Article Text

Abstract
Background Rhinitis, either allergic or non-allergic, is frequent in athletes, particularly in swimmers. In this latter case, exposure to chlorine in swimming pools seems to play a relevant role, since it can exacerbate a pre-existing allergic rhinitis (AR) or produce a non-specific irritation. The aim of this study was to detail the clinical and cytological characteristics of rhinitis in swimmers, and to assess the possible role of chlorine-induced symptoms.
Methods Elite swimmers with rhinitis symptoms underwent a complete diagnostic work-up, including allergy testing, nasal cytology and anterior rhinomanometry. Those evaluations were repeated after 1 month of use of a nasal clip during swimming. A matched group of asymptomatic swimmers was also studied. A total of 74 swimmers (54 symptomatic and 20 controls), with an age range of 9–21 years, were studied. In the control group, only mild and non-specific findings were observed, and only two had a positive skin test.
Results In the symptomatic group, 24 (44%) had AR, and 19 (35%) had a predominant neutrophilic inflammation. The use of a nose clip reduced cellular infiltration and nasal resistances only in the subjects with neutrophilic rhinitis, whereas a clinical improvement was seen also in AR.
Conclusion A neutrophilic rhinitis occurs in a large proportion of swimmers. This seems to be irritative in its nature and can be prevented by avoiding the direct contact with chlorinated water.
Statistics from Altmetric.com
Introduction
Rhinitis, clinically characterised by itching, sneezing, rhinorrhoea and obstruction, is frequent in athletes, especially in swimmers.1 In particular, the prevalence of allergic rhinitis (AR) was reported to range from 16.8% to 56%.2,–,4 The high prevalence underlines the importance of a detailed diagnosis which, in turn, allows one to identify the most appropriate strategy of management. As far as swimmers are concerned,5 it has been postulated that contact with chlorine or hypochlorite dispersed in the water of swimming pools is responsible for stimulation of the nasal mucosa. This can either exacerbate an underlying allergic inflammation or evoke per se the symptoms by an irritative mechanism.6 7
Nasal cytology is easy to perform and provides relevant information about the predominant cellular infiltration. In addition, the type of inflammation can provide suggestions about the mechanism(s) involved. On this basis, several forms of rhinitis can be identified, including the non-allergic rhinitis with eosinophilia (NARES), the non-allergic rhinitis with eosinophils and mast cells (NARESMA) and the neutrophilic rhinitis (NR).8 9
To better elucidate the relationships, if any, among symptoms, atopy, exposure to chlorinated water and nasal inflammation, we studied a group of athletes practising competitive swimming, and a control group of symptom-free swimmers. Clinical and functional evaluations, as well as nasal cytology, were carried out. In the group of symptomatic athletes, the assessments were repeated after they had used a nasal clip for 1 month during the sport activity.
Methods
Subjects and clinical evaluation
Adult, adolescent and preadolescent subjects, who had been practising competitive swimming since at least 2 years, and training three to five times per week, were studied. They had to have symptoms of rhinitis (ie, rhinorrheoa, itching, sneezing and obstruction) clearly related to the sport activity. In this regard, symptoms had to appear within 1 h after swimming, and to persist for at least 12 h.
A detailed medical history was collected and integrated by a slightly modified version of the European Community Respiratory Health Survey questionnaire. The following question was asked: ‘Do you experience symptoms rhinitis after or during swimming?’ All subjects underwent a clinical evaluation, with a special attention paid to the respiratory apparatus. Nasal symptoms were classified according to the AR and its impact on asthma recommendations.10 The severity of rhinitis was self-defined by subjects (‘How troublesome was your rhinitis in the last week?’) on a 10 cm visual analogue scale, from 0 (not at all) to 10 (very much). The presence of asthma was also assessed. If asthma symptoms were reported, pulmonary function tests with reversibility test or methacholine challenge were performed. Twenty totally symptom-free athletes, matched for sex and age, served as a control group.
The study group was re-evaluated after the use of a nose clip for 30 days. This device closes the nostrils, thus avoiding contact between the chlorinated water and the nasal mucosa. All subjects or their parents signed an informed consent, and the study was approved by the inner Ethical Committee of the Medical School of the University of Bari.
