Article Text

Abstract
Objective To describe the criteria used to guide clinical decision-making regarding when a patient is ready to return to running (RTR) after ACL reconstruction.
Design Scoping review.
Data sources The MEDLINE (PubMed), EMBASE, Web of Science, PEDro, SPORTDiscus and Cochrane Library electronic databases. We also screened the reference lists of included studies and conducted forward citation tracking.
Eligibility criteria for selecting studies Reported at least one criterion for permitting adult patients with primary ACL reconstruction to commence running postoperatively.
Results 201 studies fulfilled the inclusion criteria and reported 205 time-based criteria for RTR. The median time from when RTR was permitted was 12 postoperative weeks (IQR=3.3, range 5–39 weeks). Fewer than one in five studies used additional clinical, strength or performance-based criteria for decision-making regarding RTR. Aside from time, the most frequently reported criteria for RTR were: full knee range of motion or >95% of the non-injured knee plus no pain or pain <2 on visual analogue scale; isometric extensor limb symmetry index (LSI)>70% plus extensor and flexor LSI>70%; and hop test LSI>70%.
Conclusions Fewer than one in five studies reported clinical, strength or performance-based criteria for RTR even though best evidence recommends performance-based criteria combined with time-based criteria to commence running activities following ACL reconstruction.
- anterior cruciate ligament
- running
- review
- knee surgery
Statistics from Altmetric.com
Introduction
After ACL reconstruction,1–3 an important milestone is returning to running (RTR). The RTR is a key to the participation element of the return to sport continuum (figure 1).2 Running places relatively low demands on the knee.4 However, RTR marks the beginning of the transition from impairment-focused tasks in early rehabilitation (eg, knee range of motion (RoM) exercises, isometric quadriceps strengthening) to the functional, sport-specific tasks that characterise more advanced rehabilitation (eg, sprinting, pivoting, cutting).5 6

Examples of the three elements of the return to sport (RTS) continuum from Ardern et al 2 in the specific context of ACL reconstruction.
There is a lack of information regarding when the patient can RTR following ACL reconstruction. Steady progress through high-quality rehabilitation influences functional outcomes,7 and premature return to sport increases the risk for reinjury.8 Conversely, delayed progress may hinder motivation and psychological readiness to return to sport.9
Therefore, the aims of this scoping review were: (1) to describe the criteria used in clinical decision-making for RTR after ACL reconstruction; (2) to report how these criteria have changed over time alongside changes in surgical and rehabilitation approaches; and (3) to provide information to help clinicians and patients make quality decisions regarding returning to running after ACL reconstruction.
Methods
We conducted a scoping review because this approach is superior to a systematic review for addressing an exploratory research question.10 11 Systematic reviews aim to facilitate synthesis of a known field of research to answer questions regarding the effectiveness of a specific intervention for a particular problem. In contrast, scoping reviews map key concepts, types of evidence and gaps in the research in a particular field. As for a systematic review, a scoping review involves systematically searching, selecting and synthesising research evidence.11 We followed the methodological framework proposed by Arksey and O’Malley10 and the Joanna Briggs Institute12 when conducting and reporting this scoping review.
Our research question was: ‘Which criteria are used to determine when the patient can return to running following primary ACL reconstruction?’
We limited our scoping review to primary ACL reconstruction because the outcomes of revision surgery are typically inferior to the outcomes of primary surgery.13 14
Selection criteria
To select articles for inclusion in this scoping review, the following criteria were employed:
Type of studies
We included: sources of information as recommended in the manual ‘Methodology for JBI Scoping Reviews’12 (including primary research studies, reviews, systematic reviews, scoping reviews, meta-analyses, guidelines, rehabilitation protocol, cases series, clinical commentaries and technical notes) dealing with human subjects, with a rehabilitation programme reported or including criteria for progression to running or jogging.
Only studies published in English language were included. This restriction was based on findings from systematic reviews suggesting no evidence of bias for conventional medicine if studies written in languages other than English were excluded.15 16
We excluded: conference abstracts, opinion pieces, magazine and newspaper articles.
