Article Text

Abstract
Purpose To (1) quantify white matter (WM) alterations in female high school athletes during a soccer season and characterise the potential for normalisation during the off-season rest period, (2) determine the association between WM alterations and exposure to repetitive subconcussive head impacts, and (3) evaluate the efficacy of a jugular vein compression collar to prevent WM alterations associated with head impact exposure.
Methods Diffusion tensor imaging (DTI) data were prospectively collected from high school female soccer participants (14–18 years) at up to three time points over 9 months. Head impacts were monitored using accelerometers during all practices and games. Participants were assigned to a collar (n=24) or non-collar group (n=22). The Tract-Based Spatial Statistics approach was used in the analysis of within-group longitudinal change and between-group comparisons.
Results DTI analyses revealed significant pre-season to post-season WM changes in the non-collar group in mean diffusivity (2.83%±2.46%), axial diffusivity (2.58%±2.34%) and radial diffusivity (3.52%±2.60%), but there was no significant change in the collar group despite similar head impact exposure. Significant correlation was found between head impact exposure and pre-season to post-season DTI changes in the non-collar group. WM changes in the non-collar group partially resolved at 3 months off-season follow-up.
Discussion Microstructural changes in WM occurred during a season of female high school soccer among athletes who did not wear the collar device. In comparison, there were no changes in players who wore the collar, suggesting a potential prophylactic effect of the collar device in preventing changes associated with repetitive head impacts. In those without collar use, the microstructural changes showed a reversal towards normal over time in the off-season follow-up period.
- concussion
- injury prevention
- soccer
Statistics from Altmetric.com
Introduction
Soccer athletes face one of the highest risks of sustaining sports-related traumatic brain injuries (sTBIs) among all competitive sports.1 2 While both male and female soccer athletes are at risk of sustaining sTBI, female soccer athletes suffer increased sTBI rates,3 symptoms4 and protracted recoveries5 relative to males with similar head impact exposure.6 The risk of long-term morbidity associated with these injuries7 has encouraged research on the cumulative effects of repetitive subconcussive impacts (SCIs) throughout a player’s career.8
SCIs are impacts that do not result in the clinical manifestations of a concussion8 and a single SCI may not have serious implications; however, when aggregated over an athlete’s career, they may have deleterious cognitive effects.9 10 Neuroimaging provides objective biomarkers of white matter (WM) structural changes at acute, semi-acute or chronic stages in athletes during a season of repetitive head impacts.11–18 WM integrity can be altered by either concussive impacts or SCI,11–18 and longitudinal changes in WM microstructure are also evident in athletes exposed to a full season of SCI.12 16 19 20
A specialised neck collar has been developed to apply mild bilateral jugular vein compression that diverts flow to the vertebral veins, promoting cerebral engorgement21 and potentially reducing intracranial energy absorption.22 23 This is postulated to dampen the effects of SCI on WM integrity. This specialised collar has been shown to preserve WM integrity in previous neuroimaging studies involving season-long usage in male football and hockey athletes,10 24 but the collar has not been investigated in females nor in collision sports where players do not wear helmets.
There has been no prospective longitudinal study of female high school soccer players and their WM responses over a season of soccer with repetitive subconcussive head impacts. In the present study, we recruited female high school soccer athletes who underwent diffusion tensor imaging (DTI) at up to three time points: pre-soccer season, post-soccer season and 3 months post-soccer season. We aimed to (1) quantify and characterise WM alterations using DTI during the soccer season and in the off-season rest period, (2) determine the association between changes in WM and exposure to the repetitive subconcussive head impacts, and (3) evaluate the efficacy of jugular vein compression to prevent these WM alterations over the three time points.
Methods
Patient involvement and ethical approval information
Seventy-five participants (ages 14–18 years) were recruited from two local high school female soccer teams as part of a prospective longitudinal neuroimaging study. Athletes who were slated to make the upcoming year’s junior varsity or varsity high school soccer teams and were at least 14 years old were recruited for the study. Exclusion criteria for study participation included inability to provide written consent, history of neurological deficits, previous cerebral infarction, severe head trauma, known increased intracranial pressure, metabolic acidosis or alkalosis, glaucoma (narrow angle or normal tension), hydrocephalus, recent (within 6 months) penetrating brain trauma, known carotid hypersensitivity, central vein thrombosis, known airway obstruction or seizure disorder.