ENT evaluation
All participants underwent a detailed ENT assessment, including nasal endoscopy and anterior rhinomanometry. Nasal endoscopy was performed under local anaesthesia using a flexible endoscope (ENT-2000; Vision-Sciences, Natick, Massachusetts). Active anterior rhinomanometry was carried out with an ATMOS computerised Rhinomanometer 300 (ATMOS, Lenzkirch, Germany). Measurements were expressed in Pa/ml/s, the pressure being expressed in Pascals and the flow in ml/s. The flow pressure was set at 150 Pa according to current recommendations.11 The normal value is <0.50 Pa/ml/s per nostril and <0.25 Pa/ml/s for the total nasal resistance.
Nasal cytology
Nasal smears were obtained from the middle portion of the inferior turbinate, using a Rhino-Probe device. The samples were fixed by air drying and staining with May–Grünwald–Giemsa (Carlo Erba, Milan, Italy), then examined under a light microscope (Nikon E600; Nikon, Milan, Italy). Cell count was performed on 10 fields, at 1000× magnification under immersion. The samples were examined blindly by two different investigators.
In the normal smear, only epithelial cells and rare neutrophils are seen. According to the cell predominance, we identified (1) an eosinophilic form (nasal eosinophils >20% of total cells), (2) a mast cell form (nasal mast cells >10%), (3) a neutrophilic form (nasal neutrophils >50% of the total cells) and (4) a mixed eosinophilic–mast cell form if eosinophils were >20% and mast cells >10% of the total cells.8 12
Skin-prick tests
Skin-prick tests were carried out on the forearm, using a panel of commercial extracts (Merck SpA, Milan, Italy) that included Parietaria, Olive, Compositae, grass, cypress, birch, house dust mite, Alternaria, Aspergillus, dog and cat dander. These allergens are most frequently responsible for respiratory allergy in our region. A negative (diluent) and positive (histamine 1 mg%) control were also applied. A weal reaction (mean of the major diameter and its orthogonal) larger than 3 mm was considered positive.
Statistical analysis
Data were described as mean and SD. A χ2 test was used to compare the baseline demographic characteristics, except for nasal resistance, which was analysed by a t test. The Mann–Whitney U test was used for before versus after comparisons of cells and nasal resistance. A p value<0.05 was considered statistically significant.
Results
Seventy-four athletes, 41 male, aged between 9 and 21 years, with a mean age of 14 years, were studied. They stayed in the swimming pool for a median time of 180 min (range 90–240) each time, at least three times a week. Among them, 54 subjects (study group) reported rhinitis or asthma symptoms clearly related to their sport activity. Apart from those symptoms, all the subjects were in good health and had passed the medical exams for competitive activity. The general characteristics of the symptomatic and healthy controls are reported in table 1.
Characteristics of the symptomatic and healthy subjects
In the control group, seven subjects had a mild septal deviation and two a mild turbinate hypertrophy. Two subjects had one positive skin test (one olive and one mite). The nasal cytology was normal in 13 subjects (65%), and six (30%) had increased neutrophils, although their count was significantly lower than in symptomatic subjects (104±27 vs 462±98, p=0.01). The subject with a skin-prick test positivity to mite had only a mild cellular infiltration, suggesting a minimal persistent inflammation. The mean nasal resistance in the control group was 0.94±0.3 Pa/ml/s.