Types of participants
We included: studies of skeletally mature patients or people performing physically demanding work with primary ACL reconstruction (autograft, with or without meniscus surgery).
We excluded: studies of patients with knee dislocation, patients undergoing revision ACL reconstruction and studies including only patients who were more than 40 years old at the index ACL reconstruction (middle-aged patients with joint trauma may be more likely to have knee osteoarthritis,17 18 and this may influence the contents and progression of rehabilitation).
Types of interventions
We excluded: studies of patients undergoing ACL reconstruction plus major concomitant procedures (eg, articular cartilage surgery, posterior cruciate ligament surgery, lateral or medial collateral ligament surgery). One reason for choosing an allograft is the reduced donor site morbidity compared with autograft harvest.19 Reduced donor site morbidity may mean that rehabilitation milestones may be different (accelerated) compared with milestones for patients who choose an autograft. Therefore, it is possible that the time criterion for RTR might be different for patients who had an allograft. Excluding studies in which allografts were the sole graft option reduced the potential clinical heterogeneity in the included studies. In addition, since most patients have ACL reconstruction using an autograft,20 21 excluding allografts reduced the clinical heterogeneity in the results of our scoping review.
Types of outcomes
We included: clinical outcomes or description of RTR criteria: criteria defined by timeline, questionnaires, impairment assessments, isometric or isokinetic strength assessment, or performance-based assessments.
Study selection
Our search strategy involved a three-step approach22:
Step 1: initial limited search
We conducted a pilot search (in October 2016) in the MEDLINE and SPORTDiscus electronic databases using the terms ‘anterior cruciate ligament’ AND ‘reconstruction’ AND ‘run’ (online supplementary file A).
Supplementary file 1
Step 2: identify keywords and index terms
We analysed the title, abstract and index terms used to describe the studies identified in step 1 to identify appropriate keywords for inclusion in the final search strategy (online supplementary file B).
Supplementary file 2
Step 3: execution of final search strategy and further searching of references and citations
In November 2016, we searched the MEDLINE (PubMed), EMBASE, Web of Science, PEDro, SPORTDiscus and The Cochrane Library electronic databases using the search strategy we had developed. We also screened the reference lists of included studies, the reference lists of key systematic reviews and narrative reviews, and conducted forward citation tracking using Google Scholar in order to identify any potentially relevant studies that may have been missed in the electronic database search.
All articles were downloaded to the Covidence reference management platform (Covidence, http://www.covidence.org), cross-referenced and any duplicates deleted before the selection criteria were applied. Two independent reviewers (AJMR and PE) first screened articles for eligibility based on the title and abstract (figure 1). Then, the full text was screened for inclusion in the scoping review by the same reviewers independently. Any discrepancies were resolved during a consensus meeting. A third reviewer was available if needed, but was not required.
Data extraction
Two reviewers (AJMR and PE) independently extracted data based on the following eight categories:
Authors and year of publication.
Origin (country in which the study was conducted).
Aim(s) of the study.
Study population (age, sex) and sample size (if applicable).
ACL reconstruction surgical technique (arthroscopy or open surgery, graft type).
Rehabilitation protocol: postoperative immobilisation (protective) or no postoperative immobilisation (contemporary).
Time-based criterion (weeks) from when patients were permitted to commence running activity (jogging or running on a treadmill, jogging or running on the field).
Other criteria: questionnaire-based or assessment-based criterion or criteria to allow the patient to commence running or jogging (eg, clinical assessment, isometric strength assessment, isokinetic strength assessment, functional goal-based assessment (performance-based assessment)).
To define if a rehabilitation protocol was protective or contemporary,23 we made a judgement based on the early rehabilitation phase: Protective rehabilitation protocols were characterised by a period of postoperative time where knee RoM was controlled (eg, with a cast), non-weightbearing or only toe-touch weightbearing and avoidance of active quadriceps in terminal extension.24 25 Contemporary rehabilitation protocols were characterised by no restrictions on mobilisation,25–27 encouragement of full active knee extension RoM, quadriceps activation and early weightbearing.
