Article Text

Abstract
Mass participation endurance sports events are popular but a large number of participants are older and may be at risk of medical complications during events. Medical encounters (defined fully in the statement) include those traditionally considered ‘musculoskeletal’ (eg, strains) and those due to ‘illness’ (eg, cardiac, respiratory, endocrine). The rate of sudden death during mass endurance events (running, cycling and triathlon) is between 0.4 and 3.3 per 100 000 entrants. The rate of other serious medical encounters (eg, exertional heat stroke, hyponatraemia) is rarely reported; in runners it can be up to 100 times higher than that of sudden death, that is, between 16 and 155 per 100 000 race entrants. This consensus statement has two goals. It (1) defines terms for injury and illness-related medical encounters, severity and timing of medical encounters, and diagnostic categories of medical encounters, and (2) describes the methods for recording data at mass participation endurance sports events and reporting results to authorities and for publication. This unifying consensus statement will allow data from various events to be compared and aggregated. This will inform athlete/patient management, and thus make endurance events safer.
- sport
- endurance
- medical encounters
- epidemiology
- methodology
- running
- cycling
- swimming
- triathlon
- illness
- injury
- SAFER
Statistics from Altmetric.com
- sport
- endurance
- medical encounters
- epidemiology
- methodology
- running
- cycling
- swimming
- triathlon
- illness
- injury
- SAFER
Introduction
Protecting athlete health is a top priority for medical staff caring for thousands of participants at road running races and other endurance events held annually around the world. There is a notable increase in older (>40 years) and female race participants.1 Participant numbers in endurance running events from shorter races (5–21.1 km) to ultraendurance multiday events are high, with similar high participant numbers across other endurance sports such as cycling, triathlon, swimming, cross-country skiing and other events with varying environmental challenges (ie, high altitude, extreme heat and cold). Despite high participant numbers, there are only limited data on race day medical outcomes at such events.2–8
There is a definite risk of adverse medical events during an exercise, including acute myocardial infarction and sudden cardiac death (SCD),9–13 particularly during prolonged high-intensity exercise.2 14 15 Previously sedentary individuals1 9 16 17 and patients with risk factors for chronic or underlying disease10 18 are at higher risk. The risk of sudden death (SD) during endurance sports events such as the half-marathon (21 km) and the marathon (42 km) is well described and varies between 0.25 and 3 per 100 000 race entrants for marathons.2 13 19–26 In cycling, there does not appear to be an increased risk of SCD in young/middle-aged participants with no previous cardiac conditions,27 but in recreational cyclists the occurrence of acute cardiac events increases with age and lower performance level.28 Cycling is also associated with a risk of acute traumatic injuries.29 In mass community-based endurance cycling events, both traumatic injuries of the musculoskeletal system and cardiovascular complaints are the most frequent medical encounters reported.5 6 SD and cardiac arrests during triathlons have also been reported,30 31 with a higher risk (per 100 000 participants) in male (male=2.40, female=0.74) and older age participants (18.6 for those 60 years and older), with most deaths occurring in the swim segment.31 In other endurance sports such as cross-country skiing, an incidence of SD of about 2.2 per 100 000 has been also been reported.32
However, SD and cardiac arrest represent only the ‘tip of the iceberg’ of medical encounters at mass community-based endurance sports events.33 The incidence of a serious life-threatening medical encounter (eg, myocardial infarction, exertional heat stroke, hyponatraemia) at a distance running event, such as the marathon, varies between 16.7 and 155 per 100 000 race entrants,8 33 and this is 50–100 times higher than the incidence of SD.33 To date, non-fatal but serious medical encounters have not been well characterised across the majority of endurance events, and there is no current consensus on the definition of a ‘serious life-threatening’ medical encounter on race day. The absence of a uniform definition for serious life-threatening and somewhat less serious medical encounters makes it difficult to compare incidence and prevalence between events.
Consensus statements with uniform definitions of injury or illness and consistent data collection procedures in many sports34–37 have permitted accurate illness and injury data collection at major tournaments.38–43 Similarly, in the field of research in endurance sports medicine, consensus is needed to standardise research methods for recording injury and illness-related medical encounters at mass community-based endurance sports events.
