Article Text

Abstract
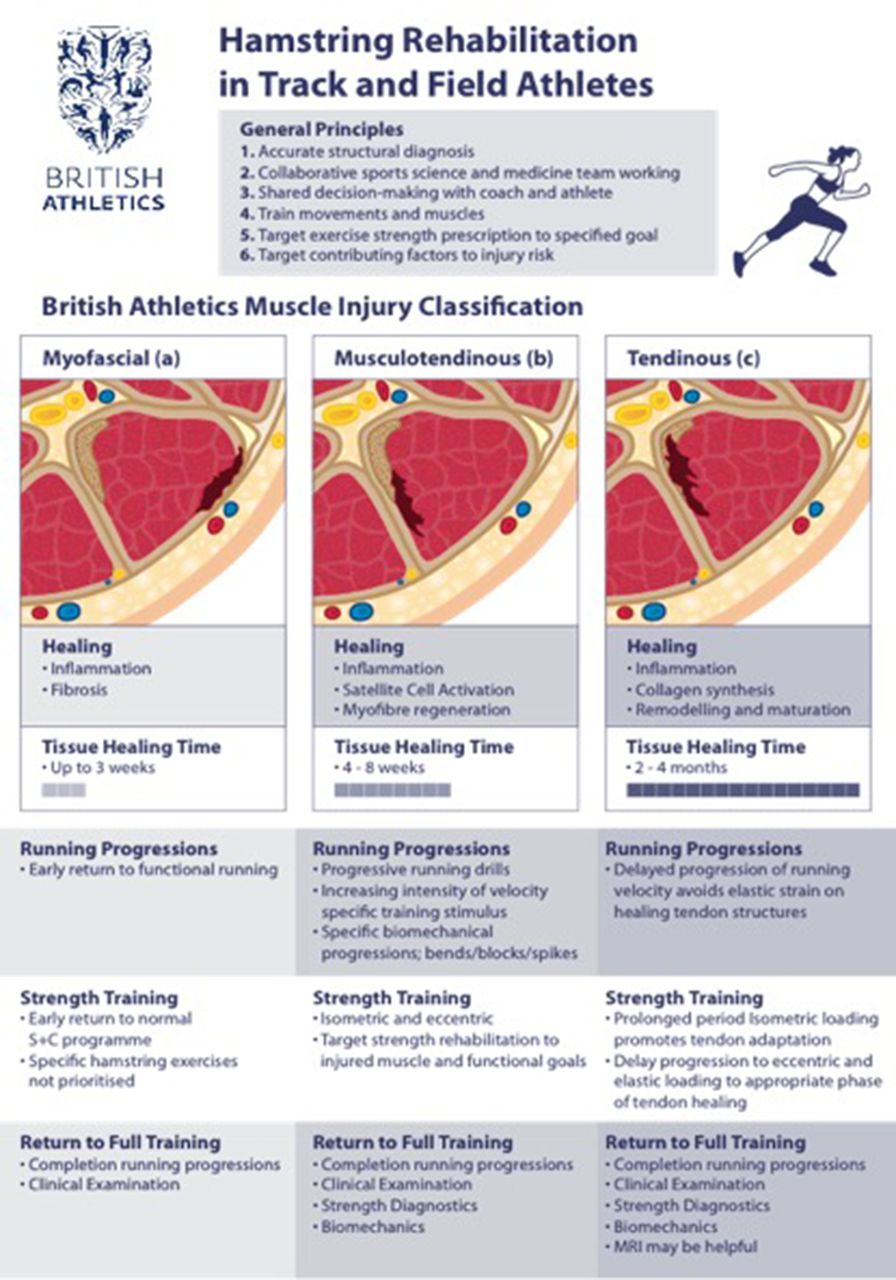
Rationale Hamstring injuries are common in elite sports. Muscle injury classification systems aim to provide a framework for diagnosis. The British Athletics Muscle Injury Classification (BAMIC) describes an MRI classification system with clearly defined, anatomically focused classes based on the site of injury: (a) myofascial, (b) muscle–tendon junction or (c) intratendinous; and the extent of the injury, graded from 0 to 4. However, there are no clinical guidelines that link the specific diagnosis (as above) with a focused rehabilitation plan.
