Article Text

Abstract
Objective To determine whether there is a relationship between physical growth and development, as determined by markers of biological maturation, and musculoskeletal conditions in adolescents.
Design Systematic review.
Data sources Electronic databases (PubMed, EMBASE and the Cumulative Index to Nursing and Allied Health Literature) were searched up to 6 September 2017.
Eligibility criteria for selecting studies Studies that evaluated the association between biological maturation or growth and musculoskeletal conditions in adolescents (chronological age 10–19 years).
Results From 20 361 titles identified by the searches, 511 full-text articles were retrieved and assessed for eligibility; 56 studies, all at high risk of bias, evaluating the relationship between maturation and/or growth and musculoskeletal conditions were included. A total of 208 estimates of association were identified across the included studies, which generally indicated no association or an unclear association between maturation, growth and musculoskeletal conditions.
Summary/Conclusions While the relationship between maturation, growth and musculoskeletal conditions remains plausible, the available evidence is not supportive. The current body of knowledge is at high risk of bias, which impedes our ability to establish whether biological maturity and growth are independent risk factors for musculoskeletal conditions.
- adolescent
- growth
- injuries
- fracture
Statistics from Altmetric.com
Introduction
Adolescence is defined by the WHO as the second decade of life,1 and represents a key period of physical, psychosocial and cognitive development, yet also a period of physical and psychological vulnerability.2 3 Puberty is a physical event that occurs during adolescence characterised by marked somatic growth, and significant musculoskeletal (MSK), physiological and sexual development,4 sometimes considered of itself to define. The prevalence of MSK conditions such as spinal pain increases during adolescence,5 6 and persistent problems in this period predict pain and disability later in life.7–10 Understanding the role of biological development in the onset of MSK conditions in adolescents is important to guide preventative efforts.
Rapid physical growth (ie, ‘the adolescent growth spurt’) and biological maturity (eg, stage of skeletal or pubertal development) have been proposed as risk factors for MSK pain and injury.11 At the anatomical level, the structural capacity of growth plates and developing bone may be exceeded during rapid periods of growth,12 13 leading to pain, injuries, fracture or the development of non-specific MSK conditions. However, there is limited epidemiological evidence to support the hypothesis that rapid growth during adolescence influences the tolerance of growth plates and bones to excessive or repetitive load. It may be that the construct of biological maturity increases risk, underpinned by the physical and neurodevelopmental changes such as motor coordination, cognitive control or negative affect that occur during adolescence, as observed by associations between Tanner staging14 15 and injury rates in adolescent athletes.16 17 In addition to physical growth, puberty is also characterised by numerous hormonal, emotional and neurological changes,4 which may also increase the risk of injury/pain.
Adolescents of the same chronological age can vary significantly in height, weight and pubertal stage. Given the wide variation in speed and timing of maturation and growth, chronological age may be less appropriate as a measure for the prediction of MSK conditions. Instead, longitudinal measures of growth such as height change velocity and cross-sectional measures of maturation such as bone age18 may more accurately capture the constructs relevant to the hypothesis that the pubertal period carries an increased risk of the development of pain and injuries.
While multiple biological, psychological, social and developmental factors may be aetiologically linked with MSK conditions, this systematic review aims to specifically determine whether there is a relationship between physical growth and/or stage of development and MSK conditions in adolescents.
Methods
A protocol for this review19 was registered a priori at the International Prospective Register of Systematic Reviews—PROSPERO 2014:CRD42014014333.
Information sources and search methods
Electronic databases (PubMed, EMBASE and the Cumulative Index to Nursing and Allied Health Literature) were searched for eligible studies from inception to 6 September 2017. The search strategy was developed for PubMed and modified for other databases (online supplementary appendix table 1). The reference lists of all included publications and relevant systematic reviews were checked, and forward citation searches (using the Scopus citation database) were performed. No unpublished studies were identified, nor was contact with experts made.
