Article Text

Abstract
Objectives To assess the efficacy of exercise, orthoses and splinting on function, pain and quality of life (QoL) for the management of mid-portion and insertional Achilles tendinopathy, and to compare different types, applications and modes of delivery within each intervention category.
Design Systematic review and meta-analysis.
Data sources Medline, CINAHL, Embase, AMED, WHO ICTRP, Web of Science, PEDro and Cochrane Library from inception to October 2017. Citation tracking of published studies and conference proceedings and contacting experts in the field.
Study eligibility criteria Controlled clinical trials evaluating either exercise, orthoses or splinting for the management of Achilles tendinopathy.
Methods Independent reviewers undertook searches, screening and risk of bias appraisal. Primary outcomes of interest were function, pain and QoL.
Results Twenty-two studies were included (1137 participants). Moderate level evidence favoured eccentric exercise over control for improving pain and function in mid-portion tendinopathy. Moderate level evidence favoured eccentric exercise over concentric exercise for reducing pain. There was moderate level evidence of no significant difference in pain or function between eccentric exercise and heavy slow resistance exercise. There was low level evidence that eccentric exercise was not superior to stretching for pain or QoL. There was moderate level evidence that a combined exercise protocol was not superior to a lower dosage protocol for improving functional performance. There was moderate to low level evidence of a significant difference in pain (mean difference (MD) 6.3 mm, 95% CI −4.45 to 17.04, moderate) or function (MD 1.83 Victoria Institute of Sport Assessment points, 95% CI −7.47 to 11.12, low) between high-dose and low-dose eccentric training. There was high to moderate level evidence of no difference in pain (moderate) or function (high) between orthoses and control. There was low level evidence of no significant benefit in adding a night splint to an eccentric exercise programme for function, and moderate level evidence for no reduction in pain (MD −3.50, 95% CI −10.49 to 3.48). Eccentric exercise was not superior to splinting for pain (moderate evidence) or function (low level evidence).
Summary We conditionally recommend exercise for improving pain and function in mid-portion Achilles tendinopathy. The balance of evidence did not support recommendation of one type of exercise programme over another. We conditionally recommend against the addition of a splint to an eccentric exercise protocol and we do not recommend the use of orthoses to improve pain and function in Achilles tendinopathy.
- tendinopathy
- exercise
- orthotics
- rehabilitation
- achilles
Statistics from Altmetric.com
Background
Achilles tendinopathy is characterised by progressive pain and decreased function of the Achilles tendon. Presentation and prognosis can vary. In the early stages, pain may be limited to the start and end of exercise activity. As the disorder progresses, pain may become persistent and can interfere with everyday activities.1 The underlying cause of pain is not clear; however, neovascularisation has been proposed as a potential cause.2 Diagnosis is based primarily on clinical history and examination, but is sometimes supplemented with imaging.2
Mid-portion tendinopathy is characterised by pain typically 2 to 7 cm from the tendon’s insertion into the calcaneus and can be accompanied by either diffuse or local swelling. Insertional tendinopathy is defined by pain and localised swelling at the calcaneal attachment and is frequently associated with calcification and ‘bony spurs’, which may be palpable at this site.3 Data on the long-term prognosis of Achilles tendinopathy are sparse, although 84% of individuals reporting with acute or subcacute symptoms returned to full activity following a multimodal treatment programme.4 However, treatment responses vary. Van der Plas et al 5 reported a resolution rate of 40% in a cohort that included elite athletes; 43% also developed symptoms in the contralateral tendon.
Improved understanding of the pathophysiology of tendinopathy (terminology of this Achilles disorder has moved from ‘tendinitis’ and ‘tendinosis’ to tendinopathy) has driven emphasis on exercise-based interventions and alteration of intrinsic risk factors, such as abnormal lower limb biomechanics, using splinting or orthoses. A popular exercise protocol focuses on progressive heavy-load eccentric strengthening exercises, based on Alfredson’s classic heel-drop exercise programme.6 It is thought that eccentric exercise affects type 1 collagen production, increasing tendon volume and tensile strength.7 Eccentric exercise may alter neovascularisation and accompanying nerve ingrowth associated with this condition.2 Flexibility exercise (either static or dynamic) used as part of a treatment programme for Achilles tendinopathy typically aim to improve flexibility around the lower leg complex and increase ankle range of motion (ROM).
Abnormal lower limb biomechanics may increase the risk of excessive or unaccustomed loading of the Achilles tendon. Alterations in the range of motion of the ankle and lower limb biomechanics (eg, excessive pronation or supination of the foot) have been associated with increased risk of tendinopathy.8 Higher calcaneal inversion at heel strike may also be associated with Achilles tendinopathy.9 Increased pronation has been proposed to induce a bowstring effect in the tendon leading to increased load and microtears in the medial tendon. Excessive supination may increase tensile stress on the lateral aspect of the tendon.10 11 Orthoses are proposed to increase rearfoot movement variability resulting in decreased tendon loading. Orthoses, either customised or ‘off the shelf’, are prescribed based on an individual’s foot shape, size and biomechanical abnormality. A key rationale is that orthoses can correct abnormal foot and lower limb biomechanics, and improve neuromuscular adaptations and muscular fatigue.12
Splinting is also frequently prescribed for treating Achilles tendinopathy. The primary aim is to rest the ankle joint in a neutral or dorsiflexed position. For practical reasons, splints are usually provided for use at night. Night splints may reduce swelling and discomfort,13 and may allow lengthening of the muscle, thus reducing strain on the tendon.14
Existing management guidelines include non-randomised trials and diagnostic studies, and they do not incorporate current evidence.15 Exercises, orthoses and splinting are prescribed in various forms and can be applied in a variety of ways. The ideal frequency, intensity, time and specific type of exercise prescription for Achilles tendinopathy is unclear. The most efficacious method and mode of exercise delivery is also unclear. Similar uncertainty applies to the use and type of orthoses and splints.