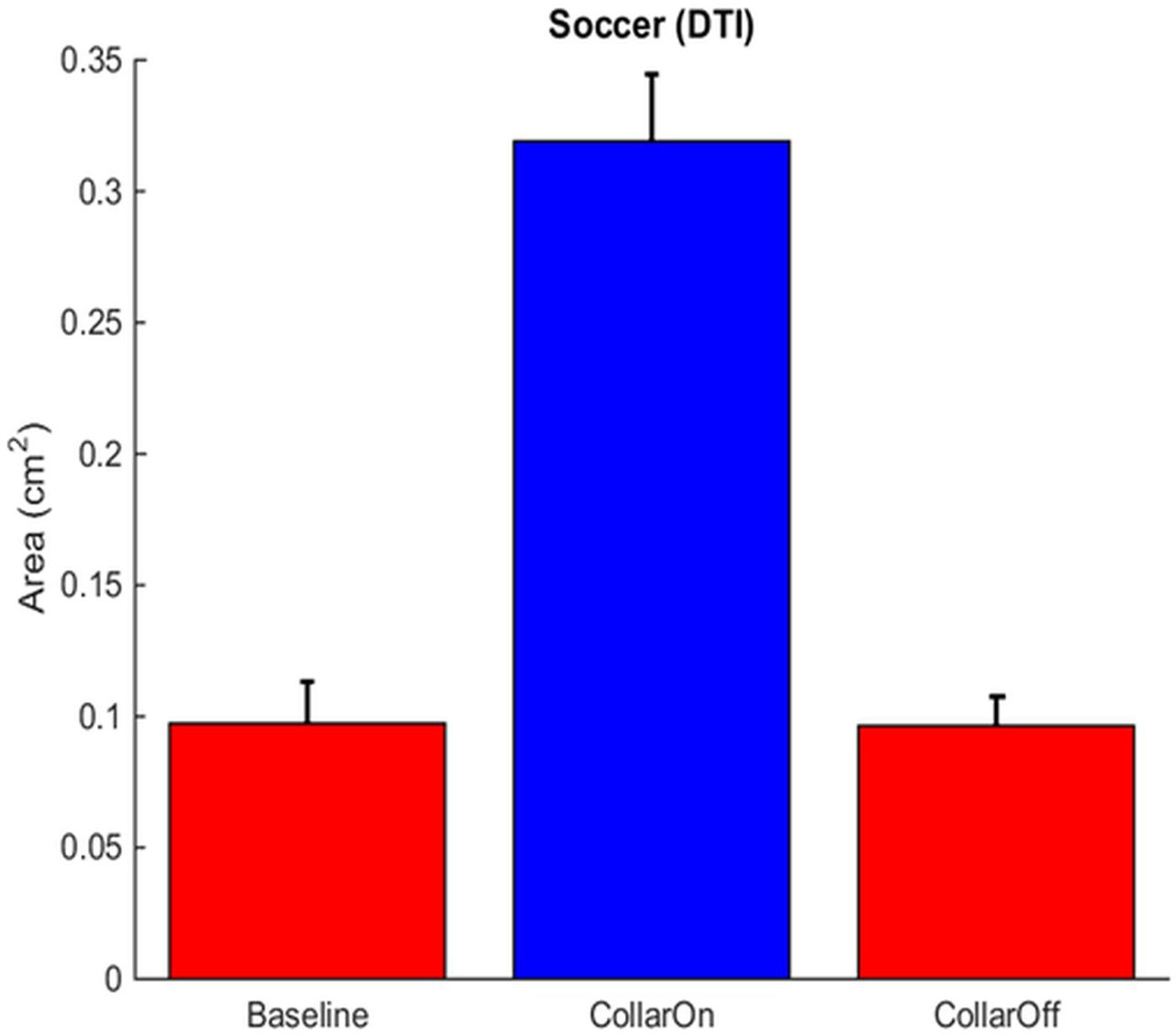
Participants underwent up to three MRI scans at three different time points: pre-season, post-season and off-season follow-up (approximately 3 months after post-season). The study design included two study groups—one group wearing a collar device designed to apply mild jugular vein compression during the competitive season and one group not wearing the collar. Group assignment was based on team. Subjects completed the study over the course of up to 10 months; however, the collar was only worn for games and practices in the collar group during their competitive season (pre-season to post-season). To evaluate the reliability and stability of DTI measures over a similar period to the competitive season time frame, a subcohort was also captured during a period of no head impact exposure (baseline to pre-season; n=11).
Among the initial 75 participants, 35 were assigned to the non-collar group, and 40 were assigned to the collar group. Fifteen participants were excluded due to dental braces, four participants were excluded as they did not make the final team roster and six additional participants were excluded because they either decided not to participate in the study (n=3), quit the team (n=1), were dropped from the team due to a non TBI-related injury (n=1) or did not meet inclusion criteria (n=1). The remaining 50 participants (23 in the non-collar group, 27 in the collar group) all underwent pre-season and post-season MRI evaluation.
Statistical analyses were performed first primarily between pre-season and post-season time points in the 50 participants who underwent both pre-season and post-season scans. Due to excessive head motion during the MRI, four participants (one in non-collar group, three in collar group) were excluded in this portion of the analyses. Therefore, the final analyses of pre-season to post-season comparison were based on data from 22 participants in the non-collar group and 24 participants in the collar group. The second part of the analyses focused on the longitudinal comparisons in those participants who completed MRI at all three time points including the pre-season, post-season and off-season follow-up. Among the 22 participants in the non-collar group and the 24 participants who had pre-season and post-season MRI data, 12 participants from each group were recruited to undergo MRI during the off-season follow-up. After excluding participants with excess head motion during scanning (one in each group), 22 participants (11 in each group) were included in the subcohort analyses which included off-season follow-up.
It should be noted that among the 22 participants in the non-collar group and the 24 participants in the collar group who had pre-season and post-season MRIs, two participants in the non-collar group and one participant in the collar group experienced concussion during the sport season. Of the three participants with a clinical diagnosis of concussion, only one was among the subgroup of participants (n=22) included in off-season follow-up scans. Since the change in DTI between different time points from these three participants with a diagnosed concussion did not differ from the rest of the participants in their corresponding group, the final analyses in the manuscript were reported with clinical diagnosed concussion cases included.
Ultrasound response and collar wear compliance
At the first fitting of the collar, a registered vascular technologist used ultrasound to ensure that the collar fit correctly and superior jugular distension was achieved as previously described10 (figure 1). Following the initial fitting, each athlete received instruction on how to properly use the device for games and practices. Throughout the soccer season, the reported daily compliance rate of collar wear in the collar group was 100% for all the games and practices. The collar group played 16 games and 37 practices and non-collar group 14 games and 27 practices.

Jugular response to both application and removal of the collar. DTI, diffusion tensor imaging.
Head impact measurement
Each participant was provided with an X Patch accelerometer (X2 Biosystems, Seattle, Washington, USA). The X Patch is a small, durable device that attaches to the back of the neck behind the ear using an adhesive and tracks head accelerations due to impacts. The data recorded by the X Patch were used in the final analysis to normalise the exposure to SCI.
MRI/DTI data acquisition, processing and analysis
All MRI data were acquired on a 3-Tesla Phillips Achieva MRI scanner (Philips Medical Systems, Best, Netherlands) using a 32-channel head coil across all time points during the study (baseline, pre-season, post-season and off-season follow-up). DTI data were acquired with a 61-direction spin echo-planar imaging sequence. The following parameters were used: TR/TE=8788/97 ms; field of view, 256×256 mm; acquisition matrix, 128×128; slice thickness, 2 mm (voxel resolution=2×2×2 mm); number of slices, 68; SENSE factor, 3; diffusion weighting factor b-value=1000 s/mm2. Seven interleaved frames of images without diffusion weighting (b0) were acquired. A high-resolution 3D T1-weighted anatomical data set (voxel size=1×1×1 mm) was acquired in the sagittal direction for image registration and review.
