Article Text

Abstract
Background: Lateral ligament ankle sprains are the single most common sports injury.
Objective: To determine the functional outcome of the ankle joint after a moderate or severe inversion injury, comparing standard treatment with an elastic support bandage against an Aircast ankle brace.
Design: Prospective, randomised controlled trial.
Setting: Two accident and emergency departments.
Method: Fifty patients presenting consecutively were randomised into two equal groups: one group was treated with an elastic support bandage and the other with an Aircast ankle brace. All patients were given a standardised advice sheet referring to rest, ice, compression, and elevation. Patients were reviewed after 48–72 hours, 10 days, and one month.
Primary outcome measure: Ankle joint function assessed at 10 days and one month using the modified Karlsson scoring method (maximum score 90).
Secondary outcome measure: The difference in ankle girth (swelling) and pain score at 10 days.
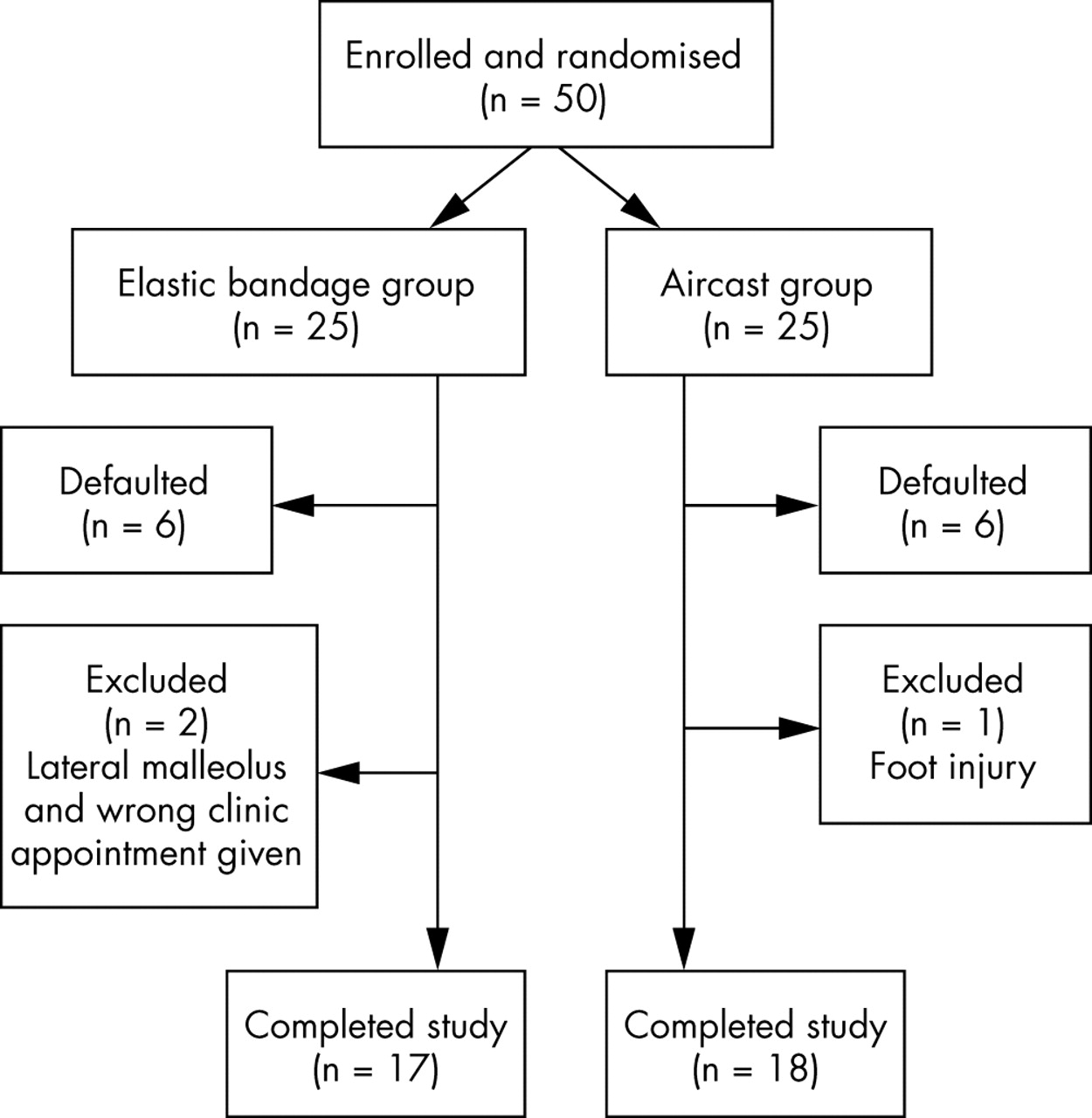
Results: Seventeen patients in the elastic support bandage group (six defaulted, two excluded) and 18 patients in the Aircast ankle brace group (six defaulted, one excluded) completed the study. There were no significant differences between the two groups at presentation in terms of age (mean 35.3 and 32.6 years respectively), sex, dominant leg, left or right ankle injured, previous injury, time to presentation (median three and four hours respectively), difference in ankle girth (mean 14.5 and 14.3 mm respectively), and pain scores (mean 6.2 and 5.8 respectively). The Karlsson score was significantly higher in the Aircast ankle cast group than in the elastic bandage group at 10 days (mean 50 v 35, p = 0.028, 95% confidence interval (CI) 1.7 to 27.7) and one month (mean 68 v 55, p = 0.029, 95% CI 1.4 to 24.8) (Student’s t test). There was no difference between the groups in the secondary outcome measures (swelling, p = 0.09; pain, p = 0.07). When hierarchical multiple regression analysis was used to correct for possible baseline confounding factors, the Aircast ankle brace group was significantly associated with higher Karlsson scores at 10 days (p = 0.009) and one month (p = 0.024).
Conclusion: The use of an Aircast ankle brace for the treatment of lateral ligament ankle sprains produces a significant improvement in ankle joint function at both 10 days and one month compared with standard management with an elastic support bandage.
- ankle sprain
- elastic support bandage
- Aircast ankle brace
- functional outcome
Statistics from Altmetric.com