The focus of this systematic review was to examine interventions that promoted active self-management in individuals with Achilles tendinopathy. We included orthoses and splinting as these interventions involve a ‘one-off’ prescription before incorporation in self-management. Therefore, we aimed to determine the efficacy of exercise, orthoses and splinting in improving function, reducing pain and improving quality of life in the management of Achilles tendinopathy. Second, we aimed to compare different types, applications and modes of delivery of interventions within the three intervention categories.
Methods
The reporting of this study was guided by the Preferred Reporting Items for Systematic Reviews and Meta-analyses recommendations.16 The study protocol was prospectively registered and published with the Cochrane Database of Systematic Reviews17 and is available online (http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD010874/full).
Study eligibility criteria
Randomised controlled trials (RCTs) and quasi-randomised controlled clinical trials evaluating either exercise, orthoses or splinting for treating Achilles tendinopathy were considered for inclusion. Cross-over trials and studies that evaluated a combination of the interventions were also eligible. Studies using within-participant designs in which contralateral limbs acted as controls were excluded. Interventions were compared with no intervention, a placebo intervention or advice to rest, and with each other.
Studies involving participants with a reported diagnosis of Achilles tendinopathy (also described as ‘tendinitis’ or ‘tendinosis’) were included. There were no restrictions placed on recruitment setting, gender, age, duration of symptoms or activity levels of participants. Participants with either mid-portion or insertional tendinopathy (or both) were considered.
We included (1) trials comparing any of the three categories of interventions (exercise, orthoses or splinting) with no intervention or placebo intervention, and (2) trials comparing different types, applications and modes of delivery of interventions within the three intervention categories. The study aimed to examine and compare ‘types’ of exercise (aerobic, strengthening, stretching, ROM and proprioceptive were considered). Studies that included co-interventions (such as drug therapies) were eligible provided these were applied to all participants. ‘Applications’ included comparison of night versus day splints and ‘modes of delivery’ included comparison of supervised versus unsupervised exercise.17
The primary outcomes of interest were (1) functional assessment measures, for example, the Victoria Institute of Sport Assessment–Achilles Questionnaire (VISA-A)18; (2) measures of pain, for example, the Visual Analogue Scale (VAS); and (3) quality of life measures, for example, the 36-Item Short Form Survey (SF-36).19 Secondary outcomes included return to previous level of activity, adverse effects, patient satisfaction, recurrence of symptoms and radiographic findings. In keeping with recommendations of the Cochrane Collaboration,20 and in consultation with the Cochrane Bone, Joint and Muscle Trauma Group,21 where possible, we presented results for the following time periods: short term (0 to 12 weeks) and intermediate/long term (3 to 12 months) and longer term (longer than 12 months).
Sources and study selection
Electronic databases were searched from inception to October 2017. These included the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register, the Cochrane Central Register of Controlled Trials (CENTRAL), the Database of Abstracts of Reviews of Effect (DARE) (the Cochrane Library, 2015 Issue 2), MEDLINE, EMBASE, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Allied and Complementary Medicine (AMED), PEDro and the Web of Science. The WHO International Clinical Trials Registry Platform (WHO ICTRP), the ISRCTN Registry and ClinicalTrials.gov were also searched for ongoing or recently published trials (July 2005 to 17 May 2017). There were no restrictions on language or publication status. All search strategies were completed by a librarian (DM) experienced in the methodology and are summarised in online supplementary material.
Supplementary file 1
Five experts in the field were contacted to access published or unpublished ongoing trials and a further 12 authors were contacted to access further study data. Grey literature searching included searching reference lists of published studies and conference proceedings of the following organisations: American College of Sports Medicine from 2011 to 2017, American Physical Therapy Association from 2012 to 2017, British Association of Sport and Exercise Medicine from 2010 to 2017, British Association of Sport and Exercise Sciences from 2010 to 2017, World Confederation for Physical Therapy from 2012 to 2017 and International Scientific Tendinopathy Symposia Proceedings 2012 to 2017. Two authors were contacted for further information regarding published conference proceedings or published trial registries.22 23
Two review authors (FW and CB) independently screened trials for inclusion based on the titles, keywords and abstracts. Subsequently, full-text manuscripts were independently assessed for eligibility by review authors (FW and CB); disagreements between reviewers were resolved by discussion to achieve consensus or by referral to a third author (DM), if required.
Data extraction and management
Two review authors (FW and CB) extracted data independently using a customised data extraction form. This included details of methods, eligibility criteria, interventions, comparisons, co-interventions and outcome measures. Any disagreements between reviewers were resolved through consensus or third-party adjudication. Study authors were contacted to clarify any study characteristics or omitted data. Some studies included an intervention arm that examined interventions outside of the scope of this review (eg, electrotherapy), and data from these intervention arms were not extracted or included within analyses.
Dichotomous data were reported as risk ratios with 95% CIs. The mean difference (MD) with 95% CI was calculated for continuous data. For continuous data reported using different scoring systems, standardised mean differences were used. In the case of pain-VAS reported in centimetres, data were converted to millimetres using the Cochrane CodFish tool (The Cochrane Collaboration, Oxford, 2014). Included studies must have reported SDs. If SDs were missing for continuous data, other included statistics (eg, 95% CI, standard errors, T values, p values and F values) that allowed for the calculation of SD using the Review Manager (RevMan) V.5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) calculator tool were used. Where studies reported outcomes at multiple time points, data were extracted at clinically relevant time points, for example, short term (0 to 12 weeks; assessed at the end of the 12-week intervention), intermediate/long term (3 to 12 months) and longer term (longer than 12 months).