Objective We present an overview of the general principles of, and rationale for, exercise-based hamstring injury rehabilitation in British Athletics. We describe how British Athletics clinicians use the BAMIC to help manage elite track and field athletes with hamstring injury. Within each class of injury, we discuss four topics: clinical presentation, healing physiology, how we prescribe and progress rehabilitation and how we make the shared decision to return to full training. We recommend a structured and targeted diagnostic and rehabilitation approach to improve outcomes after hamstring injury.
- hamstring
- rehabilitation
- muscle injury
- sprinting
Statistics from Altmetric.com
Introduction
Hamstring injuries are common in sports requiring kicking, high-speed running and sprinting, and are a significant cause of missed training and competition.1–4 In a series of international track and field competitions from 2007 to 2015, muscle injury represented 41% of all injuries and the hamstring was the most commonly affected muscle group.5
Muscle injury classification systems have provided a framework for muscle injury diagnosis.6–8 While the Munich muscle classification consensus has been implemented in elite soccer players,9 10 its classification entities have structural and functional elements that are not clearly defined, limiting its utilisation. The British Athletics Muscle Injury Classification (BAMIC) describes a MRI classification system with clearly defined, anatomically focused classes based on the site of injury: either myofascial (a) muscle–tendon junction (MTJ) (b) or intratendinous (c) and the extent of the injury, graded from 0 to 4 (figure 1).7 British Athletics is a national governing body that provides expert clinical support to elite track and field athletes.

Overview of British Athletics Muscle Injury Classification by anatomical site in biceps femoris injury.
The BAMIC has been validated in two studies demonstrating substantial intra-rater and inter-rater reliability.11 12 A retrospective clinical study demonstrated that for the different classifications, athletes’ times to return to full training (RTFT) varied with tissue type involved and the extent of injury.13 In particular, return to sport was delayed, and recurrence rates increased, with intratendon hamstring injuries. A difference in return to play and/or re-injury rates with intratendon hamstring injury has previously been identified,14–18 although its relevance may vary between different sports. Several rehabilitation programmes have been published for hamstring injuries but despite evidence that the intratendon injury may have a different prognosis, and that the different hamstring muscles have distinct actions, none of the rehabilitation programmes describe targeted guidelines relating to specific diagnoses or injury classification.19–25 Most muscle treatment guidelines describe rehabilitation with regard to healing phases (acute, subacute and regeneration) and functional rehabilitation progression24 but there has been limited comparison of different protocols.23 25 26
In this two-part paper, we (i) review the general principles of hamstring injury rehabilitation in British Athletics, and (ii) we discuss how we apply those principles to the three BAMIC subtypes of hamstring injuries
Part 1: General management principles of hamstring injury rehabilitation in British Athletics
Management principle 1
Establish an accurate structural diagnosis and injury classification
After an athlete suffers an acute hamstring injury, The British Athletics medical team prioritises initial clinical assessment—which includes injury history and clinical examination. This is followed by imaging with ultrasound and MRI within 72 hours to determine a structural diagnosis and classification (BAMIC). There is evidence from different sports that tendon involvement in muscle injury increases return to play or re-injury,13 14 17 18 27 28 and that clinical examination may not be able to discriminate the presence of tendon injury.29 While there are additional reasons to perform MRI,30 we believe the detection of the intratendon injury warrants MRI in the management of elite athletes.