Ankle ligament sprains are the single most common sports injury, accounting for 19–23% of all sports injuries presenting to accident and emergency (A&E) departments.1–3 It has been estimated that an ankle injury occurs everyday per 10 000 of the population.4,5 About 90% are inversion injuries affecting the lateral ligament complex.6 Ankle injuries also account for 3–5% of overall attendances at A&E departments in Britain7,8 and 2–6% of presentations to emergency departments in the United States.9
However, despite the high incidence of this injury, there often appears to be no common regimen for their management, with a wide spectrum of treatment options available. In most A&E departments, patients are given an elastic support bandage, but in some departments a wool and crepe wrap round bandage is used. It is also not uncommon for elastic taping to be applied. These management strategies are often passed from senior to junior ranks with only anecdotal evidence to justify their use. With the medical community moving towards the practice of evidence based medicine, research is required to validate current treatment concepts to determine the optimum functional outcome.
Ankle sprains have been classified into grades I, II, and III according to macroscopic appearance and clinical findings. For the purpose of this study, the terms mild, moderate, and severe were used corresponding to grades I, II, and III respectively. A mild ankle sprain presents with minimal swelling, localised tenderness, and minor functional deficit. This type of injury generally does not require x ray examination. Moderate and severe ankle sprains encompass a spectrum of significant pain, swelling, haematoma formation, difficulty or inability to weight bear, and degrees of functional impairment. A radiograph is required to exclude associated fractures. Mild ankle sprains were not included in the study.
The aim of this study was to determine the functional outcome of the ankle joint after a moderate or severe inversion injury, comparing standard treatment with an elastic support bandage (fig 1) with the application of a semi-rigid ankle brace manufactured by Aircast, in patients presenting acutely to an A&E department. The Aircast ankle brace used consists of two contoured thermoplastic lateral straps lined with foam pads and designed to fit against the medial and lateral malleoli of the ankle joint. There are two aircell compartments present in the thicker distal portion, and the thinner proximal area of padding contains a single layer. At the ankle joint, the padding is contoured to fit around the malleoli. The aircells can be supplemented with additional air through an inlet port using a length of plastic straw which is supplied with the brace (this was not done in this study). The rigid sidewalls are held in place with Velcro strapping. The brace is self applied, reusable, adjustable, and can be worn during the rehabilitation phase (fig 2).