Data synthesis
When appropriate, results of comparable groups of trials were pooled using a random-effects model. The choice of the model was guided by the extent of heterogeneity of effect size across the pooled studies. Clinical heterogeneity was assessed subjectively based on information about the participants, interventions and outcome measurements of each study. Statistical heterogeneity was further assessed by visual inspection of effect estimate similarities, the overlap of the CIs on the forest plots and consideration of the statistical test output of the χ2 test (p value <0.01 was interpreted as significant heterogeneity) and the I² statistic (I² of 75% to 100% may be interpreted as considerable heterogeneity, as suggested in Higgins and Green20). Where it was inappropriate to pool data, data were presented in tables and synthesised qualitatively. Where data were available, prespecified sensitivity analyses were conducted to explore the impact of using fixed-effect or random-effects analyses for outcomes with statistical heterogeneity and the effects of including data from quasi-randomised trials.
Assessment of risk of bias
After an initial meeting to discuss and align their interpretations of each item, two reviewers (FW and CB) independently assessed the risk of bias in included studies using the Cochrane risk of bias tool.20 Each study was assessed based on the published report (or, if appropriate, based on information from related protocols, published comments or after discussion with the relevant authors) in each of the following domains: sequence generation; allocation concealment; blinding (participants and personnel) and blinding (outcome assessment); incomplete outcome data; selective outcome reporting and other sources of bias (clarity of diagnosis, compliance to intervention and features of study design).
Grading of quality of evidence and strength of recommendations
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the quality of the body of evidence for each of the primary outcomes.24 The quality rating ‘high’ is reserved for a body of evidence based on RCTs. We downgraded the quality rating to ‘moderate’, ‘low ’ or ‘very low ’ depending on the presence and extent of four factors: risk of bias, inconsistency of effect, imprecision and indirectness. The GRADE approach was also used to determine the direction and strength of recommendations.25 26 Four domains contributed to the strength of recommendation: balance between desirable and undesirable outcomes of interest, confidence in magnitude of estimates of effect of the interventions, confidence in values and preferences and variability, and resource use (we assumed that there is a cost associated with orthoses and splints, and that unsupervised exercise programmes are free). This resulted in a strong or conditional recommendation for or against an intervention.
Results
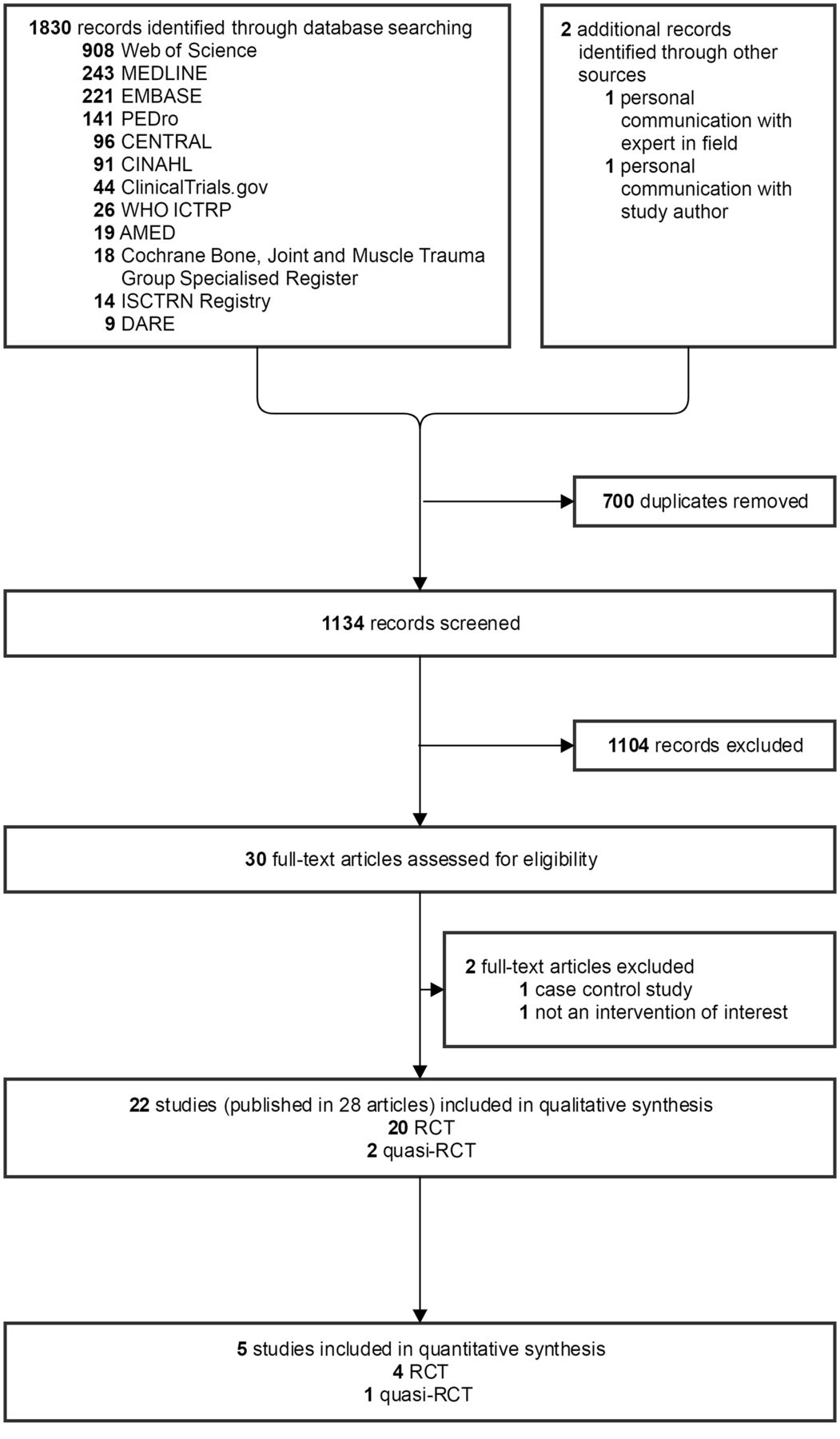
The initial search identified 1134 records for screening (after duplicates were removed). Reasons for excluding studies were not an RCT or quasi-RCT; focus on Achilles tendon ruptures; did not report the outcomes of interest; study duplicate; animal study; did not include the interventions of interest; focus on an intervention for prevention of Achilles tendinopathy. The full texts of 30 articles were assessed for eligibility; two were excluded based on study design. Finally, 22 studies, published in 28 articles, were included. One study published at baseline and two different follow-up points,27 and three other studies published both a conference abstract and a journal paper.28–30 Figure 1 summarises the study selection process.