We consider that MRI diagnostics, in isolation, are limited in providing an accurate prognosis. In some sports or athletes, including a recent study performed in Qatar, an intratendon injury may only have a moderate impact on time to return to play.18 However, the BAMIC provides a framework for clinical reasoning and rehabilitation decision-making. Different tissues, such as fascia, muscle and tendon, differ in their rates of healing and response to load following injury.31 We believe these tissues will respond optimally to specific rehabilitation strategies within a multifaceted and criteria-based system of progression.24
Management principle 2
Facilitate the collaborative expertise of the sports science and medicine team
The British Athletics sport science and medicine team collaborate within an integrated health and performance model.32 In injury management, roles and responsibilities are defined and the team aligned with the health and performance aims of the rehabilitation process. The BAMIC framework enables targeted sports medicine and science strategies. For example, the performance nutrition and medical team provide targeted nutrition, pain management or other strategies depending on the class of injury, supporting optimal adaptation to exercise for specific tissues.33–37
Management principle 3
Involve the coach and athlete in shared decision-making
British Athletics apply an integrated performance health and coaching model and a shared decision-making process when managing injuries in elite track and field athletes.32 38 This model aligns the health and coaching departments to a defined performance goal. When managing injury, the role of the medical team, in British Athletics a sports physician and physiotherapist, is to provide the coach and athlete with ongoing expert information regarding the diagnosis, benefits and risks of proposed management strategies. The medical team’s mission is to maximise the availability of athletes for full training to increase the likelihood of winning medals at the major championships. The risk of re-injury during rehabilitation and RTFT is an important factor in the shared decision-making process. A fully informed high-risk approach may be agreed on by all the participants when there are certain performance goals (eg, success at the Olympic Games).38
Management principle 4
Train movements and muscles
The hamstrings consist of three individual muscles, each of which have functional roles related to their anatomy, and demonstrate various electromyography (EMG) patterns and MRI spatial characteristics in response to exercise stimulus.39–44 In sprinting, bicep femoris (BF) is subject to the largest strain, semitendinosus (ST) the greatest lengthening velocities, whereas semimembranosus (SM) acts predominantly as a force producer.43–45 BF is activated more during the acceleration phase of sprinting and terminal swing, ST during maximum-velocity sprinting, whereas SM has an important role in absorbing and generating power in swing and stance.44 46 47 Therefore, exercise prescription should be targeted to the injured muscle to develop these specific functional roles and limit the altered spatial characteristics demonstrated post-injury.48
Sprinting is a complex, coordinated movement, and restoring normal movement patterns is essential. Cameron et al 49 50 discussed the importance of motor control on hamstring injury risk, and the use of running drills in warm up as an intervention. Progressive running drills will load the hamstring in a functional manner, with a gradual increase in velocity of movement and lengthening of the muscle, both of which are important loading characteristics.51 Altered hip and pelvis kinematics, including a reduction in hip flexion52 and an increase in anterior tilt of the pelvis53 have all been noted post-hamstring injury. Increased hip flexion54 and the ability to apply force in a horizontal direction55 are key determinants of high-speed running, and running drills can be used to retrain these elements.56
Management principle 5
Prescribe strength exercises to achieve a specific goal
The complexity of hamstring function is well recognised, both in relation to the anatomical specialisation of the muscle43 and its role in high-speed running.57 While eccentric muscle function is crucial during maximal velocity running, other hamstring adaptations may require alternative strength training stimuli, particularly isometric loading, which has recently been advocated.57 58 The primary mechanisms by which eccentric and isometric loading may positively affect hamstring function will now be discussed, and examples of exercise variations are available online on the B ritish Journal of Sports Medicine website.
Eccentric training
Develop high eccentric force
Eccentric forces are high during the sprinting cycle, especially at terminal swing phase,59–61 and eccentric force deficits and asymmetries are associated with risk of future hamstring injury.62–66 The ability to produce high eccentric force lowers the relative risk imposed by increasing age and previous injury history—factors considered as non-modifiable.66 Therefore, eccentric training (figure 2) is a key part of the prevention and rehabilitation of hamstring injuries—and is integral in conditioning for athletes who sprint.26 62 67–69

Eccentric phase of the single leg Romanian dead lift.
Increase fascicle length to enhance the length–tension relationship (get long and strong)
Hamstring injury predisposes the muscle to architectural changes (fascile shortening) that may predispose athletes to re-injury.70–74 Eccentric training increases fascicle length72 which may also lower the injury risk associated with non-modifiable risk factors.74 Increasing fascicle length may protect against future injury by shifting the angle of peak torque to longer muscle lengths.75–78
While high-volume eccentric training programmes using the Nordic hamstring exercise (NHE) have demonstrated good improvements in eccentric strength and fascicle lengthening, recent studies have demonstrated similar improvements with a low-volume programme consisting of two sets of four repetitions once a week.72 79–81 These lower training volumes may make the inclusion of eccentric exercise less of a challenge within the athlete’s strength programme, especially while in competition phases. This may help to prevent the detraining effect on fascicle length improvements demonstrated after 2 weeks of ceasing eccentric loading.82
Isometric training
Develop muscle–tendon unit specificity
The contractile element of the hamstrings may remain relatively isometric at end swing phase, with muscle–tendon unit lengthening being provided by the tendon.57 59 60 83 The isometric condition of the muscle fascicles reduces mechanical work done by the contractile component, facilitating the spring-like behaviour of the tendon during the stretch shortening cycle.84 High-load isometric training may therefore provide a more specific stimulus related to this functional demand.57 However, further evidence is required to confirm these processes, and eccentric loading may also cause a similar isometric condition of the muscle fascicles, despite an overall increase in muscle–tendon unit length, similar to that shown in the triceps surae.85 86
Develop fatigue resistance
Fatigue is consistently associated with hamstring injury3 87 88 and has been demonstrated to impair neuromuscular function.89–91 Hamstring re-injuries are more common in football players with strength-endurance deficits,48 with injured muscles fatiguing earlier and demonstrating altered activation patterns.92 Our injury audit observations at British Athletics are consistent with these findings and have demonstrated an increased incidence of injuries occurring in the final third of sprint training sessions. Strength training of the hamstrings under fatigue has demonstrated positive effects on hamstring function and reduced injury rates.93 94 While suggested protocols for the NHE include multiple repetitions, it is usual to have a brief rest period between repetitions as the athlete returns to the starting position. The Single leg Roman Chair hold (figure 3), with longer duration muscle contractions, is more effective at increasing hamstring muscle endurance than the Nordic curl.58 This suggests that isometric training may be a useful addition alongside eccentric loading to condition the hamstrings, when improving fatigue resistance is the desired training adaptation.