Supplementary file 1
Eligibility criteria
Studies were considered eligible if they evaluated exposure factors of maturation and/or growth, and the outcome of MSK conditions, in adolescents (recruited within the chronological age range 10–19 years). Prospective, cross-sectional and retrospective studies were eligible for inclusion, while case-series were excluded.
Studies needed to quantitatively measure stage or timing of maturation and/or growth. Measures of biological maturity status, defined as a single measurement in time that assesses where a child is in the continuum of biological maturation, could include status of pubertal development such as Tanner staging, testicular volume (orchidometer) or radiographic analysis of skeletal age. Measures of maturity timing, defined as the chronological age at which specific maturational events occur, could include age at peak height velocity (PHV), age at menarche, estimated percentage of predicted adult height or maturity offsets. Growth rate, defined as change in physical stature within a specific time period, had to be measured longitudinally, for example repeated standing height measurements within a specified period. Measurements of growth spurt were also included, defined as a period of rapid somatic growth. Growth spurt measures were set within a study and could include a priori thresholds for rapid height or weight gain over a specific period, for example 5 cm of height growth in a 6-month period. Anthropometric measurements that did not account for temporal change (ie, growth) and studies that only measured chronological age were excluded.
Our definition of MSK condition was intentionally broad to accommodate non-specific pain (eg, back pain or headache), MSK injuries and fractures. We did not include typically asymptomatic conditions when pain was not an outcome measure, such as scoliosis, benign joint hypermobility, negative ulnar variance and low bone density, or conditions that were incidentally identified on imaging studies. Studies had to provide a measure of the association (eg, ratio (relative) or difference (absolute) measures) between the exposure and MSK condition.
Only full articles published in peer-reviewed journals were included. Studies published in all languages were eligible and translations were sought where necessary.
Study selection and data extraction
Pairs of authors (MSS and SJK, MSS and NH) independently screened all titles and abstracts identified in the searches. Full-text copies of potentially relevant articles were retrieved and evaluated against the eligibility criteria for final inclusion. Disagreements regarding inclusion were resolved by consensus.
One review author (MSS) extracted data from all included studies, and two review authors (NH, SJK) checked the extracted data. Data were extracted using a specifically designed spreadsheet that included study design and characteristics, sample characteristics (participant source, setting, and age and gender distribution), MSK condition (type, definition, assessment method, frequency and/or duration), measures of maturation and/or growth (type, definition and categories), and measures of association such as ORs and CIs. Confounders were extracted where reported, and where multiple measures of association were presented we extracted the most adjusted estimates.
Risk of bias in individual studies
The Quality in Prognosis Studies (QUIPS) tool20 was modified to assess the quality of the included studies by substituting risk factors for prognostic factors. The modified QUIPS tool rated risk of bias in six domains: (1) study participation, (2) study attrition, (3) aetiological factor measurement, (4) outcome measurement, (5) confounding measurement and account, and (6) analysis. The risk of bias tool guide includes a series of statements to direct reviewers to issues that may introduce bias within each of the six domains, for example, ‘whether the source population was adequately described for key characteristics’ within the study participation domain, and ‘whether attempts to collect information on participants who dropped out of the study were described’ within the study attrition domain. A complete list of the guiding statements is described by Hayden et al.20 The risk of bias in each domain was rated as ‘low’, ‘moderate’ and ‘high’. Overall risk of bias for each included study was rated as either low risk or high risk. A low risk of bias study satisfied the following criteria: (1) low risk of bias on domain 2 (study attrition) and domain 5 (study confounding), and (2) low risk of bias on at least four of the six domains. Pairs of reviewers (MSS and SJK, MSS and NH) independently assessed the risk of bias of each included study. Discrepancies were resolved by consensus. The consensus process involved discussion between authors regarding their independent responses to the guiding statements and their impression of the impact of these on the overall risk of bias relevant to each domain.
Synthesis of results
Studies were divided according to type of MSK condition—pain, injury or fracture—as follows:
pain, if the outcome definition specified pain, painful episodes or symptoms pertaining to pain without reference to a specific precipitating injury
injury, if the outcome definition specified injury due to an organised activity or event (usually sport or performance); injuries could include sprains, strains or injuries from single event, or stress fractures or overuse injuries from repeated trauma; studies were not included in this category if the outcome was exclusively fracture
fracture, if the outcome definition specified fracture exclusively.