The Functional MRI of the Brain (FMRIB) Software Library (FSL) software package (www.fmrib.ox.ac.uk/fsl) was used in imaging data processing and analysis. The four commonly used DTI measures, including fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD) and radial diffusivity (RD), were calculated using standard methods.25 The four commonly used DTI metrics (FA, MD, AD, RD) are calculated from the three eigenvalues of the diffusion tensor. AD equals the magnitude of diffusion along the direction of the primary eigenvector (the eigenvector with the maximum diffusivity) and RD equals the average of diffusion of the two other eigenvectors in the plane transverse to the primary eigenvector. FA is a quantification of the degree of directionality. It is calculated as the normalised variance of the three eigenvalues of the tensor, that is, the ratio of the squared difference between eigenvalues and their mean to the sum of squared eigenvalues. Therefore, FA depends mathematically on the magnitude of change of both AD and RD and can be insensitive to the actual structural alteration if AD and RD change in the same direction.
The tract-based spatial statistics (TBSS)26 approach was used in the analysis of within-group longitudinal change and between-group comparisons. Threshold-free cluster enhancement (TFCE)27 was used in correcting multiple comparison errors.
Reliability of DTI-derived metrics
To evaluate the consistency of specific DTI parameters (FA, MD, AD and RD) and study methodology, 11 athletes were measured 7–8 weeks prior to the pre-season (baseline) scanning during a period with no head impact exposure. Intraclass correlations (ICCs) of DTI measures between the no head impact pre-season period and pre-season baseline time point were evaluated within regions of interest reported for the overall study design (e.g., pre-season to post-season comparisons). The ICCs for the DTI-derived metrics used to evaluate group comparison (collar vs non-collar) were high for FA (0.944), AD (0.776), MD (0.829) and RD (0.895); all two-sided 95% CIs overlapped; no single athlete was responsible for the numerically lower ICCs for AD, MD and RD. ICCs calculated for the entire anisotropic mask ranged from 0.93 to. 97 for DTI-derived metrics. Specific DTI-derived metrics (AD, RD and MD) demonstrate high ICCs and are sensitive to alterations in white matter associated with head impact exposure.10 28 The cumulative evidence indicates that the methods used for DTI scanning and analysis demonstrate the highly consistent reproducibility needed to support DTI-derived metrics as the endpoint for quantifying longitudinal structural changes to WM.29
Imaging outcome and statistical analysis
The primary outcome measures in the present study were within-group DTI alterations between different time points and the between-group difference of these longitudinal changes.
Imaging analyses of DTI change between pre-season and post-season (22 in the non-collar group and 24 in the collar group)
Voxel-wise analysis using TBSS was first carried out to evaluate potential cross-sectional group differences using an independent t-test at the pre-season time point. Then TBSS was used to test statistical significance in the pre-season to post-season change for each group, which was calculated using a one-sample t-test on the difference maps between the two time points. The group difference of pre-season to post-season change was tested for statistical significance based on a two-sample t-test of the difference maps of individual subjects. The randomise function from FSL was used to generate a null distribution for comparison of the resulting t-test statistics for statistical significance. The number of permutations in the one-sample t-test was determined by sample size, and 5000 permutations were used in the two-sample t-test. Multiple-comparison correction was achieved through the TFCE method incorporated into the randomise software in FSL. The median DTI values (FA, MD, AD and RD) were extracted from the brain regions that showed significant pre-season to post-season DTI change and were used in the correlation analysis. Pearson correlation was used to test whether exposure to repetitive head impacts during the season was associated with the significant DTI changes observed between the two time points. Brain regions with significant pre-season to post-season changes were segmented into clusters belonging to individual WM tracts to explore the DTI changes attributable to the repetitive head impacts. The localisation of the anatomical regions of the WM tracts was determined based on the John Hopkins University WM tractography atlas30 and the International Consortium of Brain Mapping (ICBM)-DTI-81 WM atlas.31 32
Imaging analyses of DTI change in the 22 participants (11 in each group) who underwent MRI at three time points (pre-season, post-season and off-season follow-up)
Voxel-wise analysis using TBSS was also used in the analyses of imaging data from this subset of participants. TBSS was first carried out to test the potential cross-sectional group difference using an independent t-test at all three time points with a focus on the off-season follow-up period. Between pre-season and post-season, each study group was tested for longitudinal changes (the pre-season to post-season change), which was calculated for each group using a one-sample t-test on the difference maps between the two time points. The group difference of pre-season to post-season change was tested for statistical significance based on a two-sample t-test of the difference maps (from pre-season to post-season) of individual subjects. Between post-season and off-season follow-up time point, we evaluated whether the DTI changes observed in the prior phase (from pre-season to post-season) reversed or continued to progress in the same direction with statistical significance. Between pre-season and off-season follow-up time point, we evaluated whether the WM diffusion properties had returned to the pre-season level after a 3-month off-season, non-collision period. Since we aimed to assess the progression of DTI alteration that occurred during the soccer season, a mask based on areas corresponding to the significant pre-season to post-season DTI change in the non-collar group was used in the subsequent analysis between post-season and off-season follow-up and between pre-season and off-season follow-up. In these analyses, the longitudinal DTI change within each group and the between-group difference were tested using the same methods as that between pre-season and post-season. Similar to the correlation analyses described previously, Pearson correlation was analysed between the pre-season to post-season DTI change and the head impact experienced during the season.
Results
Demographic data
As described in the Methods section, of the 75 participants initially recruited for the study, 46 participants (22 in the non-collar group, 24 in the collar group) were included in the final analyses of pre-season to post-season DTI change. A subset of these participants, including 11 from each group, were included in the final analyses of longitudinal DTI changes across three time points (pre-season, post-season and off-season follow-up).
The age range of the 46 participants who completed both pre-season and post-season MRI scans was between 14.00 and 17.76 years at pre-season. In these participants, no significant group difference was found in age, time interval between pre-season and post-season MRI, and time interval between last practice/game and post-season MRI (table 1).
Participant demographic information and time intervals in the 22 participants in the non-collar group and 24 participants in the collar group who underwent both pre-season and post-season MRI
The age range of the 22 participants who underwent MRI at all three time points (pre-season, post-season and off-season follow-up) was between 14.71 and 17.61 years at baseline. As shown in table 2, the 11 participants in the non-collar group and the 11 participants in the collar group were comparable in age. For these participants, the time interval at different phases of the study, including number of days between baseline and pre-season, between pre-season and post-season, between post-season and off-season follow-up, and the time from last game/practice to time post-season, were all comparable between the two study groups (table 2).
