Article Text

Abstract
A literature review was employed to evaluate the current epidemiology of injury related to the safety and efficacy of youth resistance training. Several case study reports and retrospective questionnaires regarding resistance exercise and the competitive sports of weightlifting and powerlifting reveal that injuries have occurred in young lifters, although a majority can be classified as accidental. Lack of qualified instruction that underlies poor exercise technique and inappropriate training loads could explain, at least partly, some of the reported injuries. Current research indicates that resistance training can be a safe, effective and worthwhile activity for children and adolescents provided that qualified professionals supervise all training sessions and provide age-appropriate instruction on proper lifting procedures and safe training guidelines. Regular participation in a multifaceted resistance training programme that begins during the preseason and includes instruction on movement biomechanics may reduce the risk of sports-related injuries in young athletes. Strategies for enhancing the safety of youth resistance training are discussed.
Statistics from Altmetric.com
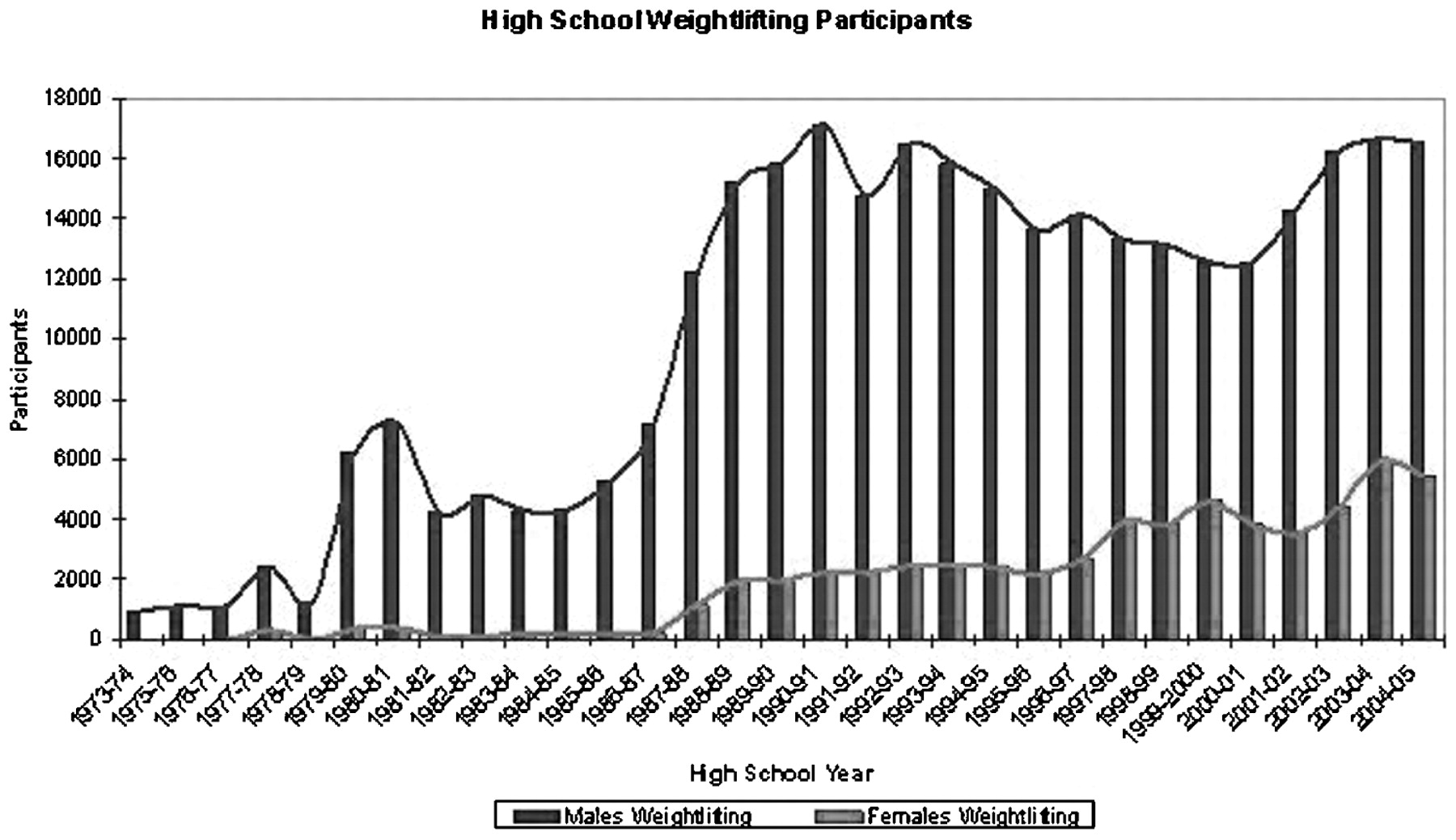
There is a growing number of young athletes participating in resistance training programmes in school-based programmes, fitness facilities and sport training centres to enhance their athletic performance and reduce their risk of injury during practice and sport competition (fig 1).1 Although some clinicians once considered resistance training unsafe and potentially injurious to the developing musculoskeletal system,2 evidence related to the safety and efficacy of resistance exercise for children and adolescents has increased over the past decade.3 4 5 6 7 The qualified acceptance of supervised and well-designed youth resistance training by medical, fitness and sport organisations is now becoming universal.8 9 10 11 12 13

Reported high school “weightlifting” (ie, resistance training) participants after the induction of Title IX (school years 1973–2005) based on the participation estimates from the High School Athletics Participation Survey conducted by the National Federation of State High School Associations. Reprinted from Quatman et al.1 Reproduced by permission of the National Strength and Conditioning Association, Colorado Springs, Colorado, USA.
