Article Text

Abstract
Background In competitive alpine skiing, there is a controversy regarding the sex-related risk of injury.
Objective To compare the risk of injury in female versus male World Cup (WC) alpine skiers.
Methods Injuries were recorded through the International Ski Federation Injury Surveillance System for six consecutive winter seasons (2006–2012), based on retrospective interviews with athletes from 10 teams at the end of each season. All acute training and competition injuries which required medical attention were recorded. Race exposure was calculated based on the exact number of runs started in the WC for each of the interviewed athletes each season.
Results Men had a higher overall rate of injury (relative risk (RR) 1.24, 95% CI 1.05 to 1.47), as well as a higher rate of time-loss injury (RR 1.23, 95% CI 1.03 to 1.48) than women in training and competitions, expressed as injuries/100 athletes/season. These sex differences were even more pronounced during WC races (RR 1.58, 95% CI 1.22 to 2.04 and RR 1.72, 95% CI 1.29 to 2.31, for overall and time-loss injuries, respectively). There was no sex difference in the risk of knee/anterior cruciate ligament (ACL) injuries.
Conclusions No previous studies from competitive skiing have reported a significantly higher risk of injuries in men than women. In contrast to recreational skiing and team sports, there was no sex difference in the risk of knee/ACL injuries and prevention efforts should be directed as much towards male as female competitive skiers.
- Ski injuries
- Injury Prevention
- Knee ACL
- Gender issues
- Elite performance
Statistics from Altmetric.com
Introduction
In team sports, it is well documented that women have threefold to sixfold higher risk of anterior cruciate ligament (ACL) injury than men.1–3 The exact reasons for this are unknown, but may be related to differences in lower extremity alignment, notch dimension, ligament size, ligament laxity, level of skill, muscle strength and coordination.4–7
In recreational skiing, several studies have reported that female skiers have twice the risk of serious knee injuries compared with male skiers,8–13 while men have a significantly higher risk of injuries to the shoulder, spine and head than women.9 ,12 ,14–19 It is unknown whether these suggested sex-related injury risks are related to anatomical and physiological differences between women and men, or reflect the different skiing patterns and behaviours. For knee/ACL injuries, it is suggested that environmental factors, such as cold temperature and snowfall,20 as well as personal factors, for example, leg dominance,21 may potentially have a higher impact on the injury risk among women than men. In addition, two case–control studies on skiers have indicated that ACL injury risk is increased during the preovulatory phase of the menstrual cycle.22 ,23 It has also been suggested that male skiers are more prone to risk-taking behaviours than female skiers.24
In competitive alpine skiing, we have previously reported a higher overall risk of injury in men than women, based on the preliminary data from the International Ski Federation (FIS) Injury Surveillance System (ISS).25 However, as the number of injuries was limited, we were not able to assess sex differences in subgroups, such as for time-loss injuries, knee injuries or ACL injuries. Studies among junior ski racers in Norway and Sweden have reported that men and women displayed the same injury rate and pattern.26 ,27 Studies on French ski racers28 and on US ski patrols/instructors29 suggest that there is no sex-difference in the risk of knee/ACL injuries among elite skiers; in contrast, a study among racers at a ski gymnasium in Austria reported that women had twice the risk of knee/ACL injury than men.30 Interestingly, this is supported by small surveys on Olympic racers31 and on national ski racers in the USA.32 In addition, of seven injuries recorded during the 1994 Olympic Winter Games33 and the 1995 Junior World Championship,34 all were suffered by women.
Thus, based on the available literature, it is unclear whether female-elite and male-elite skiers have the same injury risk and pattern. The aim of this study was therefore to compare the risk of injury in female versus male World Cup (WC) alpine skiers, based on 6-year data from the FIS ISS.