Participant demographic information and time intervals in the 11 participants in the non-collar group and 11 participants in the collar group who underwent MRI scans at all three time points
Head impact exposure during the soccer season
The descriptive statistics regarding head impact exposure at different g-force thresholds during the soccer season in the two study groups are presented in table 3 and table 4. The two groups, regardless of whether they included all the participants with both pre-season and post-season scans (table 3), or whether they included only the subset that underwent MRI scan at three time points (table 4), were comparable in the total number of hits, cumulative g-force and the average g-force/hit experienced during the season (figure 2). No statistically significant group difference was found in any of the three variables across the different g-force thresholds.
Head impact statistics in the 22 participants in the non-collar group and 24 participants in the collar group who underwent both pre-season and post-season MRI
Head impact statistics in the 11 participants in the non-collar group and 11 participants in the collar group who underwent pre-season, post-season and off-season follow-up MRI testing
(A) Graphical representation of similarity in head impacts frequency between groups weighted by intensity (represented by height and colour) distributed about the sphere of the head for the control (left, no-collar) and collar group (right).
Imaging analyses of DTI change between pre-season and post-season (22 in the non-collar group and 24 in the collar group)
Between-group DTI difference at pre-season and post-season
The two study groups (collar, non-collar) were comparable at both pre-season and post-season on all the four DTI parameters without statistically significant differences between groups.
Within-group pre-season to post-season DTI change and group difference of longitudinal change
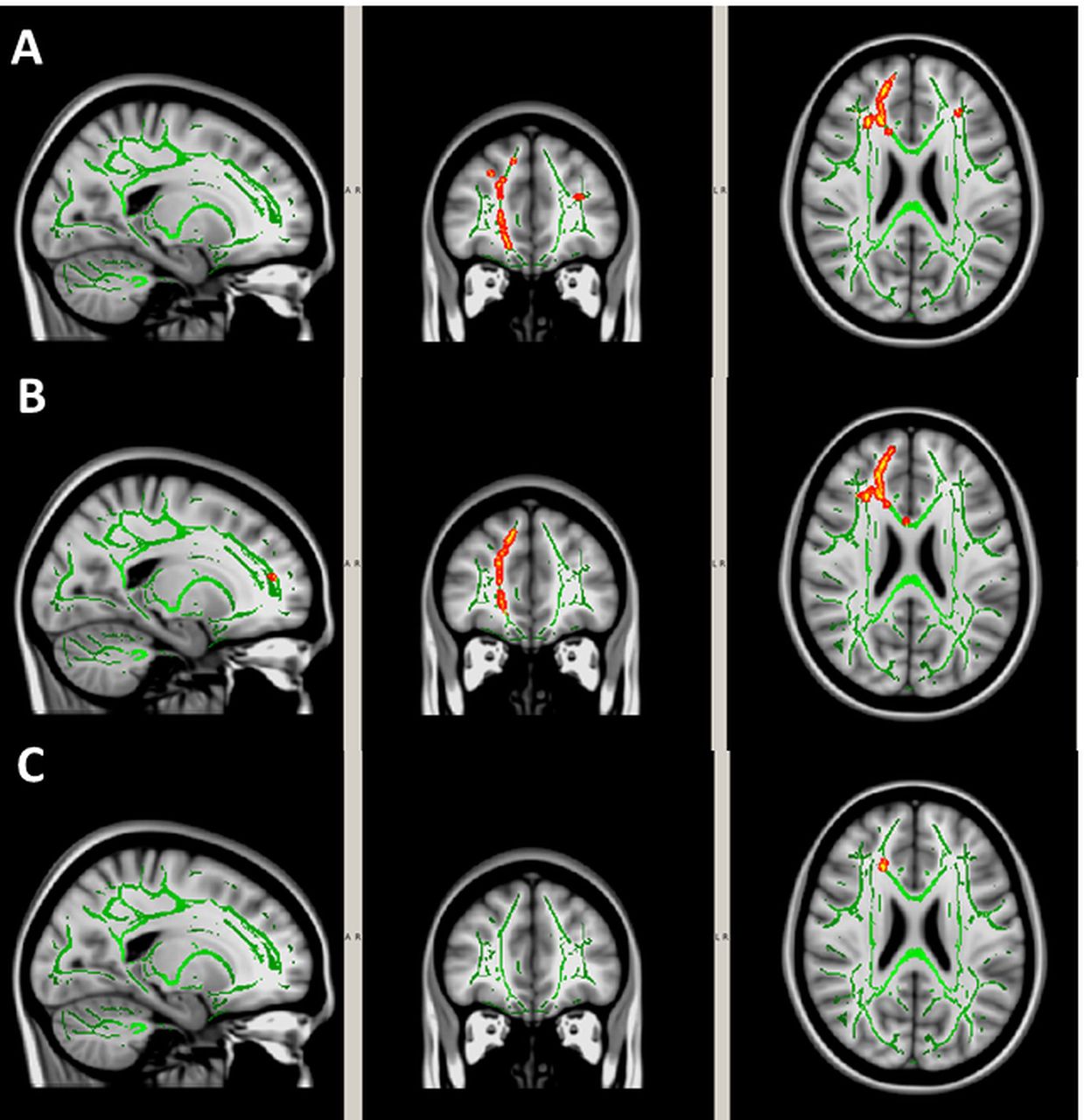
Significant pre-season to post-season decreases in MD, AD and/or RD (p<0.05, TFCE corrected) were found in extensive WM areas in the non-collar group (figure 3). The descriptive statistics of DTI percentage change are reported in table 5. These significant regions located in all 20 tracts as determined by the ICBM-DTI-81 WM atlas,32 33 including bilateral anterior thalamic radiation (ATR), corticospinal tract (CST), cingulum (cingulate gyrus part), cingulum (hippocampal part), forceps major, forceps minor, inferior fronto-occipital fasciculus (IFOF), inferior longitudinal fasciculus, superior longitudinal fasciculus (SLF), uncinate fasciculus (UF) and temporal part of SLF (table 6).

White matter (WM) regions with significant pre-season to post-season reduction in (A) mean diffusivity, (B) axial diffusivity and (C) radial diffusivity in the 22 participants in the non-collar group who underwent both pre-season and post-season MRI. The significant regions (red-yellow regions, p<0.05, threshold-free cluster enhancement corrected for multiple comparisons) were overlaid on to the WM skeleton (green) and standard T1-weighted image in MNI 152 space (grey scale). The significant regions were filled in using tbss_fill in FSL to improve visualisation.