Objectives of the consensus document
The aim of the expert group was to agree on a set of standardised definitions of medical encounters (ie, incidents, complications) and a standardised methodology to record and report medical encounters at mass participation community-based endurance sports events. Uniform collection of multicentre data will make comparisons between races possible and inform illness and injury prevention strategies. In this way we aim to reduce medical encounters and facilitate safer participation in endurance events worldwide.44
Methods
A consensus ‘MEDICAL METHODS IN ENDURANCE SPORT’ group, consisting of expert researchers and clinicians in the area of endurance race medicine, representing international community-based endurance sporting events, was convened. Our core group first met in Boston, MA (May 2016) to develop a planning document for the consensus statement. Additional members with clinical and research experience in the field were identified by the core group, and added to the consensus group. We developed the consensus document at in-person and conference call meetings over a period of 2–3 years from May 2016 to November 2018. Draft versions of the consensus statement were circulated electronically during the development period and detailed additions, editing and comments were used to finalise the definitions and methodological recommendations. Representatives of three major sporting federations (athletics, cycling and triathlon) were included in the preparation of the manuscript for endorsement of the final consensus document. Agreement was achieved by consensus of a majority group members.
Three members of the consensus group identified source information papers by conducting a literature review (MS, JB, MB) in the electronic database PubMed. The methods and outcomes of this review process are described in the online supplementary table 1. This source information was reviewed, debated and included in draft versions of the document before final consensus was reached. More details and the references for specific definitions that were used from source information are listed in the online supplementary table 2.
Supplemental material
Supplemental material
Consensus recommendations
The consensus group recognised that standard definitions were required for the following: (1) sports ‘event’, (2) medical encounters, (3) severity and timing of medical encounters, (4) diagnostic categories of medical encounters, and (5) standardising research methods, specifically the collection of data at events and the reporting format for the data.
Definitions of sports ‘event’ and ‘medical team’
Mass community-based endurance sports event
A mass community-based endurance sports event is defined as ‘a planned and organised endurance sports event, usually with >1000 entrants (recreational and/or elite), at a specific location, for a specific purpose, and for a defined period of time (single day/stage or multiple stages/several consecutive days).’45 46 A ‘community-based’ event is an event typically planned and organised by a community sports organisation with a committee that includes a race director, and may be under the auspices of a regional or national sports federation. ‘Mass participation’ is a mass gathering of race participants with >1000 race entrants,45 46 but we also recognise that events of a smaller size (<1000 race entrants) can be managed and collect data using the consensus plan. ‘Endurance sports events’ include one or more of the following sports types: distance running, cycling, swimming, triathlon, canoeing/kayaking, rowing, cross-country skiing, mixed ultraendurance events (eg, biathlon, duathlon) and other similar activities that combine any of these disciplines or function with more than one athlete as a team of entrants.
Medical team
The medical team is defined as the ‘officially designated team of medical staff (medical physicians, pre-hospital medical and basic first aid providers, registered nurses, physiotherapists, athletic trainers, and others) responsible for the medical care during the event, typically led by a medical director (or equivalent).’ Emergency medical services and medical staff of participating local hospitals can be part of the medical team or may collaborate with the medical team to provide clinical services and support event research.