Assessment of risk of bias
Since we made a descriptive analysis of variables representing choice and habits of the authors of included studies and not the results of an intervention administered to a population, we contend that our descriptive summary is unlikely to be adversely influenced by the internal validity of included studies. Therefore, we did not evaluate the internal validity of included studies.
Data management
Data were summarised and tabulated according to the eight data extraction categories (online supplementary file C). Qualitative variables were described by number (n) and percentage (%). As there is no consensus in the terms used to describe RTR, and given the variety of terms found in the pilot search, time-based criteria were described by median and IQR to ensure that results were not influenced by outliers. If a study compared two protocols with different time-based criteria or other criteria, all criteria were included in the summary. If a study reported the time to RTR, the median or the average was included in the analysis. We also assessed if there was a change over time in the time-based criterion by using a non-linear Local Regression with 95% CI (span=0.75, two degrees of polynomials). To be as exhaustive as possible, we retained open and arthroscopic surgical procedures and all rehabilitation approaches (dichotomised as protective or contemporary rehabilitation). Medians and IQR were calculated for the four groups (open surgery, arthroscopic surgery, protective rehabilitation and contemporary rehabilitation). Analyses were performed using the software R (http://www.R-project.org).
Supplementary file 3
Results
The flow chart of study selection is detailed in figure 2 (lists of excluded articles are presented in online supplementary files D and E). We selected and included 201 studies in our scoping review (figure 2).
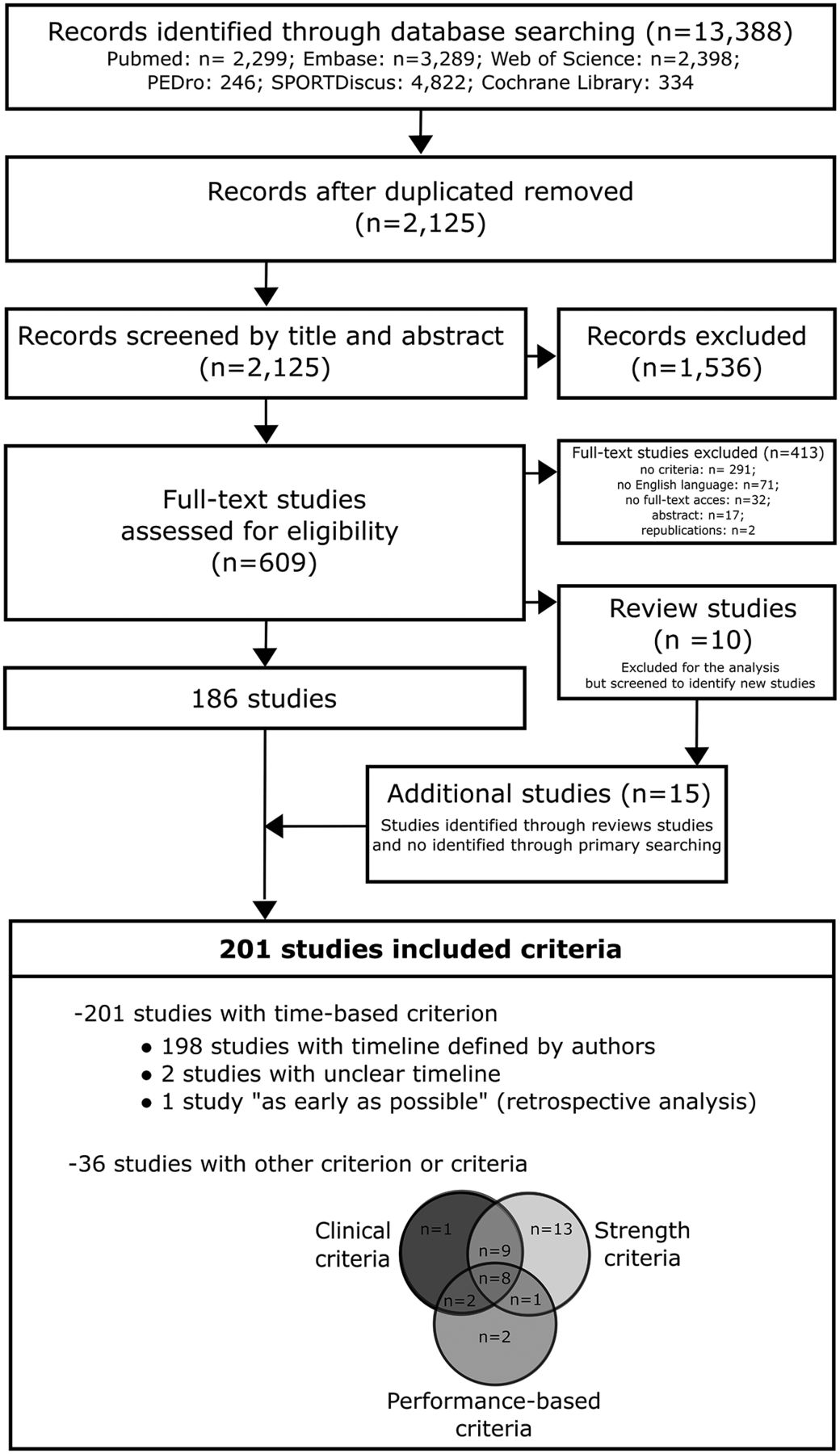
Flow chart of the study selection process.
Time-based criteria used to clear the patient to RTR following ACL reconstruction
Among the 201 studies reporting information on time-based criteria, 198 (99%) reported in the methods or in the rehabilitation programme a time from which RTR was permitted, 2 studies (1%) were unclear5 28 and 1 study made a retrospective analysis of the timeline.29 Since 13 studies included two groups with a different timeline, a total of 212 timelines were included in the statistical analysis.
The median time from which RTR was permitted was 12 postoperative weeks (IQR=3.3, range 5–39 weeks) (figure 3A). The criteria used over time are presented in figure 3B with the non-linear regression curve and the 95% CI.

Distribution of time to permit return to running (RTR) (A) and timelines over the years (B) (n=212) from studies included in the scoping review (n=198), with non-linear regression and CI (95%) representing the time-based criteria trend of the authors during recent years.
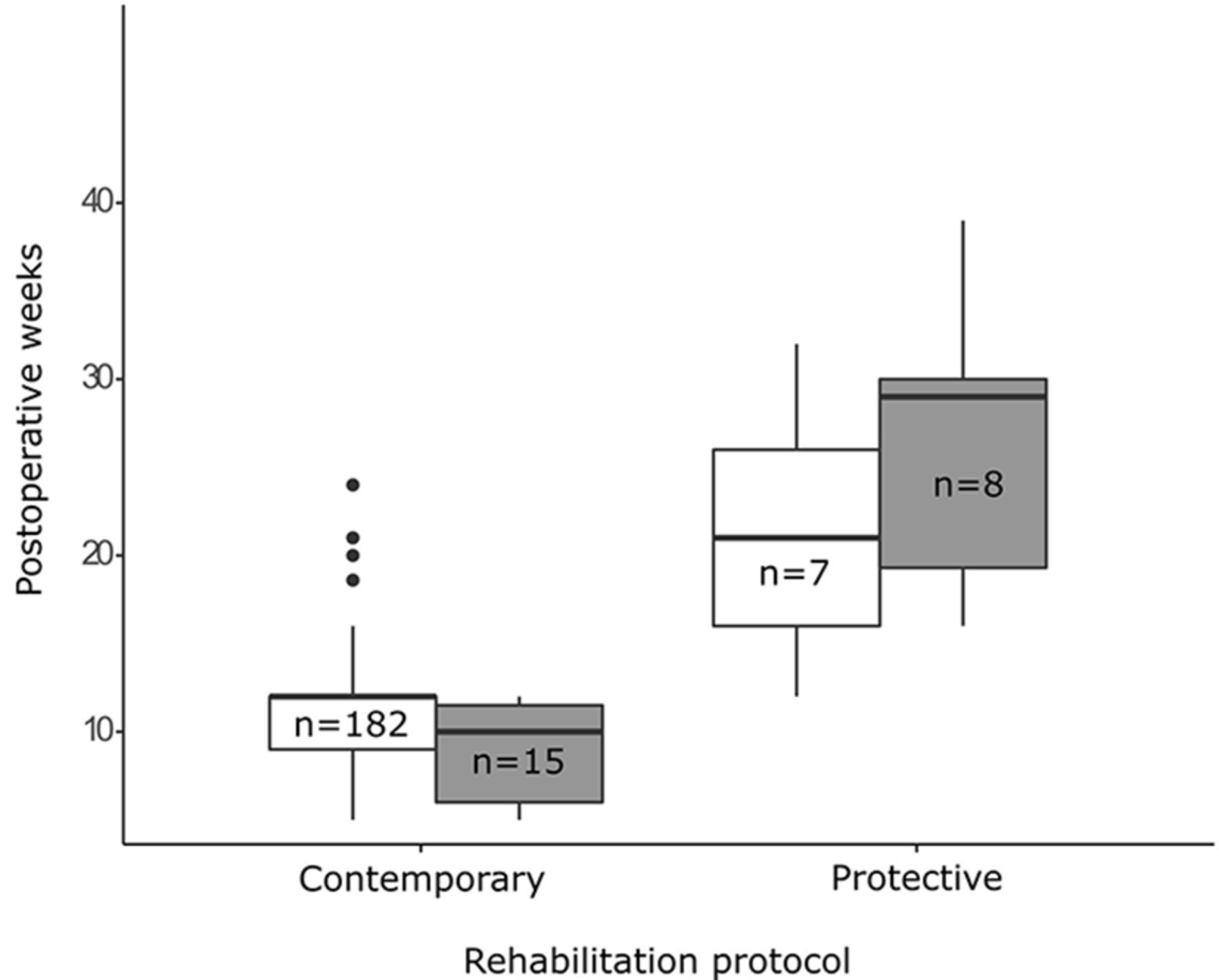
In the subgroup ‘open surgery plus protective rehabilitation’, the median time for RTR was 29 weeks (IQR=10.7 weeks). For the ‘arthroscopic surgery plus protected rehabilitation’ subgroup, the median time for RTR was 21.0 weeks (IQR=10.0 weeks). There was no difference in the median time for RTR between open surgery and arthroscopic surgery when a contemporary rehabilitation protocol was employed (open surgery plus contemporary rehabilitation: 10 weeks, IQR=3.3 weeks; arthroscopic surgery plus contemporary