Pre-season to post-season DTI percentage change in the 22 participants in the non-collar group and 24 participants in the collar group who underwent both pre-season and post-season MRI
Volume of white matter (WM) regions with significant pre-season to post-season change in MD, AD or RD in different WM tracts and the correlation between the diffusion tensor imaging change within significant regions with the total number of head impacts experienced during the season in the 22 participants in the non-collar group who underwent both pre-season and post-season MRI scans
No significant pre-season to post-season DTI change was found in any WM regions in the collar group. Using the collar group as the reference group, there were significantly larger pre-season to post-season reductions in MD, AD and RD in the non-collar group when compared with the collared reference group (figure 4). The WM regions with significant group difference were located in bilateral ATR, right CST, right cingulum (cingulate gyrus part), left cingulum (hippocampal part), forceps minor, bilateral IFOF, right SLF, right UF and right temporal part of SLF.
White matter regions with significant group difference in the pre-season to post-season reduction in (A) mean diffusivity, (B) axial diffusivity and (C) radial diffusivity between the 22 participants in the non-collar group and the 24 participants in the collar group who underwent both pre-season and post-season MRI. The significant regions (red-yellow regions, p<0.05, threshold-free cluster enhancement corrected for multiple comparisons) were overlaid on to the WM skeleton (green) and standard T1-weighted image in MNI 152 space (grey scale). The significant regions were filled in using tbss_fill in FSL to improve visualisation.
Correlation between head impact and DTI changes
The potential association between the head impact exposure experienced during the season and the pre-season to post-season changes in MD, AD and RD were first assessed in the non-collar group. DTI values (MD, AD and RD) were first extracted from the entire WM regions that presented significant longitudinal change during the season in the non-collar group. Among the three head impact variables (number of hits, cumulative g-force, average g-force/hit), the total number of head impacts showed a statistically significant correlation with the pre-season to post-season change in MD and RD (r=0.436, p=0.043 as shown in figure 5A; r=0.457, p=0.032 as shown in figure 5B, respectively). The cumulative g-force and average g-force/hit were not found to be associated with pre-season to post-season change in any of the four DTI parameters in the non-collar group.
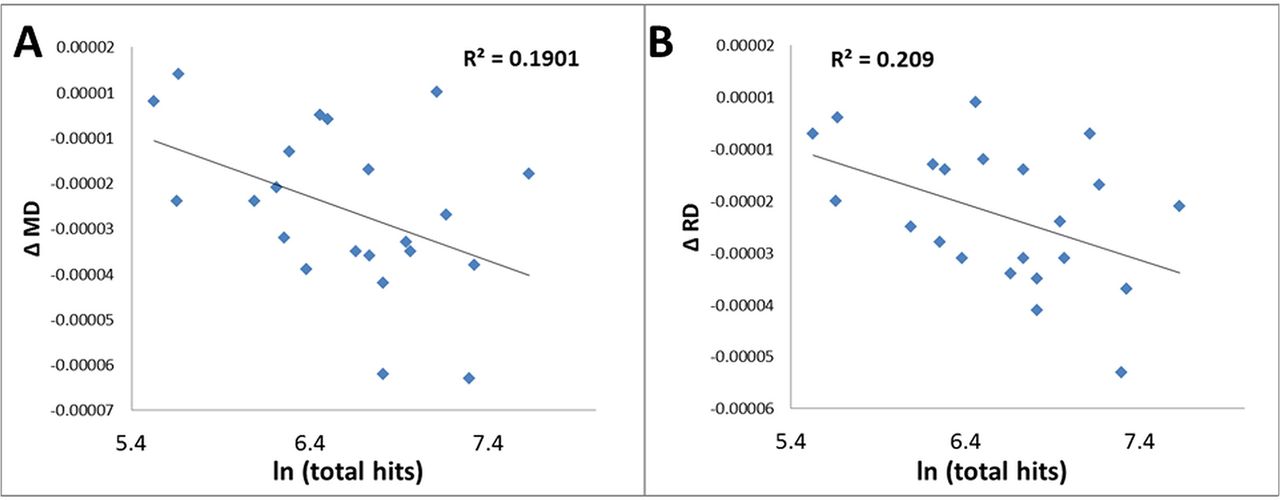
Correlations between the total number of hits and the pre-season to post-season reduction in (A) mean diffusivity (MD) and (B) radial diffusivity (RD) in the entire white matter regions (as shown in figure 4) found to show significant pre-season to post-season diffusion tensor imaging change in the 22 participants in the non-collar group who underwent both pre-season and post-season MRI.
No significant correlation was found between pre-season and post-season DTI difference in the collar group and the head impact experienced during the season.
Correlation between head impact and DTI change in individual WM tracts
These associations were further explored in individual WM tracts and to assess contribution to the overall correlation seen in the non-collar group. Among the 20 WM tracts within the regions that presented significant pre-season to post-season DTI changes in the non-collar group (table 5), six showed statistically significant correlations between the total number of hits and the pre-season to post-season DTI change (three for FA change, six for MD change, one for AD change, four for RD change; table 5). Figure 6 shows an example of the significant correlations based on the association between the total number of head impacts and the FA and MD change extracted from a significant area located in the left cingulate (cingulum hippocampal part) in the non-collar group.

Correlations between the total number of hits and the pre-season to post-season change in (A) fractional anisotropy (FA) and (B) mean diffusivity (MD) in left cingulum (hippocampal part) in the 22 participants in the non-collar group who underwent both pre-season and post-season MRI.
Imaging analyses of DTI change at all three (pre-season to post-season to off-season follow-up) time points (11 in the non-collar group and 11 in the collar group)
Longitudinal DTI alteration between pre-season and post-season
Significant pre-season to post-season decreases in MD and/or RD (p<0.05, TFCE corrected) were found in the non-collar group in a series of WM regions including bilateral ATR, bilateral IFOF, bilateral SLF and bilateral cingulum, right forceps minor and left UF (online supplementary figure S1, table 7).
