Article Text

Abstract
Objectives—To examine the relation between the clinical features of groin pain and groin magnetic resonance imaging (MRI) appearances in a group largely comprising elite Australian Rules football players. The incidence of bone marrow oedema and other MRI findings in the pubic symphysis region was noted. The relation between a past history of groin pain and these other MRI findings was also examined.
Method—In a prospective study, 116 male subjects (89 footballers, 17 umpires, 10 sedentary men) were examined before history taking and groin MRI. The clinical history was not known to the examiner (GMV) and radiologists (JPS, GTF). Clinical evidence of groin pain and examination findings were correlated with the presence of increased signal intensity within the pubic bone marrow. A past history of groin pain was correlated with the presence of other MRI findings such as cyst formation, fluid signal within the pubic symphysis disc, and irregularity of the pubic symphysis.
Results—Fifty two athletes (47 footballers, five umpires) had clinical features of groin pain with pubic symphysis and/or superior pubic ramus tenderness. A high incidence of increased signal intensity (77%) within the pubic bone marrow was identified in this group. There was an association between this group of athletes and the MRI finding of increased signal intensity (p<0.01). There was also an association between a past history of groin pain and the presence of other MRI findings (p<0.01).
Conclusions—Athletes with groin pain and tenderness of the pubic symphysis and/or superior pubic ramus have clinical features consistent with the diagnosis of osteitis pubis. The increased signal intensity seen on MRI is due to pubic bone marrow oedema. An association exists between the clinical features of osteitis pubis and the MRI finding of pubic bone marrow oedema. A high incidence of pubic bone marrow oedema was also noted. Degenerative features visualised by MRI, such as subchondral cyst formation, were associated with a past history of groin pain. A stress injury to the pubic bone is the most likely explanation for these MRI findings and may be the cause of the clinical entity osteitis pubis.
- osteitis pubis
- groin pain
- magnetic resonance imaging
- bone marrow oedema
- stress injury
Statistics from Altmetric.com
Take home message
Athletes that present with chronic groin pain and have tenderness of the pubic symphysis and/or superior pubic ramus have a high likelihood of having pubic bone marrow oedema as visualised by MRI. This oedema is probably a response to bony stress.
Diagnosing the cause of chronic groin pain in sportsmen is difficult. Athletes who participate in sports with repetitive kicking, side to side movement, and twisting seem to be most at risk.1–3 Potential diagnoses include osteitis pubis, adductor muscle/tendon dysfunction, and posterior inguinal wall deficiency (sports hernia).4–9 In the evaluation of groin pain in sportsmen, there is no consensus as to the clinical and investigative approach to treatment. Current investigations may include plain radiography with or without stress views,10, 11 triple phase bone scan,12 ultrasound,13, 14 herniography,6, 15 and computed tomography scanning.16 The magnetic resonance imaging (MRI) scan has been shown to differentiate between some causes of chronic groin pain,17, 18 but to date this technique has not been used extensively in the investigation of athletic groin pain. One retrospective study using MRI scan appearances in 11 soccer players with athletic chronic groin pain speculated that a trabecular microfracture of the superior pubic ramus may result in altered weight bearing and increased stress on the pubic symphysis leading to symphysitis.19
One cause of chronic groin pain in athletes is osteitis pubis, a disorder characterised by pubic pain and chronicity. The cause is considered to be mechanical, with inappropriate stress and shear forces acting on the pubic symphysis.1 Mechanical factors implicated have included limited hip rotation,20 muscle action on the pelvis, in particular the adductor musculature,9, 21 pelvic bone biomechanics,10, 22 and overuse.1, 23 Clinical features of osteitis pubis are described in a study of 59 athletes.1 The typical clinical history is pain that is unilateral and located in the adductor region. The most consistent signs seen were tenderness of the pubic symphysis (seen in 70%) and superior pubic ramus (seen in 40%). These are the usual symptoms described for the clinical diagnosis of osteitis pubis in sports medicine textbooks and groin injury review articles.24–26 Standard investigation of osteitis pubis includes plain radiography (asymmetrical bony erosions with sclerotic bony margins at the symphysis) and the triple phase bone scan (increased uptake on the delayed phase of the scan).1, 10, 12, 27 These investigations are useful for the diagnosis of this condition but are not of prognostic value.1, 6
Australian rules football is a collision contact sport with speed, strength, and agility demands similar to rugby or American football. It differs from these football codes, with more kicking and evasion and higher aerobic demands because of the continuous nature of play and thus is similar to world football. A high level of athletic training is required to play at the elite level in Australian rules football, and a large number of overuse injuries are reported at junior and senior levels.28 As overuse is considered to be associated with the development of sports related chronic groin pain, including the diagnostic entity osteitis pubis, this is a possible explanation for the high incidence of this condition in elite Australian rules football players.