rehabilitation: 12 weeks, IQR=3.0 weeks) (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box plot of the distribution of timeline of the two types of surgery (open surgery represented by grey boxes, arthroscopic surgery represented by white boxes) with the type of protocol of rehabilitation, including the number (n) with reported timelines for each group.
Assessment-based criteria for decision-making for RTR following ACL reconstruction
Thirty-six studies (18% of 201) reported using specific criteria to clear patients to RTR after ACL reconstruction. Sixteen studies (8% of 201) reported using a single criterion (clinical, strength or performance-based criterion), 12 studies (6% of 201) reported using two types of criteria and eight studies (4% of 201) reported using all three types of criteria (figure 2).
Clinical criteria and questionnaires
Twenty studies (10% of 201) reported using clinical criteria (table 1). The most common criteria were: knee flexion RoM (n=14), knee effusion (n=10) and pain (n=10). The most quantifiable and reproducible criteria used were full knee RoM or RoM greater than 95% of the non-injured knee (n=10), and pain <2 on visual analogue scale (n=9).
Clinical criteria and questionnaire scores used for return to running
Strength criteria
Thirty studies (15% of 201) reported using strength criteria. Eleven used an isometric test criterion, 11 used an isokinetic test criterion and two used isometric and isokinetic test criteria (table 2).27 30 The most common objective criteria were isometric quadriceps limb symmetry index (LSI; calculated by dividing the operated limb score by the non-operated limb score) >80% (n=3) and isokinetic quadriceps and hamstrings LSI>70% (n=4) (table 2).
