Article Text

Abstract
Objective: To conduct a detailed analysis of hamstring injuries sustained in English professional football over two competitive seasons.
Methods: Club medical staff at 91 professional football clubs annotated player injuries over two seasons. A specific injury audit questionnaire was used together with a weekly form that documented each clubs’ current injury status.
Results: Completed injury records for the two competitive seasons were obtained from 87% and 76% of the participating clubs respectively. Hamstring strains accounted for 12% of the total injuries over the two seasons with nearly half (53%) involving the biceps femoris. An average of five hamstring strains per club per season was observed. A total of 13 116 days and 2029 matches were missed because of hamstring strains, giving an average of 90 days and 15 matches missed per club per season. In 57% of cases, the injury occurred during running. Hamstring strains were most often observed during matches (62%) with an increase at the end of each half (p<0.01). Groups of players sustaining higher than expected rates of hamstring injury were Premiership (p<0.01) and outfield players (p<0.01), players of black ethnic origin (p<0.05), and players in the older age groups (p<0.01). Only 5% of hamstring strains underwent some form of diagnostic investigation. The reinjury rate for hamstring injury was 12%.
Conclusion: Hamstring strains are common in football. In trying to reduce the number of initial and recurrent hamstring strains in football, prevention of initial injury is paramount. If injury does occur, the importance of differential diagnosis followed by the management of all causes of posterior thigh pain is emphasised. Clinical reasoning with treatment based on best available evidence is recommended.
- football
- hamstring
- injury
- CT, computed tomography
- MRI, magnetic resonance imaging
Statistics from Altmetric.com
The hamstring strain is a condition well recognised by medical personnel, coaches, and athletes. Such injuries are a major cause of time lost from sport.1 Hamstring strains are among the most common injuries in sport and are most often observed in sports that involve sprinting and jumping.2–4 The initial Football Association Audit of Injuries study found that 12% of all injuries reported over two seasons were hamstring strains, this being the most prevalent injury. Players were 2.5 times more likely to sustain a hamstring strain than a quadriceps strain during a game.5
Many predisposing factors for hamstring strain have been suggested in the literature, including insufficient warm up,6,7 poor flexibility,6–8 muscle imbalances,6,7,9 muscle weakness,9,10 neural tension,11 fatigue,6,7 dys-synergic contraction of muscle groups,12 and previous injury.13,14 The evidence to substantiate these speculations is minimal and conflicting.12,15 The same holds true for the management and treatment of hamstring strains as there is no consensus on optimal rehabilitation,7,16 therefore management tends to be based on anecdotal evidence and experience rather than evidence based practice.
Hamstring strains are well known for their high rate of recurrence.16–19 It has been suggested that a premature return to play10,12,20 or an inappropriate rehabilitation programme10,12,13,21 may be responsible for reinjury.
Garrett22 stated that “Although muscle strains are frequently seen, our understanding of the pathophysiology, treatment, and recovery of these injuries is limited...”. The aim of this study was to provide information on the incidence, nature, mechanism of injury, and diagnostic investigation of hamstring strains. This included analysing differences in the age, position, and ethnic origin of players sustaining such injuries in football. The collection of such injury data would help to identify factors involved in injury occurrence, and in establishing the effectiveness of treatment and prevention of hamstring injuries in soccer.
METHODS
Player injuries were prospectively reported from July 1997 through to the end of May 1999 inclusive. A total of 91 of the 92 football clubs from the English football leagues (Premier and Football League) committed themselves to the project. Injuries were recorded by club physiotherapists and/or doctors on a specific player injury audit questionnaire designed for this study. Injury audit questionnaires for players who had returned to full training/competition during a particular week were returned weekly together with a form indicating which players had been absent and the number of days and competitive matches each had missed that week. Before the study, medical staff from clubs attended a briefing day and were issued with guidance notes on how to complete the questionnaires. Only professional players with a squad number were involved in the study. Participants were asked to complete a consent form and each club provided details of their squad at the beginning of each season. Table 1 presents the information obtained.