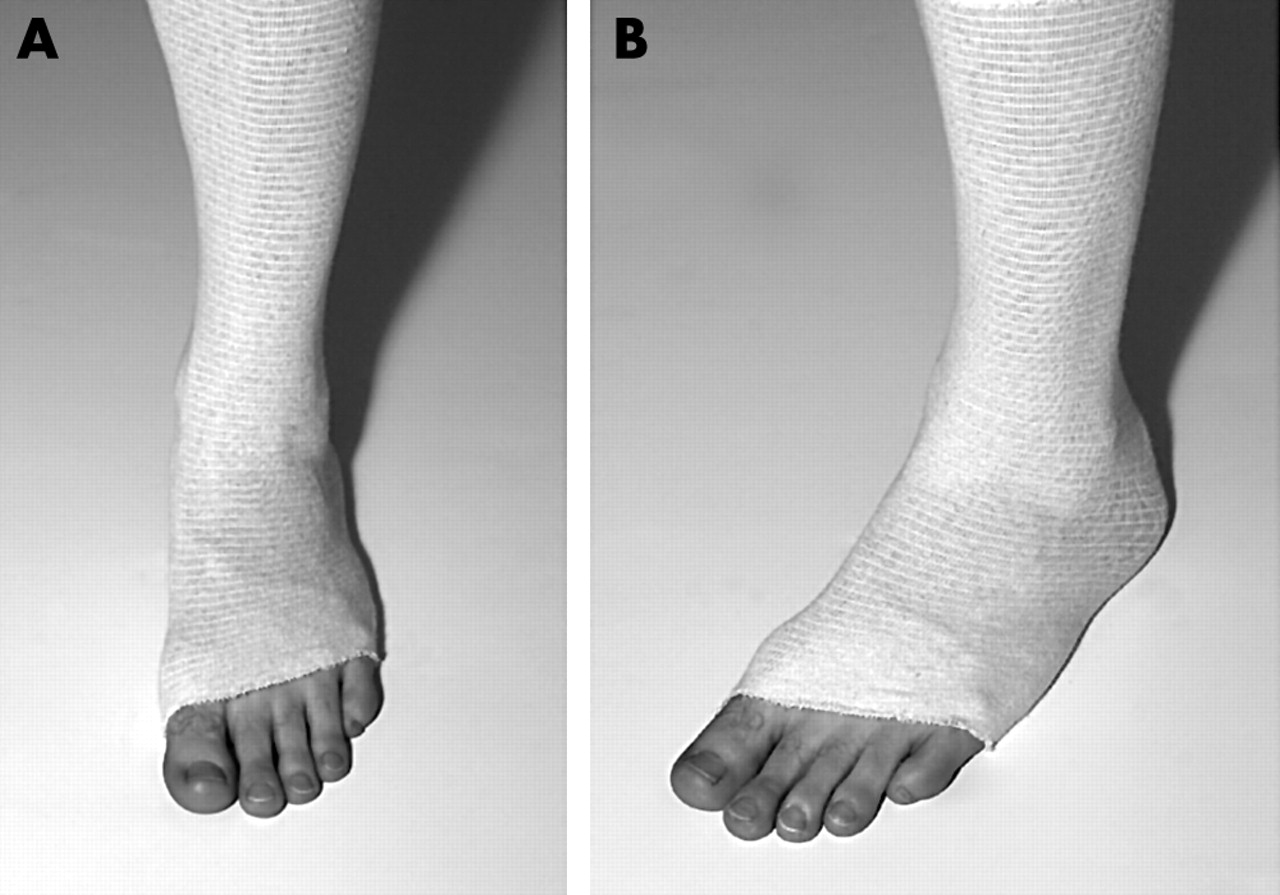
Elastic support bandage applied to a sprained ankle.

Aircast ankle brace applied to a sprained ankle.
METHOD
Setting
The study was conducted in the A&E departments of two district general hospitals: Crosshouse Hospital, Kilmarnock, Scotland and Dumfries & Galloway Royal Infirmary, Dumfries, Scotland. Both departments serve combined urban and rural populations managing 50 000 and 33 000 new attendances respectively each year.