It was recognised that some studies in category 2 could include participants whose injury included fracture, and that some studies in category 3 could include patients whose fracture was sustained during a sporting event or activity. However, it was assumed that these cases would make up only small proportions in the included studies. Where disagreements among review authors occurred in the categorisation of studies, consensus was reached via discussion. Further details of the outcome definitions within studies are reported in online supplementary appendix table 2.
Supplementary file 2
Associations were grouped separately for maturity and growth. In studies that evaluated pain as the outcome, the associations were grouped by region of pain, for example, back pain, extremity pain and neck pain. Typically, maturity or growth was dichotomised in primary studies; where reported we present ORs that quantify the association between these exposures and outcome. Conclusions were based on data from prospective, longitudinal studies where exposure measurement preceded outcome measurement because this study design provides the most robust estimates of causal association. Studies with cross-sectional and retrospective design were included but given less weight. Where available, gender-specific associations were presented separately. This decision was not prespecified, but taken post hoc due to the way data were reported in the included studies. For studies that evaluated univariate and multivariate associations, the fully adjusted or final model was presented along with all reported covariates. Homogeneity was assessed subjectively based on population, measurement and methodological aspects of the included studies. No quantitative data synthesis (meta-analysis) was performed due to heterogeneous study designs and measures (online supplementary appendix table 2). We performed a narrative synthesis, taking study quality into account. Summary statements were generated as follows: associated (along with direction), no association or unclear. Statistically significant associations were based on primary study findings; the level of significance was typically set at P value <0.05.
Results
Study selection
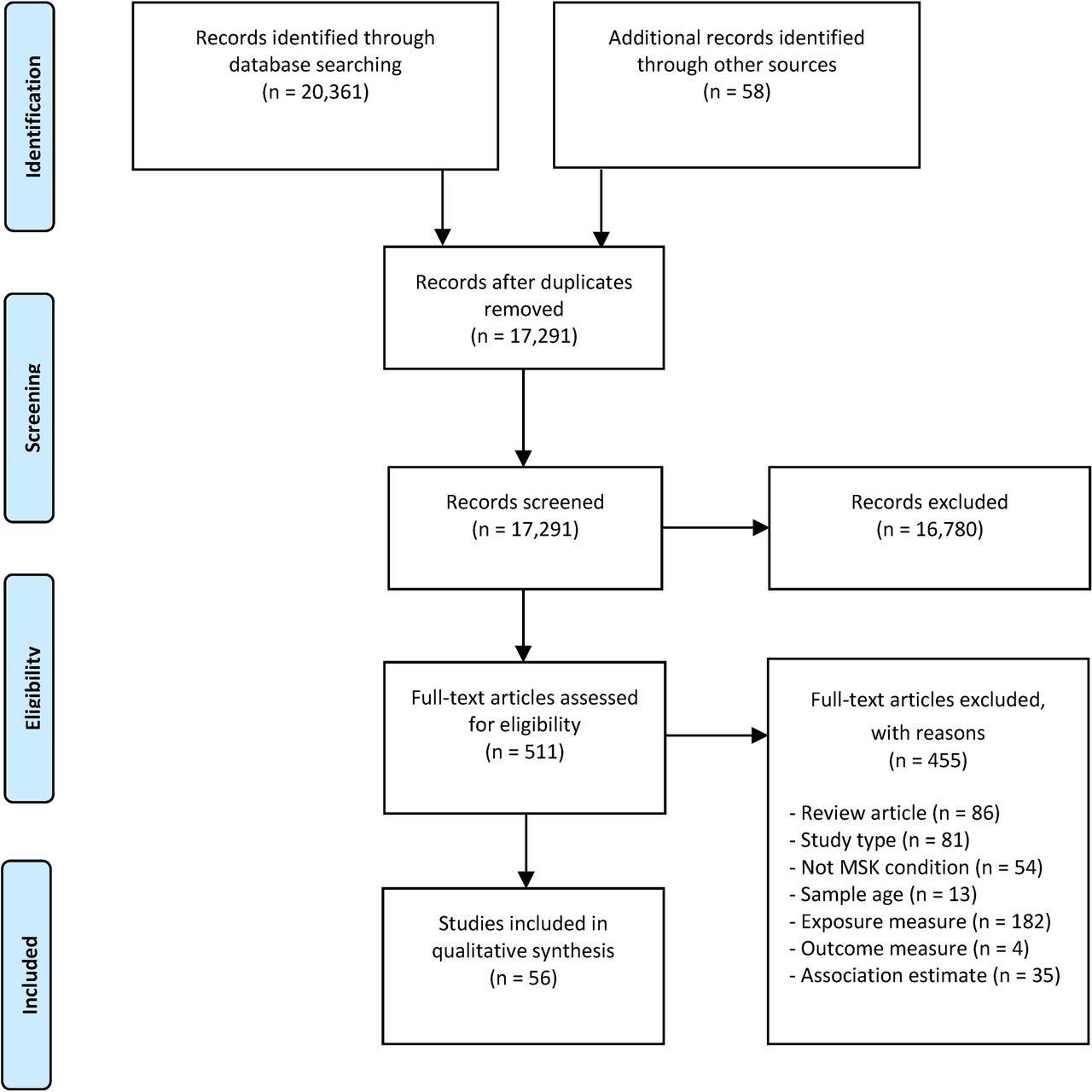
Database searches retrieved 20 361 citations, of which 17 291 remained after duplicates were removed (figure 1). After screening, 511 articles were retrieved in full text, along with 58 articles identified through forward and backward citation tracking. Fifty-six articles were finally included, of which 55 were published in English16 17 21–74 and 1 in Spanish.59