Preferred Reporting Items for Systematic Reviews and Meta-analyses flow diagram of search strategy and study selection process. RCT, randomised controlled trial.
Characteristics of included studies
Twenty included studies were RCTs. Two trials were quasi-RCTs using alternation for treatment allocation.30 31 Studies included a total of 1137 participants of which 1031 participants (1112 tendons) were included. Study characteristics are described in table 1. Participants were recruited from the general population in all studies other than Horstmann et al 32 and Mayer et al 22 who only examined runners; McAleenan et al 33 reported that 9/11 participants were ‘actively involved in sport’.
Effects of interventions across primary outcomes by comparison, with Grading of Recommendations Assessment, Development and Evaluation strength of evidence and strength of recommendation ratings
There was some variation in specific diagnoses of Achilles tendinopathy with mid-portion and insertional tendinopathy represented in studies. Seventeen studies examined mid-portion tendinopathy.13 14 22 27 28 30–32 34–42 One study examined insertional tendinopathy,29 one study included both diagnoses in the study cohort42 and four studies did not specify the diagnosis.33 43–45 Diagnosis of Achilles tendinopathy was made by study investigators in 14 studies.13 14 22 28 30–32 36 38 41–45 In other studies, an independent clinician determined diagnosis, which was, in some cases, supported by an investigator diagnosis (see online supplementary table 1). In nine studies, diagnosis was made according to prespecified clinical and ultrasound criteria.13 28 34–37 40 42 44 In the remaining studies, participants were diagnosed according to prespecified clinical criteria only.
Supplementary file 2
Exercise interventions
Nineteen studies examined the effect of eccentric exercise.13 14 27–38 41–45 The most common exercise programme was the eccentric loading protocol described by Alfredson et al.6 Three studies examined concentric exercise,35 43 45 and one study examined a stretching programme.44 One study examined a ‘heavy slow resistance’ (HSR) programme (a combined eccentric and concentric regime).34 Two studies implemented a combined exercise protocol including eccentric and concentric strengthening, stretching and power exercises.39 40 One study examined the effect of whole-body vibration training.32 All exercises were demonstrated in a clinic setting initially and performed by all participants at home except for Yu et al,45 Tumilty et al 41 and Horstmann et al,32 which were based in a clinic only. Eleven of the studies measured intervention adherence using training diaries,14 27 28 30 31 34 38–40 43 44 and three studies monitored adherence in a clinic setting.32 41 45 Eight studies reported levels of adherence.14 27 28 31 32 34 38 41 All studies are described in online supplementary table 1.
Orthoses
Two studies explored the effects of orthoses, with both studies prescribing individually fitted semirigid insoles.22 28 No studies comparing different types, applications and modes of delivery of orthoses were identified (see online supplementary table 1).
Splints
Five studies examined the efficacy of splints prescribed in addition to eccentric exercise programmes. Two studies used a splint for daytime use13 36 and the remaining three studies used a night splint to be worn continuously all night.14 27 33 No studies comparing different types, applications and modes of delivery of splints were identified (see online supplementary table 1).
Comparison of types, applications and modes of delivery
A number of studies compared types of exercise interventions (see online supplementary table 1). However, heterogeneity of studies precluded subgroup comparison of mode of delivery and applications.
Risk of bias in included studies
The risk of bias of included studies is summarised by domain for all studies in figure 2 (see online supplementary figure 1 for summary by study). Frequently, assessments included an ‘unclear’ judgement; this often reflected a lack of information on which to judge the item and could not be clarified by attempts to contact the authors. Outcome data were incomplete in four studies that were classed as ‘high risk’ for this domain.14 39 40 44 Two studies provided evidence of a protocol published a priori and were thus judged as ‘low risk’ of bias for the domain of reporting bias; all other studies were judged as ‘unclear risk’ for reporting bias.28 41
Supplementary file 3

Summary of risk of bias of included studies.
Random sequence generation (selection bias)
Studies that were at ‘low risk’ of bias in this domain demonstrated randomisation either by a computer-generated randomisation list or similar method. Eight studies provided inadequate detail and were assigned ‘unclear’. Two studies randomised by sequential allocation on presenting to the study and were judged as being ‘high risk’ of bias for this domain.30 31
Allocation concealment (selection bias)
There were no studies judged as ‘high risk’ for this domain. Nineteen were judged as ‘unclear’ as they lacked detail regarding safeguarding in their methods and provided an investigator-led diagnosis. Two studies were judged as ‘low risk’ for this domain.37 40
Blinding of participants and personnel (performance bias)
Twenty-one studies were judged as having an ‘unclear’ risk of bias for this domain. It is not possible to blind participants to an exercise intervention, but it is unclear if this introduces bias. One study blinded participants and personnel to the intervention and was judged as ‘low risk’ of performance bias.28
Blinding of outcome assessment (detection bias)
Nine studies were judged as being at ‘unclear’ risk of detection bias due to lack of details in reporting blinding of outcome assessment. Nine studies that demonstrated that outcome assessment was performed by a researcher blinded to allocation were judged as ‘low risk’. Four studies were judged as ‘high risk’ of bias as outcome assessment was performed by the lead researcher who was not blinded to allocation.27 36 44 45
Incomplete outcome data (attrition bias)
Sixteen studies were judged as ‘low risk’ of bias. Two studies were judged as ‘unclear’ due to lack of reporting detail. Four studies were judged as ‘high risk’ of attrition bias due to high loss to follow-up and inconsistencies across time points.14 39 40 44
Selective reporting (reporting bias)
Two studies published a protocol prior to the study and were judged as ‘low risk’ of reporting bias as all data were reported according to protocol.28 41 Twenty studies were judged as ‘unclear’ risk of bias as it was not possible to determine if all data were presented.