Study design
Fifty patients presenting consecutively within 24 hours of sustaining a moderate or severe lateral ligament sprain after an ankle inversion injury were randomised into two equal groups. Fracture was excluded by x ray examination. Only adults were recruited (aged 16 years and over). After informed written consent was obtained, each patient was allocated to use either an elastic support bandage or an Aircast ankle brace. A standard proforma for all patients was completed detailing age, sex, time to presentation, dominant leg, left or right ankle injured, previous injury, ankle girth, and pain scores. All patients included in the study were given a standardised advice sheet referring to the principles of RICE (rest, ice, compression, and elevation) for use after an acute soft tissue injury. Analgesia and crutches were given as required. Review arrangements were made for 48–72 hours, 10 days, and one month. The following exclusion criteria were applied:
-
Age <16 years
-
Deltoid ligament injuries
-
>24 hours since injury occurrence
-
Fractures
-
Multiple injuries
-
Residual symptoms from a previous injury
-
Dementia
-
Mental illness
-
Intoxication (alcohol or drugs)
-
Long term mobility problems
-
Neurological conditions
-
Non-local residents
Randomisation
Patients were randomised for the trial using block randomisation. Fifty small pieces of white paper were obtained. “Elastic bandage” was written on half of the pieces of paper and “Aircast®” on the other half, and they were all folded. These were drawn randomly by an independent person and placed into 50 brown envelopes numbered consecutively from 1–50 and sealed. The first 35 envelopes were allocated to Crosshouse Hospital, and the remainder to Dumfries & Galloway Royal Infirmary. The authors were blinded to which treatment each patient would receive until the envelope was opened on recruitment to the study.
Outcome measures
The primary outcome measured was ankle joint function. This was assessed at 10 days and one month using a modified version of the Karlsson scoring scale. This is a statistically validated scoring scale devised by Karlsson and Peterson10,11 and can be used to measure ankle joint function in the rehabilitation phase after an acute ligament injury. From a maximum score of 90, points are given for a series of eight categories assessing the following areas: pain (20), swelling (10), instability (subjective) (15), stiffness (5), stair climbing (10), running (10), work activities (15), and the use of a support device (5). Table 1 outlines the Karlsson scoring scale.
Karlsson scoring scale
Secondary outcome measures, recorded at 10 days only, consisted of the difference in ankle girth (swelling) between the injured/uninjured ankles and the difference in pain scores compared with initial presentation. Ankle girth was defined as the circumferential measurement of the ankle at the level of both malleoli and noted in millimetres using a tape measure. Owing to the practicalities of A&E shift work, it was not possible for the same doctor to measure ankle girth on each occasion. Pain scores were obtained using a standard subjective visual analogue scale from 0 to 10, with 0 analogous to “no pain” and 10 equivalent to “maximal pain”.
Statistical methods
Univariate analyses were performed using Student’s unpaired t test, the Mann-Whitney U test, the χ2 test, or Fisher’s exact test, where appropriate. Multivariate analysis to correct for confounding factors was performed using hierarchical multiple regression. All tests were two tailed, and statistical significance was regarded as p<0.05. Statistical analyses were performed using SPSS version 10. The absence of published data on the variance of the Karlsson score made a prospective power calculation for our primary outcome measure impossible. However, a retrospective assessment indicates that a study with complete data on 17 subjects in each group would have about 60% power to detect a difference of 15 in the mean Karlsson score.
RESULTS
Of the 50 patients enrolled into the study, 29 (58%) were male and 21 (42%) female. The age range was 16–58 years (mean 32.2). The number of patients eligible to be enrolled in the study but who declined is not known. Left and right ankles were injured equally. Forty two (84%) of the patients were right leg dominant, and 13 (26%) had sustained a previous injury to their ankle. Thirty one (62%) injuries were accidental in origin, and the remaining 19 (38%) were sports related. Levels of physical activity before injury were not noted.
Seventeen patients in the elastic support bandage group completed the study (six defaulted and two were excluded). Eighteen patients in the Aircast ankle brace group completed the study (six defaulted and one was excluded) (fig 3). Table 2 shows the baseline characteristics of all subjects enrolled in the study. There were no significant differences in any baseline characteristic between the two groups for either the subjects who completed the study or those who either defaulted or were excluded.