Definitions of medical problems/medical encounters
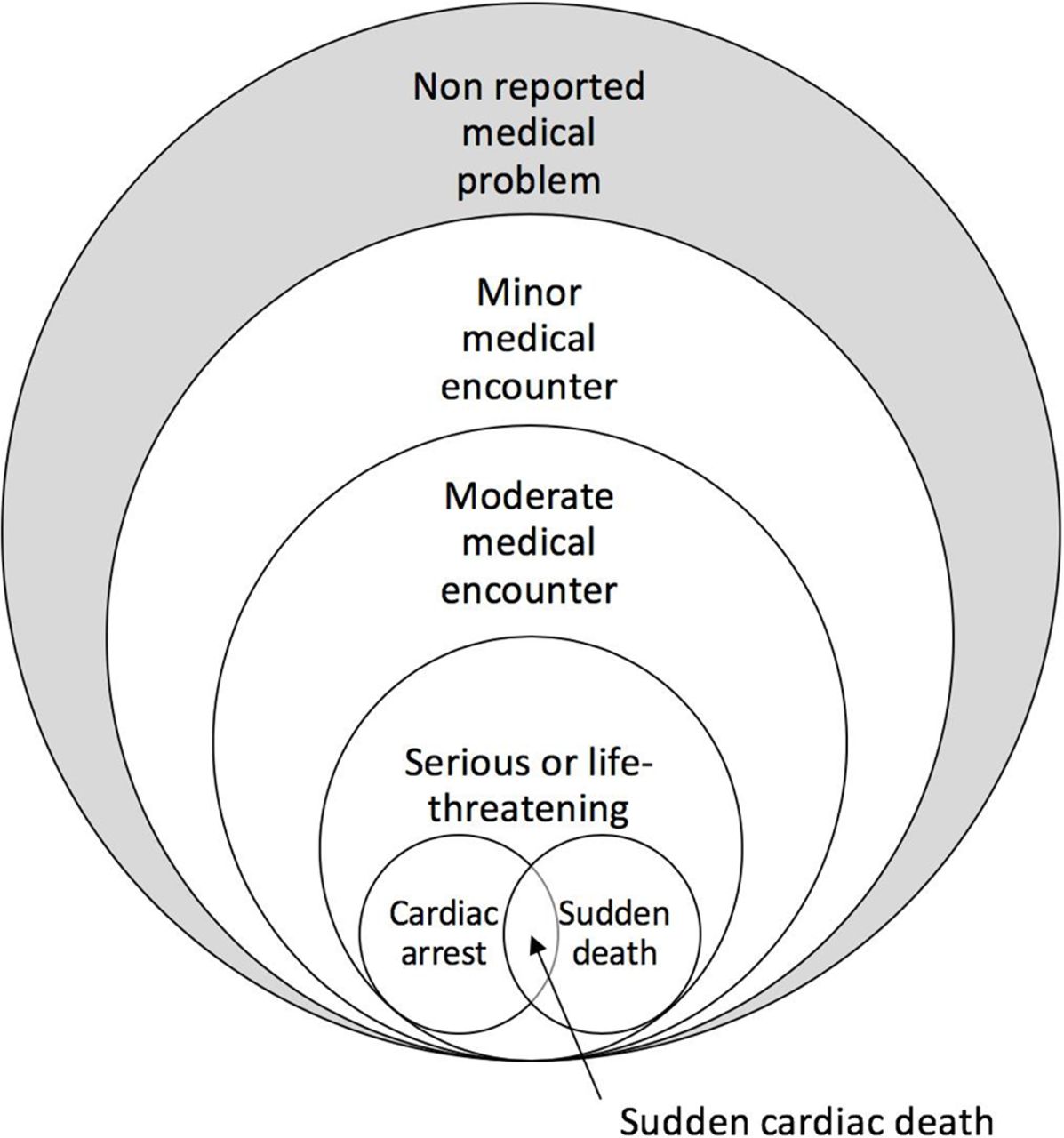
We recognised that athletes who participate in endurance events may develop a ‘medical problem’ during the event, and this ‘medical problem’ may or may not be reported by the athlete to the event medical team. For the purpose of this consensus document, only ‘medical problems’ that are reported to the event medical team will be considered as ‘medical encounters’. The consensus group agreed to use ‘medical encounter’ as the standardised term to define any reported ‘medical problem’ at an event, including both illness and injury-related encounters. We acknowledge and define a ‘non-reported medical problem’ as ‘a medical problem experienced by an athlete participating in an event, where the athlete decides not to seek assistance at all, or seeks assistance outside of the event medical team’. We classified all reported medical problems as ‘medical encounters’ to distinguish these from non-reported medical problems (figure 1).