Division, playing position, and age distribution of the cohort at the beginning of the study
New players who joined the club were included, and players leaving clubs were omitted from the study if they did not stay within one of the four English leagues.
A recordable injury was defined as one sustained during training or competition that prevented the injured player from participating in normal training or competition for more than 48 hours (not including the day of the injury). Injuries unrelated to football were not included, nor was any absence due to illness. Injuries sustained during international duty were included, as details of such injuries were reported back to club medical staff. The severity of each injury was defined as slight, minor, moderate, or major depending on whether the player was absent from training or competition for two to three days, four to seven days, one to four weeks, or more than four weeks respectively. A similar classification system has been used elsewhere.23,24 Reinjury was defined as an injury of the same nature and location involving the same player in the same season. The dominant foot was defined as the predominant foot used for kicking a ball.
Data were analysed using SPSS (Chicago, Illinois, USA). Descriptive and comparative data are presented. The χ2 significance test was used to investigate differences, and statistical significance was accepted at p<0.05 level. All players agreed to participate in the study and there were no drop outs during the study period.
RESULTS
Of the 91 clubs starting the study, completed injury records for the entirety of the 1997/1998 and 1998/1999 competitive seasons were attained from 87% and 76% respectively. During the study period, 796 injuries to the hamstrings were documented, this being more than any other muscle group. There was no significant difference between the numbers of hamstring injuries sustained in the 1997/1998 season relative to the 1998/1999 season. Table 2 displays the classification of all hamstring injuries.
Classification of hamstring injuries
Hamstring strains accounted for 12% of the total injuries sustained over the two seasons. There was no significant difference between the observed frequency of hamstring strains to dominant and non-dominant limbs (53% v 45%) based on expected frequencies. There was, however, a significant difference in the number of hamstring strains across the four divisions, with most occurring in Premier League players (28%) (p<0.01). The distribution of hamstring strains across the other divisions was: division 1, 24%; division 2, 26%; division 3, 22%.
Table 3 shows the location of hamstring strains.
Location of hamstring strain injuries