Supplementary file 1
Volume of white matter (WM) regions with significant pre-season to post-season change in MD, AD or RD in different WM tracts and the correlation between the diffusion tensor imaging change within significant regions with the total number of head impacts experienced during the season in the subset of 11 participants in the non-collar group who underwent MRI scans at all four time points
No significant pre-season to post-season DTI change was found in any WM regions in the collar group. Similar to the group comparisons made using the entire data set, group difference of pre-season to post-season DTI change were made with the collar group serving as the reference group. Significantly larger pre-season to post-season reductions in MD, AD and/or RD were found in the non-collar group when compared with the collar group (online supplementary figure S2). The WM regions that presented this group difference included the same regions as found in the within group change in the non-collar group but involved smaller regions.
Supplementary file 2
Longitudinal DTI alteration between post-season and off-season follow-up time point
During the off-season period, within the WM regions that presented significant pre-season to post-season MD, and/or RD reduction in the non-collar group (as shown in online supplementary figure S1), there was a significant increase in MD, AD and/or RD in the non-collar group but not in the collar group (figure 7). The regions with significant change in the reverse direction in the non-collar group were located bilaterally in ATR, CST, cingulum (cingulate gyrus part), IFOF, SLF, forceps minor and left UF (figure 7). Using the collar group as the reference group, there was a greater increase in MD, AD and/or RD in the non-collar group (p<0.05, all TFCE corrected, figure 8) in WM regions located in bilateral ATR, cingulum (cingulate gyrus part) and SLF; left CST, IFOF and UF; and forceps minor.

White matter (WM) regions with significant increases in (A) mean diffusivity, (B) axial diffusivity and (C) radial diffusivity at off-season follow-up when compared with post-season in the 11 participants in the non-collar group who underwent MRI at all four time points. The significant regions (red-yellow regions, p<0.05, threshold-free cluster enhancement corrected for multiple comparisons) were overlaid on to the WM skeleton (green) and standard T1-weighted image in MNI 152 space (grey scale). The significant regions were filled in using tbss_fill in FSL to improve visualisation.

White matter areas with significantly greater increase in (A) mean diffusivity, (B) axial diffusivity and (C) radial diffusivity from post-season to off-season follow-up in 11 participants in the non-collar group when compared with the 11 participants in the collar group among those who underwent MRI at all four time points. The significant regions (red-yellow regions, p<0.05, threshold-free cluster enhancement corrected for multiple comparisons) were overlaid on to the WM skeleton (green) and standard T1-weighted image in MNI 152 space (grey scale). The significant regions were filled in using tbss_fill in FSL to improve visualisation.
Comparison of DTI between pre-season and off-season follow-up time point
Within the WM regions that showed significant pre-season to post-season DTI change, the MD value was significantly lower at the off-season follow-up point (time 4) when compared with the pre-season time point (time 2) in the non-collar group. The significant regions included part of left IFOF and extended to left UF and left ATR (figure 9). No significant longitudinal DTI difference was found in the collar group. No significant group difference of longitudinal DTI change was found between the two study groups.

White matter regions with significantly lower mean diffusivity values at off-season follow-up in comparison with pre-season in the 11 participants in non-collar group who underwent MRI at all four time points. The significant regions (red-yellow regions, p<0.05, threshold-free cluster enhancement corrected for multiple comparisons) are located in the left inferior fronto-occipital fasciculus, left anterior thalamic radiation and uncinate fasciculus. The significant regions were filled in using tbss_fill in FSL to improve visualisation.
Association between head impact exposure and pre-season to post-season DTI alteration
Similar to the correlation analysis performed to the larger non-collar group with both pre-season to post-season DTI (n=22), the potential association was assessed between the head impact exposure experienced during the season and the pre-season to post-season changes in MD, AD and RD in this subset of non-collar group (n=11). DTI values (MD, AD and RD) were extracted from the entire WM regions that presented significant longitudinal change during the season in the non-collar group (n=11). Among the three head impact variables (number of hits, cumulative g-force, average g-force/hit) at different g-force thresholds, only the total number of head impacts showed a moderate but insignificant correlation with the pre-season to post-season change in MD and AD (r=0.55, p=0.08; r=0.56, p=0.07, respectively). Among the 10 WM tracts within the regions that presented significant pre-season to post-season DTI changes in the non-collar group (table 7), four showed statistically significant correlations between the change in AD and the total number of hits (left cingulum, left SLF, left IFOF and left UF (table 7, supplementary figure S3). In addition, the left cingulum and the left SLF also presented significant correlation between the MD change and the total number of hits (table 7, supplementary figure S3).
Supplementary file 3
Discussion
The current investigation evaluated WM microstructural alterations between collar-wearing and non–collar-wearing groups of female high school soccer athletes after a season of play. At the end of the season, the non-collar group was found to have significant alterations in WM integrity based on DTI-derived metrics which were associated with the number of head impacts experienced during the soccer season. These WM alterations (non-collar subgroup with off-season follow-up) reversed towards pre-season baseline during the 3-month off-season period. Although one might interpret alteration in WM integrity to be a mild perturbation that would quickly normalise, their persistence (yet with reversal towards normal) at 3 months post-season might indicate an ‘injury and attempted repair’ mechanism that is not transient and could indicate long-term cumulative effects.
WM alteration in contact/collision sports with repetitive subconcussive head impact
There is active debate whether anatomical change or long-term clinical effects occur because of head impacts exposure from soccer. In a study of retired professional soccer players, a self-report questionnaire found no evidence that heading the ball led to accelerated cognitive deficiencies or dementia among the athletes.34 In a 5-year prospective evaluation of the sequela of soccer head impacts using standard MRI and neurocognitive techniques, soccer participation had no effect on any of the measured values.34 35 Both of these studies34 35 used the clinical endpoint of ‘concussion’, and neither used the advanced techniques of measuring microstructure and function as implemented by Svaldi et al and the current study.36
The results from our recent neuroimaging studies of head impact exposure in male football players not wearing a jugular vein compression collar show a consistent pattern of pre-season to post-season change based on MD, AD and RD, but not in FA.10 28 While it is possible that preliminary results from our soccer and football studies indicate that FA is less sensitive (based on high intrasubject variance) than AD or RD metrics in quantifying the anatomical effects of repetitive head impacts, the evidence more strongly supports that the lack of sensitivity of FA in prior longitudinal studies is attributed to the variable chronicity (or timing in relation to the end-of-season imaging endpoint) of the head impacts. In general, relatively more recent (ie, acute mTBI) and thus, later in season, head impacts are associated with elevated anisotropy values,24 37 while relatively more remote (ie, chronic mTBI) or longer-term head impact exposure (eg, earlier or during the entire competitive season) are associated with depressed anisotropy.10 37 In prospective longitudinal investigations, the head impacts experienced during the season may exert differential effects on the direction of FA change depending on the timing of the impacts relative to the end of the season when FA is measured. Based on our prior evaluations of football data and the current study results in females for the non-collared groups, the DTI metrics RD, AD and MD provide the best sensitivity and specificity to quantify brain injury from repetitive head impacts sustained from competitive play. It is speculated that any change in diffusivity from pre-season could be interpreted as effects from injury and attempted repair mechanism representing accumulating effects over the entire competitive season with head impact exposure.