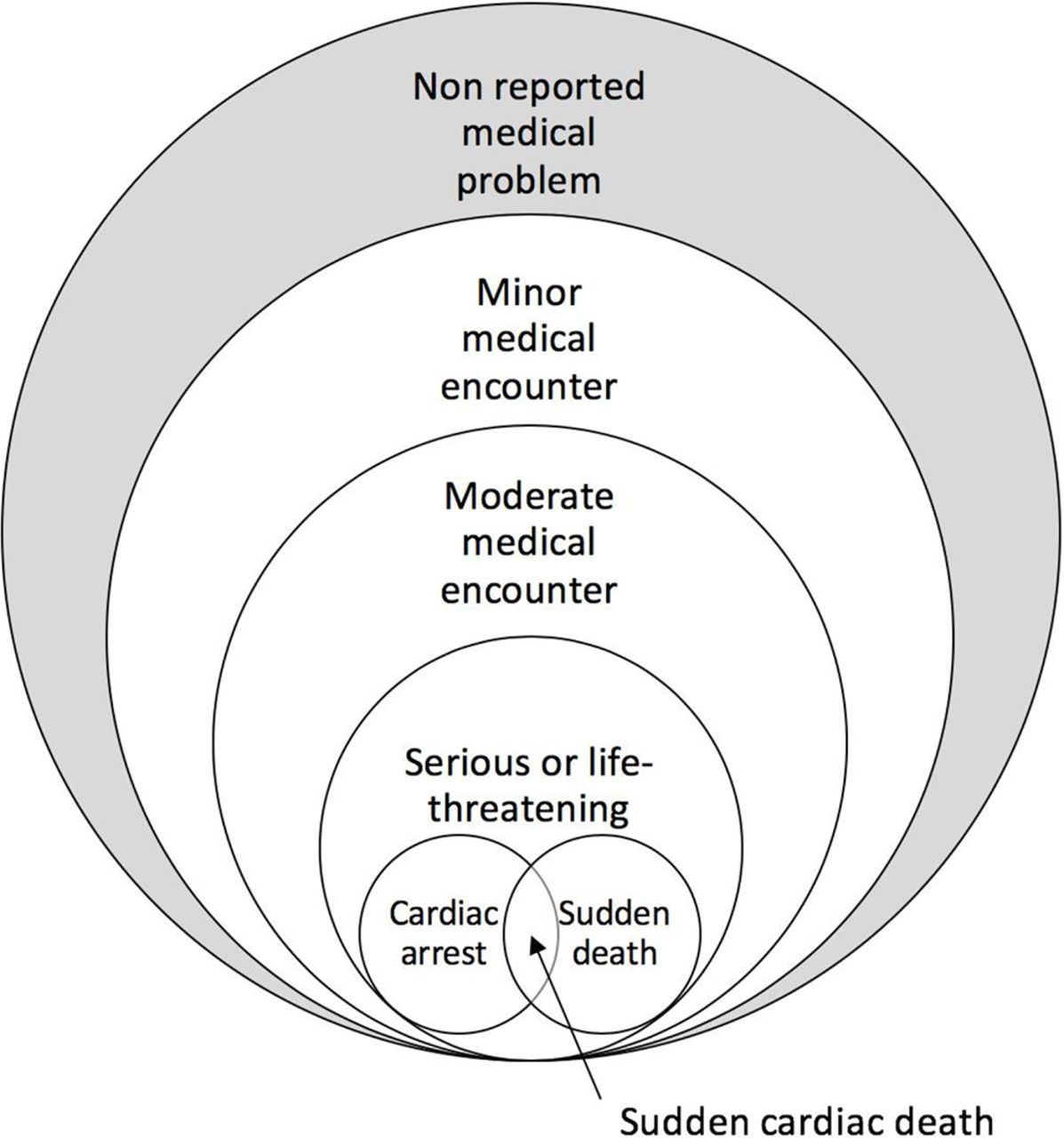
Classification of all medical problems at endurance sports events, including reported medical problems (medical encounters—not shaded) and non-reported medical problems (shaded).
