Article Text

Abstract
Ice hockey is a high contact sport where players are inherently at an increased risk for traumatic and time-loss injury. With its increasing popularity and high incidence of injury, further research is necessary to understand the risks and injuries associated with the sport and to develop performance-based outcome measures to guide return to play. This review, tailored to the practicing sports medicine team physician, focuses on the stepwise identification, treatment, time loss, return to play and subsequent risk of injury for the most common areas of injury: the head, shoulder, hip and knee. Injuries were categorised into upper and lower extremity with an emphasis on glenohumeral and acromioclavicular joint injuries, femoroacetabular impingement, medial collateral ligament tears, and high ankle sprains. With return to play a primary goal for these high-level athletes, recovery in ice hockey becomes a complex issue with efficient protocols tailored to the requirements of the sport vital to the athlete and clinician alike. By reviewing the treatments and sport-specific care, athletes can be better managed with the ultimate goal of returning to their preinjury level of play. Level of Evidence: Level IV.
- Contact Sports
- Concussion
- Elite Performance
- Epidemiology
- Olympics
Statistics from Altmetric.com
Introduction
Ice hockey is a high contact sport where players are inherently at an increased risk for time-loss injury.1 Engebretsen et al2 reported that in relation to the number of registered athletes in the 2010 Olympics, the risk of sustaining an injury was highest for ice hockey with 13–35% of registered athletes affected.2 In addition, ice hockey had the highest incidence of athlete-to-athlete trauma. The percentage of injuries that occur during games is 13.5% knee injuries, 8.9% acromioclavicular (AC) joint injuries, 6.2% upper leg contusions and 4.5% pelvis and hip muscle strains.3 Therefore, injuries of the upper extremity will be reviewed with a focus on glenohumeral and AC joint injuries.4 Furthermore, the most common lower extremity injuries for the hip, knee and ankle will be reviewed.
For this work, injury was defined as the cause for a player to be removed from competition before completing a full session, miss a subsequent session or sustain a trauma that posed a need for medical attention.1 ,4–6 Although many time loss injuries are concussions, which impact the player from continuing on-ice activity, the focus of this review is musculoskeletal injuries and treatment.3 It should be observed that if an athlete has sustained a concussion while in practice or competition the athlete should not be allowed to return to play that same day.7–9 Before being able to return to full participation the athlete should follow an established return to play exertional progression once they present asymptomatically at rest (table 1).7 The purpose of this review was to gain a well-rounded understanding of common injuries acquired in ice hockey. The understanding of the most common musculoskeletal injuries in ice hockey will strengthen the knowledge of treatments and preventative measures and ultimately progress the athlete to a safe and timely return to sport.