Clinical evaluation and MRI were used to assess a group of athletes, predominantly elite Australian rules football players, with a high incidence of sports related chronic groin pain. The principal aim of the study was to correlate clinical features of groin injury such as pain and tenderness with the MRI finding of pubic bone marrow oedema (BMO). The incidence of groin MRI abnormalities, such as BMO, cyst formation, and irregularity of the pubic symphysis, was recorded, with the relation between a past history of groin pain and these other groin MRI abnormalities also being studied.
Methods
SUBJECTS
After ethical approval from the committee on clinical investigations, signed informed consent was obtained from each participant. Eighty nine footballers, all male, were recruited from two national competition teams (Australian Football League (AFL); n = 60) and one state competition team (South Australian National Football League (SANFL); n = 29). At the end of the preseason, after at least six weeks of intensive training, subjects from each team were recruited with the following priorities: (a) athletes with current groin pain; (b) athletes with previous groin pain; (c) athletes who had never had any previous episode of groin pain.
Seventeen running athletes were recruited from the umpires used for the Australian rules football competitions (AFL and SANFL) as active subjects who, unlike the footballers, do not undertake significant twisting and cutting as part of their training. The training of these umpires is similar to that of distance runners. Each needed to have completed at least six weeks of intensive training and be in the same age range as the football players.
In addition, 10 sedentary men were recruited using the following criteria: (a) no prior episode of groin pain; (b) no physical exercise within the previous six weeks; (c) same age range as the active subjects.
HISTORY AND EXAMINATION
The clinical history was not known to the examiner (GMV) for all athletic subjects (89 footballers, 17 umpires). Clinical examination was performed at the end of the preseason training period after the athletes had undertaken at least six weeks of intensive training. The groin region, hip, and back of the subjects were examined and then a history was obtained by direct interview. Questions sought to ascertain the presence or absence of current groin pain symptoms, location and side of pain, duration of symptoms, and past history of pain.
Tenderness was graded (0 = none; 1 = mild; 2 = moderate; 3 = considerable) for the anterior-superior pubic symphysis. The presence or absence of tenderness was recorded on the right and left sides in relation to the superior pubic ramus, adductor muscle origin, and the region superior to the pubic tubercle.
Subjects were considered symptomatic when they had groin pain located in the pubic symphysis and adjacent pubic bone region, adductor area, and/or lower abdominal area during and/or after exercise occurring in the recent six week preseason period and they also had tenderness of the pubic symphysis and/or adjacent superior pubic ramus.
Pain in the groin region without associated tenderness, and pain with tenderness in locations other than the pubic symphysis and/or superior pubic ramus was noted, but these athletes were not considered symptomatic.
MRI SCAN
After examination and history taking, MRI scans (1.5T GE Signa, 1.0T Siemens Impact) were performed on all 116 subjects using T1 and fat suppressed T2 sequences. The images were obtained in planes coronal and axial with respect to the pubic body (3–4 mm slices). The time between MRI and examination ranged from 0 to 12 days (median 3 days). Images were independently reviewed without clinical information by two musculoskeletal radiologists (JPS, GTF). Discordant cases were reviewed by the radiologists, and consensus was reached.
T2 fat suppression images were subjectively graded on the right and left side for (a) intensity of bone marrow signal (0 = normal; I = subtle/equivocal; II = moderate; III = severe), (b) size (extent) of signal change (long axis dimension <2 cm, ≥2 cm), and (c) hyperintensity of the adductor muscle origins. BMO was considered present when either grade II or III signal intensity was present, indicating an unequivocal change in bone marrow appearances. When grades 0–I were recorded, BMO was considered absent, as these grades showed no change or subtle/equivocal change in pubic bone marrow appearances.
