Article Text

Abstract
Background In ice hockey, body checking is associated with an increased risk of injury. In 2011, provincial policy change disallowed body checking in non-elite Pee Wee (ages 11–12 years) leagues.
Objective To compare the risk of injury and concussion between non-elite Pee Wee ice hockey players in leagues where body checking is permitted (2011–12 Alberta, Canada) and leagues where policy change disallowed body checking (2011–12 Ontario, Canada).
Method Non-elite Pee Wee players (lower 70%) from Alberta (n=590) and Ontario (n=281) and elite Pee Wee players (upper 30%) from Alberta (n=294) and Ontario (n=166) were recruited to participate in a cohort study. Baseline information, injury and exposure data was collected using validated injury surveillance.
Results Based on multiple Poisson regression analyses (adjusted for clustering by team, exposure hours, year of play, history of injury/concussion, level of play, position and body checking attitude), the incidence rate ratio (IRR) associated with policy allowing body checking was 2.97 (95% CI 1.33 to 6.61) for all game injury and 2.83 (95% CI 1.09 to 7.31) for concussion. There were no differences between provinces in concussion [IRR=1.50 (95% CI 0.84 to 2.68)] or injury risk [IRR=1.22 (95% CI 0.69 to 2.16)] in elite levels of play where both provinces allowed body checking.
Conclusions The rate of injury and concussion were threefold greater in non-elite Pee Wee ice hockey players in leagues where body checking was permitted. The rate of injury and concussion did not differ between provinces in elite levels, where body checking was allowed.
- Hockey
- Risk factor
Statistics from Altmetric.com
Introduction
Ice hockey is one of Canada's most popular winter sports for youth, with over a half million players registered with Hockey Canada in the 2011–2012 season.1 Participation in sports such as hockey is positively associated with motor skill development,2 higher self-esteem3 and increases in perceived health and life satisfaction.4 However, hockey also has a high risk of injury.5 ,6 A study conducted over the 2007–2008 Pee Wee (ages 11–12 years) ice hockey season in Alberta reported a game injury rate of 4.20/1000 player-hours.7 Alarmingly, concussion was the most common injury with a rate of 1.47/1000 player-hours in Pee Wee body checking leagues.7
Body checking is a principle defensive tactic commonly used in ice hockey, whereby a player propels their body towards a player carrying the puck in order to separate the player from the puck. This movement is usually in a different direction than the puck carrier.8 Policy surrounding the age of introduction to body checking is perceived as a controversial topic. However, a review examining the risk factors for injury in youth hockey identified body checking as the single most consistent risk factor.9 Correspondingly, a previous study of Pee Wee ice hockey players reported that elite players exposed to body checking had a 3.3-fold higher rate of injury and 3.9-fold higher rate of concussion than players in a league where policy disallowing body checking had been in place for 20 years.7 In addition, body checking experience in Pee Wee was not found to be protective of all injury or concussion in the Bantam age group (ages 13–14 years).10 In response to the increasing evidence of the association between policy allowing body checking and injury risk, Ontario's Hockey Federation (OHF) disallowed body checking in all age divisions of House League and Select hockey (non-elite lower 70% by division of play) in the 2011–2012 season, providing an opportunity for a comparative study of injury rates in these two cohorts.
Understanding how policy changes affect all injury and concussion risk in youth sport at all levels of play is essential for future evidence-informed policy regarding injury prevention. Therefore, the primary objective of this study was to determine if the risk of all injury and concussion specifically differed for non-elite Pee Wee ice hockey players in leagues where body checking was permitted (Alberta) compared with leagues where a recent policy change disallowed body checking (Ontario).