Baseline characteristics of all subjects enrolled in study
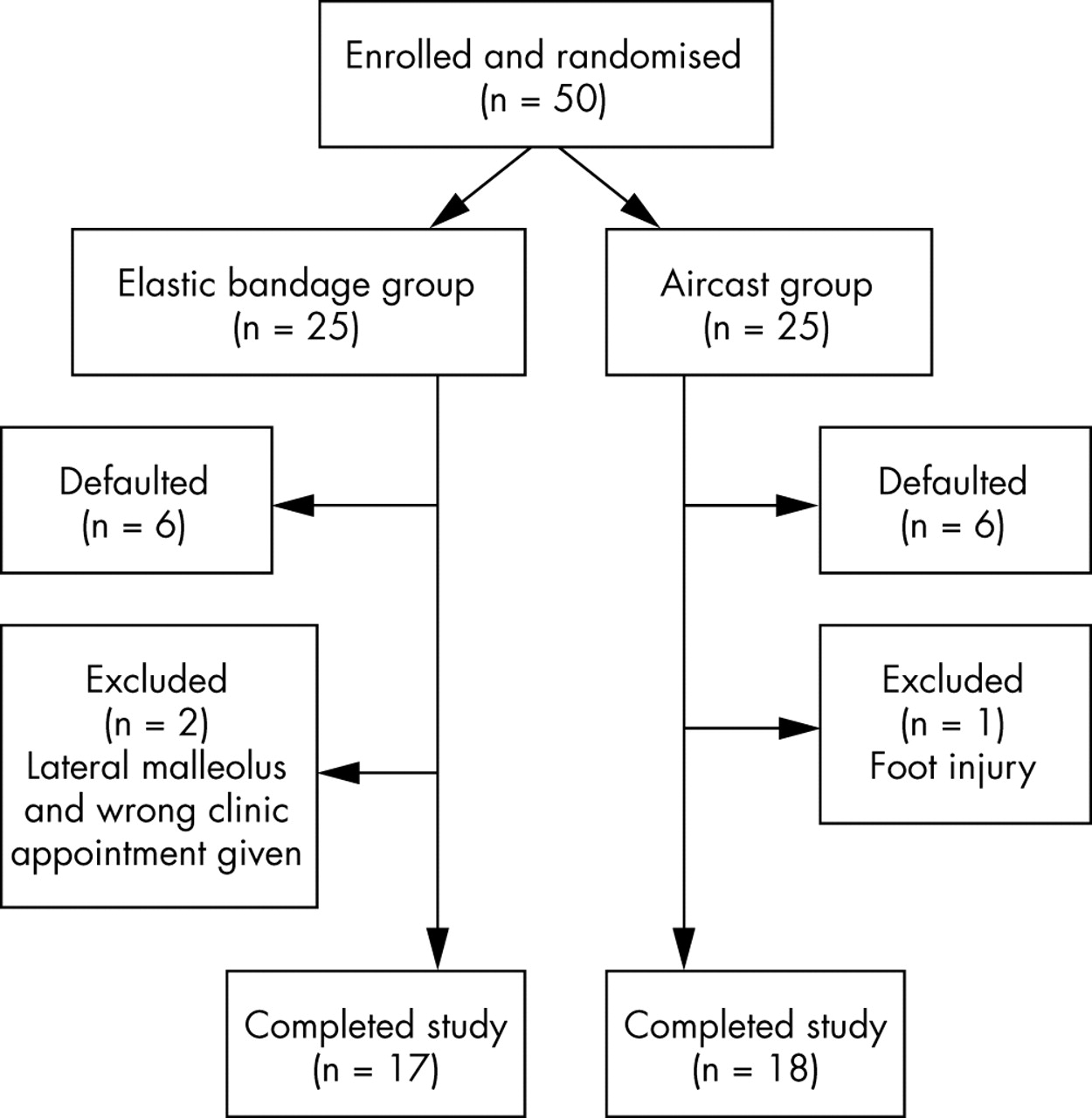
Consort diagram.