Other bias
A ‘high’ risk of bias for other sources of bias was ascribed to four studies that pooled unilateral and bilateral symptoms,27 36 39 40 and two studies that combed tendinopathy subtypes.32 42 Studies were regarded as having an ‘unclear’ risk of bias for other sources due to participants being prescribed orthoses prior to the study entry,43 and participants being told that the intervention ‘would improve their symptoms’.44 The remaining studies were regarded as ‘low risk’ of bias for other sources.
Effects of interventions on primary outcomes
Quantitative meta-analysis of pooled studies was limited due to the heterogeneity of participants, interventions, outcome measures and assessment times. Intervention effects are reported below in terms of intervention and its relationship to specific outcomes of interest. Table 1 summarises between-group comparisons across the primary outcomes of function (VISA-A, SF-36, functional performance, Foot and Ankle Outcome Scale (FAOS)), pain (VAS, 4-point Likert, Pain Disability Index (PDI), FAOS) and quality of life (SF-36, 4-point Likert) at key time points. Meta-analysis was performed on a small number of interventions where there were sufficient studies that could be pooled. These were higher versus lower dosage eccentric exercise for the outcomes of function (VISA-A) and pain (VAS); splinting plus eccentric exercise versus eccentric exercise for FAOS pain and symptoms scores.
Comparison 1: eccentric exercise versus no exercise therapy, placebo therapy or advice to rest
Self-reported pain using VAS was the most commonly reported outcome.29 32 37 42 Studies were not pooled due to substantial heterogeneity (I2=94%) and because different tendinopathy subtypes were examined. Knobloch et al,42 in a study including active participants with either insertional or mid-portion tendinopathies, reported that eccentric exercise significantly reduced pain during peak exercise (VAS) compared with controls after 12 weeks. Kedia et al 29 found that eccentric exercise did not have a significant effect on reducing pain compared with controls; this was the only study to examine insertional tendinopathy only. Horstmann et al 32 found that eccentric exercise interventions significantly reduced pain on tendon palpation compared with controls. In the longer term (4 months), Rompe et al 37 demonstrated a significant improvement in pain scores favouring the exercise intervention.
Two studies examined function (measured at 12 weeks and 4 months using VISA-A) and demonstrated a significant effect favouring the eccentric exercise interventions (see table 1).31 37 Both of these studies had co-interventions; Herrington and McCulloch31 included deep frictions and ultrasound and Rompe et al 37 included drug therapies and thus were not pooled. Quality of life was no different between groups at 12 weeks, based on results from a single study.29 Only two studies reported adherence; Herrington and McCulloch31 reported ‘100%’ adherence to the protocol by all participants and Horstmann et al 32 reported that the eccentric exercise cohort completed three exercise sessions per week.
The strength of evidence for all studies was ‘moderate’ for reducing pain (VAS), improving function (assessed by VISA-A) and improving quality of life (SF-36), downgraded due to imprecision. We conditionally recommend eccentric exercise over no therapy for improving pain and function in mid-portion Achilles tendinopathy.
Comparison 2: exercise protocols
Three studies compared the effects of eccentric exercise (based on the programme described by Alfredson et al 6 and concentric exercise protocols.35 43 45 Mafi et al 35 reported that pain on activity was significantly better following eccentric training compared with concentric training (p<0.002). Niesen-Vertommen et al 43 reported a significant difference in the decrease in pain ratings at 12 weeks favouring eccentric exercise (p<0.01). Yu et al 45 reported that pain improved significantly more in the eccentric exercise group than the concentric exercise group (see table 1). The strength of evidence for this study was ‘moderate’ for reducing pain (VAS), downgraded due to imprecision.
Beyer et al 34 compared a HSR protocol with an eccentric exercise protocol and found that both programmes demonstrated a significant improvement in pain and function at 12 weeks and at 52-week follow-up but reported no significant between-group differences at either time point. Adherence in the eccentric exercise cohort was reported at 78% and in the HSR group at 92%. The strength of evidence for this study was ‘moderate’ for reducing pain and improving function, downgraded due to imprecision.
One study compared eccentric exercise with a stretching protocol44; both groups demonstrated a significant improvement, but no significant between-group differences were observed in pain or quality of life at 12 weeks. The strength of evidence for this study was ‘low’ due to risk of bias and imprecision.
Three studies compared eccentric exercise (based on the programme described by Alfredson et al 6) with programmes of lower frequency and intensity.30 38 41 There was no difference in VISA-A (see figure 3) and pain VAS between dosage protocols (see table 1).38 41 As heterogeneity was 62% for the VISA-A outcome, a sensitivity analysis was performed. Removing a quasi-RCT30 reduced I2 to 0% and the MD to −6.22 (95% CI −11.37 to −1.07), thus favouring the lower dosage protocol. Two of these studies reported adherence; Stevens and Tan38 reported that the ‘do as tolerated’ group performed a mean of 112 exercise repetitions per day compared with 166 repetitions in the Alfredson protocol group. Tumilty et al 41 reported that the higher dose group reported a mean (SD) of 103.7 (48.6) completed exercise sessions at 12 weeks (54% of training logs returned); the lower dosage group reported a mean of 24.8 (10.8) completed sessions (74% of training logs returned). The strength of evidence for these studies was classed as ‘low’ for improving function (VISA-A), downgraded due to inconsistency and imprecision; it was classed as ‘moderate’ for reducing pain (VAS), downgraded due to imprecision.