Methods
Study design and subjects
A cohort study was conducted during the 2011–2012 ice hockey season. The study population included Pee Wee players (ages 11–12 years) from Calgary (Alberta) and the Greater Toronto Area (Ontario). Cohorts were categorised based on their exposure to rules that permitted or disallowed body checking. The primary comparison was made between non-elite players (ie, lower 70% by division of play) from Ontario, where body checking was disallowed, and Alberta where body checking was allowed. Specifically, the Ontario cohort included players from House League and Select divisions and the Alberta cohort included players from divisions 4 to 11. In order to examine provincial differences, elite players (upper 30% by division of play) where body checking was permitted in both provinces were also recruited. Recruitment was conducted in the Greater Toronto Hockey League (GTHL), North York Hockey League (NYHL) and Mississauga Hockey League (MHL) in Toronto and Hockey Calgary. Teams participating in girls-only Pee Wee leagues were excluded. A sample size calculation was based on previous study concussion rates7 powered with an incidence rate ratio (IRR)=3 (concussion rate=1.47/1000 player-hours in Alberta, adjusting for cluster and anticipated 10% drop-out rate (α=0.05, β=0.20)). A sample size of 30 teams in non-elite and 30 teams in elite levels of play would be required per province. Calgary utilised an inclusive recruitment strategy in which all league presidents were approached for participation. In Ontario, eligible teams in three associations were entered into a spreadsheet, the team order was then randomised and teams were approached to participate in this newly randomised order. Teams are entitled to a maximum of 19 players, but vary in numbers.8 Individual participants from teams recruited could choose to consent to the study.
Procedures
A previously validated injury surveillance system validated in youth ice hockey from the Canadian Intercollegiate Sport Injury Registry (CISIR) was used.5 ,7 ,11 At the beginning of the season, players completed a baseline questionnaire that captured demographic and risk factor information, including a preference towards body checking survey. During the season, team designates (parent volunteer) completed weekly exposure sheets (player participation forms). Exposure data were imputed based on the mean game and practice hours in the weeks that the team had complete weekly exposure data for teams missing occasional weeks of exposure data. If an injury occurred (including all suspected concussions) the details injury were collected using an Injury Report Form (IRF). The IRF included details on the mechanism of injury (ie, body checking, other intentional contact, unintentional contact, contact with environment (ie, puck, boards, net) without any contact with another player, no contact), time, date, session type, time loss and medical follow-up. A physiotherapist or certified athletic therapist reviewed all IRFs. For the purpose of this study, an injury was defined as any injury that required medical attention, resulted in the inability to complete the session and/or required the child to miss at least 1 day of activity. Injuries that resulted in >7 days of time loss were defined as severe injuries. All suspected concussions were referred to a sports medicine physician associated with the study for medical follow-up. Suspected concussions that were not assessed by a physician were included in injury estimates if they met the concussion definition based on the study therapist's review of the IRF. In accordance with the most recent international sport-concussion consensus guidelines, a concussion was defined as a brain injury induced by traumatic forces, either direct or indirect, and resulting in one or more clinical symptoms.12 ,13 If concussion symptoms lasted for >10 days it was categorised as a severe concussion.
Analysis
STATA V.1214 was used to perform all statistical analyses. Baseline characteristics were compared between Ontario and Alberta, and elite versus non-elite. Statistical significance was based on an α level of 5%. IRRs and 95% CIs were estimated using Poisson regression analysis, accounting for any clustering by team effect and offset by player-hours. Models for primary injury outcomes (all injury and concussion) were adjusted for other covariates including: year of play, height, weight, previous injury or concussion, level of play, position and attitudes towards body checking. Participants with missing covariate data were excluded from the adjusted models. Owing to low event rates of secondary outcomes, severe injuries and severe concussions, univariate models were reported adjusting for cluster by team and offset by player-hours. Session type was considered an important modifier given the increased risks associated with game play. Sex was not considered a covariate because of the low number of female participants.
Ethical considerations
All player participants and their parents provided written consent for entry into this project. Ethics approval was obtained from the Conjoint Health Research Ethics Board at the University of Calgary and York University's Human Participants Review Sub-Committee.
Results
In Alberta, 115 teams were approached for entry into the study and 59 (51.3%) teams completed the study; (41 did not respond, 11 refused and 4 dropped out). In Ontario, 123 teams were approached and 46 (37.4%) teams completed the study (54 teams did not respond, 17 refused and 6 dropped out). Reasons provided for known refusals included the inability to identify a designate to record data and lack of interest in the study. The final study population included 59 Alberta teams (n=590 non-elite, n=294 elite players) and 46 Ontario teams (n=281 non-elite, n=166 elite players). An average of 15 (range; 5–19) players per team in Alberta and 10 (range; 2–18) players per team in Ontario gave consent to participate in the study.