The total number of days that players were absent over the two seasons from hamstring strains was 13 116, and a total of 2029 matches were missed, giving an average of 18 days and three matches missed per hamstring strain. A rate of five hamstring injuries per club per season was observed, the range being 0–16 hamstring strains within clubs. This resulted in 15 matches and 90 days missed per club per season.
Mechanisms of injury involving player to player contact were responsible for 7% of injuries, while non-contact injuries were responsible for 91% (p<0.01). A total of 57% of all hamstring strains were sustained during running. Figure 1 displays the non-contact mechanisms of hamstring strains.

Mechanism of non-contact hamstring strains. *Other includes dribbling, heading, and diving.
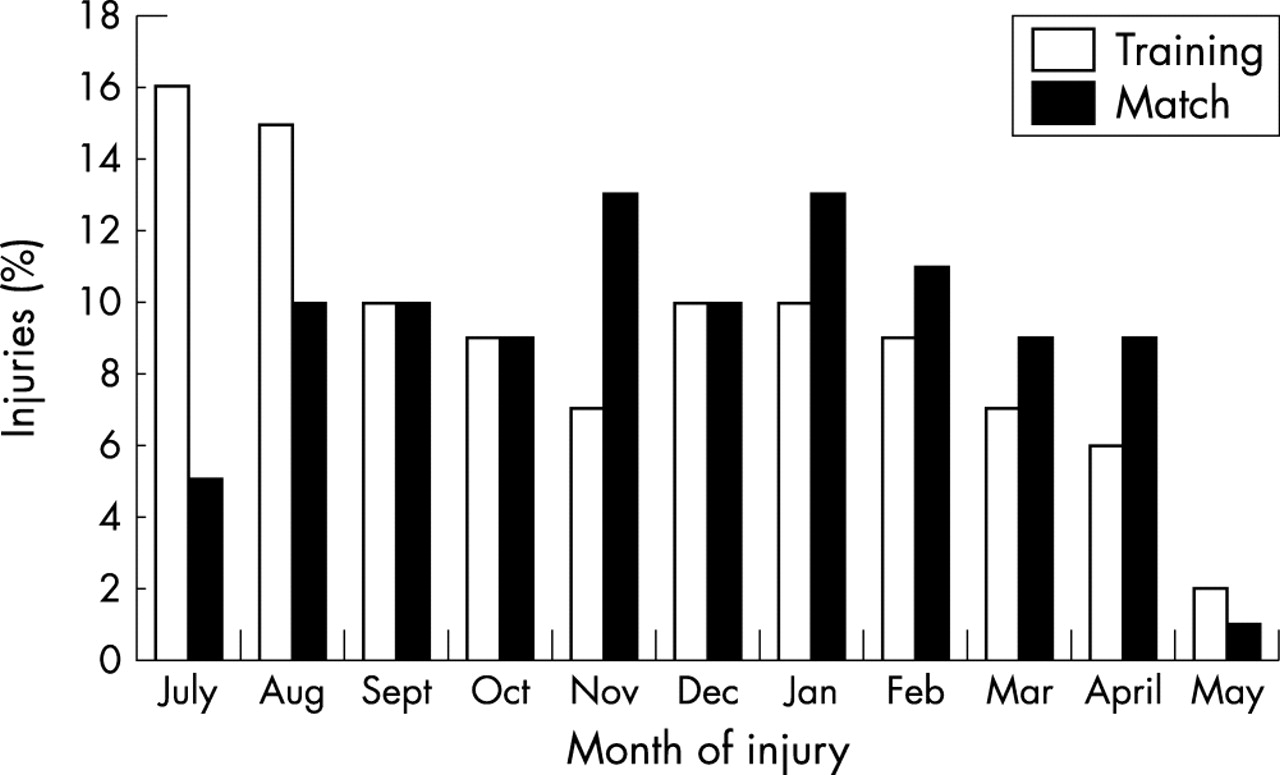
Figure 2 shows the number of hamstring strains sustained during training and matches throughout each month of the season. Approximately one third (32%) of hamstring strains were sustained during training and nearly two thirds (67%) during matches. On the basis of the percentage of total match and training injuries reported in the study (34% v 63%), there was no significant difference between the observed and expected frequency. Figure 3 shows the timing of match injuries. Nearly half (47%) of hamstring injuries sustained during matches occurred during the last third of the first and second halves of the match (p<0.01).

Month of injury of hamstring during training and matches.

{kind=link}
{kind=link}
{kind=link}
Time of hamstring strains sustained during match play.
Table 4 shows the number of hamstring strains by player position, age, and ethnic origin.
Hamstring strains by playing position, age, and ethnic origin
Based on observed and expected frequencies, goalkeepers sustained significantly fewer hamstring strains than outfield players (p<0.01). Players of black origin sustained significantly more hamstring strains than white players (p<0.05), and the 17–22 year old age groups sustained fewer hamstring strains than the older players (p<0.01).
The reinjury rate for hamstring strains was 12%, and the average reinjury rate for all injuries was 7% (p<0.01). There was no significant difference between the severity of initial injuries and reinjuries—that is, there was no difference in the number of training days or matches missed.
Of all the hamstring strains sustained, only 5% were diagnostically investigated using an imaging technique. The most commonly used technique was magnetic resonance imaging (MRI) (27), seven strains were scanned with ultrasound, and one player underwent both types of investigation. Only two players with hamstring strains had surgery, and nine received some form of injection.
DISCUSSION
In this study, a muscle strain was by far the most commonly diagnosed injury to the posterior thigh. Hamstring strains accounted for 12% of all injuries sustained over the two seasons and for the loss of 90 training days and 15 matches per club per season.