Gradual return-to-play protocol after a concussion (from the 4th International Conference on Concussion in Sport, Zurich)
Shoulder
AC joint separation
The most common mechanism of AC joint injury is a direct blow to the player's shoulder which drives the player's acromion inferiorly leading to a tear or stretch in the AC and/or the coracoclavicular (CC) ligaments.10–14 In an injured player, physical examination will demonstrate limited shoulder range of motion (ROM) while palpation of the AC joint will reveal tenderness, localised pain and possible deformity.11 To evaluate for fractures or separations of the AC joint, standard anteroposterior, lateral and axillary radiographs are recommended.14 The treatment of AC joint injuries in hockey is usually based on the classification and grades as proposed by Rockwood (table 2).11
Treatment
The treatment is based on the severity of the AC separation. Treatments for grade I and II separations include the use of a sling, analgesics, cryotherapy, immobilisation, early ROM, taping and rest.5 ,11 ,12 ,14 Recent studies have demonstrated good outcomes for a similar non-operative treatment of grade III AC separations in ice hockey.14 ,15 Unlike grade III injuries, grades IV–VI separations require surgical intervention through CC ligament reconstruction, CC repair or ligament transfer.15 During the recovery phase players should avoid activities that may aggravate the injury or limit ROM.11
Return to play
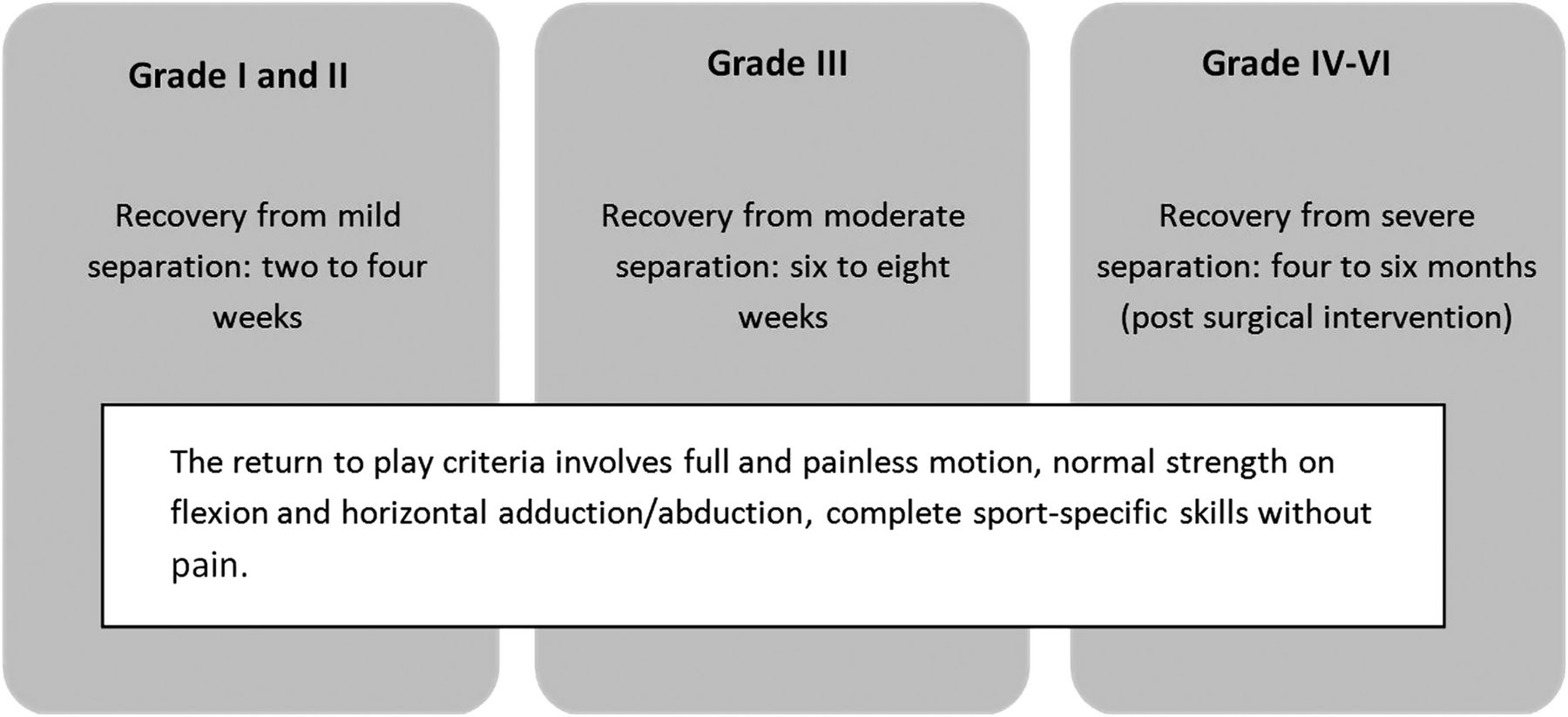
Recovery time and criteria for return to play for the majority of AC joint injuries is displayed in figure 1. The player should have full return of strength and shoulder motion on the affected side. Tape and AC joint pads may be added to protect the AC joint for pre-emptive pain management and to dissipate contact forces (figure 2).5 The period for ‘failing to progress’ is not clear and thus, recovery time is variable.11

Recovery time and criteria for return to play acromioclavicular joint separations.

Acromioclavicular (AC) joint pad. The AC joint pad is used to protect the AC joint for pre-emptive pain management and dissipate contact forces for athletes returning to play following a shoulder separation. The AC joint pad's straps anchor to the shoulder to prevent migration and may be customised by immersion in hot water.
Clavicle fractures
In general, non-displaced mid-shaft clavicle fractures can be managed without surgical intervention but clinical trials have demonstrated that operative fixation often leads to improved long-term functional and cosmetic outcomes.16 Throughout recovery, up to 6 weeks of non-contact activities may be observed while the introduction of contact sports may take 8–10 weeks.