Strength criteria used for return to running
Performance-based criteria
Thirteen studies (6% of 201) reported using performance-based criteria: balance criteria (n=6), normal gait pattern during walking or jog-in-place (n=5), or functional tests (n=7) (table 3). The objective criteria used were proprioception LSI of 100%, composite score on Y-balance test >90%, functional test LSI>70%, hop test LSI>85%, and two combined tests as 10 consecutive single-leg squats to 45° knee flexion without loss of balance, and 30 step-up-and-holds without loss of balance or excessive motion outside of the sagittal plane (table 3).
Performance-based criteria used for the return to running
Discussion
In this scoping review that included 201 articles, time was the most frequently reported criterion for clearing patients to RTR after primary ACL reconstruction. The median time for clearance to RTR was 12 postoperative weeks (IQR=3.3, range 5–39 weeks). The time criterion for RTR has changed over the years mirroring changes in rehabilitation approaches. Fewer than one in five studies reported clinical, strength or performance-based criteria for RTR, the most frequently reported being: full knee RoM or >95% of the non-injured knee; pain <2 on visual analogue scale; isometric lower limb strength LSI>70%; isokinetic quadriceps and hamstring strength LSI>70%; and hop test LSI>70%.
Time-based criteria for RTR must respect biological healing of the ACL graft
All included studies used at least a time-based criterion for RTR after ACL reconstruction. The median was 12 weeks (IQR=3.25), although there were three arbitrary time points reported in 65% of included studies (figure 3A): 8 weeks (11% of included studies), 12 weeks (42% of included studies) and 16 weeks (12% of included studies).
These three arbitrary time points might reflect different rehabilitation goals. Early RTR (ie, around 8 postoperative weeks) might reflect a focus on early return to sport. In contrast, late RTR (ie, around 16 postoperative weeks) might reflect a focus on protecting the healing ACL graft.
While our understanding of graft healing timelines in humans is limited,31 the ACL graft may undergo substantial change in mechanical properties during the period from 8 to 16 postoperative weeks.31 32 There is also wide variation in strength and functional recovery during this time.33–35 Therefore, there are likely different risks to the ACL graft and different capacities among patients to resume running. Collectively, these facts underscore the need for high-quality individualised rehabilitation and decision-making regarding rehabilitation progression—there is no one-size-fits-all recipe.36
Clinical criteria are important indicators of adequate loading when returning to running
Fewer than one in every five studies included in this scoping review reported information regarding assessment-based criteria (ie, clinical tests, strength tests, performance tests) used to guide decision-making regarding RTR. This might suggest that many authors consider time a sufficient sole criterion for RTR. On the other hand, it might also suggest there are few reliable and valid criteria for RTR. Only one in every 10 studies reported clinical criteria—the most frequently reported were knee RoM, effusion and pain. Current evidence-based rehabilitation guidelines for ACL reconstruction37 recommend patients have no effusion, active knee extension RoM of at least 0° and normalised gait pattern to progress from early impairment-based rehabilitation to the second phase (heavy strength training, neuromuscular training and sport-specific training). It is possible that abnormal clinical examination was considered a contraindication to commence running (and simply not reported in the published article), and this might explain why there was a low proportion of studies citing clinical criteria for RTR.
We suggest that these clinical criteria: pain <2 on visual analogue scale,24 28 38–45 95% knee flexion RoM,28 38–40 46–51 full extension RoM (0° knee extension),39–42 47 50 no effusion/trace of effusion,6 24 28 39–41 43–45 49 should be used as ‘non-negotiable’ clinical milestones for RTR—patients must fulfil these criteria before RTR as a way to ensure adequate loading. The knee must have sufficient capacity, first to cope with the demands of activities of daily living and rehabilitation, before commencing higher level functional tasks including running. Therefore, a symptomatic knee (that may be characterised by an increase in pain, effusion and RoM restrictions) after walking, strengthening and/or sensorimotor control exercises suggests inferior load management. In this case, delaying RTR is appropriate, irrespective of the postoperative time.