Example of isometric exercise: single-leg Roman chair hold.
Overcome selective muscle inhibition
Athletes with a history of hamstring injury exhibit both acute and chronic responses to pain causing maladaptive neural responses in the central nervous system.40 In the initial stages post-injury, it has been suggested that reduced myoelectric activity in the muscle serves as a protective mechanism to unload the healing tissue.95 However, longer-lasting selective inhibition of the hamstrings during eccentric actions has been reported, and may compromise rehabilitation and muscular adaptation.96 Specifically, chronic activation deficits during the Nordic curl post-injury have been reported with reduced hamstring activity as the knee approaches terminal extension.97 It is possible that isometric training may avoid the inhibitory mechanisms that occur during eccentric conditions, as voluntary muscle activation has been shown to be higher during isometric contractions.98 A reduction in cortical inhibition, with associated increased motor unit activation, has been demonstrated in patellar tendon pain subjects completing isometric exercise.99 100 We therefore advocate using high-load isometrics, particularly in injuries when pain and disability are greater, to improve motor unit recruitment, prior to implementing eccentric loading.
Management principle 6
Apply a multivariate model and target contributing factors to injury risk
There are numerous potential risk factors for hamstring injury which interact in a complex way increasing risk in any individual athlete.101 Rehabilitation of a hamstring injury is an opportunity to apply clinical reasoning and address potential risk factors which may be present in the training programme, musculoskeletal system and/or athlete lifestyle. A broad discussion of all these potential risk factors is beyond the scope of this paper. However, we highlight two factors that are an important focus in our clinical management of hamstring injuries.
Spine
Although there is limited evidence to endorse lumbo-pelvic training,102 we consider that appropriate management of the spine and lumbo-pelvic function should be a component of hamstring injury rehabilitation. The hamstrings perform a stabilising role on the pelvis with attachments to the sacrotuberous ligament.103 Abberant motion of the pelvis or a loss of force closure may increase strain on the hamstrings,83 104–108 and may contribute to deficits in hamstring force production.109 There is a lack of evidence to support any one lumbo-pelvic neuromuscular training intervention.110 We advocate a holistic strength training programme of the lumbo-pelvic region that targets specific biomechanical planes of movement (table 1). While no gold standard exists for measuring abdominal function,102 and the reproducibility of common motor control tests is questioned,111 tests such as the active straight leg raise have demonstrated reliability and validity,112–114 and can be used to assess improvement in lumbo-pelvic function following a training intervention.
Lumbo-pelvic re-training
While there is no direct evidence demonstrating the efficacy of managing spinal pain in hamstring rehabilitation, we believe that the concept of arthrogenic muscle inhibition, widely recognised in knee pathology,115 should be considered in the management of hamstring injury. A previously described association between spinal pain and pathology and increased risk of hamstring injury supports this consideration.116 Manual therapy has been shown to positively affect a range of lumbo-pelvic biomechanical and pain characteristics.117–120 This may be relevant given the role pelvic function has on optimising sprint mechanics and the length–tension relationship of the hamstring.57 83 121 At British Athletics, we have also used spinal epidural or nerve root corticosteroid injections to positively improve hamstring function with the intention of reducing spinal inhibition of the hamstring muscle.9 122–124
Hip
The hip is crucial for optimal hamstring function. Weakness and reduced activation of the gluteus maximus have both been cited as injury risk factors.125–127 The incidence of femoroacetabular impingement (FAI) morphology is high in the athletic population, and a common symptom is a reduction in hip flexion.128–131 This is important given that attaining high hip flexion angles is considered a critical determinant of high-speed running.54 A potential complication of reduced hip flexion during sprinting is a compensatory increase in pelvic rotation which may subsequently increase strain on the hamstring.132 Non-surgical management of symptomatic or restrictive FAI morphology should be considered in hamstring injury rehabilitation.