Glenohumeral (shoulder) dislocations
Another injury common to ice hockey is a glenohumeral dislocation which occurs when the elevated arm is forced posteriorly or from a direct blow to an abducted and externally rotated shoulder.12 To begin recovery it is recommended that the player maintains a period of immobilisation (usually 4–6 weeks) followed by strengthening exercises. For players without a history of dislocation, it is possible for return to play once their overall shoulder strength and motion return to normal. Joint rehabilitation may be achieved through the strengthening of the shoulder and periscapular muscles, but surgery is often required in recurrent dislocators to repair the torn labrum, ligaments and joint capsule.12 ,17 ,18 Traumatic anterior instability may be successfully rehabilitated after surgical intervention with a return to sport averaging 4–6 months.17 Bracing, such as the SAWA brace and Duke-Wyre brace, may help prevent a repeated dislocation for first time dislocators during the season and if discomfort and instability continues, athletes should consider surgery postseason.12 ,13 ,19 ,20
Lower extremity injuries
Hip
General hip injuries: hip pointers
Hip pointers occur when the player is checked into the boards or has a fall which compresses the gluteal muscles against the iliac crest.5 The occurring haematoma is not always visible and may present deep below the skin or in the abdominal muscles. Thus the primary concern postinjury is to minimise the haematoma that can occur by following the RICE (rest, ice, compression, elevation) protocol.5 Rest is necessary for a hip pointer to heal properly and, if necessary, it is recommended that the athlete reduce weight bearing with the use of crutches until the athlete can walk without a limp.5 Medications such as acetaminophen or acetaminophen with codeine can be helpful for analgesic needs for the first 7–10 days after the injury.5 To regain full mobility and comfort, hip abductor exercises are recommended along with supplemental padding within the hockey pants to minimise recurrent injury.5 Hip spica wrapping can be used for compresion and to reduce pain during skating.
Femoroacetabular impingement
Ice hockey players have been noted to be at an increased risk for the development of femoroacetabular impingement (FAI). Goaltenders, in particular, have been reported to be at an increased risk due to the unique style of joint position known as the butterfly technique.21 ,22 To perform the butterfly technique, goaltenders internally rotate the femur, drop to their knee joint while flexing the femur and attempt to cover the goalnet by ‘laying out’ their lower-leg pads.18 Owing to the combined motions of hip flexion and internal rotation inherent to the butterfly technique, it has been associated with the development of overuse hip injuries (FAI), especially in higher level goaltenders.21 Goaltenders may not be the only position at increased risk as Stull et al23 described that during the sprint start, the ice hockey player goes through external rotation and abduction during the push-off phase, and internal rotation through increasing hip flexion during the recovery phase, placing the player in an ‘at-risk’ hip position. Philippon et al22 observed that youth ice hockey players (aged 10–18) had significantly higher α angles and a significant correlation between increased age and increased α angles compared with a control group of age matched youth skiers. Even at young ages, competitive ice hockey players have a greater prevalence of α angles associated with FAI.
Identification