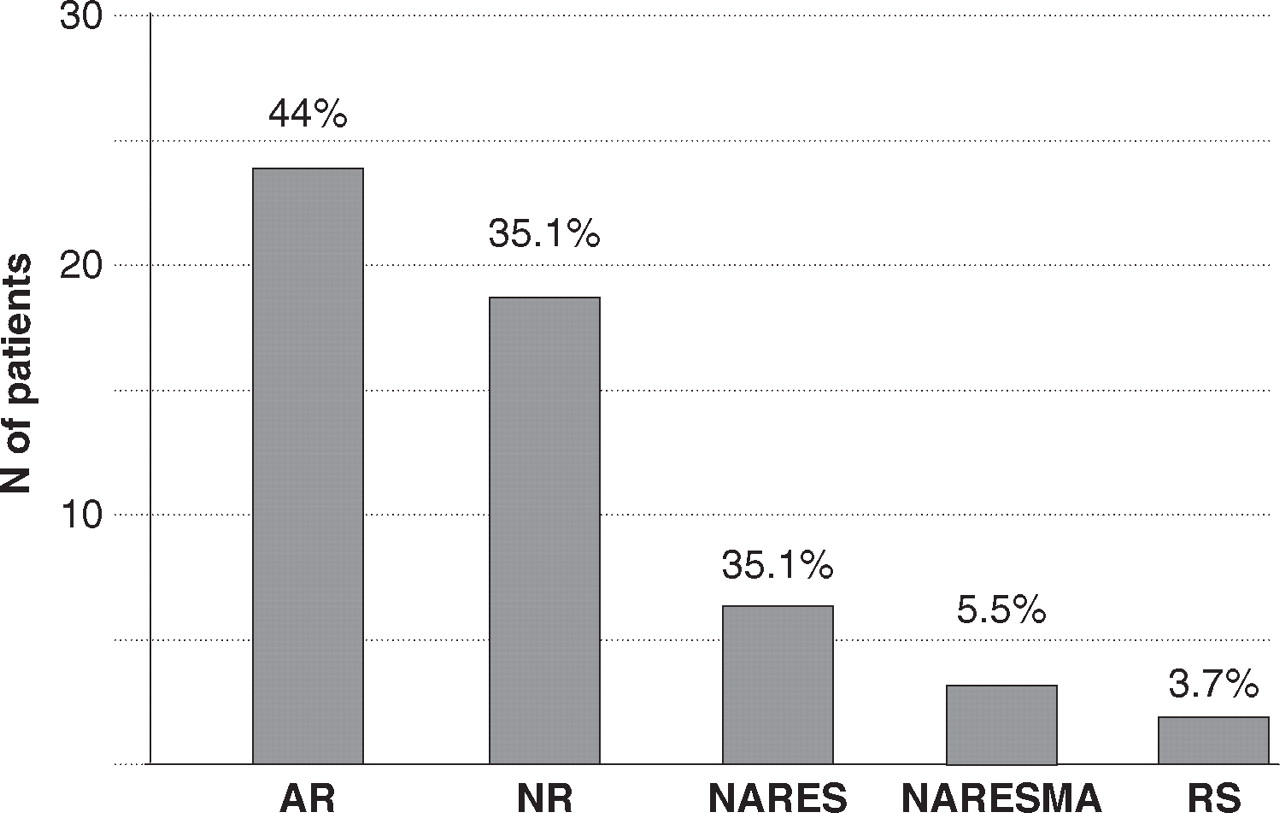
In the study group, nasal obstruction was the most frequently reported symptom (74%), followed by rhinorrhoea (61.1%) and nasal burning (57.4%). Sneezing and nasal itching were present in 38.8% and 37%, respectively. Eight (15 %) swimmers reported asthma symptoms. The presence of asthma was subsequently confirmed by pulmonary function tests and methacholine challenge. The disease was intermittent and treated with short-acting bronchodilators on demand only. In 26/54 (48%) athletes, a severe turbinate hypertrophy with serous or catarrhal exudates was seen at nasal endoscopy. In two subjects (3.7%), the presence of mucopurulent exudation from the middle meatus suggested the diagnosis of rhinosinusitis, subsequently confirmed by CT. Twenty-four of 54 subjects (44.4%) had positive skin tests to one or more allergens and displayed the typical eosinophilic inflammation. Thus, they were classified as having AR. Of the 30 athletes with a negative skin-prick test, 19 (63%) had a neutrophilic rhinitis, six had an eosinophilic form (NARES), three had a mixed eosinophil-mast cell infiltration (NARESMA), and two, as mentioned above, had rhinosinusitis (figure 1). No infectious agent was found in the nasal smears of the 19 subjects with neutrophilic rhinitis. The mean nasal resistance in this group was 3.3±0.6 Pa/ml/s, significantly different from the control group.