Methods
Injury registration
The FIS ISS was established before the 2006/2007 winter season by the FIS in collaboration with the Oslo Sport Trauma Research Center (OSTRC). The FIS ISS is based on injury registration through retrospective interviews with athletes, coaches or medical staff from 10 of the largest WC teams.25 ,35 The interviews are conducted by physicians or physiotherapists from the OSTRC at the WC finals at the end of each winter season. All the athletes who are present in person are interviewed directly, while their coaches or medical staffs are interviewed if the athlete is not present (due to injury or for other reasons). Athletes, coaches and medical staffs are asked to recall any acute injury requiring medical attention, regardless of their consequences in terms of time loss from sport, occurring in training or competition during the 5-month WC season. The interview is done using a form outlining a week-by-week calendar of the WC season as an aide-memoire. If an injury is recorded, a specific injury registration form is completed for each injury. This form includes informations about the body part injured, injury circumstances, injury type, injury severity (expressed as days of absence from full participating in training and competition), injured side and a specific diagnosis (based on team medical staff assessment). The procedures and limitations of the FIS ISS injury registration have been described in more detail previously.25 ,35
Exposure data
For each athlete interviewed, we calculated the exact number of started runs in the WC during each of the six seasons (2006–2012). An exposure file was created in Excel, V. 2010. The result list for each WC race was extracted one by one from the FIS database online into the Excel file. Specific variables were added to the result for each of the athletes, that is, date, race codex, discipline, place and sex. In addition, a new variable was created to calculate the number of started runs for each of the results, taking the specific discipline (one run in downhill and Super-G vs two runs in giant slalom and slalom) and descriptions used by the FIS for athletes who did not complete the first or second run (ie, did not start, did not finish, disqualified and did not qualify) into account. The runs from the combination events (one run in downhill or Super-G and one run in slalom) were separated into the specific disciplines. The exposure data in the Excel file were then transferred to our database (Oracle Database 11 g, Oracle Corporation, California, USA), where we linked the exposure data for each athlete to the information recorded through the interviews.
Statistical analyses
Injury risk is presented as absolute (number of injuries/100 athletes/season) and relative injury rates (number of injuries per 1000 runs). We based our calculations on the Poisson model and used a Z test to compare the injury risks between sexes and disciplines. Injury incidences and relative risks (RR) are presented with 95% CI, and a two-tailed p value ≤0.05 was considered significant.
Results
In total, 1593 interviews were completed during the six seasons (2006–2012), 708 on female and 885 on male skiers (table 1). The athlete interviews were conducted in person in 569 cases, indirectly through the coaches in 979 cases and through the doctor/physiotherapist in 45 cases. During the six seasons, 309 athletes were interviewed 1–3 times, and 201 athletes were interviewed 4–6 times. They reported a total of 577 skiing injuries, 269 from training sessions and 308 from races, mainly the WC (83.4%), including World Ski Championship and Olympic Winter Games. WC exposure (number of started runs by the interviewed athletes) included a total of 27 489 runs during the six seasons.
The number of athletes interviewed, injuries reported, World Cup (WC) injuries reported and the number of WC runs started for each of the six seasons (2006–2012)
The absolute injury rate, including all training sessions and races, was 36.2 injuries/100 athletes/season (95% CI 33.3 to 39.2), higher among men 39.7 (35.5 to 43.8) than women 31.9 (27.8 to 36.19), RR 1.24 (95% CI 1.05 to 1.47). The majority of injuries were time-loss injuries (82.3%), leading to the absence from training and competition for at least 1 day. The corresponding rate for time-loss injuries only was also higher for men (32.5 injuries/100 athletes/season, 95% CI 28.8 to 36.3) than women (26.4, 95% CI 22.6 to 30.2), RR 1.23 (95% CI 1.03 to 1.48; figure 1).