Notably, the location of the changes in the female soccer athletes’ WM in the current study are of particular importance given that the mechanism of impact in most soccer headings is through a manoeuvre of thrusting the forehead into the ball (although an impact to any area of the skull is possible).38 Our findings of changes involved many important WM tracts, including ATR, cingulum, forceps minor, SLF, IFOF and UF, which are frequently reported to be abnormal in response to TBI, blast-related brain injury and sports-related concussion.9 19 39–47 These are prominent WM fibre tracts that are located in the frontal lobes and connect directly with the frontal and prefrontal brain regions. They are implicated in planning complex cognitive behaviour, personality expression, decision-making and moderating social behaviour, long-term memory, visual perception and spatial attention.48 More diffuse alterations in WM have been reported following competition in ice hockey and football.10 24 This correlation of DTI findings with the suspected mechanism of impact location lends further credence to our hypothesis that the mechanism of action, from the internal jugular vein compression, can reduce force impartation to the brain from head impacts and help ameliorate DTI changes is consistent across sexes and sport. The potential risk of WM injury should be considered in the context of the developing WM pathways in youth and adolescent age female athletes.49 Females demonstrate sex and age interaction in brain development that differ from males, some of which indicate that female brain development occurs earlier than males with most differences observed at age 13–15 or younger.50–52 During maturational periods, axonal diameter growth, thickening of the myelin sheaths and increases in WM organisations continue and lead to optimisation of signal transduction allowing for cognitive, emotional and motor skill development.49 53 54 Therefore, in the context of potential sports-related head injury and alterations to brain microstructure, it is important to investigate maturing female athletes to characterise the potential WM alterations during a crucial developmental window while they are involved in competitive contact sports with frequent head impact exposure.
Association between WM alteration and head impact exposure
We report correlation quantitatively between head impacts and alteration in DTI representation of brain microstructure in several WM tracts (ATR, forceps minor, SLF, cingulum, inferior longitudinal fasciculus, UF). This finding may suggest that these frontal regions are vulnerable to the subconcussive, repetitive head impacts to which female soccer athletes were exposed. However, it is important to note that there might be a number of other factors that can alter cortical functioning but are not fully understood. Based on the findings derived from the football and current soccer studies,10 the WM regions with significant pre-season to post-season MD, AD or RD reduction in the non-collar group sometimes co-localise at the same region.10 An AD reduction is often interpreted as a compromise of integrity in the axonal membrane55–57 while a RD reduction has been found to be associated with extracellular space compression, cytotoxic oedema (axonal swelling) or inflammation.58 59 Simultaneous AD and RD reduction will change the diffusivity of water molecules in both longitudinal and cross-sectional directions of WM fibre, but in the meantime, this may not significantly change the degree of directional coherence (which is what FA reflects).
Sensitivity of different DTI measures in detecting WM alteration in SCI
We did not anticipate that the standard deviation of FA was more than 100 times higher than that for AD, MD and RD in the reliability analyses of regions of interest (baseline to pre-season). FA measures may be more reliant on fibre orientation and crossing fibres and therefore be more susceptible to having the effects of repetitive head impacts masked.60 However, the results from this current study might indicate that FA is relatively less sensitive than AD or RD metrics in quantifying the effects of repetitive subconcussive head impacts. Another possible interpretation for the lack of sensitivity of FA in this study may be attributed to the variable chronicity in the head impacts. In general, relatively more acute mTBI and potentially subconcussive head impacts are associated with elevated anisotropy values24 37 while relatively more chronic mTBI symptoms or longer-term head impact exposure (eg, entire competitive season) are associated with depressed anisotropy.10 37 In the current study, the head impacts experienced during the season may exert differential effects on the direction of FA change depending on the timing of the impacts relative to the end of the season when FA is measured. Based on correlative animal studies with histology, decreased RD found in the non-collar participants may be associated myelin pathology while the changes in AD are speculated to be indicative of axonal damage (decreased diffusion along the parallel axis of the axon).61 The current DTI changes from a competitive season in soccer in combination with prior results in football indicate that both RD and AD (and MD by virtue of its associative calculation) may be needed to evaluate the underlying pathological processes associated with repetitive head impacts in sport.
Female soccer athletes who wore collars appeared to be protected from brain imaging change associated with repetitive SCI
The longitudinal DTI scans of the young female soccer athletes who wore jugular vein compression collar devices when exposed to head impacts, both post-season and at the 3-month off-season follow-up evaluation period, showed no change in their WM DTI metrics. Studies examining sTBI using DTI to report WM alterations varies in off-season follow-up period anywhere from 3 months to 1 year post-sTBI event. Such WM alterations have also been observed in studies examining football players after being exposed to a season of SCI, as reported DTI changes persisted 6 months post-season.14 28 Similar investigations using fMRI in a cohort of football athletes showed that it took between 2 and 4 months of post-season rest for full functional reversal to occur.62 63 Relevant to the current study, Svaldi et al reported cerebrovascular reactivity alterations persisted in female soccer players 4–5 months post-season64; however, the WM alterations showed significant reversal towards normalisation in our off-season follow-up based on DTI in the present study. This supports the notion that WM alterations noted in the current report could also be indicative of ‘injury’ with subsequent reversal in directionality reflecting the biological systems repair to itself (figure 10).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![[bjsports-2018-099571supp001.jpg]](https://bjsm.bmj.com/content/bjsports/53/24/1539/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
![[bjsports-2018-099571supp002.jpg]](https://bjsm.bmj.com/content/bjsports/53/24/1539/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
![[bjsports-2018-099571supp003.jpg]](https://bjsm.bmj.com/content/bjsports/53/24/1539/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
Longitudinal trajectories of normalised diffusion tensor imaging measures over the four time points (using pre-season as reference) in the 11 participants in the non-collar group and 11 participants in the collar group. *Post-season is significantly lower than the pre-season and the **off-season follow-up is significantly increased relative to post-season but were still significantly reduced relative to the pre-season measurement. AD, axial diffusivity; FA, fractional anisotropy; F/U, follow-up; ICC, intraclass correlation; MD, mean diffusivity; RD, radial diffusivity.