When Student’s t test was used, the Karlsson score was significantly higher in the Aircast ankle brace group than the elastic support bandage group at day 10 (mean 50 v 35, p = 0.028, 95% confidence interval 1.7 to 27.7) and one month (mean 68 v 55, p = 0.029, 95% confidence interval 1.4 to 24.8) (fig 4). When hierarchical multiple regression analysis was used to correct for possible baseline confounding factors, the Aircast ankle brace group was significantly associated with higher Karlsson scores at day 10 (p = 0.009) and one month (p = 0.024, 95%) (table 3).
Karlsson scores

Karlsson scores for the elastic bandage and Aircast ankle brace groups.
There were no significant differences between the two groups in the secondary outcome measures using Student’s t test: mean ankle girth: elastic bandage 14.4, Aircast ankle brace 8.5; p = 0.09; 95% confidence interval −1.1 to 12.7 (fig 5); mean pain scores: elastic bandage 2.9, Aircast ankle brace 1.8; p = 0.07, 95% confidence interval −0.01 to 2.3 (fig 6). However, with hierarchical multiple regression analysis, a significant difference in ankle girth between the two groups was noted (p = 0.014). No significant difference in pain scores was shown (p = 0.095) (table 4).
Pain scores and ankle girth at 10 days

Difference in ankle girth between the elastic bandage group and Aircast ankle brace group at presentation and 10 days.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pain scores in the elastic bandage group and Aircast ankle brace group at presentation and 10 days.
DISCUSSION
A sprained ankle is an extremely common injury seen in A&E departments for initial management. The mechanism of injury is not confined to the sporting arena, but often occurs accidentally during normal daily activities. It affects a wide age group and can result in considerable disability and interference in the everyday lives of ordinary people. The treatment goal for a competitive athlete will include early and effective return to sport with no residual symptoms, and, for patients attending after an accidental injury, a return to work or daily activities as soon as possible is normally desired.
However, despite their regular occurrence, management of this injury varies widely between A&E departments and often between clinicians working in the same department. There is as yet no “gold standard” method of management used universally. Instead clinicians rely on a combination of personal experience and clinical judgment.
The use of an ankle orthosis tends to be limited to sports groups or teams that are supervised by either physiotherapists or sports medicine practitioners. Little research has been directed towards management of such injuries in the general population, coordinated through a busy A&E department where resources will be restricted and orthosis use limited.
Management strategies can be divided into three main categories: cast immobilisation, operative repair, and functional treatment (bandage or ankle brace and mobilisation). A diverse array of studies is present in the literature comparing one of these methods against another. As a result of the heterogeneous nature of the various research projects, they perform poorly under meta-analytical review. It is difficult to compare the results of studies directly, but a few common themes have emerged.
Operative repair may be advocated for the definitive treatment of a severe ankle sprain resulting in instability, but studies have shown little long term benefit over conservative management.4,12 Early mobilisation of ankle sprains has been shown to be more comfortable, result in less pain, and provide an earlier return to work than treatment with cast immobilisation.13,14 Cast immobilisation does not improve healing compared with an active mobilisation rehabilitation programme and may have negative implications in relation to muscle wasting and stiffness.4 Functional treatment is considered better in achieving more effective mobilisation and an earlier return to daily activities.11,13 The use of ankle braces has been shown to be superior to an elastic support or compression bandages.15 Patients treated with an elastic support bandage took longer to return to work11,16,17 and reported increased subjective instability.16 One study did not even detect any symptomatic difference between a group who received no treatment for their sprain compared with those receiving an elastic support bandage.2 With various types of ankle brace available on the market, the best one to use remains open to debate.15 On the basis of current evidence, a management strategy should therefore use the principle of functional treatment advocating support with a form of ankle brace and early mobilisation to reduce the potential for long term residual complications.13,18
Concern has been raised over the effectiveness of applying elastic support bandages to sprained ankles in A&E departments without supportive evidence.2,19 Common sense and anecdotal evidence support these concerns; however, patients are often reassured by the subjective feeling of support that an elastic bandage provides. Recent papers have highlighted that, despite the lack of evidence, elastic support bandages are currently used as first line treatment in more than 70% of British A&E departments.20,21 Aircast ankle braces are used selectively in 7.2% of departments, and have never been used by more than 70% of all units.20 In our study, a statistically significant improvement in the functional outcome of the ankle joint was present in the Aircast ankle brace group at both 10 days and one month after the injury. The Karlsson scoring scale was used, as it provided a practical and reproducible method of assessing ankle joint function. The scale reflects many of the subjective measures that may be considered a determinant of adequate ankle function. We did not analyse the specific components of the score that contributed to the overall differences between the groups. This result only proves that the Aircast ankle brace is superior to an elastic support bandage in determining functional outcome. Its does not prove that patients treated with an elastic support bandage derived no benefit. Interestingly, both groups had a higher Karlsson score at one month than at 10 days, suggesting that, independent of the treatment used, the injury will improve progressively with time. Patients in the Aircast ankle brace group also reported a great deal of comfort and satisfaction using the brace.