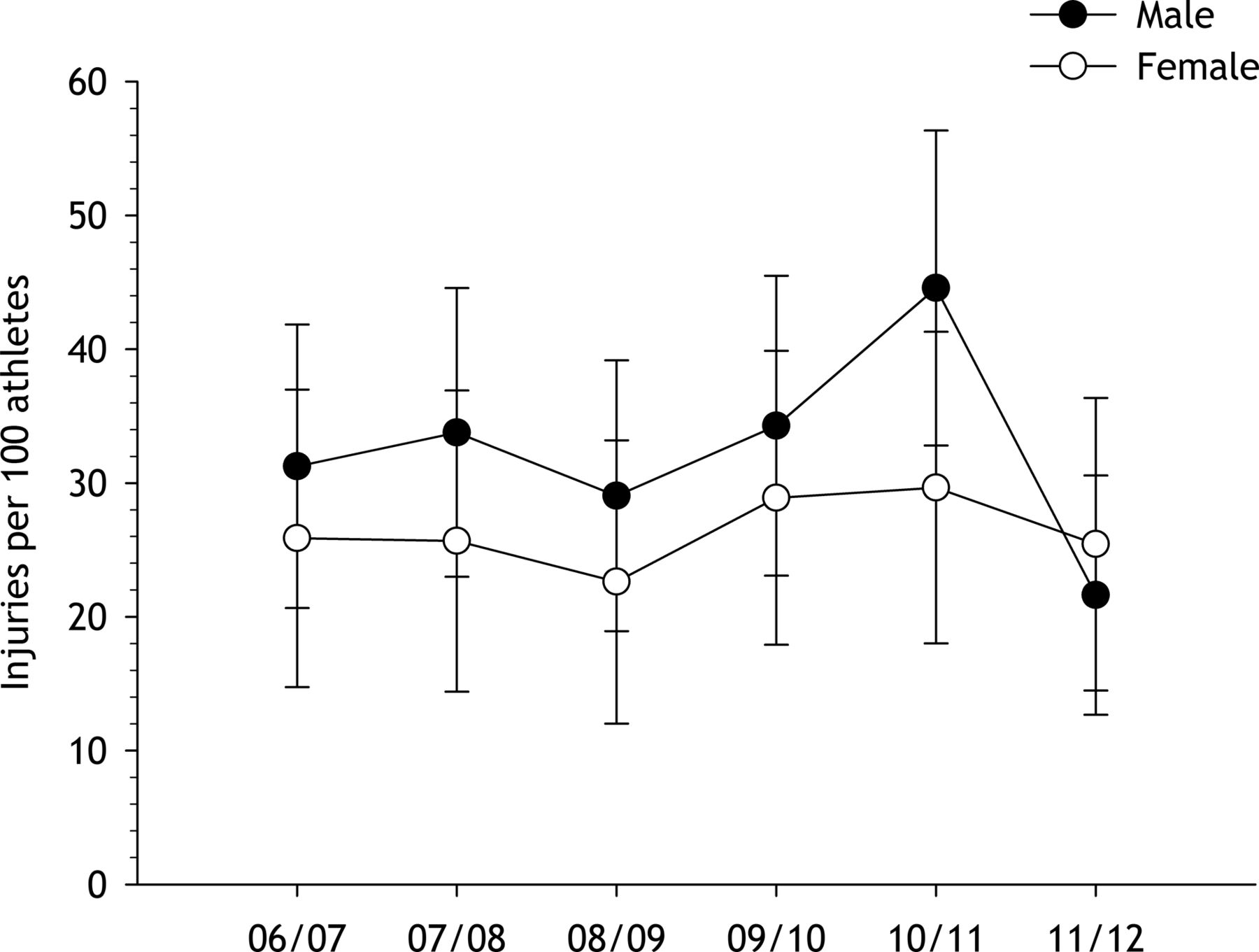
Time-loss injury rates, expressed as the number of injuries/100 athletes (with 95% CIs) among women and men for each of the six seasons (2006–2012).
Of the 577 injuries reported, 257 (45.5%) occurred in WC races. The relative injury rate, expressed as injuries per 1000 runs, was higher for men (11.3, 95% CI 11.1 to 11.5) than women (7.1, 95% CI 7.0 to 7.3), RR 1.58 (95% CI 1.22 to 2.04). For time-loss injuries only (n=201), the corresponding incidence was 9.1 injuries/1000 runs (95% CI 8.9 to 9.3) for men versus 5.3 (95% CI 5.2 to 5.4) for women (RR 1.72, 95% CI 1.29 to 2.31; figure 2).

Time-loss injury incidences in World Cup races, expressed as the number of injuries per 1000 runs (with 95% CIs) among women and men for each of the six seasons (2006–2012).
Of all time-loss injuries (n=475), 43% were severe (absence 28 days), 31% moderate (8–28 days), 15% mild (4–7 days) and 9% minimal (1–3 days; in 8 cases, information on severity was not available at the time of interview). Men had a higher absolute rate of moderate injuries than women, and during WC races, a higher relative rate of moderate and severe injuries (table 2).