The region of the pubic symphysis was assessed for irregularity of the pubic symphysis (graded as no change, moderate change, and considerable change) and for the presence or absence of (a) subchondral bone cysts, (b) fluid signal in the pubic symphysis disc, (c) distortion (or “beaking”) of the superior pubic symphysis (graded for size into less than or equal to 2 mm, 2–7 mm, and greater than or equal to 8 mm). Additional data recorded separately for the right and left sides included (a) pubic ramus sclerosis, (b) abnormal appearances at the site of the conjoint tendon, and (c) the presence or absence of an inguinal hernia.
STATISTICAL ANALYSIS
Correlation between the presence of symptoms and signs in the athletes and MRI scan findings were assessed by χ2 to calculate significance levels. A p value of less than 0.05 was considered significant in all analyses.
Results
The basic data for the footballers were as follows: mean (SD) age 22 (3.4) years (range 17–33); mean (SD) height 182 (19.3) cm (range 174–203); mean (SD) weight 85 (8.9) kg (range 64–110). No difference with respect to age, height, or weight was detected between those with pain and tenderness of the pubic symphysis and superior pubic ramus and those without, or between those with BMO and those without. The only difference between the groups was the expected finding of a lower weight for the umpires (70 (6.0) kg (range 65–85)) compared with the footballers.
