Article Text

Abstract
Objective: To examine the prevalence of dieting, reasons for dieting and prevalence of disordered eating among adolescent elite athletes and age-matched controls, and to examine the differences between athletes competing in leanness and non-leanness sports.
Methods: First-year students of 16 different Norwegian Elite Sport High Schools (athlete group, n = 682) and two randomly selected ordinary high schools from a county representative of the general Norwegian population (control group, n = 423) were invited to participate in this cross-sectional study. A total of 606 athletes and 355 controls completed the questionnaire, giving a response rate of 89% and 84%, respectively. The questionnaire contained questions regarding training patterns, menstrual status and history, dieting, use of pathogenic weight control methods and the drive for thinness (DT) and body dissatisfaction (BD) subscales from the Eating Disorders Inventory.
Main outcome measure: Disordered eating, defined as meeting one or more of the following criteria: DT score ⩾15 (girls) and ⩾10 (boys), BD score ⩾14 (girls) and ⩾10 (boys), body mass index <17.9 kg/m2 (girls) and <17.5 kg/m2 (boys), current and/or ⩾3 previous efforts to lose weight, use of pathogenic weight control methods and self-reported menstrual dysfunction.
Results: A higher prevalence of control subjects were dieting and classified with disordered eating compared with the athletes. An improvement of appearance was a more common reason for dieting among controls compared with athletes. No differences in dieting or disordered eating were found between leanness and non-leanness sports athletes.
Conclusions: Self-reported disordered eating is more prevalent among controls than adolescent elite athletes, and losing weight to enhance performance is an important reason for dieting among adolescent elite athletes.
Statistics from Altmetric.com
Adolescent athletes represent a group that most closely embodies an “ideal” of physical perfection. However, study findings1 2 as well as practical experience indicate that some highly trained elite athletes diet and are dissatisfied with their bodies. Not all athletes have a body that fits, or have a subjective feeling that their body fits, into the sport specific “ideal”—and those athletes often experience pressure to achieve this “idealistic” body type.3 4 This is especially at issue for pubertal female athletes who may gain a significant amount of fat.2 5 The prevalence of dieting is 15% and 33% among adolescent boy and girl high school athletes respectively, and 17% and 44% among non-athlete boys and girls.6 Prevalence rates of disordered eating are around 16% and 26% in athletes and controls, respectively.6 The prevalence of disordered eating is likely higher among elite athletes competing in sports emphasising a thin body size or shape and in sports that utilise weight categories.7
In general, studies indicate a higher frequency of disordered eating and or eating disorder in adult elite athletes than controls, particularly in athletes competing in sports that emphasise leanness or low body weight.1 7 8 9 10 In contrast, some studies on high school athletes report no greater risk for the development of an eating disorder than controls.6 9 11
Moreover, some studies suggest a similar or lower risk of eating disorders compared with controls for female athletes in aesthetic sports and running, and female athletes representing lower competitive levels.12 13 14 15 Of the few studies that include male athletes, some indicate an increased risk of disordered eating in athletes competing in weight class sports such as wrestling and rowing,1 16 17 18 although others indicate a lower risk for EDs in male figure skaters and swimmers.19 20 A recent study on high school athletes attending Elite Sports Schools reported that boy athletes in leanness sports had a twofold higher frequency of disordered eating compared with boys in non-leanness sports (risk ratio = 2.11, 95% CI 1.11 to 4.04).6 Although leanness sports (ie, sports where weight is perceived as important for performance) are considered as risk sports for disordered eating, our practical experience is that adolescent elite athletes seeking treatment for eating disorders represent a wide range of leanness and non-leanness sports. There is also an alarmingly high number of adolescents in general who suffer from eating disorders.21 22 However, studies focusing on disordered eating among representative samples of adolescent elite athletes and age-matched representative controls are lacking. Most of the published studies on athletes have focused on female athletes only, have small samples, include only one or a few sports, fail to consistently describe competitive level, employ different tests or do not include a control group.9 23 Thus, there is a need for a study which includes a representative population of young elite athletes representing a wide range of sports and in which all athletes are exposed to the same instruments or questionnaires.