Self-reported baseline characteristics of players by province and level are displayed in table 1. Among non-elite teams there were similar proportions of players playing different positions, female players and similar injury history in Alberta and Ontario. However, non-elite players in Alberta reported a greater preference for body checking and a greater proportion reported a prior concussion. There were a greater proportion of players in their second year of Pee Wee in Ontario compared with Alberta.
Baseline characteristics comparing non-elite and elite Pee Wee (11–12 years) Hockey Players in Alberta and Ontario, 2011–2012
Over the 2011–2012 season, Alberta non-elite players had more game-hours per player on average (40.9 (95% CI 40.08 to 41.70)) than Ontario players (31.13 (95% CI 29.60 to 32.67)). Elite players from Alberta and Ontario had similar game-hours per player (44.7 (95% CI 43.62 to 45.83) in Alberta and 42.9 (95% CI 39.94 to 45.89) in Ontario). Non-elite players from Alberta practiced an average of 34.84 h while non-elite players from Ontario practiced 30.33 h. Elite players from Alberta practiced an average of 42.96 h while elite players from Ontario practiced 53.89 h.
There were a total of 120 injuries (77 concussions) reported by non-elite Pee Wee players in Alberta in 44 682.08 player exposure hours and 19 injuries (11 concussions) per 17 272.5 player exposure hours in Ontario (games and practices combined). The injury rates and unadjusted IRRs specific to game-related injuries among non-elite players are summarised in table 2. Injuries that met the injury definition included: cuts, joint swelling, ligament sprains, fractures, muscle strains and concussions. Of the 101 game injuries sustained by non-elite players in Alberta, 37.6% resulted in >7 days of time loss and were categorised as severe injuries accordingly. In Ontario, 57.1% of the 14 injuries were categorised as severe. Some of the suspected concussions that met the injury definition were not assessed by a physician. The proportion of game-related concussions among non-elite players assessed by a physician was 64.2% (95% CI 52.4% to 76.0%) in Alberta and 87.5% (95% CI 57.9% to 100%) in Ontario.
Game-related injuries among non-elite Pee Wee ice hockey players (2011–2012)
Table 3 summarises the results of the risk factor analysis for non-elite players. When adjusted for year of play, previous history of injury/concussion, level of play, position and attitude towards body checking; policy allowing body checking (Alberta) was significantly associated with a greater rate of all injury (IRR=2.97, 95% CI 1.33 to 6.61) and concussion (IRR=2.83, 95% CI 1.09 to 7.31). The model was based on a Poisson regression model with robust SE adjusted for clustering by team. There were 735 participants with complete data included in the estimation of the adjusted IRR for injury and 753 participants included in the estimation of the adjusted IRR for concussion. Sensitivity analyses were performed to assess both previous non-concussive injuries in the last year and history of concussion for each outcome. These adjustments did not change the results in a practical or significant way. Therefore, the final statistical model included previous injury (no concussion) in the last year for the outcome of injury and previous concussion for the outcome of concussion. Player height and weight were initially included in the model but were removed due to multicollinearity with year of play. Being in the first year of play as well as having a history of concussion was associated with a significant increase in the rate of concussion.
Risk factor analyses for game-related injury, concussion and severe concussion in non-elite Pee Wee ice hockey in Alberta and Ontario (2011–2012)
Elite players (upper 30% by division of play) in Ontario and Alberta (players in both provinces exposed to body checking 2011/2012 season) had similar injury and concussion rates (table 4). There were 385 participants with complete data included in estimating the adjusted IRR for injury and 393 participants included in estimating the adjusted IRR for concussion. The proportion of suspected game-related concussions that were assessed by a physician among elite athletes was 88.9% (95% CI 78.1% to 99.7%) in Alberta and 84.6% (95% CI 61.9% to 100%) in Ontario. Time loss following a suspected concussion for both elite and non-elite players depended on whether or not a player saw a physician (table 5).