Strength and performance-based criteria are relevant parameters to judge the patient’s capacity to RTR
Strength was the most frequently reported category of RTR criteria (n=31, 16%). Since the hamstring and quadriceps have an important role in the active stabilisation of the knee52 and in motor control strategy,53 it seems reasonable to include strength criteria in RTR decision-making. Adequate quadriceps strength and hamstrings strength are also important criteria for safe return to sport decision-making.51 52 The most frequent recommendations for the strength evaluation for RTR were: (1) isometric assessment: an LSI of lower limb >70%26–28 54 and quadriceps LSI>80%6 34 47 50; (2) for isokinetic assessment: quadriceps and hamstrings LSI>70%.25 27 55 56
Only 17 articles (7%) used performance-based criteria for clearance to RTR, despite the fact that running represents a functional progression from the impairments that early rehabilitation focuses on addressing.2 57 58 Equally, despite the fact that adequate postural control and normal gait pattern are important precursors for RTR,28 34 41 43 44 47 50 59 60 there was no assessment of gait reported in the included articles. For example, walking with a gait deviation might suggest inferior load management, and alert the clinician that the patient may not be ready to RTR.
Functional tests replicating some of the physical requirements for running may include hop tests performed with a controlled and balanced landing.46 59 61 62 Other functional tests, such as single-limb squats at 45° knee flexion, performed without loss of balance and without dynamic knee valgus, or step-up-and-holds,34 may also be appropriate tests for determining whether the patient is ready to RTR. These tests, described with precise instructions about the quality of the knee flexion (without knee valgus), are simple tests, require little equipment and have the advantage of doubling as rehabilitation exercises. Balance tests that aim to assess aspects of movement quality (eg, Y-balance test and modified Star Excursion Balance Test)34 may also provide information regarding movement control that is relevant for RTR, and complements the other tests mentioned previously.
Quality of movement performance is equally as important as quantity, and performance-based tests allow the clinician to assess both aspects. This information is useful for decision-making regarding RTR, and for further progressions during rehabilitation (eg, commencing sport-specific training). Therefore, it seems reasonable to suggest that quality decision-making regarding functional progressions in rehabilitation (including RTR) should be individualised and based on a test battery comprising multiple criteria including function, strength and time.37 Frequent functional testing, using a range of different tests, that starts early in the rehabilitation process, characterises high-quality rehabilitation.36 This information provides important feedback to the clinician that can be subsequently used to target specific deficits and make changes, as necessary, in a timely way. Clinicians are not clairvoyants—without regular assessment, it is impossible to know whether the planned rehabilitation is high quality and appropriate for the individual patient.
We suggest that the clinician consider for strength and performance-based criteria: hamstring LSI and quadriceps LSI>70% evaluated by isometric assessments, and hop test LSI>70%. The addition of a single-leg squat or step-up assessment performed without increase in knee valgus may also be considered. Further research is needed to help guide the clinician regarding which combination of strength and performance-based criteria should be used to assess whether the patient is ready to RTR.
Brace or no brace to RTR?
Only six of the 201 included studies63–68 compared outcomes between patients who did and did not wear a brace during postoperative rehabilitation. In five of these studies, RTR was permitted at the same time for all patients, irrespective of whether they wore a brace or not (7 weeks,63 12 weeks64 65 68 or 16 weeks66 postoperative). In one study, patients who did not wear a brace during postoperative rehabilitation commenced running earlier than patients who wore a brace (10 weeks vs 12 weeks).67 However, it is important to note that these timelines for RTR were reported as part of the rehabilitation programme, not as a result of a statistical comparison. This suggests the time criteria reported reflected clinical decision-making by the respective researchers. We hypothesise that postoperative bracing does not influence RTR. However, a randomised controlled trial is necessary to test this hypothesis.
When is it safe to RTR?