Severity and timing of medical encounters
The definition of a medical encounter and the definitions of medical encounters classified by severity (minor, moderate, serious/life threatening, sudden cardiac arrest (SCA), SCD and SD) (table 1) are depicted in figure 2. For purposes of clarity, we also offer examples of similar terminology from the published literature, with key references (table 1).
Definitions of medical encounters and medical problems

{kind=link}
{kind=link}
Classification of medical encounters by severity. (A) Minor medical encounters. (B) Moderate medical encounters. (C) Serious life-threatening medical encounters. (D) Sudden cardiac arrest. (E) Sudden death. (F) Sudden cardiac death.
Timing of the medical encounters
We recognised that a medical encounter at a sports event can occur at different times during or following the event and that documenting the timing of the encounter is clinically important. There is also a need to clarify which encounters are related to a specific event, to make comparisons possible. We did not include any medical encounter that occurred before the official start of the event, for example, during a warm-up period. The consensus group defined the following three time periods for the timing of a medical encounter:
During the event (from the official start to completion of the event by the individual athlete).
Immediately after finishing (from the time an athlete completes the event to 1 hour after the athlete completes the event).
Delayed presentation (between 1 and 24 hours) after the athlete completes the event to record serious/life-threatening medical encounters, SCA, SCD and event-related death that may present as a delayed clinical presentation (eg, hyponatraemia).
The time period in which a medical encounter occurs should be recorded in the participant’s medical encounter report form. For example, a 3-hour finisher of a marathon that starts at 08:00 would be classified as ‘during the event’ from 08:00 to 11:00, ‘immediately post-finish’ from 11:00 to 12:00 and ‘delayed presentation’ from 12:00 to 11:00 the following day.
Diagnostic categories of medical encounters
Medical encounters at mass community-based endurance sports events can be broadly classified into two main diagnostic categories: illness-related and injury-related medical encounters. Illness-related medical encounters are usually classified by major organ system affected, while injury-related encounters are usually classified by major anatomical regions affected. The consensus group did consider a number of potential diagnostic coding systems including the International Classification of Diseases (ICD, version 10) and the International Classification of Primary Care codes. However, in the discipline of sports and exercise medicine these coding systems have some limitations, as there are a number of specific exercise-related injuries and illnesses that are not coded in these systems. The Orchard Sports Injury Classification System (OSICS) was developed in 1992 as a specific sports injury classification system, was tested for reliability in 200447 and, in one study, was superior to the ICD-10 coding system with higher intercoder agreement and being statistically significantly faster to use.48 The original OSICS coding system underwent revisions, mainly by including diagnoses that were not covered in previous versions and is one of the world’s most commonly used systems for coding injury in sports injury surveillance.49 For this consensus, diagnoses of medical encounters at mass community-based endurance sports events were reviewed extensively by the consensus group, and deficiencies in all the coding systems (including the OSICS) were identified, particularly for illness-related diagnostic codes. Therefore, for the purposes of this consensus, modified versions of the OSICS 10.1 medical and injury diagnostic classifications of more common medical encounters (illness and injuries) were used.47 49
Illness-related diagnostic categories
We recommend the use of a diagnostic classification system of illness-related medical encounters by main organ system, followed by more specific diagnostic codes for the more common illness-related medical conditions during endurance sports events (online supplementary table 3). We retained the broad main organ system categories in the OSICS 10.1 illness classification system, but found the system to be deficient for many common specific illness types that are seen at endurance sports events, for example, exercise-associated muscle cramps, exercise-associated postural hypotension, dehydration and hyponatraemia. The group therefore added specific illness types, and this resulted in a substantial modification of the OSICS 10.1 illness classification system.47 49 The severity of illness-related medical encounters was classified as minor, moderate, serious/life threatening and SCA/SCD using the definitions described above.
Supplemental material
For illness-related medical encounters, additional information related to the location of the illness on the course (eg, related to hills, course conditions), prerace medical history (eg, prerace acute illness, use of medications prior or during the event) and other factors possibly contributing to the illness (eg, weather conditions, equipment failure, athlete inexperience) can also be collected (online supplementary table 4).