{kind=link}
PRISMA flow diagram of studies through the review. MSK, musculoskeletal; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Description of included studies
Of the 56 included articles, 25 (20 discrete samples) evaluated associations with pain,21–45 22 articles (19 samples) with injury16 17 46–65 and 9 articles (8 samples) with fracture.66–74 Table 1 reports the exposure measures and outcomes, while the study design, sample size, characteristics of participants, measurement of maturation or growth, and measurement of MSK conditions are presented in online supplementary appendix table 2.
Exposure measures and outcomes
Risk of bias assessment
No article adequately addressed all bias domains (online supplementary appendix table 3). High risk of bias was identified in 23 articles for study participation, 35 for study attrition, 10 for aetiological factor measurement, 9 for outcome measure, 27 for study confounding, and 15 for statistical analysis and reporting. Regarding overall study risk of bias, only two studies were at low risk of bias in at least four of the six QUIPS domains; neither study was at low risk in relation to study attrition. Therefore, all included studies were judged to be at high risk of bias.
Supplementary file 3
Associations between biological maturity or growth, and pain
MSK pain
A total of 101 associations (52 longitudinal, 49 cross-sectional) from 21 studies23–32 34–44 evaluated relationships between adolescent development and back, neck or extremity pain, or any report of MSK pain. There were 58 associations between biological maturity (35 status, 23 timing) and MSK pain, and 43 associations between growth (26 rate, 17 spurt) and MSK pain.
Three studies24 30 35 (n=62 970) reported nine longitudinal associations between maturity and back, neck or extremity pain, or any report of MSK pain (online supplementary appendix table 4). Two studies24 30 reported seven associations that indicated increased pain frequency with later maturity, while one study35 reported no association between pain frequency and maturity timing.
Supplementary file 4
Eight studies25 26 29 30 36–38 40 (n=12 212) reported 43 longitudinal associations between growth and back, neck or extremity pain (online supplementary appendix table 4). There were no consistent patterns of association; 3 studies26 29 38 reported 5 associations indicating increased pain with higher rates of growth, and 8 studies25 26 29 30 36–38 40 reported 38 associations indicating no relationship.