Game-related injuries among elite Pee Wee ice hockey players (2011–2012)
Number of calendar-days lost from suspected game-related concussion according to whether or not participants saw a physician
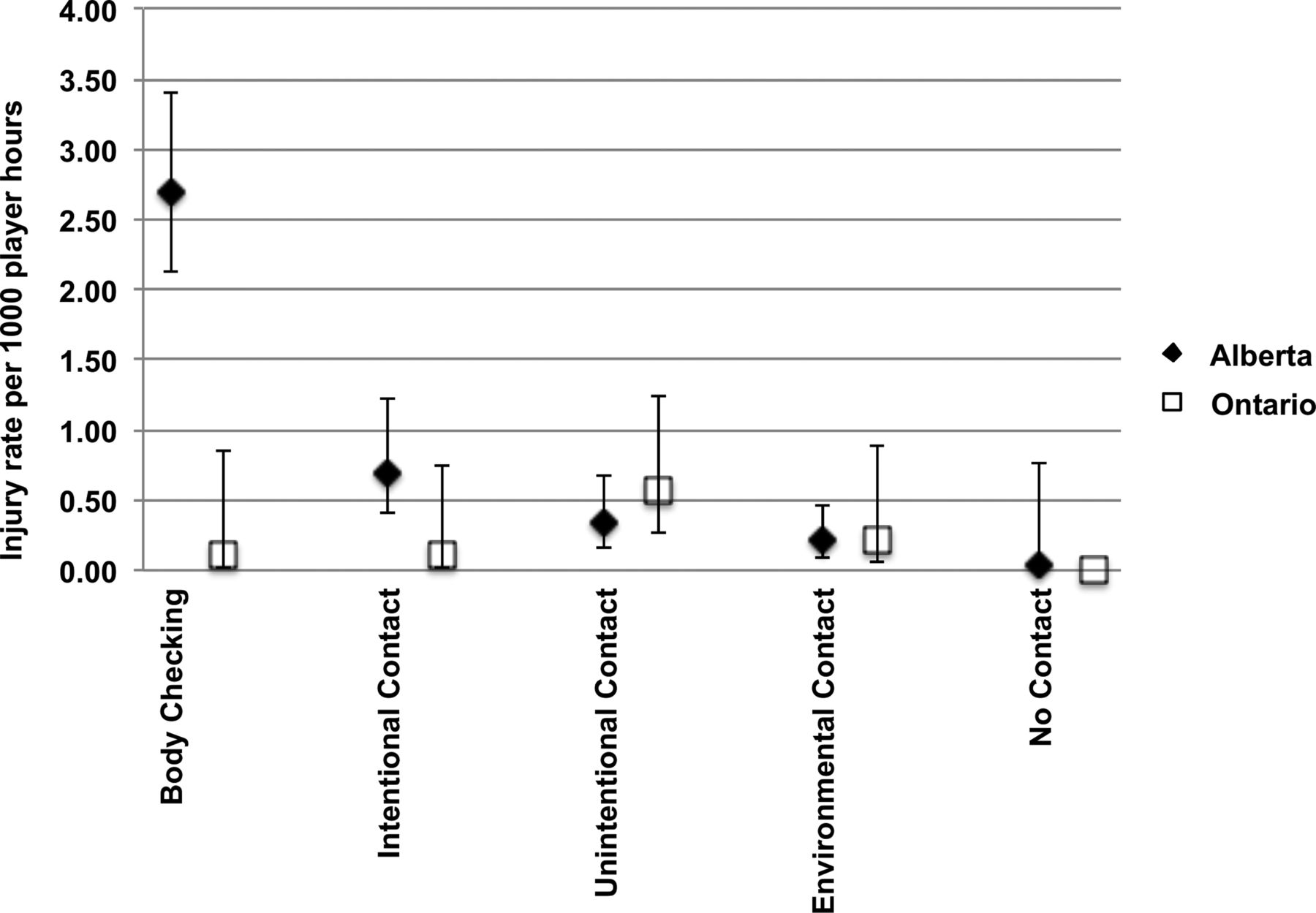
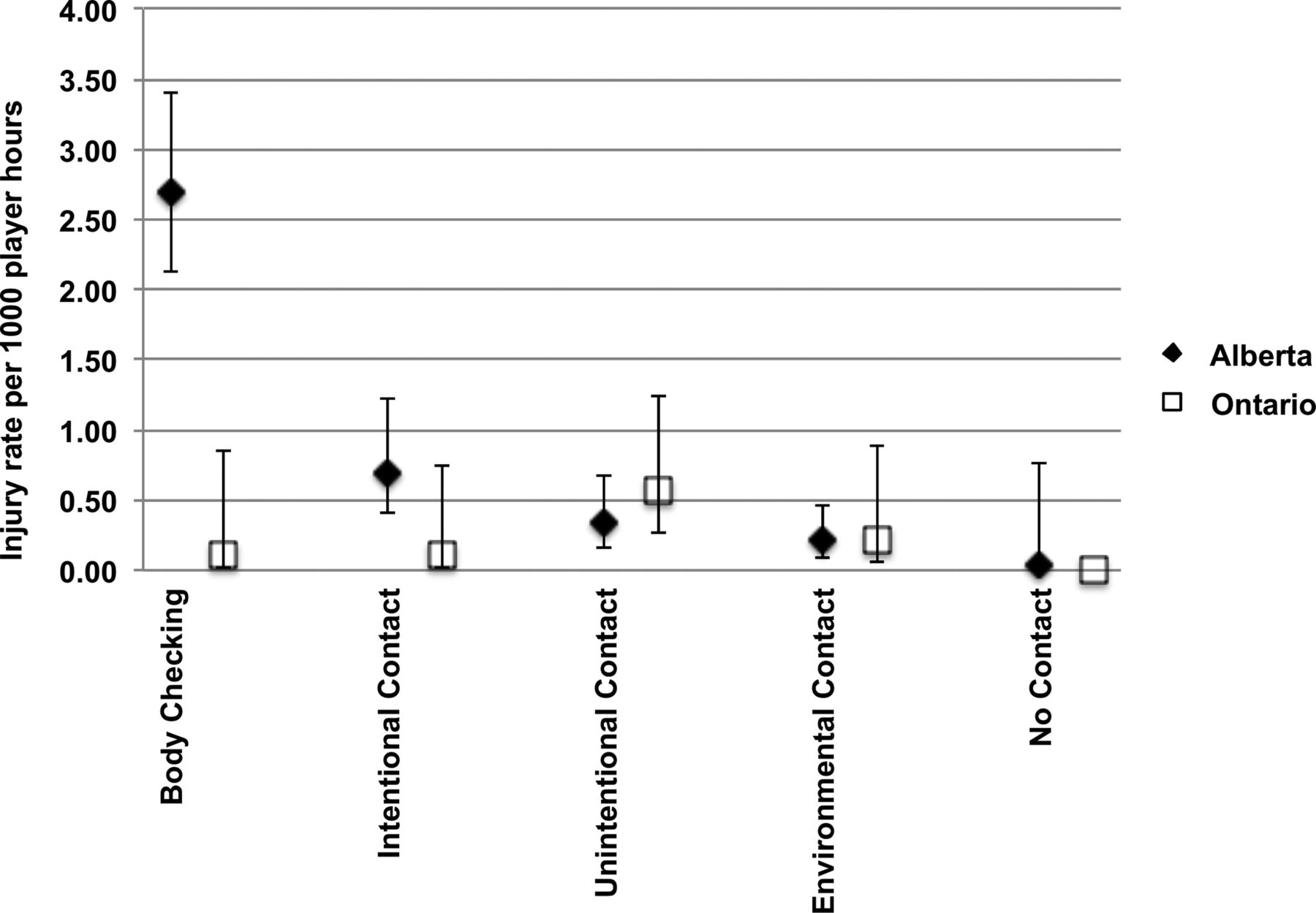
Figure 1 displays game injury rate (IR) by mechanism. Eight of the 101 injuries in Alberta and five of the 14 injuries in Ontario had no mechanism on the injury report form. In Alberta (body checking permitted in non-elite), the primary mechanism of injury was body checking (body checking IR=2.66 (95% CI 2.13 to 3.40) injuries per 1000 player-hours). The primary mechanism of injury in the Ontario non-elite cohort (non-checking) was unintentional contact (unintentional contact IR=0.57 (95% CI 0.26 to 1.25) injuries per 1000 player-hours). The body checking IR among the elite players from Alberta and Ontario was similar (body checking IR=2.36 (95% CI 1.56 to 3.55) and 2.11 (95% CI 1.06 to 4.07) per 1000 player-hours, respectively).