Supplemental material
Injury-related diagnostic categories
We recommend the use of an injury-related medical encounter classification by the main anatomical region affected by the injury, followed by more specific diagnostic codes (online supplementary table 5). More specifically, the OSICS 10.1 injury classification system was slightly modified to include some additional injuries, mainly chronic (or ‘overuse’) injury codes that were not present in the OSICS 10.1 injury classification system. The severity of injury-related medical encounters was classified as minor, moderate, serious/life threatening or death using the definitions described above.
Supplemental material
For injury-related medical encounters, additional information related to the location on the course where the injury occurred (eg, related to hills, course conditions, distance from the start, nearest distance marker), onset of the injury (acute injury, chronic injury, acute exacerbation of a chronic injury), mechanism of the injury (eg, traumatic, non-traumatic, contact or non-contact, nature of the contact) and other factors contributing to the injury (eg, violation of rules, weather conditions, equipment failure, athlete inexperience) could also be collected (online supplementary table 6).
Supplemental material
Data collection
Research methods related to event data collection, athlete demographics, sports code, sports participation history, medical incident data collection procedures and reporting of the data are critical for quality of any scientific studies in this field. Data collection would ideally occur in a prospective cohort study design, but data collected using a retrospective cohort are also very valuable, provided data collection was accurate, comprehensive and that standardised terminology and definitions were adopted.
The consensus group recommends that general race data and medical encounter data at mass community-based endurance sports events should be collected in a standardised format. The data collection forms should be translated for use around the world, that data collection manuals be developed and that training of data collectors take place. International federations and organisations that endorsed this consensus are encouraged to implement these data collection procedures.
General race data collection
The following categories of general race data should be collected: race day data, athlete demographics, athlete race performance, geographical data of the course, environmental conditions on race day and medical team data (table 2). We recognise that not all race organisers, medical staff and researchers are able to collect detailed general race data in all the categories. Therefore, the consensus group classified general race data as ‘minimum/essential data’ and ‘additional data’.
Data collection (essential and additional data) on race day, athlete demographics, athlete race performance, course geography and environmental conditions on race day
Race medical encounter data collection
The consensus group recommends a uniform data collection procedure at the event medical facilities to record all medical encounters. For this purpose, the consensus group recommends using a standardised race medical encounter data (R-MED) form for illness-related medical encounters (online supplementary table 4) and injury-related medical encounters (online supplementary table 6). The R-MED forms were developed as a research tool and as a simplified standardised clinical data record form, where most data are entered by ticking ‘boxes’ so that forms can easily be used in a busy medical tent situation. Consensus group members are also developing electronic versions of these forms for widespread implementation.
We suggest that international federations, national federations, event organisers and race medical directors adopt this consensus, and use at least the minimum race day data collection format (table 2) and the R-MED forms (online supplementary tables 4 and 6) to collect data at all events, wherever possible.
Data reporting
We recommend that the following are reported routinely for all athletes (including subgroups, eg, by age groups and sex).
Individual athlete data
It is acknowledged that athletes could participate in multiple events, or the same event over a number of years. Therefore, documentation of individually coded, deidentified athlete data is recommended so that the number of athletes who participated in multiple events or in the same event over a number of years can be counted.
Incidence of medical encounters
The incidence of all medical encounters is reported as the number of encounters (numerator) per race starters (denominator). In addition, the incidence of medical encounters should be reported by subcategories of severity of medical encounters (minor, moderate, serious/life threatening), organ system (illness related), anatomical region (injury related) and final diagnosis (illness or injury type).
It is conventional that the incidence of medical encounters is reported as the patient presentation rate (medical encounters per 1000 race starters).50 In data analysis from earlier studies that predate electronic chip timing, the incidence can be reported per 1000 race entrants or finishers.8 In cases where small numbers of specific encounters are reported (eg, serious/life-threatening medical encounters or SCD), the denominator can be 10 000 or 100 000 race starters.50 For comparison between different incidences of illness or injury-related medical encounters, illness or injury rate ratios could be determined.