Part 2: Specific hamstring injury rehabilitation guidelines based on the BAMIC
We aim to incorporate the principles described above into the rehabilitation of all hamstring injuries but we adjust the timing and balance of the rehabilitation programme depending on the specific BAMIC class. Within each class, we discuss four topics: clinical presentation, healing physiology, rehabilitation progression and RTFT. We provide guidance on exercise prescription in tables throughout, however given that individuals vary in how they heal and adapt to resistance training,133–137 appropriate clinical reasoning is reccommended for the individual athlete. 133–137
Class a: Myofascial
Clinical presentation
Myofascial injuries may present with a sudden or gradual onset of posterior thigh pain during, or occasionally after, a training session or competition. We noted that range of movement (ROM) and strength testing were often maintained, despite the presence of pain on manual muscle tests, particularly in comparison to equivalent grade injuries in b or c classes. We speculate that clinical manual muscle testing is less affected as fascial tears predominantly affect the myofascial expansions connecting the deep fascia to the epimysium with relative sparing of the contractile element of the muscle–tendon unit.138 Tracking of oedema between the fascial layers, which is characteristic of this injury at the fascial interface,6 7 139 may result in pain and palpation tenderness over a non-specific and wide area as the fascia is richly innervated.138
Healing physiology
Fascia provides stability and dissipates tensional stress, contributes to pain mechanisms, as well as facilitating coordinated movement.138 It consists of multiple layered sheets of richly innervated collagen fibres which enclose muscle groups.140 Hyaluronic acid between the fascial layers enables sliding between the epimysium and deep fascia.138 Fascial healing is different to muscle and tendon. A recent consensus statement on fascial tissue research describes healing through an initial inflammatory phase followed by a fibrotic stage after fascial injury.141 Fascial wound healing studies suggest that after 7 days fibroblasts are the majority cell type, collagen synthesis has peaked, and that the healing scar tissue has reached half of maximal strength before returning to full strength by 3 weeks.140 142
Loading progression
Running progressions
The most frequent grade of (a) class myofascial injuries are small 1a injuries and that has been used as an example for this discussion.13 Grade 2a (and particularly 3a) injuries occur less frequently but the principles of progression and monitoring are the same. With relatively fast fascial healing time frames, and an intact muscle–tendon unit, initial management is characterised by quick progression back to functional activities, emphasising an early return to running drills. Pain management strategies, such as oral analgesia or manual therapy, may be employed to support this functional return. As the athlete may reduce hip flexion as a protective mechanism to reduce strain on the healing hamstring, we encourage them to gradually increase the degree of hip flexion, and the velocity with which the hip is extended, progressively through rehabilitation. Running drills precede high-speed running and can be progressed even in the presence of moderate pain levels (eg, 4–5 out of 10 on visual analogue scale), which usually dissipates over the course of the first week. We have shared some key areas the athlete should focus on when performing drills (figure 4). Please see the full description and online supplementary videos (online supplementary appendix 1).
Supplemental material

Technical cues during running drills.
A typical progression of technical drills and running sessions for a Grade 1a injury in a 400 m runner is described in table 2.
Example of running progressions for a female 400 m runner with 1a biceps femoris injury
Strength training progressions
As the contractile element is intact, and strength is often well maintained, specific hamstring loading is not prioritised. Instead, we emphasise a return to the athlete’s normal strength training programme, including appropriate hamstring loading, alongside the running drill progression. As a result, less disruption to normal training programmes is seen in this class of injury, as rehabilitation takes on a functional emphasis.