Unsurprisingly, we found that the time criterion for RTR was different depending whether a protective or contemporary rehabilitation protocol was employed. With contemporary rehabilitation, patients were permitted to commence running earlier than in protective programmes (where there was a period of postoperative immobilisation). This suggests RTR is—at least to some degree—tied to expectations of underlying physical capacity to meet the demands of running. Few studies used multiple criteria in addition to the time criterion for RTR, suggesting that there is no standard assessment for this key step in the return to sport continuum.
A missing piece of information is whether RTR at a median 12 weeks postoperative is safe. It is unclear how many patients had exacerbations of symptoms, or sustained new knee injuries. This information is important to guide clinical expectations and adequate loading for the individual. To answer the question ‘Is RTR at a median 12 postoperative weeks safe?’, research designs that incorporate physical activity/rehabilitation exposure, objective assessments (clinical, strength and performance based) and injury (either new acute injuries or gradual-onset injuries) registration are needed.
Methodological considerations
In line with scoping review methodology, we did not impose date limits on our search or article inclusion. Therefore, we have included articles where surgical and rehabilitation approaches may be different from contemporary clinical practice. We felt it was important to cover the breadth of clinical practice, including how practice has changed over time. We accounted for this in our descriptive synthesis by differentiating between the surgical techniques (open surgery vs arthroscopic surgery) and the rehabilitation protocols (protective vs contemporary rehabilitation protocols).
Differences in how studies defined RTR could influence our results. Not all authors used the same terms to describe the running activity (eg, running, jogging, slow running, and so on). The use of the term ‘running’ may have different meanings in different articles, and a conceptual definition of a specific term to describe the resumption of running may be important for future research. We propose the term return-to-running activities to describe the phase of RTR at a slow speed (8–10 km/hour), but it may be relevant to establish consensus on the definition of the term ‘running’. Since authors report general criteria that governed rehabilitation progression, our analysis of the time-based criteria reflects a general time frame, instead of the precise time each patient was permitted to RTR in each study.
One study reported a rehabilitation protocol that included using restricted body weight progression to running.69 New technologies (eg, anti gravity treadmill) may provide the clinician with alternative ways to progressively increase loading during RTR. These technologies might have merit in facilitating adequate loading that enables the patient to commence running earlier. However, it is unclear whether these approaches translate to earlier progression through rehabilitation, and this might be an avenue for future research.
Clinical implications
RTR decision-making should be individualised for each patient. No universal timeline to RTR exists. For many patients, it might be reasonable to expect readiness to RTR around the 8th–16th postoperative weeks, provided there is adequate loading: pain <2 on visual analogue scale, 95% knee flexion RoM, full knee extension RoM and no effusion. The clinician may choose to use a battery of tests for individualised clinical decision-making regarding RTR including (1) strength tests, (2) qualitative performance-based assessments, with focus on dynamic knee control, and (3) quantitative performance-based assessments such as hop tests. However, it is unclear whether these time-based and assessment-based criteria relate to safe RTR.
Conclusion
In this scoping review including 201 studies from 1981 to 2016, time was the most frequently reported criterion for RTR and fewer than one in five studies reported clinical, strength or performance-based criteria for RTR. It seems reasonable to recommend performance-based criteria combined with time-based criteria to commence running activities following ACL reconstruction.
What are the new findings?
Only one in five studies reported clinical, strength or performance-based criteria for return to running (RTR).
The most cited time-based criterion for RTR was 12 postoperative weeks.
An approach combining assessment goal-based criteria with time-based criteria is a reasonable approach for RTR after ACL reconstruction.
Supplementary file 4
Supplementary file 5
Acknowledgments
The authors acknowledge and thank Thomas Davergne for his contribution to the help in the searches in the database.
References
Footnotes
Contributors All authors have contributed to the development of the research questions and study design. AJMR, PE and JPR identified the method of the scoping protocol. AJMR and PE developed and conducted the search strategy and data extraction. All authors developed the first and subsequent drafts of the manuscript. All authors reviewed and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been updated since it was published Online First. The title has been corrected in order to fix a grammatical error.