There was no significant difference between the two groups with regard to ankle girth, but when hierarchical multiple regression analysis was applied, a significant difference was shown, suggesting that the use of an ankle brace possibly had an effect on the degree of ankle swelling. The validity of this assumption is debatable. The method of assessing ankle girth by manual measurement of the circumference of the joint with a tape measure is open to practical error. More than one investigator measuring the girth introduces the potential for further error. Other more accurate and reproducible methods—for example, volume displacement of water in a “dunk tank”—can be used to calculate swelling, but these are impractical to perform in an A&E department. Therefore it would be prudent to disregard this value. With respect to pain scores, no difference was shown between the two groups. This result was predictable because of the highly subjective method of scoring pain using visual “pain ladders” and the difference present between patients in determining both pain threshold and perception.
What is already known on this topic
Ankle sprains are a common injury seen in A&E departments. It is widely accepted that functional treatment produces a superior outcome than immobilisation. However, the method of functional treatment used to support the ankle joint is still open to debate.
This study is limited in its conclusions by several factors. Statistical analysis included correction for baseline variables; however, the use of analgesia and crutches was excluded. Analgesic preparations used differed in the two departments. The prescribing of crutches can vary between medical staff, as does the perceived requirement for crutches among patients. Follow up of patients ended after one month, but this is longer than routine A&E review. Concern may be raised over the small sample size. However, this has to be taken into consideration within the limits of performing research in busy A&E departments. Despite the frequency of presentation, patients were often reluctant to be recruited into the study. A long waiting time before being seen by medical staff and the practicalities of travelling to three review clinic appointments in a large geographical area were cited as reasons for non-participation. The large proportions of patients that attend A&E departments under the influence of alcohol, drugs, or as the result of violence also affect recruitment. The study could not be truly double blinded. Although the authors did not know which treatment a patient would receive until the envelope was opened, it was not possible to conceal this at the review clinics because of residual skin impressions on the ankle left by either treatment, thus introducing an element of possible bias.
Although the economic benefits that the use of an ankle brace may produce is outwith the remit of this paper, it is important to consider that, although more expensive at source than an elastic support bandage, if patients improve more quickly and return to work earlier, there may be possible economic benefits for the state. One study in 1997 estimated potential financial savings equivalent to US$8 million per year to the economy if all ankle sprains in Sweden were managed with a brace rather than surgery or cast immobilisation. The initial increased cost of bracing would be recouped by achieving return to work half a day earlier.22
What this study adds
This study compares the use of an elastic support bandage, used in most A&E departments, with the use of an ankle brace manufactured by Aircast. The results suggest that the latter produces a significant improvement in ankle joint function at both 10 days and one month.
CONCLUSION
The results obtained in this study suggest that the use of an Aircast ankle brace in the treatment of moderate and severe lateral ligament ankle sprains, presenting within 24 hours of injury, produces a significant improvement in ankle joint function, at both 10 days and one month, compared with standard management with an elastic support bandage. There is no significant difference in ankle girth (swelling) or pain scores at 10 days between the two treatment methods. Further research is required on a larger sample group to confirm this hypothesis, with the opportunity of producing a cost effective analysis of any perceived advantages.
Acknowledgments
We thank the medical and nursing staff of both A&E departments for their assistance with this study, particularly Mr James Stevenson and Dr Crawford McGuffie for their support and enthusiasm.
REFERENCES
Footnotes
-
Patient consent has been obtained for figures 1 and 2
-
Competing interests: none declared