Limitations of the study
One of the limitations of the current study given that the focus was the female athlete was its inability to account for hormonal fluctuations of the studied population. In particular, hormonal cycling could introduce confounding variables affecting intracranial pressure and volume of female populations.65 Others suggest that the presence of progesterone acts in a neuroprotective capacity by improving the intracranial pressure after a TBI and dampening its impact.66 67 This may underlie decreased recovery time and improved neurological outcomes in women injured during the luteal phase of their menstrual cycle, when progesterone levels were at their highest, compared with women who were either on birth control or in follicular phase of their menstrual cycle, when progesterone secretion was lowest. Another consideration was that DTI changes were not tied to assessments of athlete behavioural outcomes, that is, symptoms, physical or cognitive function. While prior studies have indicated that accelerometry devices affixed in helmets have the potential for up to 10%–40% measurement error, the current study employed accelerometers affixed directly to the mastoid which may reduce false-positive measurement of accelerations driven from the problems affixing to the study participants’ helmets.68 69 The current use of accelerometry was focused primarily to monitoring group exposure to head impacts, but with the associations noted with changes in WM microstructure, further efforts to achieve algorithmic solutions to accelerometry measurement error, for example, combining and synchronising video information with wearable sensor recording to cross-verify head impact events, are warranted to verify the current associations.70
Conclusion
We reported DTI neuroimaging findings in female high school soccer athletes after a full-season exposure to repetitive SCI. Changes in diffuse WM regions were found in the players who did not wear a jugular vein compression collar, and these changes were associated with head impacts as measured by head-mounted accelerometry. The significant DTI alterations in the non-collar group partially reversed towards baseline in 3 months post-season, implying damage and repair mechanisms. The specialised neck collar that provided jugular vein compression during head impact exposure appears to have helped to preserve WM integrity in these female athletes during their competitive season.
What are the findings?
Prospective neuroimaging modalities provide an objective imaging biomarker to quantify longitudinal white matter (WM) structural changes in female soccer players.
Female athletes who did not wear the jugular vein compression collar had significant pre-season to post-season decreases in mean diffusivity, axial diffusivity and radial diffusivity in extensive WM areas.
Female athletes wearing a jugular vein compression collar did not show similar WM changes.
WM changes in athletes not wearing a jugular vein compression collar partially resolved at 3 months off-season follow-up lending support to the contention that these WM changes may be pathological.
How might it impact on clinical practice in the future?
The prefrontal brain regions may be vulnerable to subconcussive, repetitive head impacts that are part of female soccer.
Our data support a call for replication studies and further clinical trials to determine whether there are benefits from jugular compression to prevent symptom and alterations to brain microstructure and neurofunction from concussive level head impacts.
Acknowledgments
The authors would like to thank from Seton High School: Ron Quinn, Lisa Larosa, Holly Laiveling and the entire soccer coaching staff as well as the Seton administration and athletic director Wendy Smith; from Madeira High School soccer head coach Dan Brady, athletic director Joe Kimling and principal David Kennedy for their support and assistance to conduct this study. Thank you to the soccer parents and players. We appreciate their patience with the testing scheduling, follow-ups and equipment additions. Their enthusiastic support made this study possible. Special acknowledgement goes to the Athletic Trainers at Seton High School, Cindy Busse and Madeira High School, Glenna Knapp. Without their time, commitment and passion for the health and well-being of their student athletes, this study would not have been possible. We would also like to thank University of Cincinnati interns Casey McCall, Danielle Reddington, Preston Heath and Jacob Snyder for their assistance with the daily accelerometer tracking. We would like to thank Dustin Grooms from Ohio University and Johnny Ellis from the University of Cincinnati for their help in MRI protocol improvement and data collection. The authors would like to thank Priotity Designs, specifically Jamison Float, who provided fitting and technical support for the Q-Collar, and James Lua and James Rowland who provided data visualization graphics. The authors would also like to thank Lacey Haas, Brynne Williams, Kaley Bridgewater and Matt Lanier in the Imaging Research Center as their support made this study possible.
References
Footnotes
Twitter @gregmyer11
Contributors GDM contributed to the conception and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, obtaining funding and supervision. KDBF contributed to acquisition of data, drafting of the manuscript, and administrative, technical or material support. ST contributed to acquisition of data, drafting of the manuscript, and administrative, technical or material support. RG contributed to acquisition of data, drafting of the manuscript, and administrative, technical or material support. CDC contributed to acquisition of data, drafting of the manuscript, and administrative, technical or material support. JD contributed to acquisition of data, drafting of the manuscript, and administrative, technical or material support. BG contributed to acquisition of data, drafting of the manuscript, and administrative, technical or material support. JL contributed to conception and design, critical revision of the manuscript for important intellectual content, and analysis and interpretation of data. DS contributed to conception and design, drafting of the manuscript and material support. PG contributed to conception and design, critical revision of the manuscript for important intellectual content, and analysis and interpretation of data. WPMIII contributed to conception and design, critical revision of the manuscript for important intellectual content, and analysis and interpretation of data. MA contributed to the analysis and interpretation of data, critical revision of the manuscript for important intellectual content, and statistical analysis. PL contributed to the analysis and interpretation of data, critical revision of the manuscript for important intellectual content, and statistical analysis. WY contributed to conception and design, critical revision of the manuscript for important intellectual content, and analysis and interpretation of data.
Funding The authors acknowledge funding support from The Heidt Family Foundation, Robert S Heidt Sr Wellington Foundation and Q30 Sports Sciences, LLC.
Competing interests DS is the inventor of the Q-Collar approach and has financial interest in the results of the current research. One author (GDM) consults for Q30 Innovations to support applications with the US Food and Drug Administration but has no financial interest in the commercialization of the Q-Collar. Q30 Sports Sciences has financial interests in the development of the Q-Collar.
Patient consent Obtained.
Ethics approval Cincinnati Children’s Hospital Medical Center IRB.
Provenance and peer review Not commissioned; externally peer reviewed.