Injury incidence for each injury severity category (expressed as the number of days of absence from training and competition) among women and men throughout the six seasons (2006–2012)
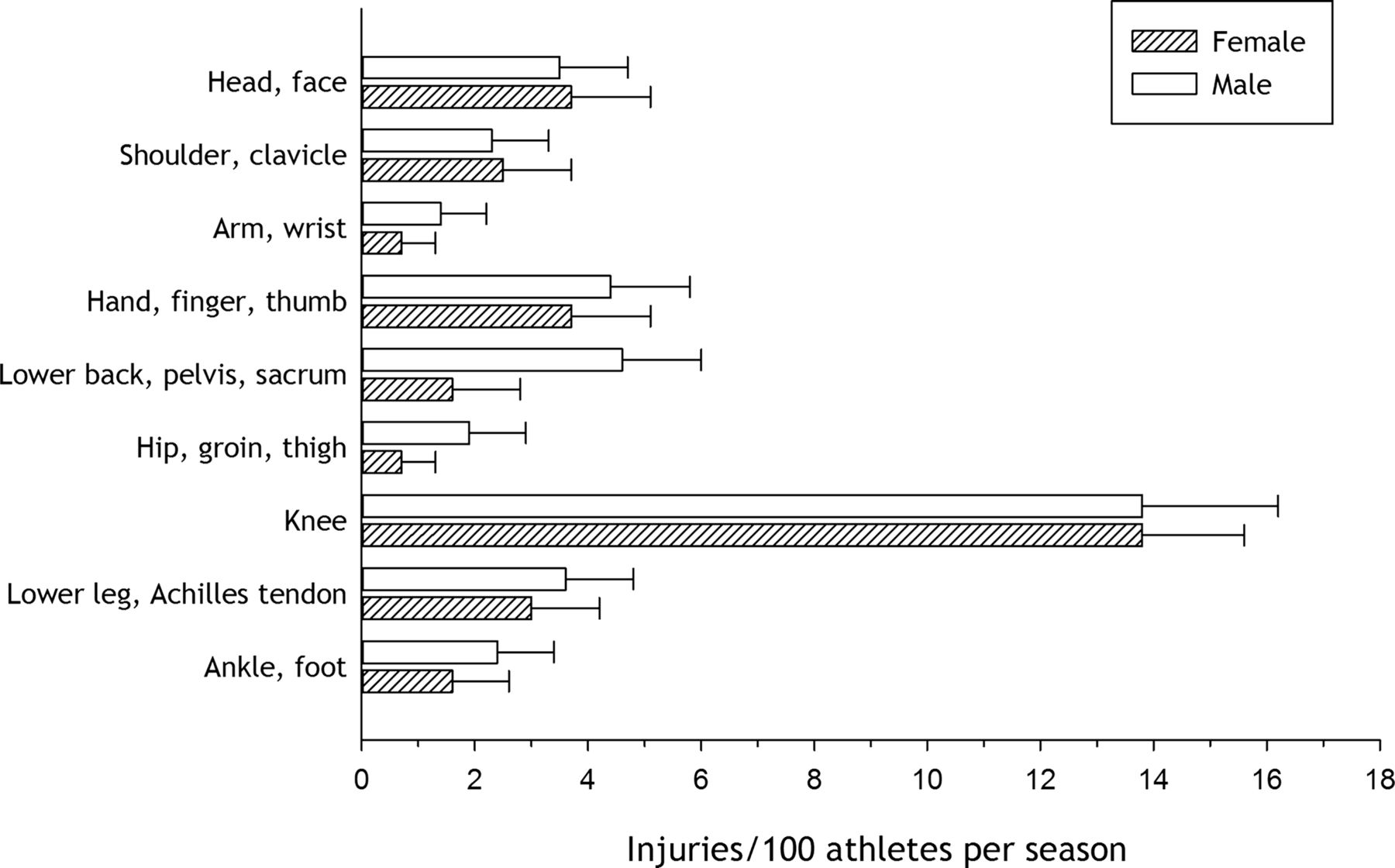
Of all injuries reported (n=577), the most common injury location, expressed as body part, was the knee (38%), followed by hand/finger/thumb (11%), head/face (10%), lower leg/Achilles tendon (9%), lower back/pelvis/sacrum (9%) and shoulder/clavicle (7%). There was no sex difference in the absolute rate of knee injury (RR 1.00, 95% CI 0.77 to 1.31, Figure 3). Also, there was no difference in the absolute rate of ACL injury between women (5.4 injuries/100 athletes/season, 95% CI 3.7 to 7.1) and men (5.5, 95% CI 4.0 to 7.1; RR 1.03, 95% CI 0.68 to 1.58). For injuries to the lower back/pelvis/sacrum, men (4.6, 95% CI 3.2 to 6.1) had a significantly higher absolute injury rate than women (1.6, 95% CI 0.6 to 2.5; RR 2.98, 95% CI 1.5 to 5.8). Men (5.4, 95% CI 3.9 to 7.0) also had a higher absolute rate of muscle and tendon injuries than women (2.1, 95% CI 1.0 to 3.2; RR 2.56, 95% CI 1.43 to 4.57). We could not detect any sex differences in absolute injury rate for any other body location or injury type.