Current public health initiatives now aim to increase the number of youth who participate regularly in “muscle strengthening” activities,14 and contemporary physical education programmes include resistance training as part of a health-enhancing approach to fitness education.15 16 In addition, some fitness facilities and sport centres serve the youth fitness market by providing programmes for children and adolescents that enhance musculoskeletal strength, improve motor skill performance and reduce the risk of sports-related injuries.5 7 11
On the other hand, there is substantial interest and concern from the general public, medical societies and the scientific community regarding the safety and appropriateness of resistance training for young athletes. Boys and girls as young as 6–8 years of age participate in resistance training activities and the weekly training volume (combined sports practice, sports competition and resistance training) of some teenage athletes rivals that of adults.17 18 Moreover, advanced training programmes that include weightlifting movements and plyometrics are now recommended as part of performance-enhancing and injury-reducing youth programmes.19 20 21 22 The growing popularity of youth resistance training and the complex nature of youth sport participation raise new questions and concerns about the safety of youth resistance training, the risk factors associated with resistance training-related injuries in youth and the effectiveness of preventive measures. Our purpose is to review the current epidemiology of injury related to the safety and efficacy of resistance training among youth and to provide age-appropriate training recommendations for children and adolescents.
Definitions
By definition, the term “resistance training” refers to a specialised method of physical conditioning that involves the progressive use of a wide range of resistive loads, different movement velocities and a variety of training modalities including weight machines, free weights (barbells and dumbbells), elastic bands, medicine balls and plyometrics. The term “resistance training” should be distinguished from the sports of weightlifting and powerlifting in which individuals periodically train with heavy loads and attempt to lift maximal amounts of weight in competition. Resistance training should also be distinguished from the sport of bodybuilding in which the goal is muscle size, symmetry and definition. In this review, the term “youth” refers to both children and adolescents.
Incidence and distribution of youth resistance training injuries: replacing dogma with data
Incidence of injury
Current research findings indicate a relatively low risk of injury in children and adolescents who follow age-appropriate resistance training guidelines, which include qualified supervision and instruction.4 23 24 A wide variety of resistance training programmes from single-set sessions on child-size weight machines to multi-set protocols using different types of equipment have proved to be safe and efficacious.17 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 Of note, significant gains in strength without any report of injury have been reported in prospective studies in which weightlifting movements (including modified cleans, pulls and presses) were incorporated into youth resistance training programmes.44 46 47 49 These findings are supported by others who found that the sport of weightlifting can be safe for youth provided that well-informed coaches supervise all training sessions and competitions in order carefully to prescribe the weight lifted.50 51 In the vast majority of resistance training intervention studies summarised in table 1,17 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 the injury occurrence in children and adolescents was either very low or nil and the resistance training stimulus was well tolerated by the young subjects.
Intervention studies of resistance training in youth
Three prospective research studies have reported training-related injuries in youth that required cessation from training or time away from a training session.28 35 37 Namely, anterior shoulder pain that resolved within one week of rest,28 a strain of a shoulder muscle that resulted in one missed training session35 and non-specific anterior thigh pain that resolved with 5 minutes of rest.37 A review of these findings revealed estimated injury rates of 0.176, 0.053 and 0.055 per 100 participant hours, respectively, which suggest that supervised resistance training protocols are relatively safe for youth.28 35 37 Furthermore, Rians and colleagues28 found no evidence of either musculoskeletal injury (measured by biphasic scintigraphy) or muscle necrosis (determined by creatine phosphokinase levels) in children after 14 weeks of progressive resistance training on hydraulic resistance machines.