RTFT decision-making
Class a injuries tend to have a quick recovery time.13 RTFT is primarily based on the clinical examination of ROM, strength, palpation pain and Askling H-test143 (table 3), alongside the successful progression of running without exacerbation.144 The clinical information is provided to the RTFT decision process and these injuries usually represent a low risk of re-injury.13 38
RTFT progression specific to diagnostic class
Class b: MTJ
Clinical presentation
Class b injuries occur at the MTJ,7 13 typically as a sudden onset mechanism during high-velocity sprinting or jumping.15 The force generating capacity of the muscle is impaired as contractile function is diminished. Contractile testing usually reveals pain and weakness, and ROM is reduced, as the injured fibres are painful to stretch.145
Healing physiology
Muscle injury induces a satellite cell response and early scaffold on which muscle regeneration can occur, enabling early return of muscular function.146 Evidence from healing physiology research suggests that the functional scar is no longer the weakest point of the muscle at approximately day 10 post-injury. Maturation of type 1 collagen is well underway by early in the third week, with myofibre regeneration by the end of the third week.146 Understanding this satellite cell response, myofibre regeneration and scar scaffold provide the basis for optimal loading, and interventions from the sports science and medicine team, such as nutritional or heat strategies, to support this physiological recovery of muscle–tendon unit function.
Rehabilitation progression
Running progressions
Running drills are introduced as walking becomes pain free, in agreement with previous reviews.19 20 Running progression is not usually as quick as the class (a) myofascial injuries, due to muscle fibre disruption. Greater emphasis is placed on keeping pain to a low level (below 3 out of 10 on a visual analogue scale) during drill execution in comparison to class (a) injuries. Dynamic drills commence as clinical markers of strength and ROM improve (approximately day 5 for a 2b injury). Drills with low hamstring elongation stress are used at a time when tissue healing is in the acute stage.51 Completing drills of increasing volume and intensity (online supplementary appendix 1), and further improvement in the clinical markers of ROM, strength and a negative Askling-H test (table 3), are milestones for us to introduce higher speed running (table 4). Specific biomechanical demands are placed on the hamstrings during bend running, spiked running and block starts, and these are key sport specific functional progressions within late stage rehabilitation.147–149
Running progressions in male 100 m and 200 m sprinter with 2b biceps femoris injury
Strength training progressions
In our experience, the most commonly injured muscle group in class (b) injuries is the long head of BF, which is consistent with data from other reports.145 150 151 Numerous studies report different spatial recruitment patterns between exercises, with hip dominant exercises loading the proximal hamstring and knee dominant exercises loading the distal hamstring.40 42 75 152 153 The ratio of lateral to medial hamstring activation is higher for hip-based exercises such as the single-leg Romanian dead lift, 45° hip extension and Glut-Ham raise154 due to the greater moment arm at the hip providing a mechanical advantage.155 This may promote greater hypertrophy in BF than knee dominant exercises such as the Nordic curl.80 However in absolute terms, the Nordic curl provides the greatest EMG activation of BF and therefore both hip and knee training interventions are required.154 An example of potential training progressions with targeted adaptations for a 2b BF injury is described in table 5. It includes a combination of hip and knee dominant exercises, eccentric and isometric variations, and exercises that will develop both high force, fatigue resistance and high strain characteristics. Initial exercise prescription is at higher volumes and lower load, with a gradual increase in load through rehabilitation as tissue tolerance improves. It is important to increase load to optimise hamstring adaptation.156 Increased load is accompanied by a reduction in strength training volume as running intensity/volume increases to achieve more performance-based goals (tables 5 and 6). Successfully tolerating each stage of progression allows further progression in load magnitude and muscle length, using clinical markers of ROM, strength, pain on palpation and area of palpation tenderness to monitor reaction.
Hamstring loading progressions for 2b distal biceps femoris injury
Running progressions in a female sprint hurdler with 3c proximal biceps femoris Injury
Weekly programme design is an important consideration for strength training prescription. Reduced levels of hamstring activation have been demonstrated following the performance of a set of Nordic curls.157 Neuromuscular function post-sprint training follows a bimodal recovery pattern, with the initial recovery observed immediately post-training being followed by a secondary decline the following day.158 A decline in neuromuscular performance occurs following concentric exercise when metabolic disturbance is sufficient; however, this recovers quickly and decline in performance does not persist as it does with eccentric exercise.159 160 Together, these findings suggest that high-speed running is not recommended either immediately after or the day following heavy hamstring strength training. However, the addition of a heavy weight training session containing significant eccentric load after high-speed running does not result in increased muscle damage or loss of function.160 Therefore, when considering rehabilitation structure, it is recommended that eccentric hamstring loading is programmed 1–2 hours after high-speed running sessions, with the following day a lower intensity running session, placing less demand on the hamstring.