{kind=link}
{kind=link}
{kind=link}
Comparison of 12-week functional outcomes measured by Victoria Institute of Sport Assessment–Achilles (0–100) questionnaire between high intensity eccentric exercise (Alfredson protocol) and lower intensity eccentric exercise protocols.
Silbernagel et al 39 examined a combined protocol of eccentric, concentric, power and stretching exercise in a high dosage programme (where pain was allowed) compared with a lower dosage programme (which was pain free). No significant between-group differences in functional measures (plantar flexion measurement, a vertical jump test and a toe raise test) were observed at either 12 weeks or 6 months. Pain (reported during activity) was not significantly different between the groups at 12 weeks; however, at 6 months, there was a Risk Ratio of 3.33 (95% CI 1.03 to 10.79) in favour of the lower dosage protocol. The strength of evidence for this study was classed as ‘moderate’, downgraded due to imprecision.
One study compared a supervised eccentric exercise programme with a supervised whole-body vibration training protocol.32 No significant between-group differences in pain on tendon palpation (VAS) were reported at 12 weeks. The strength of evidence for this study was classed as ‘moderate’, downgraded due to imprecision.
The current balance of evidence does not support a clear recommendation of one type of exercise protocol over another for Achilles tendinopathy.
Comparison 3: orthoses versus no orthoses or placebo therapy
The effects of individually fitted semirigid insoles were investigated in two studies.22 28 Mayer et al 22 reported no significant difference in pain measured on the PDI compared with no intervention. The strength of evidence for this study was classed as ‘moderate’, downgraded due to imprecision. In the study by Munteanu et al,28 participants were prescribed custom-made orthoses or ‘sham’ orthoses, in addition to an eccentric exercise programme; adherence was 57% in the exercise programme and 48–58 hours of wear per week of the orthoses. No significant between-group differences in function were reported at 12 weeks or 12 months of follow-up. The strength of evidence for this study was classed as ‘high’.
There was moderate strength of evidence showing treatment effects comparable with placebo or no intervention, and there are costs associated with orthoses. We give a conditional recommendation against the use of orthoses to improve pain or function in mid-portion Achilles tendinopathy.
Comparison 4: splinting plus eccentric exercise versus eccentric exercise only
Five studies examined the effect of combining splinting with an eccentric exercise programme (when compared with eccentric exercise only); two studies used a splint for daytime use,13 36 and three studies used a night splint to be worn continuously all night.14 27 33 Two studies assessing function with the VISA-A at 12 weeks demonstrated no significant differences between groups; the level of evidence was judged as ‘low’ due to risk of bias and imprecision; one of these studies33 did not state what type of tendinopathy was examined and the other27 examined mid-portion tendinopathy and thus studies were not pooled. In the longer term, De Vos et al 27 found no significant between-group differences (eccentric exercise plus night splint vs eccentric exercise only) at 12 months and 5 years5 46; the strength of evidence for these studies were judged as ‘low’ due to risk of bias and imprecision.
Pain was evaluated using a VAS,13 36 and in two studies using the FAOS symptoms and pain scales.13 14 No significant between-group differences in pain were reported on any of these measures. The strength of evidence for these studies was judged as ‘moderate’, downgraded due to imprecision. One study used the ‘physical functioning’ domain of the SF-36 as an outcome and reported no significant differences in outcome between groups; the strength of evidence for this study was judged as low due to risk of bias and imprecision.36
Only two studies that examined splinting and exercise reported adherence. De Vos et al 27 reported ‘good’ adherence in 72% of participants for the eccentric exercise only group and at 74% for the exercise plus splint cohort. Roos et al 14 reported ‘greater than 75%’ adherence to exercise and splint use for the first 12 weeks of the study but only 50% adherence to exercise after 12 weeks (splint use remained at 75%).
There was low to moderate strength of evidence showing treatment effects comparable with exercise alone, and there are costs associated with splinting. We give a conditional recommendation against the addition of a splint to an exercise protocol for improving pain or function in Achilles tendinopathy.
Comparison 5: eccentric exercise versus splinting
Two studies compared eccentric exercise to splinting.14 36 Roos et al 14 reported no significant differences between treatment approaches at 12 weeks and 12 months in FAOS domains of pain, symptoms, activities of daily living (ADL) and sport; the strength of this evidence was judged as ‘moderate’ due to imprecision. Petersen et al 36 reported no significant differences in physical functioning (SF-36) at 12 weeks; the strength of evidence from this study was judged as ‘low’ due to risk of bias and imprecision.
There was low to moderate strength of evidence showing comparable treatment effects, positive effects of eccentric exercise described in comparison 1, a conditional recommendation against splinting described in comparison 4, and there are costs associated with splinting relative. We conditionally recommend eccentric exercise over splinting for improving pain or function in mid-portion Achilles tendinopathy.
Secondary outcomes
Mafi et al 35 measured patient satisfaction and reported an RR of 2.25 (95% CI 1.25 to 4.05) in favour of eccentric exercise compared with concentric exercises. Horstmann et al 32 reported no significant differences in ultrasound images of tendons following a supervised eccentric exercise programme compared with whole-body vibration training or a wait-and-see approach. This study also found that at 12 weeks, eccentric exercise significantly reduced self-reported impact of pain on running and social activities (VAS) compared with controls; there were no significant differences between groups in self-reported impact of pain on other functional activities (impact on family life, recreation or other physical activities). Munteanu et al 28 reported no significant differences between prescription of orthoses and control groups in physical activity, self-reported perception of effectiveness and frequency of adverse events. Similarly, in comparisons of exercise programmes and splinting protocols, no significant differences in effect were reported for ‘sport’, ‘quality of life’ or ‘ADL’ scales in the FAOS.13 14
Discussion
The objective of this systematic review was to determine the efficacy of exercise, orthoses and splinting in improving function, reducing pain and improving quality of life in the management of Achilles tendinopathy. Overall, there was significant heterogeneity and a ‘moderate’ strength of evidence for these interventions.