CLINICAL FEATURES
Fifty two of the 106 athletes (47 of 89 footballers and five of 17 umpires) were considered to have current symptoms (pain) and signs (tenderness of the pubic symphysis and/or superior pubic ramus). One athlete (footballer) had pain but no tenderness. Table 1 gives information on the distribution of pain.
Pain and tenderness characteristics by clinical category
Fifty three athletes (41 footballers, 12 umpires) were without pain. The total number in this group was 54 as it included the athlete with pain but no tenderness. Sixteen of the group (13 footballers and three umpires) had experienced previous episodes of sports related chronic groin pain but had no clinical symptoms at the time of examination.
MRI SCANS: SIGNAL INTENSITY
Seventy six of 106 (72%) athletes (68 footballers and eight umpires) had pubic BMO (figs 1 and 2). A total of 47 of this group of 76 (62%) with pubic BMO (42 footballers and five umpires) had groin pain with tenderness of the pubic symphysis and/or superior pubic ramus.

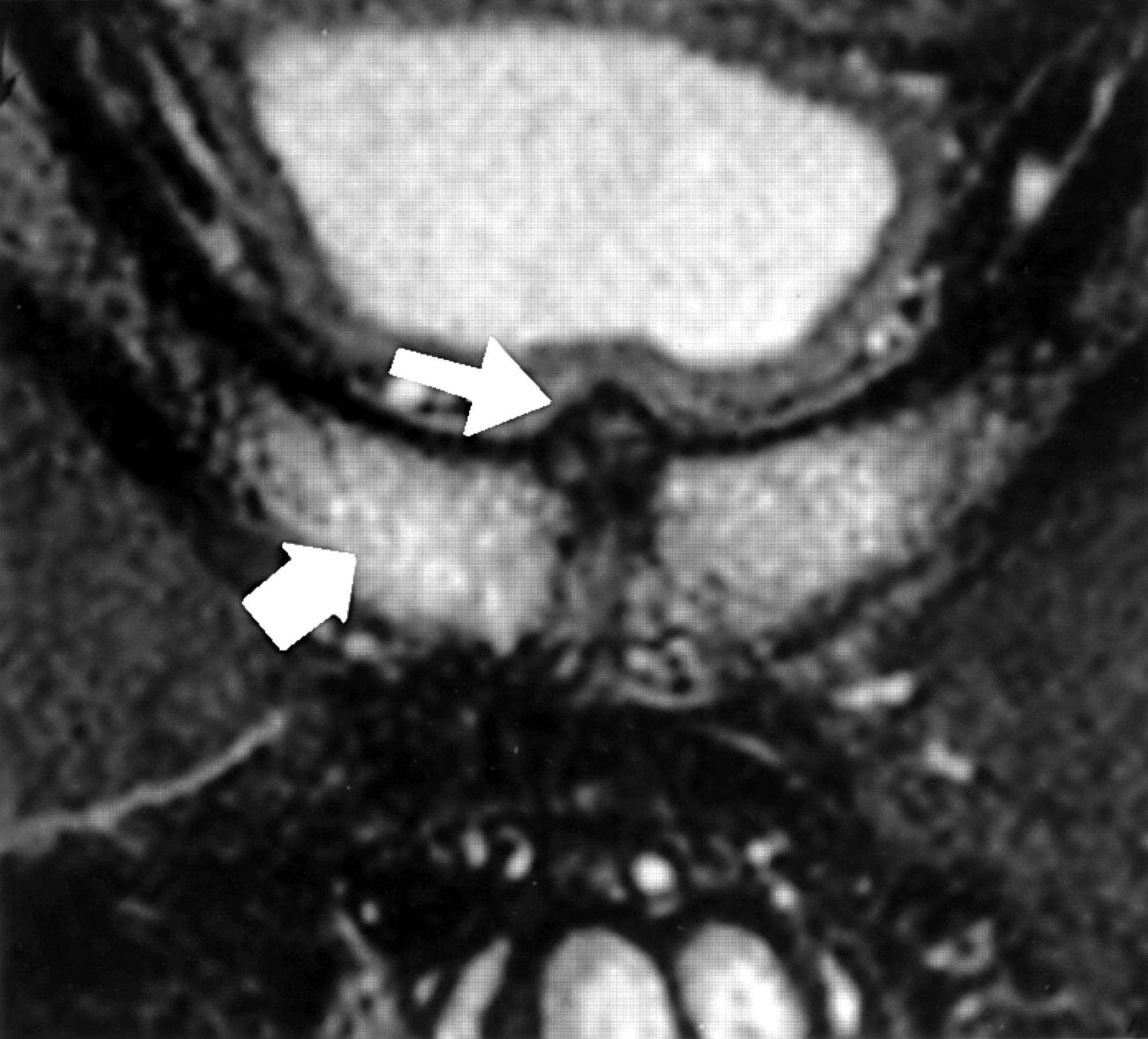
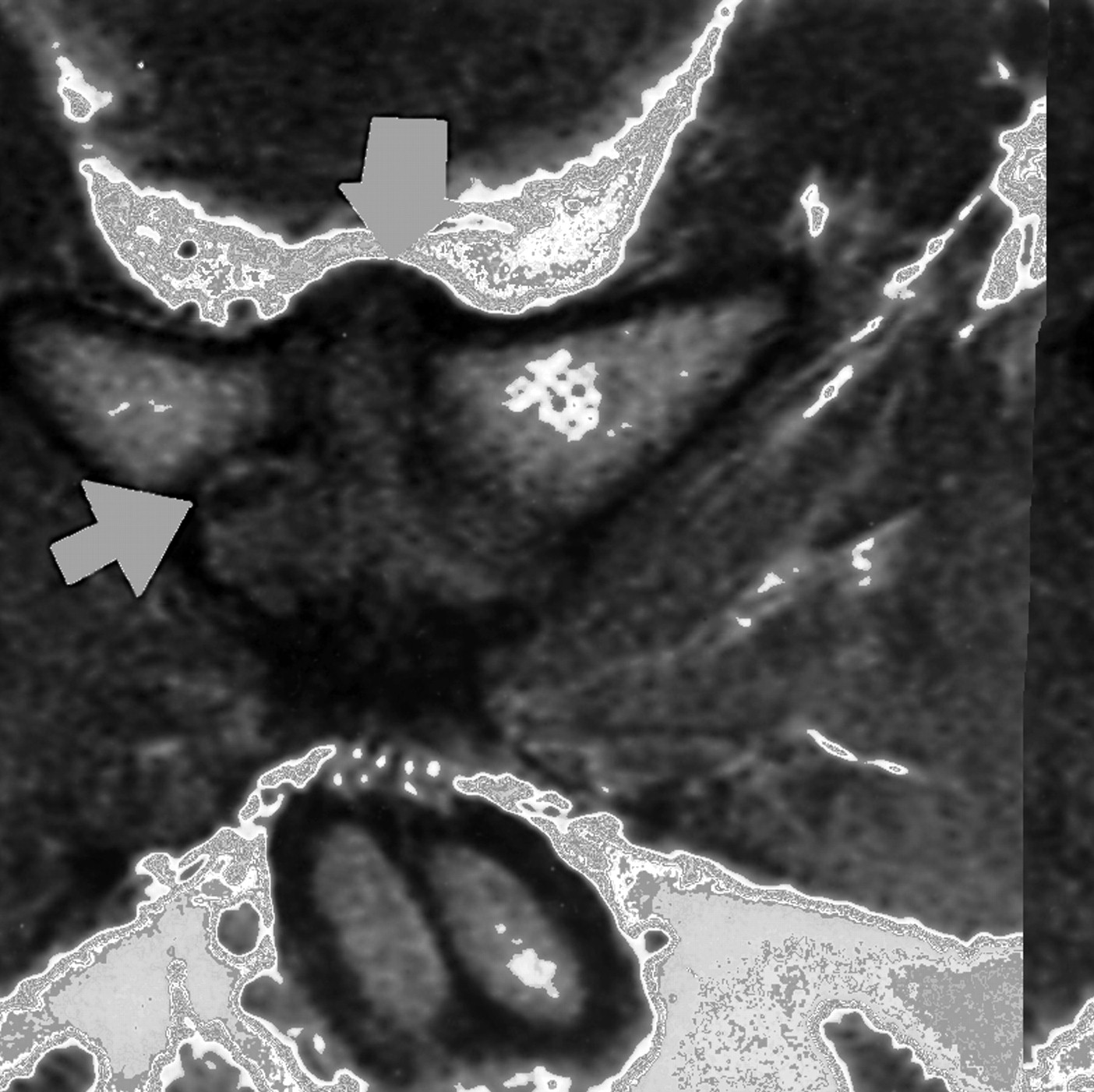