FAI is caused by morphological abnormalities of the femoral head-neck junction and/or the acetabulum that results in abnormal contact between the femur and acetabular rim.21 ,22 There are two main types of FAI, cam and pincer types, however, mixed type FAI has been described when both cam and pincer impingement are present.21 ,22 Cam impingement more commonly occurs in young athletic males and is the most commonly diagnosed type in ice hockey players.21–24 Cam impingement is the femoral cause of FAI due to an aspherical femoral head–neck junction that causes recurrent microtrauma and injury to the chondrolabral junction of the acetabulum, especially with hip flexion and internal rotation.21–25 Often presenting initially as groin pain, sports hernias or adductor strain, which are common secondary injuries due to FAI, which in turn classically presents as a limitation in hip motion, specifically during flexion and internal rotation.25 Pain resulting from FAI is most often described in the anterior hip or groin; athletes may show the location through cupping their hands over their hip from anterior to posterior known as the ‘C-sign’.26 For a thorough examination, the player should be examined seated, supine lateral and prone (table 3). If FAI is suspected, radiographs and MRI are the best modalities in the diagnosis because the clinical examination has demonstrated a low diagnostic accuracy.25 ,26
Recommended physical examination of FAI as described by Yen et al26
Treatment
While non-operative methods should be initiated to treat FAI, in those athletes with cam lesions and acetabular labral tears, surgery is usually recommended with resection of the cam lesion and labral repair. Resection of the cam lesion of the femoral neck and a labral repair is usually performed. Philippon et al demonstrated that treatment of FAI and labral lesions in professional ice-hockey players resulted in successful short term outcomes and a prompt return to sport, with the time to participating in skating/hockey drills averaging 3–4 months following surgery. Furthermore, the Modified Harris Hip Score improved from 70 preoperatively to an average of 95 at follow-up (average follow-up 24 months) in the 28 professional players.27
Return to play
Pierce et al21 described a functional programme for ice hockey goaltenders, which can also be adapted to other on-ice positions, to assist in rehabilitation postarthroscopic hip surgery with an expected on-ice return of 4 months. The programme is divided into a four-phase rehabilitation protocol with six phases dedicated to an on-ice programme. The phases are athlete dependent, meaning that the individual athlete's rehabilitation abilities should be taken into consideration.21 The completion of the programme will be decided when the injured player obtains successful pass of a score higher than 17/20 or 20/20 (for professional athletes) in the Vail Hip Sports test without pain or swelling during drills.21
Subsequent risk and future
Persisting symptoms and adverse outcomes may be associated with surgical under-correction or over-correction of the cam lesion, and thus a need for revision surgery arises.25 Overall, the current recommendation for long-term outcome suggests that early intervention should occur before irreversible joint damage, such as osteoarthritis, disables the player.25 With surgical intervention for hip dislocations, 99.5% of patients continued to play professionally with a mean recovery time of 45.1 ± 22.1 months.28 Likewise, Philippon et al29 reported that 93% of 45 arthroscopically treated ice hockey athletes returned to professional competition while 78% maintained their professional activity 1.6 years after surgery. These recommendations are not based on controlled randomised studies, but rather on prospective cohort studies and expert opinions.
Thigh and knee
Quadriceps contusions
Quadriceps contusions occur when an object such as a puck hits the thigh (quadriceps muscles), causing the tearing of the muscle fibres at or directly adjacent to the area of impact. The result of the impact includes immediate pain and potential loss of knee motion due to a haematoma.5 ,30 Physical examination and measurement of knee flexion is a prognostic indicator in quadriceps contusions (table 4).31 After diagnosis, the injured leg is placed in a hinged knee brace at 120° of knee flexion or an elastic compression wrap in a position of flexion to limit haematoma formation.5 ,30 Ice is recommended to decrease the amount of bleeding, and