Diagnosis of rhinitis in the 54 symptomatic subjects according to clinical and cytological results. AR, allergic rhinitis; NARES, non-allergic rhinitis with eosinophilia; NARESMA, non-allergic rhinitis with eosinophils and mast cells; NR, neutrophilic rhinitis; RS, rhinosinusitis.
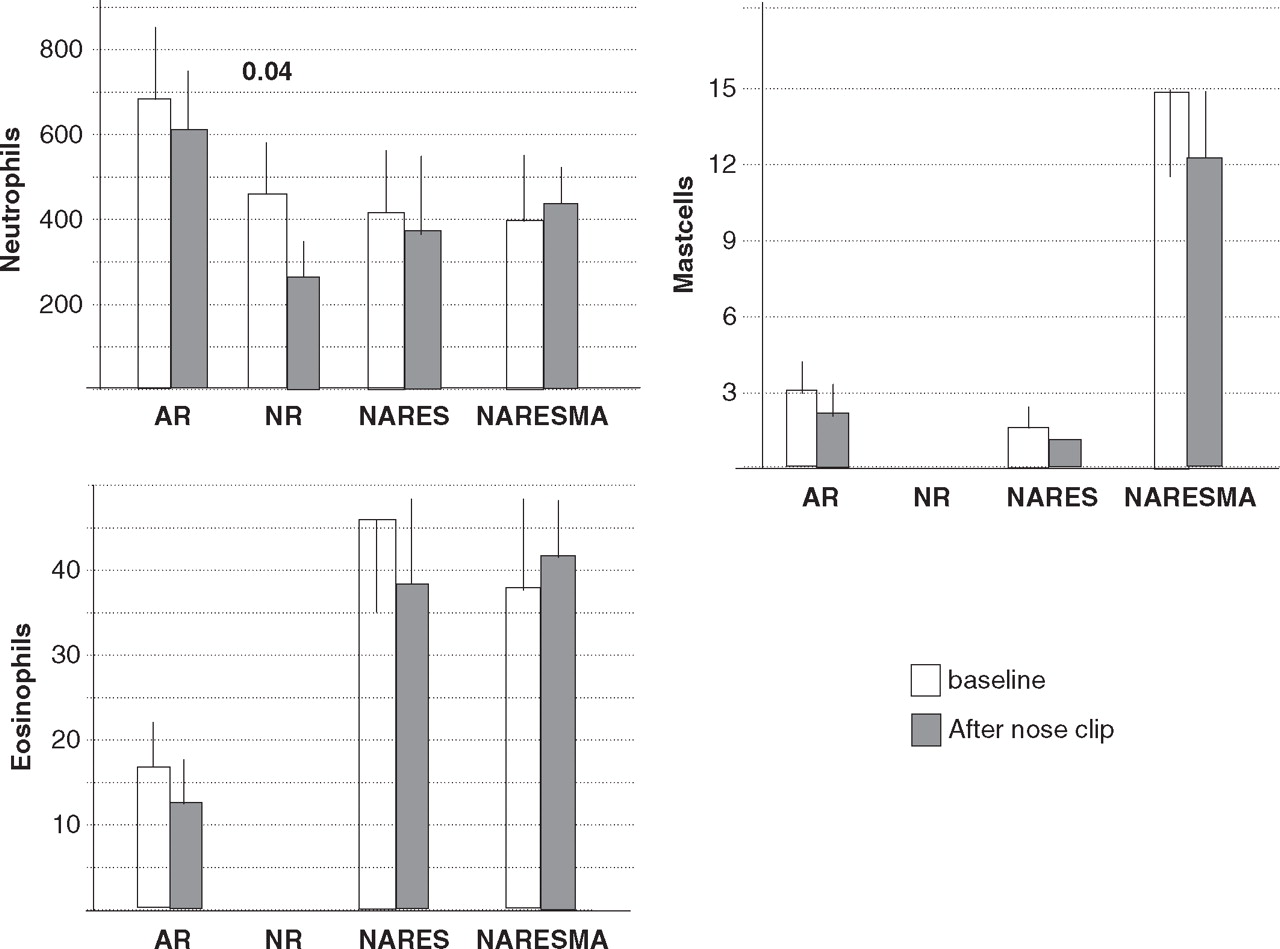
After 1 month of use of the nose clip, a significant reduction in the cellular infiltration was seen only in the subjects with neutrophilic rhinitis (figure 2). Similarly, a reduction in the nasal resistance was overall seen in all cases, but the significance was reached only in subjects with neutrophilic rhinitis (figure 3). A significant symptomatic improved was observed in all groups, but in patients with NARESMA. The improvement in symptoms was greater in subjects with NR, where the symptoms disappeared almost completely (figure 4).

