, which make it difficult to determine whether these strength ratios are valuable or not.8 18 Therefore, the dynamic control profile, as described by Graham-Smith et al,16 was also included to explore the relationship between hamstring and quadriceps strength throughout the entire test range of motion.
No association was found between the dynamic H:Q ratios (knee flexion (‘hamstring’) eccentric peak torque at 60°/s to knee extension (‘quadriceps’) concentric peak torque at 300°/s) (table 2), a finding supported by a previous meta-analysis.5 Additionally, there was no difference in the dynamic control profile over the entire range of motion or the angle of crossover. Figure 2 clearly demonstrates that the ratios for both the injured and uninjured players were indistinguishable. Although this dynamic ratio might be considered a valuable tool when interpreting isokinetic strength in previously injured players, it adds little value for the clinician to establish risk of hamstring injury for the individual. Our findings suggest that H:Q ratios in any form are ineffective in risk factor identification.
Mean body mass did not differ between groups, but players with greater body mass (>1 SD above the mean, >82 kg) did have a lower risk for a hamstring injury than the intermediate weight group. However, the absolute difference between the injured and uninjured players was less than 1 kg. This finding is therefore also not clinically useful, and as previously reported,5 13 25 we would not consider body mass as an important risk factor for hamstring injury.
Non-modifiable risk factors
Age has consistently been identified as a risk factor for hamstring injury,5 10 20 25 38 as in the current study, where we observed a 7% increased risk of hamstring injury per year added. The injury risk of the youngest group (<22 years) was 85% less than the intermediate group, while we detected no difference in risk between the intermediate and the oldest groups (table 2). This supports the results of previous studies where fewer hamstring injuries were found in the younger age group.39 Playing positions were retained in the multivariate analyses to investigate whether it might influence age, as goalkeepers were on average 1 year older than the other playing positions combined. It did not, however, change the risk for these players significantly, even though outfielders were five times more likely to get injured compared with goalkeepers.
Surprisingly, a history of previous injury was not found to be associated with risk of hamstring injury, although it is consistently identified as a risk factor in the literature.5 40 This finding was further explored, attempting to reduce the risk of recall bias in self-reporting injuries (or unwillingness to disclose previous injuries), by analysing a subgroup of players where the previous injury status was known through detailed injury surveillance. Again, no significant association was found. In contrast, a retrospective investigation of the same league over previous seasons did identify previous injury as a risk factor.18 To interpret these contrasting results, consider that two large randomised control trials were being conducted at the Aspetar Orthopaedic and Sports Medicine Hospital concurrent with this prospective study.41 Both these studies incorporated a structured criteria-based rehabilitation programme, including a large number of QSL players. The first randomised controlled trial reported a low re-injury rate of 6%23 compared with other football leagues.42 A reduced risk in previously injured players has been reported before43 due to the effect of successful intervention programmes. Our finding suggests a similar effect, where the introduction of systematic criteria-based rehabilitation programmes may have reduced the risk associated with previous injury.
Strengths and limitations
To detect strong to moderate associations in prospective cohort studies, it is suggested that 30–40 injury cases are needed, while for small to moderate associations to be detected, 200 injury cases are needed.17 Importantly, even though this is one of the largest prospective studies to date on risk factors for hamstring injury, we were not able to include enough cases to detect small associations, illustrating the difficulty in performing adequately powered investigations. However, the effect sizes calculated for each strength variable never exceeded 0.3, failing to reach clinical significance.
Intraseason variability in the repeated measures over the 2-year observation period may have limited our ability to identify an association between strength and injury risk. Injury surveillance was carefully monitored during each season; however, we cannot discount that the clinical criteria used to confirm a hamstring injury may have involved other differential diagnoses.
All tests performed used the same isokinetic testing system with highly experienced assessors in a multinational, multilanguage clinical setting for professional athletes. Although every effort was made to ensure players understood the test procedure and instructions, it is possible that some players did not comprehend the instructions fully. However, this reflects a ‘real-world’ scenario, increasing the external validity of the study.
We also acknowledge the homogeneity of our study population of professional male football players, which limits the generalisation of these findings to other sports, age groups or female players. Other factors such as training culture and possible prevention strategies within different teams or climate specific to the Middle East region could have influenced the results.
Clinical implications
It is clear that isolated strength variables, including the new test device for the Nordic hamstring exercise and a more comprehensive interpretation of strength ratios, have limited clinical application in identifying individual players at risk. Our continued pursuit of risk factor identification through performance tests seems incongruous. Muscle strength continues to form part of a multifactorial complex model that may lead to injury. However, our findings should urge the clinician to exercise caution and not translate the results of these commonly used screening tests into risk of injury for the individual player.
Conclusion
None of the other 24 strength-related variables were found to be associated with hamstring injury. Increased concentric quadriceps strength when adjusted for body weight was the only associated with hamstring injury when considered categorically, although the magnitude of this difference is likely too small to be clinically relevant. The use of strength measurements and different strength characteristics in musculoskeletal screening to predict future hamstring injury is unfounded.
What are the findings?
Isolated strength measurements cannot assist the clinician in predicting risk of hamstring injury.
Functional and dynamic measures of isokinetic H:Q ratio are not useful in determining individual risk of injury.
Age and playing position are non-modifiable risk factors associated with an increased risk of hamstring injury.
Population-based risk of injury in previously injured players might be reduced by implementation of criteria based rehabilitation programmes.
How might it impact on clinical practice in the future?
Greater consideration might be given to the use of strength testing and strength ratios in identifying players at risk for hamstring injury.
Muscle strength continues to be identified in the causation of hamstring injury and must be considered in prevention measures.
The small association found with strength highlights again the multifactorial nature of hamstring injury.
References
Footnotes
Contributors ND: principal investigator, data collection and analyses, writing, editing and outline of the manuscript. EW: first principal supervisor of PhD programme, concept and outline as well as writing and editing of the manuscript. RB: second main supervisor, concept and outline as well as writing and editing of the manuscript. AFB: statistical analyses and data analyses, writing of the manuscript. RW: investigator and coauthor, particularly with the data collection and writing of the manuscript. AB: organisation and planning of study, data collection and writing of manuscript. AM: study design and ethical approval, data collection and organisation, and writing of the manuscript. AF: statistical analyses.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional Review Board, Anti-Doping Lab, Qatar.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Patient-level data and/or full data set and/or and/or statistical code are available from the corresponding author.