by being flexed and wrapped, ensures less space for swelling.5 After 24 h, gentle, active and pain-free motion of the knee should be instituted along with stretching and quadriceps strengthening exercises and low-impact weight-bearing exercises such as jogging in a pool or working on a stationary bike.5 ,30 While Ryan et al31 described the average time of disability as 13 days for mild contusions, 19 days for moderate contusions and 21 days for severe contusions, the authors have anecdotally found that most athletes, when treated immediately after injury, can return to on-ice activity within a few days once their knee motion and strength return.
Medial collateral ligament
Identification
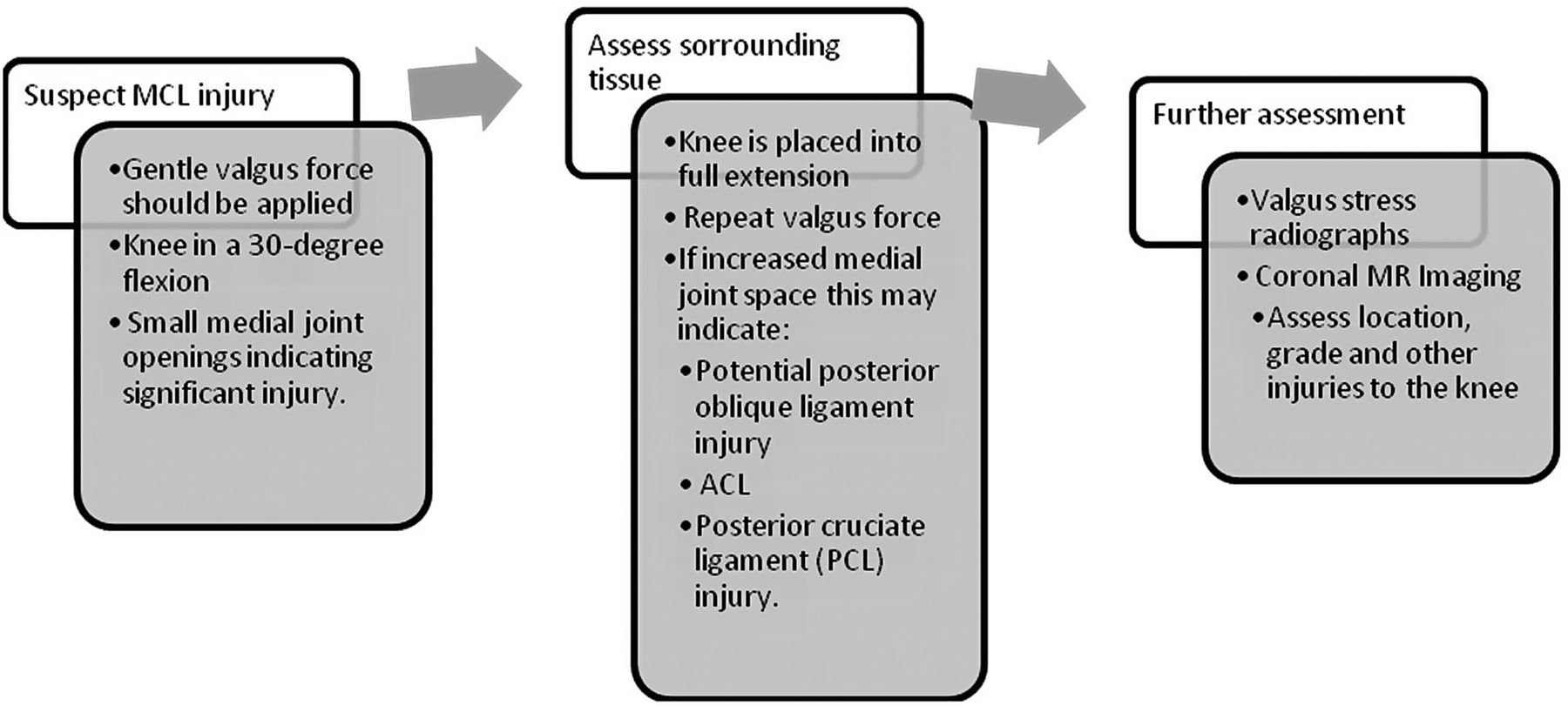
The medial collateral ligament (MCL) is the most commonly injured knee structure during ice hockey participation due to frequent on-ice collisions which may produce a twisting valgus force to the knee.4 ,5 When an MCL injury is suspected, an accurate examination begins immediately with a relaxed player and an exposed contralateral leg to use as a control for medial joint line opening.32 The step-wise identification process is depicted in figure 3. Isolated MCL injuries usually result in localised soft tissue swelling, while ACL tears result in a generalised knee effusion and haemarthrosis.32 ,33 The MCL injury's original reference for grading scale has been the American Medical Association (AMA) Classification with grade I representing a mild opening (0–5 mm), grade II representing a moderate opening (5–10 mm) and a grade III as complete opening (>10 mm).32–34 However, recent research has reported that a grade III MCL injury is present on valgus stress radiographs when medial compartment gapping is greater than 3.2 mm when compared with contralateral knee at 20° of flexion.34
Treatment
Grade I and II MCL injuries have been treated with non-operative management through cryotherapy, compression and elevation. The RICE protocol is used to decrease the swelling of the knee joint by minimising bleeding through the use of a compression wrap or an elastic sleeve.35 Throughout this treatment, initiation of active knee motion is used to prevent stiffness with associated strengthening exercises. The treatment for medial knee injuries is dependent on whether the injury is isolated or combined with other ligament injuries. Non-operative treatments for grade III injuries focus on restoring quadriceps function, improving knee motion and controlling oedema through a focus on exercises that restrict side-to-side activities. It is recommended to use a hinged knee brace in the early phases of rehabilitation and discontinue it after the competitive season is completed.35
Return to play
If proper rehabilitation for an MCL injury is followed, the athlete can usually return to sport after 0–2 weeks for grade I injuries and 2–4 weeks for grade II injuries.32 Likewise, if the athlete follows a well-guided rehabilitation programme, most athletes return to full competition 6–8 weeks following isolated MCL grade III injuries. For rehabilitation, ROM and quadriceps reactivation is recommended to decrease the amount of time loss for the athlete.33
Subsequent risk and future
An MCL reconstruction may occasionally be required for high-level athletes who wish to return to play and who have continued instability from an MCL tear. However, the reconstruction of grade III MCL injuries remains controversial.36 It is recognised that the non-operative treatment of some grade III MCL tears may lead to chronic valgus instability or rotatory instability.35 Despite the best rehabilitation efforts, associated quadriceps weakness, abnormal movement patterns, laxity and reduced knee function have been documented.37 Using an anatomic reconstruction, good outcomes have been achieved. Lind et al38 reported that medial stability according to the International Knee Documentation Committee (IKDC) criteria was normal to nearly normal in 98% of patients, although the overall IKDC score demonstrated that 13% of patients were rated as abnormal with combined MCL reconstruction at follow-up. When presenting concurrently with an anterior cruciate ligament (ACL) tear, reconstructed grade III MCL tears demonstrated significantly higher functional scores than those athletes who were treated non-operatively.39