{kind=link}
Game injury rate by province and mechanism among non-elite players. Error bars indicate 95% CIs.
Discussion
This is the first study to evaluate a body checking policy change that disallowed body checking in non-elite youth ice hockey, immediately following that policy change. Among Pee Wee non-elite hockey players there was a threefold greater rate of injury and concussion associated with playing in a league that permitted body checking (Alberta) when compared with a league where policy change no longer permitted body checking (Ontario). Body checking was also identified as the most common mechanism of injury in non-elite players playing in body checking leagues. These results extend previous reports of the risk associated with policy allowing body checking among Pee Wee hockey players at all levels of play.7
Pee Wee players in body checking leagues in Alberta during the 2007–2008 hockey season had a threefold greater risk of all injury and a fourfold greater risk of concussion than players in Quebec where body checking was not permitted. This previous study differs in that the non-body checking comparison province was Quebec where policy disallowing body checking had been in place for over 20 years. Consistent with this, a previous meta-analysis including four studies examining body checking as a risk factor for concussion demonstrated a combined greater risk in leagues allowing body checking (OR=1.71 (95% CI 1.2 to 2.44)).9
The game-related concussion rate (# concussions/1000 game-hours) appears to have increased in Alberta (concussion rate=2.78), in comparison to the previously reported rate in 2007/2008 (concussion rate=1.47).7 This may be associated with a greater awareness and reporting of concussions in youth ice hockey. This trend is also seen in the no-body checking cohort where the concussion rate in Ontario was 0.91, in comparison to the previously reported rate in 2007/2008 in Quebec (concussion rate=0.39).
There were similar rates of injury and concussion among elite players (top 30% of divisions) from both provinces exposed to body checking. This suggests province is not associated with differences in all injury or concussion data capture. However, elite players in Alberta did have a greater rate of more severe concussion (>10 days of time loss), than players in Ontario. This may suggest a true difference in concussion severity or could be due to other factors such as slight differences in the physician availability and management of concussion between the two provinces despite standardisation of return-to-play protocol based on the international consensus on sport concussion at the time of the study.13
Non-elite players from Alberta demonstrated a stronger preference towards body checking than players from Ontario. Similar differences were reported in a study by Emery et al7 comparing players from Alberta and Quebec. Fraser et al15 examined the initial experiences with body checking of players aged 11–12 years from Ontario using semistructured interviews. The interviews suggested players appear to associate the introduction of body checking with aggression, power, invincibility and fear, whereby, some players play tough and some players shift their focus away from winning the puck and towards taking the body.15 This may explain a greater preference towards body checking in non-elite players from Alberta where a greater proportion of players were previously exposed to body checking than Ontario, or alternatively selection bias related to players who did not prefer body checking discontinuing participation. The preference towards body checking was similar among elite players (exposed to body checking) from both provinces in this study.
Limitations
This study had some limitations. A greater proportion of teams in Alberta agreed to participate compared to Ontario. However, the main reason for refusal in both provinces was the inability to identify a team designate. Injury rates are based on the injury report form being initiated by the team designate and followed up with referral to a study physician or physiotherapist/athletic therapist if injury lasted for >7 days, representing a slight deviation from previous studies7 ,9 where a physiotherapist/athletic therapist would follow-up with teams on a weekly basis. This is reflective of the resources available to non-elite teams who may not have access to healthcare professionals and may have resulted in an underestimation of the injuries. However, both provinces used the same criteria for injury definition and therefore it is unlikely that this reporting bias would have affected the provinces differently.