The evaluation of maximal muscle strength has also proved to be relatively safe for children and adolescents. Faigenbaum et al52 evaluated the safety and efficacy of 1 repetition maximum (RM) testing in 96 children (6–12 years) and reported that healthy boys and girls can safely perform maximal effort strength tests on weight machines provided that appropriate testing procedures are followed. In other reports, children and adolescents safely performed 1 RM strength tests using free weights.36 37 53 54 55 These data suggest that children and adolescents can safely engage in this type of strength testing provided that appropriate loads are used, established guidelines are followed and qualified professionals are present. Although some observers are opposed to the use of 1 RM testing in children,12 it is important to realise that many of the forces that youth are exposed to in sports and recreational activities (eg, gymnastics, rugby and running) are likely to be greater both in duration and magnitude than properly performed maximal strength tests.
A summary of descriptive and observational studies that reported on the frequency or incidence of injury in youth from resistance training, weightlifting or powerlifting are presented in table 2.23 51 56 57 In one retrospective evaluation of injury rates in adolescents it was noted that resistance training and weightlifting were markedly safer than many other sports and activities.23 In that study, the overall injury rate per 100 participant hours was 0.8000 for rugby and 0.0035 and 0.0017 for resistance training and weightlifting, respectively.23 In support of these findings, Pierce and colleagues51 followed 70 competitive weightlifters (7–16 years) over a one-year period (1224 lifts were performed in competition) and reported no injuries that limited training or required medical attention.
Descriptive and observation studies on the frequency or incidence of injury in youth from resistance training, weightlifting or powerlifting
A retrospective survey of resistance training injuries in 354 adolescent American football players found 27 injuries (causing more than 7 days of missed participation), which resulted in estimated injury rates in junior high school athletes (mean age 13.3 years), high school freshman/junior varsity athletes (mean age 15.6 years) and high school varsity athletes (mean age 17.2 years) of 0.11, 0.091 and 0.51, respectively, per person-year.57 In the aforementioned study,57 only 36% of the training sessions performed by junior high school athletes were supervised by a coach. Brown and Kimball56 estimated an injury rate of 0.29/100 participant hours in adolescent powerlifters who presumably trained with heavy loads on the bench press, deadlift and back squat exercises.
Although discussions of resistance training-related injuries typically include muscle strains and lower back pain, if safety standards for youth resistance training are not followed there is the potential for a catastrophic injury. In one case report, a 9-year-old boy died at home when a barbell rolled off the bench press support and fell on his chest while he was “playing” with his older brother’s weights.58 Serious accidents have also been reported in adults who resistance train for recreation and sport.59
Location and type of injuries
The potential for soft tissue injuries from repetitive use is an important consideration related to resistance training. In a recent evaluation of “weightlifting” injuries (ie, resistance training injuries), presenting to US emergency rooms, Quatman and colleagues1 reported that the trunk was the most commonly injured body part for both men (36.9%) and women (27.4%) between the ages of 14 and 30 years. Others reported that the lower back region was the most frequent site of injury site in adolescent athletes who participated in a resistance training programme.56 57 60 In a retrospective study involving adolescent powerlifters, 50% of reported injuries were to the lower back.56 Of potential relevance, the average powerlifter in that report trained 4.1 times per week (99 minutes per training session) and a majority of the training sessions were performed without supervision from a “trained coach”.56 In contrast, Myer and colleagues24 reported that injuries to the trunk constituted only 12% of reported injuries in youth aged 8–13 years. While the potential for injury to the lower back is a concern, many modifiable and controllable factors need to be considered when evaluating these data (eg, quality of supervision and instruction, exercise technique, progression of training loads and weekly training volume).
Growth plate injuries
Another concern associated with youth resistance training is the potential for injury to the physis or growth plate in a young lifter’s body. The growth plate can be three to five times weaker than surrounding connective tissue and it may be less resistant to shear and tension forces.61 Injury to this section of bone could result in time lost from training, significant discomfort and growth disturbance.62 A summary of case reports of resistance training-related physeal injuries in youth is provided in table 3.63 64 65 66 67 68
Summary of case reports of resistance training-related physeal injury in youth
Although a few retrospective case reports noted injury to the growth cartilage in youth,63 64 65 66 67 68 most of these injuries were caused by improper lifting techniques, poorly chosen training loads or lack of qualified adult supervision. For example, in one case report a 13-year-old boy had bilateral fracture separations of the distal radial epiphyses when he lost control of a barbell as he attempted to press a 30 kg weight overhead while exercising alone in a “makeshift gymnasium” at home.66 It is unclear from this report if this adolescent received instruction on proper resistance training procedures or if he was involved in an activity that could be characterised as “horse play”.