Anterior cruciate ligament
Identification
Tears of the ACL are not common in ice hockey players and players who have minimal instability from an ACL tear can occasionally continue playing through the season.5 When they occur, they are most commonly due to on-ice collisions with another player or the goalpost. Examination in the training room immediately after injury, before pain, swelling and muscle guarding set in, are usually very accurate in arriving at a diagnosis. The Lachman and the pivot shift tests have proven to be effective clinical diagnostic tools. However, the Lachman test is the most effective test in the diagnosis of ACL tears (figure 4).40

Lachman test to diagnose anterior cruciate ligament tear. One hand used to secure and stabilise the athlete's distal femur while the other firmly grasps the proximal tibia. The leg should be at 20–30°. A gentle anterior translation force is applied to the proximal tibia (demonstrated by the red arrow). The examiner assesses for a firm/solid or soft endpoint.
Treatment
ACL tear management focuses on the ability to restore normal function, reduce symptoms, and an attempt to return to play.40 The low friction activity of on-ice skating can occasionally allow a player to return to play during the season and to plan for an ACL reconstruction after the competitive season is completed. If a player has knee instability while training or with on-ice activity, it is recommended to have the ACL reconstructed using a patellar tendon or hamstring autograft.5
Return to play
In athletes presenting with an ACL tear combined with cartilage injury, the clinical goals are to restore a more normal state of knee motion, relieve symptoms and return the athlete to near preinjury activity. The International Sports Medicine Association identified that for an ACL reconstruction and/or rehabilitation programme to be considered successful, the knee must be absent of symptomatic knee joint instability, quadriceps and hamstring strength asymmetry, the presence of no more than mild-knee joint effusion.41 There is however, a lack of standardised objective criteria to accurately assess the ability of a patient to safely return to their previous level of activity following ACL reconstruction.
Subsequent injury risk
The risk of a second ACL injury is highest during the first year following the athletes return to sport.42 Additionally, risk to the contralateral limb is significantly higher than the reconstructed limb suggesting that reinjury is not exclusive to the original involved limb.43
Ankle
Skate (lace) bite
Skate bite, also known as lace bite, typically presents when new skates are introduced and not broken in or when skates become old and inflexible.5 The inflexibility of the skate tongue along with repeated ankle dorsiflexion within the skates puts pressure on the anterior aspect of the ankle irritating the tibialis anterior tendon.5 This may result in tendonitis and decrease the athlete's ability to participate in on-ice activities. The treatment for this injury is the fashioning of a soft piece of foam rubber to the outside of the hockey sock or skate to relieve pressure and decrease irritation (figure 5).5 Likewise, manually breaking in the skate's tongue by bending it repeatedly will decrease pressure on the tibialis anterior tendon. Although anti-inflammatory drugs can be used, the only way to fix the problem is through ‘breaking the skates in’.43

Lace bite protection. Lace bite pads can be purchased and attached onto the skate's tongue (inside) and help to alleviate pressure or pro-wrapped directly to the players foot (A). Combination padding such as a boot bumper contains gel pads molded inside an elastic lining to protect against friction and abrasion of the boot and skate laces (B).