Pressure from coaches to lose weight, frequent weight cycling, early start of sport-specific training, overtraining, injury and irresponsible coaching behaviour may be risk factors for the development of disordered eating.3 In addition, dissatisfaction with body shape or weight and dieting are well-known risk factors for disordered eating.24 25 It is therefore important to examine reasons for dieting among adolescent elite athletes to enable us to develop preventive strategies. The development of eating disorders often begins in adolescence, when changes in body shape affect personal appearance6 One of our previous studies reported that most adult athletes who met the criteria for eating disorder started dieting and developing an eating disorder during puberty or adolescence.3
Based on the considerations presented above and the scarcity of scientific research related to disordered eating behaviour among adolescent elite athletes, we assessed disordered eating among adolescent elite athletes and age-matched controls. Our research questions were:
1. Is disordered eating more common among adolescent elite athletes compared with controls?
2. Are there any differences in reported reasons for dieting among adolescent elite athletes compared with controls?
3. What are the variables/predictors associated with disordered eating among adolescent elite athletes and the controls?
Methods
Participants
This study consisted of a group of adolescent elite athletes and age-matched control subjects. Inclusion criteria for athletes and controls included enrolment as a first-year student at one of all the Norwegian Elite Sport Schools (athletes) or at one of two randomly selected high schools in Buskerud county in Norway (controls) and a birth date in 1992 (ie, age of 15 or 16 at the time of data collection). An exclusion criterion was lack of permission from parents to participate. Following initial screening, 682 athletes and 423 controls who attended the first year of the selected high schools during the autumn of 2008 were invited to participate.
The athletes represented 50 different sports. For parts of the analysis, the sports were classified into leanness and non-leanness sports (table 1). Leanness sports were defined as sports in which leanness and/or low weight were considered important, and non-leanness sports were defined as sports where these factors are considered less important.26 Four athletes competed in both leanness and non-leanness sports, and these athletes were classified as athletes in leanness sports for the analysis. The study was approved by the Regional Committee for Medical and Health Science Research Ethics in Southern Norway, and by the Norwegian Social Science Data Services. The respondents gave written consent to participate.
Classification of the 50 different sports into leanness/non-leanness sports
Assessment procedures
Questionnaire
A questionnaire including a battery of assessment questions regarding training history, physical activity and nutritional patterns, menstrual history, oral contraceptive use, dieting and weight regulation history, use of pathogenic weight-control methods, injuries, self report of previous and/or current eating disorders and the standardised questionnaire Eating Disorders Inventory –2 (EDI-2) was administered to the respondents. The EDI-2 is a validated and commonly used self report to assess eating disorders, and it consists of 11 subscales.27 In this study, only the drive for thinness (DT, α = 0.86 for girl athletes and controls, 0.83 for athlete boys and 0.71 for control boys) and the body dissatisfaction (BD, α = 0.91 for athlete and control girls, 0.63 for athlete boys and 0.75 for control boys) scales were used in the analysis. The BD assesses dissatisfaction with body areas—hips, buttocks, thighs and stomach. These areas have previously been shown to be more important in females than in males,28 so two of the BD questions were changed for the male participants in this study. The phrase “I like the shape of my buttocks” was changed to “I like the shape of my upper body,” and “I think that my buttocks are too large” was changed to “I think that my torso is too small.” Classification of underweight through body mass index (BMI, kg/m2) was age-adjusted using the values suggested by Cole et al.29 Therefore, females with BMI <17.9 and males with BMI <17.5 were defined as underweight (box 1). Consent to collect data was obtained from the head of each school. The athletes and the controls completed the questionnaire in the presence of one of the research group members.
Box 1. Criteria for being classified with symptoms of disordered eating
Drive for Thinness score⩾15 girls and ⩾10 boys
Body Dissatisfaction score⩾14 girls and ⩾10 boys
Body mass index <17.9 kg/m2 girls and <17.5 kg/m2 boys
Trying to lose weight now
Tried to lose weight before ⩾3 times
Pathogenic weight control methods: use of diet pills, laxatives, diuretics or vomiting to reduce weight
Self-reported menstrual dysfunction; primary amenorrhea or secondary amenorrhea
Defining symptoms of disordered eating
To be classified with symptoms of disordered eating, one or more of the criteria listed in box 1 are required. These criteria were chosen based on previous studies of elite athletes1 7 and based on the DSM-IV diagnostic criteria for eating disorders.30 The criteria were also based on the assumption that disordered eating occur on a continuum of severity.31 Therefore, we considered it important to examine symptoms of disordered eating, including body dissatisfaction, drive for thinness, underweight, dieting and use of pathogenic weight-control methods, menstrual dysfunction and not only a clinical conception of eating disorders. Pathogenic weight control methods were defined as destructive and unhealthy techniques used to influence body weight, such as purging, use of laxatives, diuretics or dieting pills.