Thirteen studies23 27–29 31 32 34 37 39 41–44 (n=44 266) reported 49 cross-sectional associations between maturity and back, neck or extremity pain, or any report of MSK pain (online supplementary appendix table 4). There were no consistent patterns of association.
Head/face or chest pain
A total of 32 associations (9 longitudinal, 23 cross-sectional) from 8 studies21 22 24 28 30 33 39 45 evaluated relationships between adolescent development and head/face or chest pain. All associations were between maturity (21 status, 11 timing) and pain.
Three studies24 30 33 (n=6692) reported nine longitudinal associations between maturity and head/face pain (online supplementary appendix table 4). There was no consistent pattern of association; one study24 reported two associations that indicated increased pain probability with later maturity, and two studies30 33 reported seven associations indicating no relationship.
Six studies21 22 28 34 39 45 (n=25 990) reported 23 cross-sectional associations between maturity and head/face or chest pain (online supplementary appendix table 4). There was no consistent pattern of association.
Associations between biological maturity or growth, and injury
Sporting injuries
A total of 46 associations (40 longitudinal, 5 cross-sectional, 1 retrospective) from 18 studies16 17 46 48–50 52 54–56 58–65 evaluated relationships between adolescent development and sporting injuries (athletic, football, gymnastics, handball, ice hockey and multisport injuries). There were 42 associations between maturity (12 status, 30 timing) and sporting injuries, and 4 between growth (1 rate, 3 spurt) and sporting injuries.
Fourteen studies16 17 46 49 52 54 56 58–61 63–65 (n=3363) reported 36 longitudinal associations between maturity and sporting injuries (online supplementary appendix table 4). There was no consistent pattern of association; 5 studies16 17 49 56 65 reported 5 associations indicating higher injury rates/severity with later maturity/early pubertal timing, 11 studies17 46 54 56 58–61 63–65 reported 26 associations indicating no relationship, and 4 studies52 56 63 64 reported 5 associations indicating higher injury rates/severity with early maturity/late pubertal timing.
Two studies55 59 (n=265) reported four longitudinal associations between growth and sporting injuries (online supplementary appendix table 4). There was no consistent pattern of association; one study55 reported two associations indicating higher football injury rates with growth spurt, and one study59 reported two associations indicating no relationship between handball injury rate and growth spurt.
Three studies48 50 62 (n=772) reported five cross-sectional and one retrospective association between biological maturity and sporting injuries (athletic, gymnastic and organised physical activity injuries) (online supplementary appendix table 4). There was no consistent pattern of association; one study reported three associations indicating higher organised physical activity injury rates with early maturity, two studies50 62 found no association between biological maturity and sporting injury (gymnastics and athletics) frequency, and one study48 reported one association indicating higher organised physical activity injury rates with earlier maturity offset timing.
Ballet injuries
A total of four associations (three longitudinal, one retrospective) from two studies47 53 evaluated relationships between adolescent development and ballet injuries (online supplementary appendix table 4). Both studies (n=334) found no association between adolescent development and ballet injury rate.
Stress fracture
Two studies51 57 (n=12 292) reported two longitudinal associations between maturity (maturity timing) and stress fracture injuries (online supplementary appendix table 4). One study57 reported no relationship, and the other51 reported higher injury rates with late pubertal timing.
Associations between biological maturity or growth, and fracture
A total of 23 associations (3 longitudinal, 20 retrospective) from 9 studies66–74 evaluated relationships between adolescent development and fracture. All associations evaluated aspects of maturity (13 status, 10 timing) and fracture.
Two studies72 74 (n=1654) reported three longitudinal associations between maturity and fracture (online supplementary appendix table 4). There was no consistent pattern of association; one study74 found advanced maturation (both Tanner stage and bone age) was associated with a higher incidence of fracture, and one study72 found no association between age at PHV and fracture.
Seven studies66–71 73 (n=4042) reported 20 retrospective associations between biological maturity and fracture (online supplementary appendix table 4). There were no consistent patterns of association.
Summary of associations
A total of 208 associations were identified. Table 2 provides an overall summary of the associations between biological maturity, growth and MSK conditions.