High ankle sprains: syndesmosis injury
Identification
One of the most debilitating ankle injuries for ice hockey players are high ankle sprains also known as a syndesmosis injury.5 High ankle sprains are less common and affect the ligaments that are proximal to the lateral ankle ligaments traditionally involved in lower ankle sprains. High ankle sprains occur when the foot is twisted externally, resulting in microtears or tears of the junction between the tibia and fibula just above the level of the ankle.44 The ligaments affected are the anterior inferior tibiofibular ligament, the inferior tibiofibular ligament, the inferior transverse tibiofibular ligament and the interosseous ligament.44 Various tests such as direct palpation, the squeeze test, external rotation stress test, cotton test and the fibula translation test have been used to diagnose a syndesmosis injury.44 The ankle typically presents as normal on routine X-rays even with a syndesmosis injury, but when the ligaments are stressed through a squeeze or external rotation test there may be an abnormal alignment of the ankle joint on fluoroscopy depending on the severity of the injury.45 The authors have found that having the athlete remove their skates and stand and gently twist their ankle in the locker room will usually help to diagnose this injury immediately off ice.
Treatment
The initial treatment for high ankle sprains includes the RICE protocol. Proper assessment may include anteroposterior (AP), mortise, and lateral ankle radiographs to assess for fractures, which often occur due to a similar injury mechanism and can have similar symptoms. Once swelling in the ankle has decreased and ankle motion has increased, the athlete can start an ankle-strengthening programme.5 A three-phase approach has been proposed by Williams et al.46 in which the first phase begins as the acute, protection phase. The focus initially is on immobilisation, weight bearing and the control of the inflammatory process.46 Athletes then progress to the subacute phase with a focus on normal mobility, increased strength, improved neuromuscular control and the promotion of joint mobility.46 Finally, the advanced training phase consists of a confident return to play by including more aggressive training exercises and sport-specific activities.46 The programme may protect the ankle from being reinjured and provide appropriate proprioceptive training to re-recognise joint location.5 Continuing to skate on the ankle will delay the healing of the involved ligaments and may limit further on-ice activity.
Return to play
High ankle sprains have been particularly bothersome in ice hockey players because of the frequent twisting and turning required for on-ice activities which can delay their return to participation compared to other sports. Once an athlete has minimal swelling and appropriate strength, a functional on-ice evaluation should be performed to assess readiness for return to play. This is especially important for high ankle sprains because an athlete should not play through pain because of risk of reinjury. High ankle sprains can take up to 12 weeks to heal in ice hockey players.5
Low ankle sprains
Identification
Low ankle ligament sprains (anterior talofibular ligament, calcaneofibular ligament and the posterior talofibular ligament) occur most often with the foot in plantar flexion, inversion and adduction.47 ,48 The athlete will report ‘rolling over’ on his or her ankle and describe acute lateral ankle pain.48 The ‘rolling over’ action causes damage to the lateral ankle ligaments resulting in swelling, pain, problems with weight bearing and haematoma.47 ,48 Over time, the pain and swelling will diffuse and palpation of the injured area will help to localise the ligaments that have been torn.48 To assess ankle instability it is recommended to perform the anterior drawer test and the talar tilt test.48 Standard ankle radiographs can also be performed to rule out fracture.
Treatment
It is generally accepted that almost all low ankle sprains in ice hockey players can be treated through non-operative and functional measures.47–49 The RICE therapy should begin immediately to limit bruising and swelling.48 Lace-up ankle supports and taping have also been reported to be effective in reducing swelling and injury prevention.47 External support has shown to be beneficial to aid with earlier mobilisation due to continuous weight bearing support within the ankle (figure 6).47 Functional rehabilitation through balance exercises is recommended to decrease time until recovery, focusing on improving ankle motion.48 ,50 Ankle sprains do not usually require surgical treatment.47 However, with chronic instability, severe injuries or concurrent injuries, surgical ligament repair or reconstruction maintains the advantage of less common recurrence when compared with non-operative treatments.47

External ankle support for use following a low ankle ligament sprain. An external ankle support may be beneficial to aid with earlier mobilisation due to the continuous weight bearing support it provides within the ankle.