Nasal cytology (total count per 10 fields) in the 54 symptomatic swimmers according to the type of disease, before and after using the nose clip. Left lower panel: eosinophils; left upper panel: neutrophils; right panel: mast cells. Significant differences are shown above the bars. AR, allergic rhinitis; NARES, non-allergic rhinitis with eosinophilia; NARESMA, non-allergic rhinitis with eosinophils and mast cells; NR, neutrophilic rhinitis.

Nasal resistance (Pa/ml/s) in the 54 symptomatic swimmers according to the type of disease before and after using the nose clip. AR, allergic rhinitis; NARES, non-allergic rhinitis with eosinophilia; NARESMA, non-allergic rhinitis with eosinophils and mast cells; NR, neutrophilic rhinitis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
VAS scores in the 54 symptomatic swimmers according to the type of disease before and after using the nose clip. AR, allergic rhinitis; NARES, non-allergic rhinitis with eosinophilia; NARESMA, non-allergic rhinitis with eosinophils and mast cells; NR, neutrophilic rhinitis; VAS, visual-analog scale.
Discussion
Various hypotheses on the pathogenesis of rhinitis in swimmers have been proposed, although a clear explanation has not yet been achieved.6 13 14 One of the most reasonable hypotheses is that chlorine, which is constantly present in swimming pools as an antimicrobial agent, produces an irritation of the nasal mucosa and can either reveal a latent nasal hyper-reactivity or directly provoke irritating symptoms. For this reason, we examined a group of competitive swimmers, training and competing in swimming pools, who suffered from nasal symptoms after their sport activity. Clinical data, nasal cytology and nasal resistance were recorded, and the effect of the use of a nose clip during the pool activity was also assessed. The first notable result was the high prevalence of allergy within the athletes, in agreement with previous reports.1,–,3 In fact, 35% of the whole population (healthy plus symptomatic) and 44% of the symptomatic swimmers had positive skin tests. Another important aspect was the high prevalence of neutrophilic rhinitis, found in about 35% of the symptomatic subjects. Other forms of rhinitis as NARES and NARESMA accounted for a minority of the cases. Finally, in subjects with rhinitis, there was a high prevalence of concomitant asthma (15%), and this is in agreement with the data described in large epidemiological studies.15 16
In competitive swimmers, several factors, including the temperature and pH of the water, or hyperventilation, may affect the nasal physiology,17 18 but the presence of chlorine is probably the most relevant one. The irritant effect of chlorine accounts, in fact, for the neutrophilic inflammation. In patients with AR or NARES, the neutrophilic infiltration is superimposed to the already present inflammation. The ‘irritative’ hypothesis is indirectly confirmed by the fact that the use of a nose clip is able to significantly reduce the nasal resistance and the neutrophilic component of inflammation only in the pure NR. On the other hand, the nose clip resulted in a symptomatic improvement not only in NR but also in AR and NARES. This can be attributed to the elimination of the irritative component of rhinitis. Of note, also, 30% of the asymptomatic swimmers had a neutrophilic infiltration but at a lower degree than symptomatic subjects.
Conclusion
In summary, these data confirm that in competitive swimmers, the prevalence of rhinitis is high, and neutrophilic inflammation, likely due to chlorine, occurs frequently. These aspects are of crucial importance and suggest the opportunity to avoid high concentrations of chlorine in swimming pools.19 Nasal cytology allows easy identification of neutrophilic inflammatory rhinitis.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was provided by the inner Ethical Committee of the Medical School of the University of Bari.
-
Provenance and peer review Not commissioned; externally peer reviewed.