{kind=link}
{kind=link}
{kind=link}
Injury incidence, expressed as injuries/100 athletes/season, for the different injury locations for female versus male skiers.
Almost half of the knee injuries (46.4%, n=102) occurred in WC races; thus, we also calculated the relative injury rate taking race exposure into account (injuries per 1000 runs). Similar to what we found for absolute injury rate, there was no difference in the relative rate of knee injury between women and men (table 3). The corresponding rate of ACL injuries (n=41) was 1.7 (95% CI 1.0 to 2.4) for men versus 1.2 injuries/1000 runs (95% CI 0.6 to 1.9) for women (RR 1.38, 95% CI 0.74 to 2.58).
Injury incidence based on all WC injuries reported as well as for knee injuries only in the different alpine disciplines
The relative injury rate, as well as that of knee injuries, was highest in downhill, followed by Super-G, giant slalom and slalom (table 3).
Discussion
This is the largest study to date comparing injury risk during the competitive season between female-elite and male-elite skiers. The principal findings were that men had a higher overall risk of injury, as well as higher risk of time-loss injury than women in training and competition. However, while men had a higher risk of moderate and severe injuries than women, there was no sex difference in the risk of knee/ACL injuries.
No previous studies from competitive alpine skiing have reported a significantly higher risk for injuries in men than women, apart from our own initial report from the first two seasons of the FIS ISS.25 The current study builds on the initial report, where we observed a higher overall injury rate among men than women, but did not detect a significant difference for more serious (ie, time-loss) injuries, most likely due to low study power. In contrast, in a study among junior ski racers attending an elite high school programme in Sweden, based on time-loss injuries reported during a 5-year period, no significant sex differences were observed in the injury rate or pattern.26 Even though a direct comparison of the injury risk between junior ski racers and WC athletes should be carried out with caution, these studies indicate that the injury risk in men may increase relative to women as the racers mature to compete at the WC level.
Our results are also in contrast to those reported from older studies on competitive racers. A study on injuries reported from 251 Norwegian ski races during the 1981/1982 winter season did not detect any sex differences.27 In three small studies, the world's best skiers were asked whether they had sustained a severe injury during their career, and the injury definition was an impairment to health and working ability for more than 20 days.31 ,36 ,37 Two of the studies reported no sex difference in the proportion reporting previous severe injuries,36 ,37 while the third study found a significantly higher proportion among women.31 However, competitive skiing has changed substantially since the 70s and 80s and these studies should be interpreted with caution due to major methodological limitations; response rates were low and there would be a selection bias due to skiers retiring early because of severe injuries. The current study is the most comprehensive to date on sex differences in the risk of injury. Injuries were recorded among athletes from 10 different nations throughout six consecutive winter seasons, while previous studies have reported injuries among athletes from single national teams,26–28 ,32 during single events33 ,34 or were based on retrospective recall without exposure recording.31 ,36 ,37 In the current study, we were able to calculate the exact exposure (number of started runs in competition) for each athlete each season based on the FIS racing database.