Return to play
Most low ankle sprains are managed non-operatively and with a functional rehabilitation programme. This is because the ice hockey boot provides excellent support and protection for low ankle sprains. Return to play usually occurs within a few days to a week, although complete ligament healing may take from 6–12 weeks.51
Conclusions
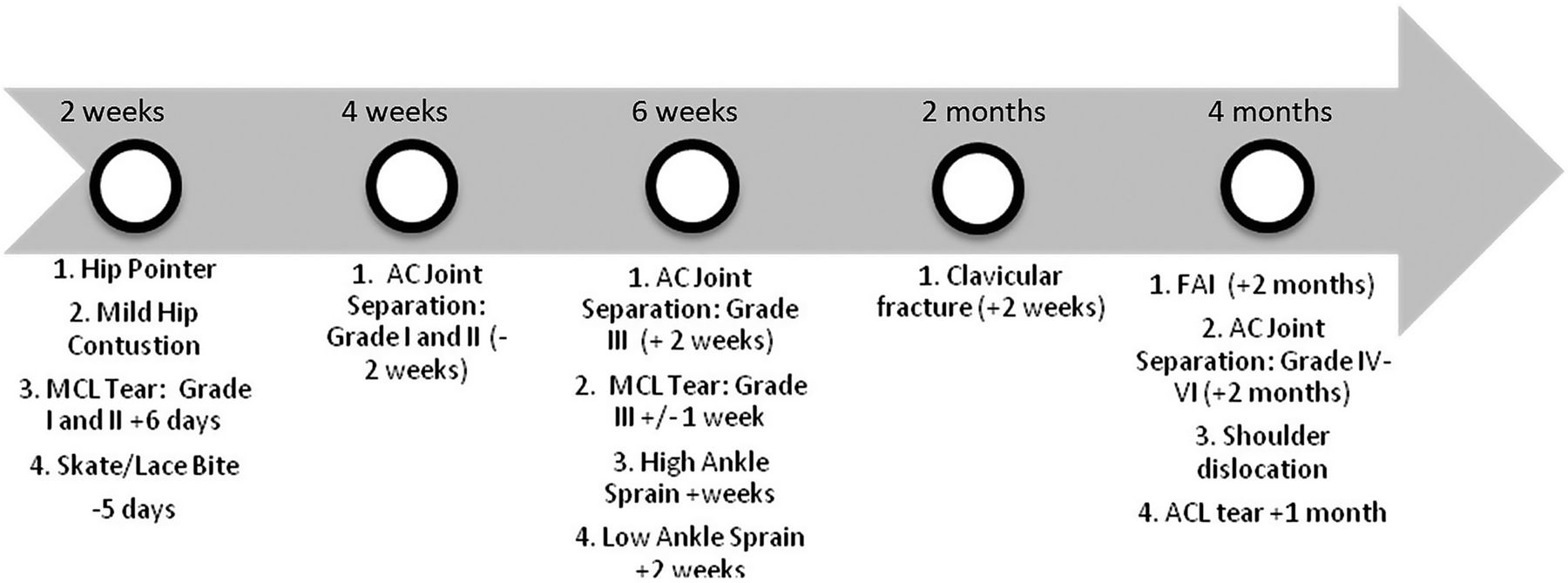
The current review provides an overview of the most commonly encountered ice hockey injuries (figure 7) and evidence-based methods of treatment of the most common time loss extremity injuries. Most time-loss injuries in ice hockey can be managed non-operatively with a functional return to on-ice activity. Ice hockey is a contact sport with unique injury patterns. Knowledge of these injuries and treatment regimens will help to minimise downtime and safely return athletes to competition.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Musculoskeletal time-loss injuries.
What are the new findings?
-
Most time-loss injuries in ice hockey can be managed non-operatively.
-
The most common shoulder injuries in ice hockey include acromioclavicular joint separations, clavicle fractures and glenohumeral dislocations.
-
Ice hockey has unique injury patterns.
-
There remains a need for additional scientific information with regard to external risk factors of injury.
How might it impact on clinical practice in the near future?
-
Valuable information on the identification, treatment and return-to-play is presented for common musculoskeletal ice hockey injuries.
-
This work will give all shareholders in the athlete a resource to guide treatment and recovery.
-
As care of high-level athletes continues to evolve, more work should be performed to optimise return to play in ice hockey specific injuries.
Acknowledgments
The authors would like to thank Luke O'Brien, PT for his assistance in the descriptions of proper physical examination of injuries and rehabilitation protocol. In memory of Scott Winkler, former Colorado College Division I ice hockey player, who passed away unexpectedly on 12 June 2013.
References
Footnotes
-
Contributors RFL, RKS, ANS, BSH, BMM, LE and CAW involved in substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; and were responsible for drafting the work or revising it critically for important intellectual content, and final approval of the version to be published; agreement to be accountable for all the aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
-
Funding This study was funded by the Steadman Philippon Research Institute.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com