The eccentric loading programme originally described by Alfredson et al,6 characterised by high dosage and requiring good adherence, formed the basis of the majority of interventions in this review. Compared with controls, such protocols improved function by 18.0 and 20.6 points on the VISA-A measure.31 37 This MD was higher than the minimal clinically important difference for VISA-A (15 points38) and may be clinically meaningful. However, caution should be applied to interpretation of findings from these two studies since both included co-interventions. Herrington and McCulloch31 included deep frictions and ultrasound to both intervention and control groups, and Rompe et al 37 allowed both groups to use paracetamol and non-steroidal anti-inflammatory drugs for pain relief. Therefore, it is not possible to confirm that outcomes were solely resultant from the exercise interventions.
Results of pain outcomes were less clear, with study findings differing depending on the tendinopathy subtype examined. Two studies including both mid-portion and insertional tendinopathies reported that eccentric exercise significantly reduced pain in the short term (12 weeks) compared with controls.32 42 In the longer term, exercise also reduced pain.37 Thus, there is a significant effect of eccentric exercise in reducing pain scores at both the short and long term in mixed tendinopathy. Kedia et al 29 examined insertional tendinopathies only and reported no significant difference at 12 weeks. While these results suggest that eccentric exercise may have a different effect depending on tendinopathy subtype, further investigation is needed. There was no significant effect for the quality of life or radiology outcomes.
In addition to the high volume of exercise required in the classic eccentric loading protocol, programmes are characterised by their encouragement of individuals to push through pain. Subsequently, a number of studies trialled interventions of lower dosage and intensity, and compared these with the traditional Alfredson protocol. There were no significant differences in VAS and VISA-A scores.
Studies comparing eccentric exercise programmes with other exercise programmes demonstrated varying differences in pain, function or quality of life although the majority showed no significant difference between exercise types. Three studies compared an eccentric exercise programme with a concentric programme, and eccentric protocols had greater effectiveness compared with concentric protocols. As so many studies lacked clarity regarding whether concentric loading was completely avoided during eccentric programmes, it is possible that many eccentric programmes did contain some concentric work. When eccentric exercise was compared with a HSR programme that combined eccentric and concentric work, there was an equally positive response when the programmes were compared, but no significant difference between them. A single study by Norregard et al 44 found no evidence that an eccentric programme was superior to a stretching programme. As the early stages of the Alfredson programme is so similar to a simple stretching programme, this may provide an explanation. Mixed interventions in one study only (eccentric, concentric, stretching and power exercises) showed no significant differences in pain or function outcomes compared with lower intensity programmes or active rest.39
No studies that examined the role of splinting in managing Achilles tendinopathy compared splinting with a no-intervention control group, so it is not possible to evaluate the effect of splinting alone. The addition of splinting to exercise programmes did not result in significantly different effects compared with exercise alone. In light of this evidence, and given the costs associated with splinting, we conditionally recommend against splinting for improving pain or function in Achilles tendinopathy. There was a lack of evidence to recommend orthoses in the management of mid-portion Achilles tendinopathy. The studies included in this review did not demonstrate any significant benefit of orthoses over control approaches in pain or function. The addition of orthoses to eccentric exercise did not significantly improve outcomes compared with exercise alone.
As with exercise interventions, an important factor to consider in examining orthoses or splinting interventions is the tendinopathy subtype. The most common type of Achilles tendinopathy is mid-portion, and insertional tendinopathy is considered differently as it is challenging to treat because of a different injury mechanism.3 Some studies did not state what type of tendinopathy participants had, and this information could not be provided by the author when contacted.33 43–45 One study42 included participants with both types of tendinopathy but did not report subgroup results separately. Only Kedia et al 29 examined insertional tendinopathies, and this cohort in particular requires further study.
Studies reported a variety of chronicity of symptoms varying from 1 to 180 months; six studies did not report exact time periods, other than inclusion criteria requiring symptoms lasting more than 3 months (see table 1). It is likely that there will be variation in response to interventions, depending on symptom chronicity. No study accounted for chronicity, and due to heterogeneity of studies, it was not possible for this review to do so (with subgroup analysis). Further research is required to examine response to interventions based on length and history of symptom duration.
We aimed to compare types, applications and modes of delivery of all interventions. However, due to the small number of heterogeneous studies, this objective was only fulfilled in comparing exercise types. Even within this comparison, few studies examined exercise types other than eccentric strengthening, limiting conclusions and recommendations. There is a need for more studies comparing types, applications and modes of delivery, particularly in the use of splinting and orthoses, before their efficacy is established.
Comparisons with other reviews
A difference between this review and others on the topic was the inclusion of studies that reported bilateral symptoms. This meant the limb, rather than the participant, was the unit of analysis. This point was specifically made by Munteanu et al 28 who noted that for those with bilateral symptoms, only data from the most painful side would be recorded and analysed to satisfy the assumption of independent data.47 There is a risk for bias when including such studies. We accounted for bias by assigning ‘high risk’ to these studies for the ‘other source of bias’ domain. There is a risk that patients with bilateral problems may have greater disability (poorer function) and perhaps pain. None of these studies were pooled for meta-analysis.