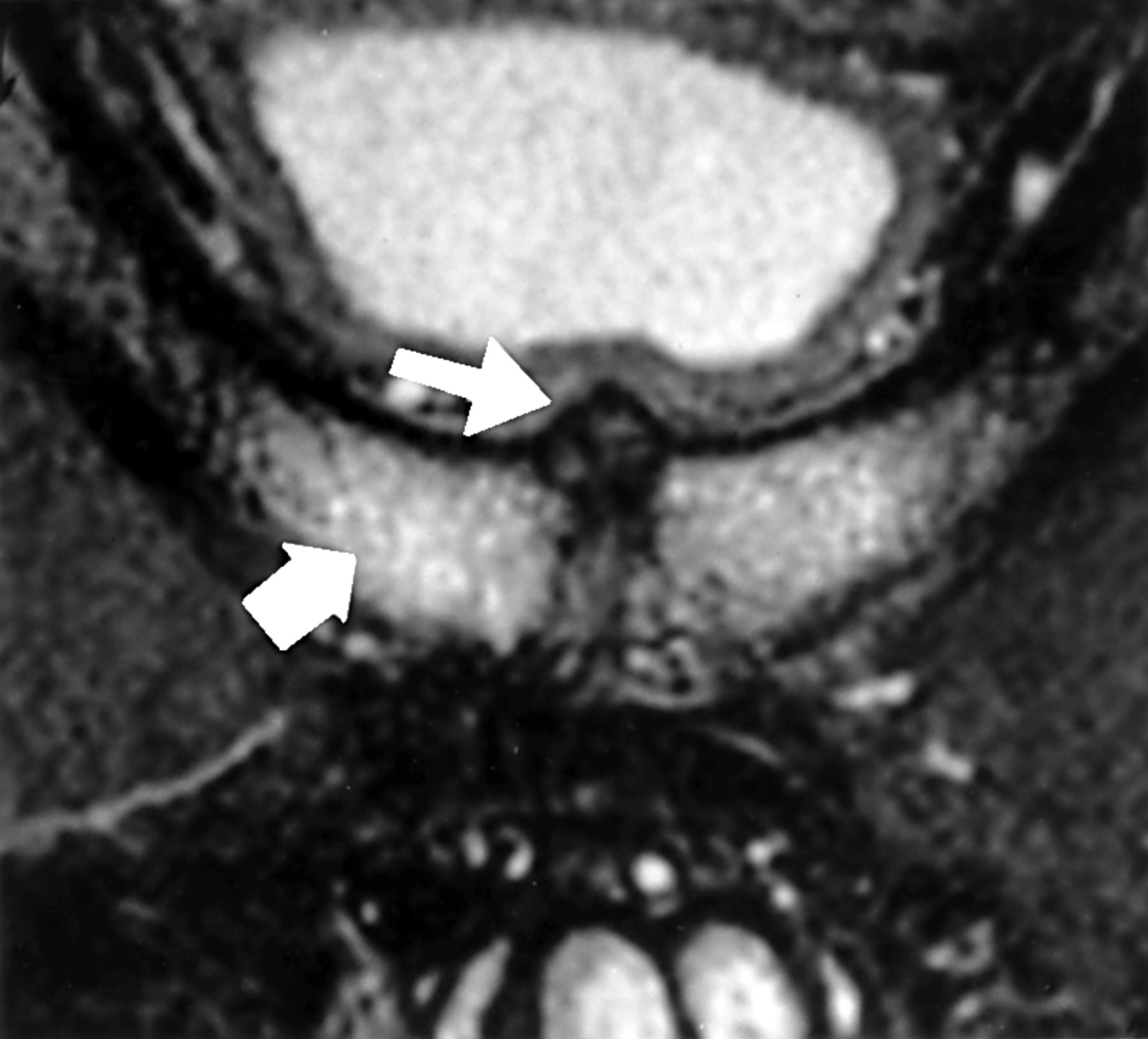
Fat suppressed T2 image in the plane axial to the pubic bodies. Diffuse marrow oedema (thick arrow) and a small subchondral cyst are present. The adductor origins (thin arrow; this side had some signal intensity change) and the conjoint tendon site (small arrow) are visible.
Fat suppressed coronal T2 image showing beaking of the superior pubic symphysis (thin arrow). Note severe bilateral marrow oedema in pubic bodies extending into the superior pubic rami (thick arrow) with an irregular pubic symphysis joint.
For 49 of this group of 76 (64%) with pubic BMO (46 footballers and three umpires), the size (extent) of signal change was greater than or equal to 2 cm in the long axis. Forty of this group of 49 (81%) with pubic BMO ≥2 cm in size (37 footballers and three umpires) met our symptomatic criteria. Table 2 summarises the incidence of BMO in the groups.
Magnetic resonance imaging signal intensity (grade and size) and subjects by clinical category
There was an association between having symptoms and having BMO on MRI (χ2 test 25.8, p<0.01). As the size of the BMO increased to more than 2 cm, the strength of association increased (χ2 = 46.5, p<0.01). When footballers alone were evaluated, significance was also achieved (χ2 = 9.3, p<0.01).
There was no association between either the group with no symptoms or the group with a past history of groin pain and the finding of BMO or BMO ≥2 cm.
MRI SCANS: OTHER FINDINGS
Table 3 gives other MRI findings (figs 2, 3, and 4). Images also showed the conjoint tendon (medial posterior inguinal wall) site, but no abnormality was detected in this region except in those that had undergone previous surgery to this region. Similarly no inguinal herniae were detected in this study.
Other magnetic resonance imaging scan findings by clinical category
Coronal T1 image showing pubic beaking of the superior pubic symphysis (thick arrow) and a large subchondral cyst (thin arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Same subject as fig 3 . Fat suppressed coronal T2 image showing a subchondral cyst (thick arrow), beaking of the superior pubic symphysis, and moderate marrow oedema of the pubic bodies and adjacent pubic rami. Note also a hyperintense line (thin arrow). The significance of these lines (seen in some subjects) is not understood and is part of a study using correlative computed tomography scans.
Athletes with moderate or considerable tenderness of the pubic symphysis were more likely (χ2 = 12.8, p<0.01) to have pubic beaking of 8 mm or more.