The fact that some participants chose to not use the referral to the study physician or seek other medical assessment following a suspected concussion is a limitation of our study. In these cases, suspected concussions were included if they met the concussion definition based on the study therapists’ review of the injury report form. The proportion of suspected concussions among non-elite players assessed by a physician was lower in Alberta than Ontario (64.2%, 95% CI 52.4% to 76.0% vs 87.5%, 95% CI 57.9% to 100%). While this is not a significant difference, it could lead to a slight overestimate of the IRR if the injury form by the designate was inaccurate. Demographics and baseline risk factors are based on self-report, which may lead to non-differential misclassification bias, though this is not really a concern given that we found significant differences between the non-elite cohorts. It is unlikely our results are influenced by other factors that would cause an increase in the rate of injuries in Alberta. The elite team point estimate of the IRR indicated no practical or statistically significant difference between Alberta and Ontario for all injuries (adjusted IRR 0.98; 95% CI 0.53 to 2.96) and concussions specifically (adjusted IRR 1.22; 95% CI 0.61 to 2.46).
Conclusion
Playing in a league that permits body checking is associated with a threefold increase in the rate of injury (including concussion) among non-elite ice hockey players aged 11–12 years. This research will inform future studies evaluating the effectiveness of the 2013 national policy change by Hockey Canada (eliminating body checking at all levels of play in Pee Wee) in preventing injuries and concussions across all levels of play in Pee Wee and the implications of such policy change for older age groups. Hockey remains a collision sport with several inherent features that increase athletes’ susceptibility to injury. Future studies that explore other potentially modifiable factors that contribute to injury/concussion risk are important to reduce the risk of concussion among youth ice hockey players.
What are the findings?
Pee Wee (11 and 12 years) ice hockey players in Pee Wee leagues that permit body checking are at a threefold greater risk of all injuries and concussion compared with similar players in leagues where body checking policy change has disallowed body checking in non-elite levels of play.
A policy change that disallowed body checking in non-elite Pee Wee ice hockey was associated with a significantly lower the risk of concussion in this population.
Further research is necessary to evaluate the recent national policy change disallowing body checking at all levels of play in Pee Wee.
How might it impact on clinical practice in the future?
This research highlights the reduced public health burden of concussion and injury in non-elite 11 and 12 year old ice hockey when policy disallows body checking.
This study informs the potential public health implications for future policy change in more elite levels of play and older age groups.
Acknowledgments
The authors would like to thank the Pee Wee players, parents, coaches, team designates, athletic therapists, physiotherapists, study coordinators and study physicians for their assistance with this research. They would also like to thank the Ontario Hockey Federation, Hockey Calgary and Hockey Canada for supporting this research.
Footnotes
Twitter Follow work being done by Sport Injury Prevention Research Centre at @SIPRC_
Contributors AMB contributed to all research activities in Toronto and takes responsibility for the integrity of the data and accuracy of the data analysis. She led the analysis and manuscript preparation. AKM led all research activities in Toronto, and critically reviewed the manuscript. BEH contributed to the design of the study, acquisition of funding, analysis and interpretation of results, and critically reviewed the manuscript. MAR contributed to all research activities in Calgary and critically reviewed the manuscript. LP-D contributed to the technical aspects of the data analysis, participated in data interpretation and critically reviewed the manuscript. JK was responsible for technical aspects of the data analysis and participated in data interpretation and critically reviewed the manuscript. WHM contributed to the design of the study, interpretation of results and critically reviewed the manuscript. CAE takes responsibility for the integrity of the data and the accuracy of the data analysis. She led the design, acquisition of funding, all research activities as well as critically reviewed the analysis and manuscript preparation.
Funding This study was funded by the Canadian Institutes of Health Research (CIHR), Alberta Children's Hospital Institute for Child and Maternal Health and the Max Bell Foundation. AMB is supported by the Hotchkiss Brain Institute Dr T Chen Fong Doctoral Scholarship in Neuroscience. CAE is supported by an Alberta Children's Hospital Foundation Chair in Pediatric Rehabilitation. AKM is supported by a CIHR Chair in Child and Youth Health Services and Policy Research. The role of the sponsors and funding bodies was to provide financial support for this research and the translation of the findings to all community partners.
Competing interests None declared.
Ethics approval The Conjoint Health Research Ethics Board at the University of Calgary and York University's Human Participants Review Sub-Committee.
Provenance and peer review Not commissioned; externally peer reviewed.