Statistical analyses
The statistical analyses were carried out using SPSS version 15.0 (SPSS, Chicago). Results are expressed as the mean value (SD) for continuous data and absolute numbers (N) and percentage (%) for categorical data. The independent sample t test was used to evaluate mean differences and χ2 tests examined categorical frequencies. When the expected counts were less than five, the Fisher exact test was used. A binary logistic regression analysis was carried out for predicting the likelihood between symptoms of disordered eating as the dependent variable and gender, BMI and sports group (leanness/non-leanness) for athletes. For controls, the variable physical active (yes/no) was used instead of sports group. Odds ratios are given with 95% CIs. The significance level was set to 0.05.
Results
A total of 29 athletes and 77 controls were excluded from the study (exclusion due to age: n = 24 athletes and 58 controls, not informant consent: n = 5 athletes and 19 controls). Of the 682 athletes and 423 controls eligible for the study, 66 athletes and 66 controls elected not to participate, and 10 athletes and two controls did not complete the questionnaire satisfactorily. A total of 606 athletes and 355 controls completed the study, giving a response rate of 89% for the athletes and 84% for the controls.
Subjects’ characteristics
All athletes and controls were 15–16 years old by the data collection time. A higher number of controls compared with athletes were defined as overweight according to BMI criteria (table 2). A total of 21.8% of the athletes had competed at an international level. Eighty-two per cent of the controls reported that they were physically active or participated in organised sports. No differences in frequency were observed between overweight athletes competing in leanness sports (7%) and non-leanness sports (12%) or between underweight leanness (4%) and non-leanness athletes (1%) according to the BMI classifications.
Anthropometric data presented for athletes and controls
Dieting
A higher percentage of controls than athletes reported dieting (p<0.001) and use of pathogenic weight-control methods (p = 0.017) (table 3). The most frequent reason for dieting among girl and boy controls and girl athletes was to improve appearance, whereas boy athletes most often reported enhanced performance as a reason for dieting (table 4). One-third of the athlete boys and 13% of the athlete girls were dieting as directed by their coach or teacher, and this was higher than among boy and girl controls respectively. A higher frequency of overweight athletes (30%) and controls (51%) reported dieting behaviour compared with normal weight and underweight athletes (p<0.001) and controls (p<0.001).
Prevalence of disordered eating and the different symptoms among athletes and controls
Reported reasons for dieting among athletes (ATH) and controls (CON) that diet now and/or have dieted before ⩾3 times.
A similar frequency of athletes representing leanness sports (13% dieting and 6% use of pathogenic weight control methods) and non-leanness sports (11% dieting and 5% use of pathogenic weight control methods) reported dieting and use of pathogenic weight control methods.
Symptoms of disordered eating
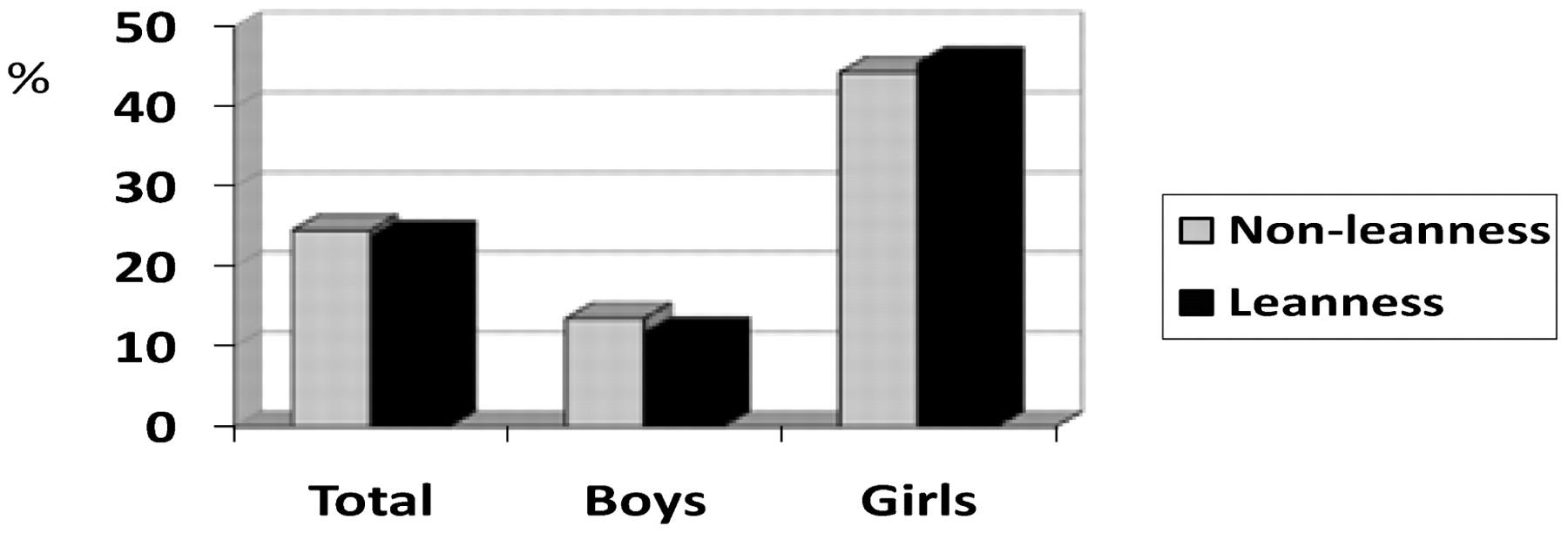
When comparing athletes in leanness sports (n = 159) with those competing in non-leanness sports (n = 447), a higher prevalence of disordered eating was only found among girls compared with boys in the same sports groups (p<0.001) (fig 1).