Associations between maturity, growth and musculoskeletal conditions
Discussion
Despite being a commonly held theory, there is little published empirical evidence that biological maturity and growth in adolescence are associated with MSK conditions. While 56 articles were identified in our searches, there remain knowledge gaps for common conditions. The data that are available provide limited evidence due to high risk of bias in prospective studies and the inherent limitations in studying risk in cross-sectional studies.
A strength of this review was the comprehensive evaluation of both biological maturation and growth as risk factors for specific types of MSK pain, injury and fracture. We separated specific exposures and types of conditions (ie, between factors and effects) to appropriately evaluate studies that propose causality. The ability to conclusively answer our question was constrained by limitations in included studies; these included poor reporting quality, high loss to follow-up, lack of clarity regarding the number of participants providing aetiological and outcome measures, and variable analytical methods.
ORs for the association between maturity status versus back pain ranged from 1.1 to 1.9, which indicates a small risk of advanced maturation.75 ORs were seldom below 0.6 or above 1.6. We presented covariates (when included) alongside estimates of association to assess whether potential confounders such as age, sex and history of MSK disorder were included in study designs and statistical models.76 The included studies generally did a poor job of accounting for potentially confounding factors. For example, of the 208 associations identified, 111 (~53%) were univariate, 157 (~75%) did not account for chronological age, and the factors in the model were unclear in 11 (~5%) of associations. This issue is reflected in the risk of bias domain for study confounding, where three-quarters of studies in this review were deemed at moderate-to-high risk. Regardless, the general lack of strength and consistency of the associations raises doubts about the hypothesised causal relationship between biological maturation and MSK pain and injuries.
Measurement of maturity and growth were generally found to be at moderate-to-high risk of bias. For example, arbitrary thresholds and categories were often set for maturity timing. In one study,35 timing of puberty was measured via questions about age at the time of the first ejaculation (boys) and the first menstruation (girls), and timing of puberty was grouped into three categories: early (12 years or younger for boys and 11 years or younger for girls), average (13 or 14 years for boys and 12 or 13 years for girls) and late (15 years or older for boys and 14 years or older for girls). Other studies used different thresholds for ‘late’ puberty, including menarche at >12 years21 and at ≥15 years.63 Similarly, measurement of growth spurt was commonly categorised as ‘high growth spurt’, arbitrarily defined as >5 cm in a 6-month period (not accounting for baseline height or other factors). The arbitrary cut-point for high-growth spurt in this example may be erroneously high as this growth rate is typically only attained by the top three per cent of adolescents.77 The issue of measurement error (misclassification) also negatively impacts confidence in this body of knowledge. The validity and reliability of self-reported measures of pubertal status and timing have been queried in previous research.78–80 Pubertal assessment by children or their parents may not be reliable and should be augmented by a physical examination.79 Ensuring that measures are valid and reliable, in addition to addressing other sources of bias (such as measurement recall bias), is required before the relationship between biological maturation and MSK conditions can be clarified.
In addition to considerations of reliability and validity of the maturity and growth measures used in included studies, there is also the question of heterogeneity. We decided a priori to separate exposure measures into the broad categories of ‘growth’ and ‘maturity’; this was performed via a process of consensus among the authors. While we contend that this represents a sensible and meaningful division, there was heterogeneity between measures within each category. In the context of our findings, it may be that the lack of consistent direction and magnitude of associations could be partly due to this heterogeneity. We cannot be sure of the importance of the variability between measures, but this provides reason to be somewhat cautious in our conclusions.
Timing of information (temporality) was typically not well considered in studies that evaluated biological maturation as risk factor for adolescent MSK conditions. Per the Bradford-Hill criteria for causal inference,81 the exposure must precede the onset of the disease. Studies in this review seldom established whether participants had a history free of the MSK condition at enrolment; only 8 of the 208 associations adjusted for physical complaints,23 functional somatic syndromes,30 43 previous low back pain43 or fracture history.63 There were studies that measured the exposure after the occurrence of the outcome, and this was particularly common in studies on fracture.66–69 71 73 The timing of maturation and growth events in relation to conditions needs to be properly addressed in future studies that aim to evaluate biological maturation factors for adolescent MSK conditions.