Of note, injury to the growth cartilage has not been reported in any prospective youth resistance training study that provided professional guidance and instruction.17 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 Furthermore, there is no evidence that resistance training will negatively impact growth in height during childhood and adolescence.3 4 The risk of growth plate injury may be greater when young athletes perform jumping and landing activities during competitive sport play that induces ground reaction forces of up to five to seven times body mass.69 70
Relative safety of youth resistance training
Although youth resistance training does involve some degree of inherent risk of musculoskeletal injury, this risk does not appear to be any greater than other sports and recreational activities in which children and adolescents regularly participate.23 71 Zaricznyj and colleagues71 evaluated the incidence of sports-related injuries (based on accident reports) in school-age youth over a one-year period and found that resistance training resulted in 0.7% of 1576 injuries, whereas American football resulted in 19% of all injuries. When the data were evaluated in terms of injury to participant ratio in school team sports, American football (28%), wrestling (16%) and gymnastics (13%) were at the top of the list.71 In support of these observations, more recent data indicate that American football had the highest injury rate (4.36 injuries per 1000 athlete exposures) for nine sports studied.72
A related concern regards the performance of plyometric exercises (also called stretch-shortening cycle exercise) for children and adolescents. Although some observers suggested that a predetermined baseline level of strength (eg, 1 RM squat should be 1.5 times body weight) should be a prerequisite for lower body plyometric training,73 this contention is not supported by current research and clinical observations.19 46 74 75 76 77 Plyometric training can be a relatively safe and effective method of conditioning for children and adolescents if appropriately prescribed and sensibly progressed over time.11 19
Nonetheless, the addition of any type of resistance training to the total exercise dose of young athletes (ie, sports practice, sports competition and free play) should be carefully considered as this type of training may add to the chronic repetitive stress placed on developing musculoskeletal systems. Injury or illness can result if the intensity, volume or frequency of training exceeds the ability of the participants to perform technically sound movements or to recover from earlier training bouts. For example, a 12-year-old boy developed exertional rhabdomyolysis after he was instructed to perform excessive (>250) repetitive squat jumps in a physical education class.78
Risk factors
By addressing the risk factors associated with resistance training-related injuries it is possible to reduce the risk of injury and enhance the training experience for young athletes. Although additional research is warranted, common risk factors that have been associated with sports-related injuries in youth include: the adolescent growth spurt; age; biological maturity; body size; poor coaching; fitness and previous injury.79 Other hypothesised but untested factors include: poor conditioning; muscle imbalances; inadequate nutrition; improper equipment; hazardous playing conditions; poor exercise technique; training errors and lack of coaching education.79 80
Myer and colleagues24 recently examined data from the United States Consumer Product Safety Commission in order to evaluate resistance training-related injuries from patients presenting to US emergency rooms (fig 2). They found that as the age group increased (8–13, 14–18, 19–22 and 23–30 years) the number of accidental injuries decreased significantly for each successive age group. Of potential relevance, they noted that two-thirds of the injuries sustained by 8–13-year-old patients were to the hand and foot and were most often related to “dropping” and “pinching” in the injury descriptions (fig 3). Conversely, the number of joint sprains and muscle strains was higher in the older age groups.

Estimated number of “weightlifting” (ie, resistance training) injuries presenting in US emergency rooms between the years 2002 and 2005. Reprinted from Myer et al.24 Reproduced by permission of the National Strength and Conditioning Association, Colorado Springs, Colorado, USA.

{kind=link}
{kind=link}
{kind=link}
Percentage of injuries of the oldest and youngest age categories. Note that the small prevalence of leg injuries in the 8–13 years age categories provides invalidated results and should be interpreted with caution. Reprinted from Myer et al.24 Reproduced by permission of the National Strength and Conditioning Association, Colorado Springs, Colorado, USA.
Although supervised and age-appropriate resistance training is currently recognised by medical and fitness organisations to be a safe and effective method of exercise for children and adolescents,8 9 10 11 teachers and coaches need to be aware of proper resistance training procedures because the aggressive progression of training loads and the improper performance of free weight lifts can be injurious.56 60 A recurring theme in most youth resistance training-related injuries is the lack of qualified adult supervision and instruction. Without guidance from professionals knowledgeable in youth resistance training procedures, children and adolescents who use exercise equipment are more likely to have an injury as a result of unsafe behaviour, equipment malfunction and lack of proper supervision.24 81 82
Prevention
Resistance training to prevent other sport injuries
In addition to enhancing strength and power, regular participation in a preseason conditioning programme that includes resistance training may facilitate injury risk reduction during sports participation. Comprehensive resistance training programmes that included plyometric exercises (and instruction on jumping and landing techniques) have been found to enhance movement biomechanics, improve functional abilities and reduce the number of sport-related injuries in young athletes.83 84 85 86 Indeed, most multifaceted conditioning programmes that included progressive resistance exercise have proved to be an effective strategy for reducing sports-related injuries in adolescent athletes.83 84 85 87 88 89 90 However, one limitation of intervention trials that use multiple interventions in a trial arm is that it is difficult to characterise the contribution of each aspect of the intervention to the decrease in injury.