Each club sustained an average of five hamstring injuries per season. This is comparable to an Australian football study which observed an average of six hamstring strains per club per season, with hamstring strains representing 15% of all injuries.3
The high incidence of injury in this muscle group may be partly because the group functions over two joints3,5,18 and is therefore subject to stretch at more than one point.3,18 Also, the greater proportion of fast twitch fibres in the hamstring muscles compared with other thigh and leg muscles means that they are capable of high force production.5 Common muscle imbalance patterns may invoke the use of the hamstrings as a slow twitch muscle, which may predispose the muscle to injury when challenged to perform high velocity fast twitch actions. It may therefore be worth while addressing any muscle imbalances when assessing and treating these injuries.
The biceps femoris (53%) was the most commonly strained muscle of the hamstring complex. This finding is supported by other studies.1,5,25 The anatomy of the biceps femoris may help to explain its higher rate of injury. Firstly, it has a long and a short head, both with separate nerve supplies.26 This dual innervation may lead to asynchronous stimulation of the two heads.27,28 Mistimed contraction of the different parts of the muscle group may mean a reduced capacity to generate effective tension to control the imposed loads of the muscle.28
There may be anatomical variations in the attachments of biceps femoris, which may predispose certain people to injury.29 Burkett29 suggested that an extensive femoral attachment of the short head of the biceps femoris with an overlying strength deficit predisposes to hamstring strain. The long head of the biceps femoris originates from the lower part of the sacrotuberous ligament,20,26,30,31 therefore it could be argued that the biceps femoris has a triarticular function and is therefore more predisposed to injury than the other hamstring muscles. The insertion of the biceps femoris into the head of the fibula my also be a predisposing factor to injury. A previous knee or ankle injury resulting in alteration in the movement of the superior tibiofibular joint may affect the biomechanics of the biceps femoris. This notion is speculative. Zuluaga et al28 stated that incomplete knee excursion caused by meniscal damage may lead to excessive loading of the biceps femoris. The biceps femoris acts as a lateral rotator of the semiflexed knee and the extended hip.26 Given the rotational demands of football, this function may also predispose the biceps femoris to injury. Despite this, it suggests that the sacroiliac joint and the superior tibiofibular joint should be examined when assessing players with suspected biceps femoris strains. The function of the biceps femoris as a lateral rotator should also be acknowledged when strengthening and stretching this muscle.
It was interesting to note that nearly 20% of practitioners did not specify the exact name of the hamstring muscle injured, diagnosing the injury as “hamstring strain”. This could be for one of two reasons—either the therapist’s diagnosis was simply non-specific or the pathology was so non-specific that an accurate diagnosis was not possible. In six out of 32 MRI scans performed on players with posterior thigh injury (non-contact mechanism), the scan was normal and not consistent with hamstring muscle strain; the authors diagnosed this as “referred posterior thigh injury”.16 Garrett et al1 found that two out of 10 patients who sustained acute hamstring injuries had no acute abnormality on computed tomographic (CT) scan. This supports the notion that the presentation of posterior thigh pain does not necessarily mean “there is always an isolated local pathology”32 within the muscle. Upton et al33 stated that most problems have a basis within the muscle complex, but, in 15% of cases, associated factors are involved. Such factors may include lumbar spine, sacroiliac joint, neural tension, ischiogluteal bursa, piriformis syndrome, avulsion of the ischial tuberosity, compartment syndrome of the posterior thigh, bone tumours, and hamstring syndrome/fibrous adhesions. Posterior thigh symptoms may be local or referred. Readers are encouraged to be aware of this and the various possible differential diagnoses when assessing players with posterior thigh pain. Correct diagnosis is the basis of adequate treatment,8 and management should be aimed at correcting all abnormalities detected on examination.23
Devlin18 stated that “imaging is not always performed” because most hamstring injuries are managed conservatively. Of the 749 hamstring strains in our study, only two required surgery. O’Connor et al34 described three case studies of athletes with chronic and unresolving posterior thigh pain. The cases were eventually diagnosed as chronic compartment syndrome of the posterior thigh and were successfully treated with a limited fasciectomy. This again highlights the importance of structures other than the hamstring muscles themselves being responsible for posterior thigh pain.