Did-not-start rate
The did-not-start is the percentage (%) of athletes who registered, but did not start the event calculated as follows: [(the number of athletes who entered or registered for the event − the number of athletes who started the event)/(the number of athletes who entered or registered for the event)] * 100.
Did-not-finish rate
The did-not-finish is the percentage (%) of athletes who started the event, but did not finish the event calculated as follows: [(the number of athletes who started the event − the number of athletes who finished the event)/(the number of athletes who started the event)] * 100.
Overall medical encounter rate and severity-based encounter rates: minor, moderate and severe/life threatening
The medical encounter rate is the proportion of athletes (usually per 1000 athletes) who started the event and had a medical encounter or severity-based encounter, calculated as follows: [(the number of athletes who had a medical encounter/the number of athletes who started the event) * 1000]. In older studies, the denominator isa often entrants or finishers and these rates can also be calculated for events.8
SCA and SCD rate
The SCA or SD rate is the proportion of athletes (usually per 100 000 athletes) who started the event, and who had an SCA with or without successful resuscitation (including defibrillation) during or within 1–24 hours after the event calculated as follows: [(number of athletes who had an SCA/number of athletes who started the event) * 100 000].
SD rate
The SD rate is the proportion of athletes (usually per 100 000 athletes) who started the event, and who died from any cause during or within 1–24 hours of finishing the event and deemed to be directly related to the event calculated as follows: [(number of athletes with SD/number of athletes who started the event) * 100 000].
Clinical implications and future research
Standardising definitions of medical encounters and methodology for data collection will help calculate more accurate incidence rates of medical encounters during endurance sports events. High-quality data collection will also allow dependable comparisons among different endurance events. Data collection as outlined in this consensus statement will allow more detailed study of intrinsic and extrinsic risk factors, environmental conditions and prerace medical disorders associated with endurance events. If those who organise mass community-based endurance sports events adopt these guiding principles, it will (1) guide the direction of future preventive strategies to reduce medical encounters, and (2) allow better allocation of medical resources (equipment, personnel, and so on) for endurance events of all sizes. This consensus will form the basis of expanding the Strategies to Reduce Adverse Medical Events for the Exerciser (SAFER) studies2–4 51 to a SAFER International Million+Athlete Program. Ultimately, the aim for research in this field is to protect athlete health in all endurance race participants around the world.44
Endorsements
International Institute for Race Medicine (IIRM)
International Association of Athletics Federations (IAAF)
Union Cycliste Internationale (UCI)
International Triathlon Union (ITU)
Acknowledgments
The authors acknowledge the contributions of medical staff for their service to the athletes participating in endurance events over many years, race organisers who support this consensus and all the athletes for their interest and participation in the races.
References
Footnotes
Contributors MS: responsible for the overall content as the consensus statement guarantor, consensus concept, manuscript planning, search strategy, search and data interpretation, manuscript (first draft), manuscript editing, facilitating funding. CK, WOR, JAD, DCJvR, MH: consensus concept, manuscript planning, manuscript editing. PDH: consensus concept, manuscript editing. CT, JK: manuscript planning, manuscript editing. JB: search strategy, search and data interpretation, manuscript (first draft), manuscript editing. PEA, SB, XB, SM: manuscript editing. EJ: manuscript editing (data collection and reporting). MB: consensus concept, manuscript planning, search strategy, search and data interpretation, manuscript (first draft), manuscript editing.
Funding Partial funding for generating the consensus was received from two IOC Research Grants: (1) IOC Research Center grant to the University of Pretoria and (2) IOC Grant for study entitled: ’Reducing Medical Complications and Injuries at Endurance Sports Events: A 20-year Longitudinal Study (2008–2027). INTERNATIONAL MILLION+ ATHLETE PROJECT-SAFER (IMAPS)'.
Disclaimer The funding agency did not influence the content of the consensus statement.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Patient consent for publication Not required.