{kind=link}
Prevalence of symptoms of disordered eating among athletes competing in leanness versus non-leanness sports.
In a logistic regression analysis, gender and BMI proved to be significant predictors of symptoms of eating disorders among both athletes (p<0.001 and p = 0.012) and controls (p<0.001 and p<0.001) (table 5).
Logistic regression analysis with disordered eating as the dependent variable in athletes and controls
Discussion
The main findings of this study were the higher prevalence of symptoms of disordered eating among controls compared with athletes and the lack of difference in prevalence among athletes competing in leanness sports versus those competing in non-leanness sports.
Prevalence of disordered eating among athletes and controls
We found a lower frequency of disordered eating behaviour in Norwegian adolescent elite athletes than that of age-matched regular high school students. Thus, these findings add support to previous, less well-controlled studies9 11 which indicate that self-reported disordered eating is less of a problem among adolescent athletes than it is in the community at large.
Fulkerson et al11 suggested that athletes’ positive outlook of life and high self-efficacy may serve as protective factors for disordered eating. Other reasons that might explain athletes’ lower prevalence of disordered eating could be the fact that these athletes are all highly trained, a lower percentage than controls have high BMI values, and a lower percentage are dissatisfied with their bodies. In general, athletes have a higher self esteem than non-athletes.33 34 Also, the lack of difference in frequency of disordered eating symptoms observed between leanness and non-leanness athletes supports the suggestion that being an athlete lowers the risk of disordered eating in adolescent elite athletes’ eating.
The study by Rosendahl et al6 on high school athletes reported no difference in prevalence of disordered eating between athletes and controls. In contrast to our finding, they reported a higher prevalence of disordered eating in athletes competing in leanness sports compared with athletes whose sports did not require leanness.6 In a previous published two-part study (which also included a clinical evaluation of athletes with symptoms of disordered eating) we found that the elite athletes under-reported disordered eating symptoms; when compared with controls, a higher number of elite male and female athletes met the criteria for eating disorders (DSM-IV).7 35 Whether the adolescent athletes participating in the present study are under-reporting remains to be answered in the clinical part of this study.
Our finding that a high frequency (11%) of these well-trained adolescent athletes are dieting, and even using extreme weight-loss methods such as diuretics, vomiting and laxatives is alarming. This behaviour has health consequences, likely impairs performance and could result in positive doping tests. The high prevalence of disordered eating reported could be due to the increased awareness of low percentage of body fat as a performance variable,36 lack of educated coaches37 38 and reported experiences of being told by coaches to reduce weight.39 The athletes look at the “ideal” sport-specific body that usually is an adult athlete’s body. This is especially at issue for pubertal female athletes who may gain a significant amount of fat, which is not considered appropriate in all sports. We have reported previously that some female athletes try to delay puberty to enhance performance.40
Reasons for dieting in athletes and controls
As expected, both athletes and controls reported dieting to improve appearance. Dieting is considered normal among adolescents.41 However, losing weight to enhance performance is one of the most important reasons for dieting among athletes. Because these young athletes are perfectionists and extremely performance-oriented, they could be at increased risk for development of an eating disorder.42 Also, the reported reasons that could be related to coaches and parent pressure are an important finding and should have implications for preventive work. The higher prevalence of boy athletes compared with girl athletes who reported dieting due to the fact that coaches had told them was an unexpected finding. This has been reported as a problem among female coaches previously.3 Since the focus in the literature has been on coaching pressure towards female athletes and weight reduction, it was an important finding that this is also true among adolescent elite boy athletes
Variables associated with disordered eating among adolescent athletes and controls
Gender, BMI and sports group (leanness/non-leanness) were the independent variables tested for association with disordered eating among athletes. Instead of sports group, the variable physically active (yes/no) were used for controls. The only variables that were associated with symptoms of disordered eating were gender and BMI. As expected, the highest odds ratios (OR) were between disordered eating and gender (table 5). The prevalence of disordered eating was five times higher for girl athletes (OR = 5.310, 95% CI 3.491 to 8.078) and almost eight times higher for girl controls compared with boys (OR = 7.595, 95% CI 4.538 to 12.713).The finding that there was no association between symptoms of disordered eating and athletes competing in leanness sports, non-leanness sports, physically active controls or non-physically active controls was surprising. It could be that dieting, especially among athletes, is more related to weight-related causal attributions or perceived weight-related coach pressure.2 Also, one could speculate that the higher prevalence of disordered eating and clinical eating disorders in older elite athletes in leanness sports7 could be due to a longer period than these young athletes of exposure to sport-specific requirements such as a specific weight class and/or extreme leanness. A controlled longitudinal study is required to answer this question confidently.