RTFT decision-making
RTFT testing includes the same clinical and functional processes as class (a) injuries (table 3), but due to the disruption to the muscle–tendon unit, more thorough eccentric strength assessment is also conducted using the Nordbord (figure 5).161 Results of this strength testing are interpreted to pre-injury baseline values of limb symmetry and peak force, as well as event group normative data (eg, sprinter/long jumper).

Nordbord assessment of eccentric hamstring strength.
Class c: Intratendon
Clinical presentation
Class (c) intratendon injuries typically present with a sudden onset, high force mechanism. Although frequently occurring during sprinting, they can also occur during a high-velocity stretch.162 ,163 Initially, class (c) injuries may demonstrate an antalgic gait, and a significant loss of ROM and power. However, in a high-grade (3c) intratendon injury with loss of tension, the clinical presentation may have less pain on palpation and stretch than would be expected with such an extensive injury.29 163 An interesting observation in these injuries is the speed at which clinical symptoms can improve. If significant parts of the contractile element of the muscle–tendon unit remain intact and the intratendon injury is partial, then force production in low-level tasks or clinical assessments may return quickly. As described further below, tendon healing is slow in comparison to muscle and fascia. In addition, Schache et al 164 describe how the tendon provides an increasing role in muscle–tendon unit force production as running speed increases, as the muscle–tendon unit demand increases non-linearly. Therefore, as clinical symptoms settle, if training progresses at too fast a rate, this may pre-dispose the athlete to re-injury at a time when tendon healing is still taking place.13 14 The British Athletics approach to intratendon injury with loss of tension (3c) has consistently been to prescribe structured and targeted conservative rehabilitation. Surgical intervention is not recommended as primary management for this class of injury.
Healing physiology
Tendon healing occurs in a very different way to muscle. Tendon repair is characterised by extracellular matrix deposition and a functionally limited scar that requires collagen synthesis and remodelling for return of tensile strength.165 The tendon remodelling phase, which occurs from around 6 weeks after injury, replaces the early type III collagen and extracellular matrix with longitudinally orientated type I collagen.165 166 Consolidation occurs over the subsequent 6 weeks and maturation over many months.167 This is necessary to restore the tendon stiffness and function required for athletic activity such as elite-level sprinting.
Rehabilitation progression
Running progressions
The rehabilitation framework for 3c injuries provides a longer time at each stage of running progression than those described for a 2b injury, due to slower tendon adaptation. Forces in the hamstring increase non-linearly as the percentage of maximal running speed increases, while the length change in the muscle remains the same.83 At the end of swing phase, tendon elongation may be primarily responsible for this length change.59 Tensile stress placed on the tendon will therefore be high. A gradual increase in running speed will provide this stimulus functionally, as the amount of negative work increases as the percentage of maximal running speed increases.168
To avoid re-injury, a gradual increase in training volume and intensity (table 6) is prescribed with enough time spent at each stage to accumulate high chronic workloads and avoid loading spikes, which is believed to mitigate injury risk.169–172 In 3c injuries, this concept is even more important as the greater severity of injury and subsequent loss of normal training time mean that protective chronic training loads are lost.
Strength training progressions
A body of evidence exists suggesting that during dynamic human movement an increase in muscle–tendon unit length occurs via the passive component (ie, tendon) while the contractile component remains isometric.59 85 168 173 174 As a result, and considering the slower healing physiology described, we recommend that eccentric loading is delayed in class (c) injuries to avoid placing excessive mechanical strain on the healing tendon structures. This is in contrast to other rehabilitation guidelines advocating early inclusion of eccentric loading.175 However, these guidelines do not consider the specific structure injured and how this may relate to healing physiology and muscle–tendon interaction. In a typical 3c injury, this delay is approximately 3 weeks. Given that increases in fascicle length have been shown to occur after only 14 days of eccentric loading,72 we believe that this delay will not negatively affect this adaptation in the overall rehabilitation process.
The primary variables considered during strength training are progressions in load, length and contraction mode (table 7).51 Bohm et al 176 concluded that load magnitude, of greater than 80% maximal voluntary contraction, rather than the mode of contraction, was the key determinant to develop the material and mechanical properties of tendon. Therefore, considering the tendon healing and adaptation process, early eccentric loading will not necessarily provide additional benefit to the healing tendon over isometric loading, but may cause excessive strain when considering muscle–tendon interactions.86 168 Long-term loading (>12 weeks duration) was also identified as a key variable in tendon adaptation, and further supports our belief that these injuries require a longer approach to rehabilitation. The optimal loading frequency for tendon adaptation has been recommended as 36–72 hours between sessions, to ensure that tissue synthesis occurs rather than degradation.177 The location of injury also needs consideration. In the case of a proximal tendon injury, knee-based eccentric exercises are started first to avoid over straining the proximal injury site, progressing to hip-based eccentrics at a later stage as tissue healing progresses (figure 6).75

Example of a knee dominant exercise used in early eccentric loading (A. fly wheel) progressing to a hip dominant eccentric exercise (B. 45° hip extension).