Previous reviews reported strong evidence for eccentric loading exercises (including the Alfredson protocol).48 49 However, studies included in these reviews were often not RCTs and a number involved co-interventions. The lack of a control group in non-RCT studies as well as co-intervention inclusion is likely to overstate the treatment effect of the eccentric exercise protocol. Sussmilch-Leitch et al 50 supported the use of eccentric exercise (no data were pooled for effect size), but of the eight studies supporting this finding, five were excluded from our review because of methodological limitations. Furthermore, a number of studies in the review compared eccentric exercise with a ‘control’ group performing concentric exercise; our review is the first to present this separately. Since the review by Sussmilch-Leitch et al 50 was published in 2012, seven more studies have been published that met the eligibility of this current review. A review by Scott et al 51 concluded that there is ‘weak evidence’ to support the use of foot orthoses, splinting or bracing in managing Achilles tendinopathy. This was in agreement with our review. More recently, Malliaras et al 52 examined tendinopathy loading programmes with focus on mechanistic outcomes (such as torque measures) and did not examine patient report measures.
Thus, this current review is the first to present evidence from only RCTs (or quasi-RCTs) using clinical, patient-centred outcomes as measures. It explores all types of exercise whereas previous reviews have focused on eccentric exercise. It uses gold standard risk of bias and quality measures, and presents evidence appropriate for self-management of Achilles tendinopathy.
Implications for clinical practice and further research
There is a strong argument for more research into using exercise in the management of Achilles tendinopathy. Current research is dominated by the use of eccentric programmes with a lack of studies examining other types of interventions. This is likely a reflection of clinical practice where there is great emphasis on eccentric programmes based on the protocol first published by Alfredson et al.6 Our results suggest there is evidence that this type of programme is superior to some other conservative interventions for improvement in function and reduction of pain. However, studies that used function as an outcome measure were confounded by the use of co-interventions and should be interpreted with caution. While overall, the balance of evidence did not support a recommendation of an ideal exercise protocol, there is some evidence that eccentric exercise may be superior to concentric exercise. Although, not significantly different to HSR, stretching or combined protocols. There were no differences between high dose and a low dose interventions, suggesting that clinicians may reduce adherence burden by prescribing a lower dose protocol.
There is a need for research examining a variety of exercise programmes beyond eccentric loading to clarify which exercise mode is most effective. Future studies need to be sufficiently homogeneous in terms of participant profiles, degree of chronicity, subtype of tendinopathy (insertional or mid-portion) and use of key (valid and reliable) outcome measures to facilitate meta-analysis. Adherence should be objectively measured where possible and clearly reported, particularly when programmes of different dosages are compared.
In general, studies in this review were underpowered and at considerable risk of biases across a number of domains. Only two studies performed an a priori sample size calculation and one of these examined a smaller sample size than required. Exercise protocols frequently lacked sufficient detail for the reader to replicate the programme. Although central to the efficacy of exercise interventions, compliance was infrequently measured and rarely reported. The paucity of studies at present supports a strong need for RCTs examining orthoses and splinting; the few studies in this review suggested that there may be potential benefit, but further investigation is needed.
Limitations of this review
The type of tendinopathy examined is an important factor to consider in examining both exercise and orthoses or splinting interventions. Some studies included in our review did not state what type of tendinopathy participants had, and this information could not be provided by authors. Some studies had co-interventions that are likely to confound results. Our protocol stated that these would be included as long as they were applied to both intervention and control groups. The influence of co-interventions should be considered when interpreting findings as they are likely to overestimate the effects of the primary intervention. Multiple primary outcomes were selected for this review. This was decided at the protocol stage as a reflection of the diversity of outcomes used in tendinopathy studies. Specifically, VISA-A was reported as a measure of function; although it records self-report functional capacity, it also collects information regarding pain. There was a paucity of reporting of objective functional measures and future studies should include such. Studies included in this review examined an active/recreational population, and findings may not apply to other population groups such as elite athletes or inactive people.
We aimed to examine interventions focused on ‘self-management’ of Achilles tendinopathy (exercise, orthoses and splinting) rather than externally applied, passive interventions (such as electrotherapy). However, some interventions that could reasonably be included in ‘self-management’ (such as education, graded activity/rest and cryotherapy) were excluded from the scope of this review.
Conclusions
We conditionally recommend exercise in improving pain and function in mid-portion Achilles tendinopathy. Some studies support the use of eccentric loading protocols in improving outcomes compared with other exercise programmes, but the balance of evidence did not support recommendation of one type of exercise programme over another. We conditionally recommend against the addition of a splint to an eccentric exercise protocol, and we do not recommend the use of orthoses to improve pain and function in Achilles tendinopathy.
What is already known on this topic?
Exercise is a popular management strategy for Achilles tendinopathy.
Eccentric strengthening programmes are a popular approach to treatment, but there is a lack of consensus if this is the most efficacious approach.
Splinting and orthoses may be useful in managing Achilles tendinopathy, but there is a need to explore optimal prescription and to examine efficacy.
What are the findings?
There is a strong emphasis in research towards using eccentric loading exercise protocols in the management of Achilles tendinopathy.
There has been a greater emphasis only in recent years on exploring other exercise interventions.
There is moderate quality evidence that exercise is efficacious in reducing pain and improving function in the management of Achilles tendinopathy, but the optimal mode of exercise remains unclear.
While a number of exercise-based intervention have significant positive effects on pain and function in Achilles tendinopathy, the current evidence does not support the recommendation of one type of exercise programme over another.
On the balance of evidence, splinting or orthoses are conditionally recommended against in the management of Achilles tendinopathy.
References
Footnotes
Contributors FW conducted the literature search, extracted and analysed data, synthesised findings and constructed the manuscript. MW and CB assisted in data extraction, analysis and synthesis and contributed to the final manuscript. DM constructed and executed searches. KB advised on statistical analysis and TO’D constructed and edited the manuscript.
Funding This review was supported by the National Institute for Health Research via Cochrane Infrastructure funding to the Cochrane Bone, Joint and Muscle Trauma Group.
Disclaimer The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.