The explanation for the sex difference observed is not known. We know that in WC alpine skiing, men and women compete in different courses, usually longer and with a higher vertical drop and higher skiing speed for men.38 Thus, skiers may have too little time to react and adjust to sudden variations in postural stability and forces acting on the body, for example, caused by sudden changes in course and snow conditions. High skiing speed also means high kinetic energy, and it is reasonable to suggest that in the event of a quick energy conversion, such as during crashes, severe injuries may occur.39 A higher risk of severe injuries among men than women can also be related to different skiing patterns (technique and strategy) and risk-taking behaviours. In recreational skiing, it is suggested that men are more prone to risk-taking behaviours compared with women.24
Interestingly, while we found that men had a higher overall risk of moderate and severe injuries than women, there was no difference in the risk of knee/ACL injuries. From systematic video analyses of injuries in WC alpine skiing, we know that knee/ACL injuries mainly occur while skiing, before or without falling, while the majority of injuries to the upper body occur as a result of falling/crashing.40–42 Considering the mechanisms of injuries and the current findings, it seems reasonable to suggest that the male to female ratio concerning injury risk changes according to the different injury types. Previous studies support that there is no sex-related difference in the risk of knee/ACL injuries among expert skiers.26 ,28 ,29 However, it should be mentioned that a study on ACL injuries among young ski racers in Austria, reported a higher risk among women than men. They also suggested that poor core strength is a critical factor for ACL injuries in young ski racers.30 While experienced WC athletes are thought to be extremely fit,43 ,44 it is suggested that young female athletes are not always sufficiently prepared for elite ski racing, and may therefore be at higher risk of injury.39 This may explain why we found a higher male to female ratio among WC athletes than what have been reported among junior ski racers.26 ,27 ,30
In contrast to recreational skiing and team sports, where women are more at risk for knee/ACL injuries,1–3 8–13 we suggest that anatomical and physiological differences between women and men in WC alpine skiing will have less influence on the risk of knee/ACL injuries because the high energy involved will cancel out potential sex-related intrinsic risk factors. Based on our current findings and the fact that the majority of knee/ACL injuries occur while still skiing, we suggest that the skiing pattern (technique and strategy) and risk-taking behaviour are more critical for knee/ACL injury risk rather than sex-related intrinsic risk factors. An obvious consequence of this is that the prevention of knee/ACL injuries must be directed as much towards male as female skiers.
Conclusion
Men had a higher rate of time-loss injury than women in training and competition, and this sex difference was even more pronounced during WC races. However, while men had a higher overall risk of moderate and severe injuries than women, there was no sex difference in the risk of knee/ACL injuries. Therefore, in contrast to recreational skiing and team sports, the prevention of knee/ACL injuries should be directed as much towards male as female competitive skiers.
What are the new findings?
-
This is the largest study to date comparing injury risk during the competitive season between female-elite and male-elite skiers.
-
No previous studies from competitive alpine skiing have reported a significantly higher risk for injuries in men than women.
-
In contrast to recreational skiing and team sports, where women are more at risk for knee/anterior cruciate ligament (ACL) injuries, there was no difference in female versus male World Cup alpine skiers.
How might it impact on clinical practice in the near future?
-
Prevention of knee/ACL injuries must be directed as much towards male as female competitive skiers.
Acknowledgments
We would like to thank the World Cup athletes, coaches and medical team personnel who participated in this study and the International Ski Federation staff and officials for all practical support.
References
Footnotes
-
Contributors TB, TWF, LN and RB contributed to study conception, design and methodology. TB and TWF coordinated the study and managed the data collection. TB wrote the first draft of the paper, and all authors contributed to the final manuscript. TB and RB are guarantors.
-
Funding The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Norway Regional Health Authority, the International Olympic Committee, the Norwegian Olympic Committee & Confederation of Sport, and Norsk Tipping AS. The FIS Injury Surveillance System is supported by the International Ski Federation and was established through a generous grant from DJO.
-
Competing interests None.
-
Ethics approval The study was reviewed by the Regional Committee for Medical Research Ethics, South-Eastern Norway Regional Health Authority, Norway.
-
Provenance and peer review Not commissioned; internally peer reviewed.