Study limitations
Our use of a wide range of criteria may have led to a higher number of false positives; on the other hand, more strict criteria may result in too many false negatives.7 In our opinion, this is less advisable than too many false-positive subjects considering the serious health consequences of eating disorders. The onset of eating disorders often occurs during adolescence, so it is particularly important to minimise false negatives, and early detection is important for treatment efficacy. The use of BMI for classifying overweight in athletes has limitations, since the influence of large muscle mass on the BMI in athletes might misclassify individuals as overweight and obese.43 Finally, a clinical evaluation of athletes classified with disordered eating and athletes who did not report disordered eating is needed to examine the prevalence of true eating disorders.
Conclusions and further research
We found a higher prevalence of self-reported eating disorders among non-athletes compared with adolescent elite athletes. Due to the high response rate and the large number of sports included, these data are generalizable to other elite adolescent athletes. The fact that some young athletes are inducing vomiting and using diuretics and diet pills should be taken seriously. The experienced pressure from coach or teacher to reduce weight is higher among athletes than controls, and a significant number of boy athletes reported that their coach had told them to lose weight compared with girl athletes. Thus, there is ample evidence that continuous preventive work among both the youngest athletes and controls is needed.
Finally, disordered eating symptoms have been under-reported among adult elite athletes previously, so it is possible that the prevalence of disordered eating is underestimated in this study.
There is a need for controlled longitudinal studies on boy and girl athletes from a much earlier age than 15. Thereby, possible risk and trigger factors for disordered eating can be explored, and then controlled intervention studies aiming to prevent the development of disordered eating in athletes could be administered. Furthermore, identifying disordered eating among athletes should include athletes who are in a negative energy balance, or engage in unhealthy weight control practices that have clinical significance and that can severely compromise health and performance. Thus, there is a need for sport-specific instruments designed for athletes in different kind of sports and competition levels. Previous research on risk models in female elite athletes has shown that variables predicting clinical EDs are different for leanness sports athletes compared with non-leanness sports athletes and controls.7 Therefore, there is a need for further development and validation of screening instruments designed for athletic populations.
What is currently known about this topic
In adult elite athletes, the prevalence of disordered eating and clinical eating disorders is higher in elite athletes competing in leanness sports as compared with those competing in (i) non-leanness sports and (ii) controls.
What this study adds
The prevalence of self-reported symptoms of disordered eating was higher among controls than in adolescent elite boy and girl athletes.
There was no difference in disordered eating problems among athletes competing in leanness sports and those competing in non-leanness sports.
A significant number of young elite boy athletes were told coaches that they should reduce weight.
Acknowledgments
We wish to thank all the subjects and their coaches for full cooperation and support during this study. In addition, we are grateful to J Roosevelt Boettiger’s comments on the manuscript. The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the Eastern Norway Regional Health Authority, Norsk Tipping AS and the Norwegian Olympic Committee & Confederation of Sport. This project has been established through a grant from Olympiatoppen.
REFERENCES
Footnotes
Competing interests None.
Provenance and Peer review Commissioned; externally peer reviewed.
Ethics approval Ethics approval was provided by the Regional Committee for Medical and Health Science Research Ethics in Southern Norway, and by the Norwegian Social Science Data Services.
Patient consent Obtained.