Several previous epidemiological reviews link adolescent growth and development with MSK conditions, such as back pain and sports injuries.11 82–86 A position statement from the American Medical Society for Sports Medicine states that overuse injuries may be more likely during the adolescent growth spurt.87 This has led to the recommendation to monitor adolescent growth rate and limit training workloads during rapid growth periods.87 This recommendation does not appear to be based on robust published research evidence. To date only one other focused review has systematically evaluated puberty specifically as a risk factor for MSK conditions (limited to back pain) in the young.84 The authors concluded that a causal link between puberty and back pain is possible. That review found five studies (all included in the current review) that were all deemed to be of high quality based on their methodological checklist that evaluated study sample, data collection, study factor, outcome measure, modifiers/confounders and biological gradient. In contrast, we deemed all studies to be at high risk of bias based on the QUIPS steering questions. We also applied a consistency threshold of 100% for association, which differed from the previous review of 75%. Like us, the authors of the previous systematic review did not perform meta-analysis due to heterogeneous study designs.
Our review demonstrates that there is considerable uncertainty regarding the aetiological role of maturation and growth in adolescent MSK conditions, and highlights the knowledge gaps. For example, periods of rapid growth have been linked to the onset of traction apophysitis, such as Osgood-Schlatter disease.88 We found only one article that explored this question27; skeletal age and disorders of the knee extensor mechanism were studied in 40 young male soccer players, and no association was found. Perhaps the most biologically plausible relationship is between rapid growth and fracture, given a reduction in cortical bone mineral density occurs as growth increases during early-mid puberty.13 Only two prospective studies attempted to determine whether maturation was associated with fracture in adolescents.72 74 In one study,74 Tanner stage and skeletal age measures were positively associated with a higher hazard of fracture over a 6-year follow-up period, while the other study found no association between age at PHV and fracture.72 Nevertheless, the role of rapid growth in the aetiology of fracture is still to be determined.
Future research should be designed to observe change in individuals over a sufficient period to account for the wide variation in tempo and timing of maturation and growth. Measurements need to be adequately valid and reliable, and frequent enough to capture rapid change. It may be that frequent repeated measurement to ascertain growth velocity in adolescence (while logistically difficult) provides a better measure than measuring the multifactorial construct of maturation. Large samples of adolescents need to be selected to adequately capture the MSK outcomes of interest and appropriate measure taken to minimise attrition. Many of these issues relate back to developing an appropriately clear research question. Researchers must clearly delineate the specific exposure construct of interest in the formulation of their research question, and ensure appropriate covariates are included in the analysis to limit issues with confounding.
Conclusion
Our study did not find clear association between maturation, growth and MSK conditions in adolescents. Clinicians should avoid supposing a causal relationship as studies on the topic report inconsistent findings and are at high risk of bias.
What is already known?
Adolescence is characterised by marked somatic growth, and significant musculoskeletal, physiological and pubertal development.
Musculoskeletal conditions become increasingly prevalent during adolescence and commonly predict pain and disability later in life.
What are the findings?
A meaningful association between biological maturation, growth and musculoskeletal conditions in adolescence is doubtful.
Clinicians should refrain from inferring a causal relationship between maturity, growth and musculoskeletal conditions in adolescents.
The data that are available on this topic provide limited evidence due to high risk of bias.
References
Footnotes
Contributors All authors conceived the study and wrote the study protocol. MSS, NH and SJK selected the studies. MSS extracted the data. NH and SJK checked the extracted data. MSS analysed the data. All authors interpreted the data. MSS wrote the first draft of the manuscript and all authors contributed to the writing of the final version.
Funding CGM’s (APP1103022) and SJK’s research fellowships are funded by Australia’s National Health and Medical Research Council. CGM holds a programme grant funded by Australia’s National Health and Medical Research Council (APP1113532).
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Not commissioned; externally peer reviewed.