Hamstring loading progressions for 3c proximal biceps femoris injury
RTFT decision-making
The most important measures remain clinical, functional and strength testing for class c injuries (table 3). Given the higher risk of re-injury in class c injuries, and a longer period of modified training, we gather further information to help the RFTF decision-making process (figure 7). This includes biomechanical analysis to compare ground contact times and stride length to pre-injury values, and force plate testing with the strength and conditioning staff to assess whether the strength qualities required for elite sprinting have been met. The judicious use of repeat MRI can assess the appearance of structural tendon integrity which may provide additional information, particularly when an athlete is looking to accelerate the rehabilitation process. A repeat MRI scan within rehabilitation may also provide additional information if the initial MRI had a very extensive high signal intensity pattern that obscured full assessment of tendon integrity. However, MRI appearance may not be a good correlate of tendon or muscle–tendon unit function and MRI appearance should only be one factor that contributes to clinical reasoning. The limited available evidence suggests that use of MRI in return to play decision-making has limited benefit although this has not been specifically evaluated for intratendon injuries.178 The importance of the initial shared decision-making process and agreement on the rehabilitation approach must be emphasised with this class of injury, as at times patience may be required to ensure appropriate tendon adaptation and healing for the reasons already discussed.

Return to full training decision-making.
Limitations to our approach
This paper presents the British Athletics rehabilitation approach to hamstring muscle injuries in an elite athletics cohort. While the clinical reasoning principles are transferable, the rehabilitation approach may not be appropriate for athletes in different sports, particularly those with lower tendon or muscle–tendon unit demand. Further basic science and clinical research is required on the specific structural, healing and functional properties of intratendon injuries, including potential differences between the intramuscular tendon and free tendon. While MRI is unlikely to provide an accurate prognosis in isolation, we believe the modality has value in providing a framework for clinical reasoning and limited value in monitoring rehabilitation progress. The rehabilitation programme we have presented is our interpretation of the available evidence but we recognise that our specific approach requires evaluation and testing in prospective studies.
Summary
This paper outlines the British Athletics approach to the management of hamstring injury rehabilitation with a general discussion on rehabilitation principles and specific rehabilitation guidelines based on the BAMIC, as summarised in figure 8. Since implementing this structured and targeted approach to diagnosis and rehabilitation, our injury audit has demonstrated a marked reduction in the previously published re-injury rates. We believe a generic approach to hamstring injury rehabilitation has limitations and we encourage clinicians working in other sports to identify loading and rehabilitation strategies to limit hamstring injuries in elite sports.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of British Athletics Rehabilitation strategy.
What is already known
Injuries to the hamstring muscle group can be at the muscle–tendon junction, at the myofascial border, or intratendinous.
Evidence exists for the efficacy of eccentric strengthening in the rehabilitation of hamstring injuries.
What are the new findings
The clinical application of the British Athletics Muscle Injury Classification and the principles of hamstring injury rehabilitation in the management of elite track and field athletes.
We advocate rehabilitation that is specific to the injured anatomical structure within a clinical reasoning framework.
We contend that isometric strengthening of the hamstrings complement eccentric loading.
Milestone criteria are suggested to aid progressions and decision-making
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Acknowledgments
The authorswould like to recognise the work of colleagues in the British Athletics Sports Science and Medicine team past and present who have contributed to the evolution of this strategy. We also thank Danny Talbot, Andrew Pozzi and Harry Aikines Aryeetey for help producing figures and drill videos, and in particular Jon Murray for acting as a subject for hamstring exercise videos. The authors also acknowledge the work of Louise Carrier for help producing the infographic. Ben Macdonald would like to specifically thank Dr Polly Mcguigan for her invaluable insight into muscle function and support over many years working together.
References
Footnotes
Correction notice This article has been corrected since it published Online First. The second author's name has been corrected.
Contributors BM, NP, SM, RC, SK and MJ all contributed to the initial drafting and editing of the manuscript. RC led the design of the infographic.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.