What is already known on this topic
There is clear evidence that resistance training can be a worthwhile and beneficial activity for children and adolescents.
A growing number of youth are participating in resistance training programmes in schools, recreation centres and sports training facilities.
Little is being done to address the risk factors associated with resistance training-related injuries in young athletes.
What this paper adds
This paper suggests that most injuries related to youth resistance training are a result of inadequate professional supervision, which underlies poor exercise techniques and inappropriate training loads.
The risk of musculoskeletal injury resulting from age-appropriate resistance training, weightlifting and plyometrics does not appear to be any greater than other sports and recreational activities in which children and adolescents regularly participate.
Comprehensive conditioning programmes designed and supervised by qualified professionals who have an understanding of youth resistance training guidelines as well as the physical and psychosocial uniqueness of children and adolescents appear to be an effective strategy for reducing sports-related injuries in young athletes.
Prevention of resistance training injuries
Research findings suggest that a majority of resistance training-related injuries in children and adolescents are the result of accidents, improper exercise technique or lack of qualified supervision.24 82 91 Attention to weight room etiquette, safe use of equipment, age-appropriate training and proper handling of heavy objects may limit the risk of accidental injuries among young lifters. Of note, qualified professionals who have an understanding of youth resistance training guidelines and who are knowledgeable of the physiological and psychosocial uniqueness of children and adolescents should provide supervision and instruction (eg, UK Strength and Conditioning Association level 1 strength and conditioning coach or National Strength and Conditioning Association certified strength and conditioning specialist). Although there have been no preventive trials that have focused specifically on measures to prevent resistance training injuries in children and adolescents, the following recommendations appear warranted for apparently healthy youth:
All youth should have the emotional maturity to accept and follow coaching instructions.
All youth should wear comfortable attire that does not restrict movement patterns and athletic footwear that provides good traction and support.
Resistance training sessions should begin with dynamic warm-up activities.
Resistance training sessions should include exercises for all of the major muscle groups including the hips, abdomen and lower back.
The focus of youth resistance training programmes should be on learning proper exercise technique and not on the amount of weight lifted.
Qualified professionals who have an understanding of youth resistance training and paediatric fitness should provide supervision and instruction.
Qualified professionals should ensure the training area is safe, adequately ventilated and free of any potential hazard.
Qualified professionals should monitor each participant’s ability to tolerate the exercise stress and should modify the training programme when appropriate.
Qualified professionals should systematically vary the training programme over time in order to minimise the risk of injury or overtraining.
Lifestyle factors that influence training adaptations such as proper nutrition, sufficient hydration and adequate sleep should be addressed in youth sport programmes.
Further research
Well-designed longitudinal epidemiological studies are needed to understand better the long-term effects of structured resistance training on youth. This research should ensure the collection of exposure data (time exposed) to support injury incidence determination and comparisons with other sports and recreational activities. Accurate recording of information such as equipment design and layout, level of supervision, training experience, quality of instruction and programme design variables (eg, exercises, sets, repetitions, load and frequency) may be helpful to the evaluation of possible injury risk factors. Studies are also needed to determine the effects of injury prevention strategies (eg, coaching education and preparatory resistance training) on acute and overuse injuries in young athletes. Although youngsters as young as 6–8 years of age play organised sports, no preventive trials have evaluated the effects of fitness conditioning (including resistance training) on sports-related injuries in children.
Epidemiological research will also help to provide descriptive information on the location and type of injuries that are most prevalent, where the injuries happened, when the injuries occurred and time loss associated with injury. Descriptive data on the resistance training protocol of young athletes may provide additional insight into possible injury mechanisms and risk factors and how programme design variables may influence the rate and severity of injury. Cumulatively, these data will aid in the development and implementation of evidence-based prevention measures in schools, fitness centres and sports training facilities that cater to children and adolescents.
REFERENCES
Footnotes
Funding GDM received funding support from the National Institutes of Health grants R01-AR049735 and R01-AR055563.
Competing interests None.
Provenance and Peer review Commissioned; externally peer reviewed.