There was an association between a past history of sports related chronic groin pain and each of the following: presence of a bone cyst (χ2 = 9.0, p<0.01); presence of pubic symphyseal fluid (χ2 = 9.4, p<0.01); beaking greater than 3 mm (χ2 = 7.9, p<0.01); moderate/considerable pubic symphysis joint irregularity (χ2 = 13.3, p<0.01). Very few athletes had these findings without any current or previous history of groin pain (table 3).
Discussion
CLINICAL FEATURES
The clinical features of chronic groin pain with tenderness of the pubic symphysis and/or superior pubic ramus is consistent with the clinical diagnosis of osteitis pubis. It has been stated that making this diagnosis is “clinically relatively easy with bone scan and Xray being helpful in confirmation”.1 It was not possible to undertake confirmatory x ray or bone scans in this study. It should also be stated that there is appreciable overlap of symptoms and signs between osteitis pubis and other sports related causes of chronic groin pain such as a sports hernia.5 This is particularly so when considering superior pubic ramus tenderness and the area slightly superior to this being the area of tenderness for a sports hernia. These points should be noted when interpreting the remainder of our discussion about our symptomatic group.
MRI SCANS: SIGNAL INTENSITY
The increased signal intensity of the pubic bone marrow seen in this study indicates BMO, a non-specific finding associated with stress injury.29 Additional causes of BMO include direct trauma, osteomyelitis, and infiltrative neoplasm,30, 31 but these were considered unlikely in the described clinical situation.
As the extent of BMO increased, a larger proportion of athletes were considered to be symptomatic. It has been proposed that MRI detects different stages in the continuum of bony response to stress, with a stress fracture being considered the end result of the biological reaction to external stress.32 The observation that a larger extent of pubic BMO increased the likelihood of symptoms is in keeping with bony stress response.
We used umpires as active running subjects who do not twist and/or cut in their usual training for comparison with the footballers. Of the umpires without pain and tenderness, only 25% had BMO of any degree and none had BMO regarded as significant, compared with the footballers in the same group (62% and 21% respectively; table 2). This is consistent with the known features of osteitis pubis that athletes who twist and turn seem to be most at risk but long distance runners are also affected.1
Five athletes meeting the symptomatic criteria did not have BMO. At the time of the study, two of this group had undertaken at least five months of a restricted training/running rehabilitation programme for groin pain. BMO may have resolved after rehabilitation with restricted training activities, or an alternative entity may have been responsible for the symptoms. Another two of the athletes experienced onset of symptoms in the two weeks before the study. Explanations for this could include (a) incorrect clinical diagnosis and (b) MRI changes may not yet have developed because of the recent onset of the symptoms. It has, however, been suggested that the MRI appearances seen in stress reaction of bone are abnormal before the onset of symptoms.32 The fifth case without BMO had MRI evidence of old Perthes disease and a small hip joint effusion, suggesting that an incorrect diagnosis had been made.
Alternative diagnoses of sports related chronic groin pain such as adductor tendinitis and posterior inguinal wall deficiency were not supported by the findings in this study.
CLINICAL FEATURES AND MRI FINDINGS
As described, there was a correlation between tenderness of the pubic symphysis assessed as grade 2 or above and the presence of beaking of 8 mm or more. Pubic beaking is considered to be due to hypertrophy of the superior pubic ligament and/or osteophyte formation. Tenderness in this region experienced by those with osteitis pubis may be due to pressure on the bony beak during palpation. The presence of superior pubic beaking was taken to indicate degenerative or other significant bony pathology which may also have been responsible for the clinical features.
HYPOTHESIS OF THE PATHOPHYSIOLOGY OF BMO
It is proposed that there are centres of rotation on the pubic bone near the pubic symphysis during simulated walking.33 Mechanical properties of the pubic symphysis joint show that the symphysis has some movement in the shear and rotation planes but resists distraction forces poorly.34 It seems reasonable to state that, in sports requiring intensive aerobic training, kicking, and sudden changes in running direction such as Australian rules football, there is an increase in forces on the pubic bone leading to an increased probability of fatigue bony stress injury in this region. Fatigue stress injuries are thought to be either compressive (common) or tension (uncommon) in nature. A stress fracture results from overload of the bone causing mechanical failure in a bone that is not capable of resisting these forces because of an inability to form sufficient bone (a compressive injury) or excessive bone resorption (a tension injury). It is hypothesised that a tension stress injury of bone seems the most likely cause of the BMO observed in this study, with the proposal being that the bone overload results from tension/torsional forces acting on the centres of rotation in a closed pelvic chain near the pubic symphysis. This remains an area for future study.