Only 5% of hamstring strains in this study were diagnostically investigated, with MRI being the most commonly used technique. Current diagnostic techniques may not be sensitive enough to determine the source of posterior thigh pain, especially where adverse neural tension, sacroiliac joint, or lumbar spine dysfunction is suspected as the cause of symptoms.20 MRI may not be necessary for routine imaging of muscle strain injury, as accurate history taking and physical examination skills provide a sound diagnosis of muscle strain injury in most cases.18,25 The use of diagnostic investigations in assessing and treating hamstring injuries is an area that requires further research.
This study shows that an overwhelming number of hamstring strains occurred while players were running. The speed (sprinting, jogging), nature (with or without the ball, backwards, sideways), and phase (decelerating, acceleration, etc) of running when the injury was sustained was not recorded in this study, although this information would have been useful to learn more about the causes of these injuries. Analysis of the biomechanics of running suggests that hamstring strains occur during the end of the swing phase when the hamstrings are working to decelerate the limb while also controlling extension of the knee.14 The hamstrings must change from functioning eccentrically, to decelerate knee extension in the late swing, to concentrically, becoming an active extensor of the hip joint. It has been proposed that this rapid changeover from eccentric to concentric function of the hamstring is when the muscle is most vulnerable to injury.14 Zuluaga et al28 also suggested that, during this swing phase, the hamstrings are placed under extremely high loads in an elongated position. This has implications for rehabilitation, as the hamstring must be functionally strong in the phase of injury before return to play. This is why an individualised rehabilitation programme emphasising high velocity eccentric exercises (with the hamstrings in an elongated position) has been proposed by many authors during the late stage of functional rehabilitation.12,15,19,23 Garrett et al4 suggested that, because hamstring muscles are most often injured in high speed or high intensity situations, the hamstrings must be trained and rehabilitated at a high intensity. In further support of this, Jönhagen et al20 proposed that one of the reasons for recurrence of hamstring injury was poor eccentric hamstring strength, especially at high angular velocities.
This study shows that players with a black ethnic origin are more at risk of sustaining a hamstring strain than white players. No other studies comparing these ethnic origins with risk of hamstring injury could be found. However, in a study of clinical risk factors for hamstring injuries in Australian rules football, Verrall et al14 found that players of aboriginal descent had a significantly greater risk of sustaining a hamstring injury. They proposed that, as such players are generally considered to be the “fastest, most skilful and most exciting players”, they may have a greater proportion of type II fibres, which may predispose them to injury. A small study that looked at the treatment of hamstring strains with sacroiliac mobilisation showed that those people with increased anterior tilt of the inominate bones were more at risk of sustaining a hamstring injury.17 It is common for players of black origin to have an anteriorally tilted pelvis, perhaps predisposing them to this type of injury. Although this is speculative, the anatomical link between the hamstrings, lumbar spine, pelvis, and sacrum suggests that the biomechanics of these structures should be evaluated when assessing posterior thigh pain.
This study also shows that players in the 17–22 age group had a lower risk of sustaining a hamstring injury. Verrall et al14 also found that hamstring strains were more common in older people but were unable to offer an explanation for this. Goalkeepers sustained fewer hamstring strains than outfield players, which may be explained by the demands of the goalkeeper, as running (which is the principal mechanism of injury for this type of injury) is not a major component of the goalkeeper’s game. Hamstring injuries were most common in the Premiership and became less common in the lower leagues. This may reflect the increased physical demands in the higher leagues where the pace of games may be faster.
Hamstring strains were mostly sustained at the end of matches and training sessions. This would support the notion that fatigue may be a predisposing factor for such injuries as previously discussed. A complex neuromuscular coordination pattern appears to occur during the running cycle.14,18 Any factor that adversely affects this pattern may result in injury.14 It has been suggested that the dual innervation of the biceps femoris may cause asynchrony, as poor coordination may allow separate parts to activate at different times.14 Kyröläinen et al35 looked at the recruitment pattern of leg muscles during different running speeds. The greatest changes in muscle activity pattern were observed in the biceps femoris muscles as the speed increased from a slow jog to maximum speed. Pinniger et al36 found that, when footballers became fatigued during sprinting, there was earlier activation of the biceps femoris and semitendinosus muscles. Asynchrony may be due to local muscle fatigue14 and/or neural fatigue as a result of “irritation or damage along the path of the nerve supplying the muscle”.20 General fatigue secondary to poor sleep patterns, stress, or suboptimal nutrition could result in central nervous system fatigue. A muscle’s decreased ability to generate force is thought to reduce its energy absorption capacity, which in turn predisposes the muscle to injury.24,37 This highlights the importance of addressing the endurance of the hamstring muscle group in preventive and rehabilitation programmes. Emphasis is generally placed on increasing the strength and power of this muscle group.
Take home message
Hamstring strains are the most common injury in football accounting for an average of 90 days and 15 matches missed per club per season. Prevention of initial injury is therefore emphasised. The importance of differential diagnosis and management of all causes of posterior thigh pain are highlighted in the treatment of such injuries.
The recurrence rate for hamstring injuries was 12%, which was significantly greater than the reinjury rate for all other injuries (7%). The high reinjury rate has been cited as one of the frustrations of treating hamstring injuries.14 It is generally believed that skeletal muscle is capable of virtually complete regeneration after injury.38 However, Stauber et al39 pointed out that, if pronounced connective tissue proliferation is present after repeated muscle injury, complete restoration of normal function may be impaired or even impossible. In their study, which looked at the recovery from six weeks of repeated strain injury to rat soleus muscle, Stauber et al40 concluded that the muscle recovered slowly and incompletely from chronic strain injury. These authors suggested that further work to design optimal intervention and prevention procedures for muscle fibrosis from chronic muscle injury was needed. In their study of CT of hamstring muscle strains, Garrett et al1 noted the presence of calcifications at the involved site of some college athletes with hamstring injuries. The authors stated that the significance of these calcifications was unclear, but pointed out that the CT appearance of calcification does not always return to normal. This shows that the exact pathophysiology of reinjury remains unknown. Therefore, complete rehabilitation of injuries before return to play is emphasised, but primary prevention of initial injuries is even more important. Practical studies evaluating the use of strategies to prevent hamstring strain in football would be useful.
It is interesting to note that some clubs sustained very few hamstring strains throughout the two seasons, whereas other clubs sustained a large number. Similarly some clubs reported no recurrence of these injuries, whereas others reported a high rate of recurrence. This may represent a large number of variables in diagnosis, training techniques, and medical management, but it does at least suggest that these injuries can be prevented and managed.
This study did not record exposure data, making it difficult to compare the results with other studies. However, accurate exposure time would have been difficult to obtain given the large number of clubs participating in the study. At the outset of the study, there were no criteria for what constituted a hamstring strain so there may be wide variation in diagnosis between medical personnel. Referred posterior thigh pain may also have been missed in this study. More detail on running as a mechanism of injury, specifying the nature, speed, and phase, would also have helped, as would more detail on playing position. Future studies should address these issues.
Hamstring strains are common in football. A rate of five hamstring injuries per club per season was observed, resulting in 15 matches and 90 days missed per club. The biceps femoris muscle was the most commonly strained of the hamstring group. Such injuries were usually sustained during running and at the end of match halves. The groups of players sustaining higher than expected rates of hamstring injury were Premiership and outfield players, players of black ethnic origin, and players in the older age groups. The reinjury rate for hamstring injury was 12%. In trying to reduce the number of injuries and recurrences of hamstring strains in football, prevention of the initial injury is vital. If injury does occur, the importance of differential diagnosis, followed by the management of all causes of posterior thigh pain, is emphasised. Clinical reasoning with treatment and rehabilitation based on best available evidence is recommended.