HYPOTHESIS OF THE PATHOPHYSIOLOGY OF THE OTHER MRI FINDINGS
A past history of sports related chronic groin pain without current symptoms did not correlate with pubic BMO signal intensity changes but did correlate with other MRI findings suggestive of degenerative symphyseal changes. The BMO seen in this study may represent an acute bony response to stress injury, with other MRI findings developing secondary to chronic motion or instability of the pubic symphysis joint region. Specifically, it is postulated that stresses across the pubic symphysis joint may lead to a loss of ligamentous/capsular integrity at this joint allowing abnormal motion. The latter may lead to degenerative changes, as visualised on MRI scans (superior beaking, pubic symphysis joint irregularity, and fluid signal in the pubic symphysis disc). This hypothesis cannot be verified until it can be shown that these MRI findings are a consequence of a stress response, and hence further investigation is needed. We are currently following the development, or otherwise, of these findings in athletes with a new diagnosis of groin pain and BMO of their pubic bone, with the use of serial MRI scans to attempt to verify our hypothesis.
In the clinical setting of a stress injury, the subsequent development of a movement disorder of the pubic symphysis may explain the degenerative bony changes and the chronicity of symptoms experienced by many sufferers of sports related chronic groin pain.
STRENGTHS AND WEAKNESSES OF THIS STUDY
Strengths of the study include: (a) its design, with examination before history taking; (b) no prior clinical knowledge of the athletes by the examining clinician and radiologists; (c) the strength of association between the clinical features and MRI findings; (d) the limited alternative diagnostic interpretations for the principal MRI finding of BMO as it is most likely a consequence of a stress injury.
Weaknesses include: (a) the interpretation of the clinical features as being consistent with a diagnosis of osteitis pubis without using the gold standard (x ray/bone scan) in making this diagnosis; (b) MRI findings showing no evidence of a sports hernia (posterior inguinal wall deficiency) should be interpreted with caution as it is generally accepted that this diagnosis is clinical only; (c) the interpretation that a tension/torsional force mechanism is the cause of the stress response is speculative as it is also quite likely there are compressive and shear forces; (d) the interpretation that the other MRI findings, such as features of degeneration, have been caused by a stress response is also speculative.
CONCLUSIONS
Athletes with groin pain and pubic symphysis and/or superior pubic ramus tenderness have clinical features consistent with the diagnosis of osteitis pubis. The increased signal intensity seen on MRI is due to pubic BMO. Hence an association was shown to exist between the clinical features of osteitis pubis and the MRI finding of pubic BMO. A high incidence of pubic BMO was also noted. Degenerative features on MRI such as subchondral cyst formation were associated with a past history of groin pain. We propose that a stress injury to the pubic bone is the most likely explanation for these MRI findings and may be the cause of the clinical entity osteitis pubis.
Acknowledgments
The authors acknowledge the financial support of DePuy, South Australian branch for assistance in radiographer payments. We thank Dr Greg Lovell and Dr Peter Barnes for their help with the manuscript and Mr Adrian Esterman, Department of General Practice, Flinders University, Adelaide for performing statistical analyses. We also acknowledge the MRI radiographers at Flinders Medical Centre and Perrett Medical Imaging and we would also like to thank the professional athletes of the football clubs (Adelaide Crows, Port Adelaide Power, and Norwood Redlegs) and umpires (SANFL Umpires group) who gave their time freely to participate in this study.
Presented at the Australian Conference of Science and Medicine in Sport, Adelaide, South Australia in October 1998. Winner of the Young Investigator award for the Best Clinical Paper.
No author or related institution has received any financial benefit from research in this study.
Take home message
Athletes that present with chronic groin pain and have tenderness of the pubic symphysis and/or superior pubic ramus have a high likelihood of having pubic bone marrow oedema as visualised by MRI. This oedema is probably a response to bony stress.