Article Text

Abstract
Objective To identify areas of priority and activity for international sportsfederations (IFs) with respect to athlete health and safety, and global health. Results serve to direct the work of the Association of Summer Olympic IF Medical and Scientific Consultative Group, the International Olympic Committee and to influence IFs’ planning and priorities.
Methods The 28 IFs participating in the Summer Olympic Games (2016) were asked to rank the relative importance of 11 health-related topics and to report their activities or research initiatives on 27 identified topics using an electronic survey. A comparison with a similar survey (2012) was made.
Results The response rate was 100%. In general, the ‘fight against doping’ had the highest priority followed by ‘image as a safe sport’. The topics with the lowest importance ratings were ‘increasing the number of elite athletes’, and ‘health of the general population’. Despite ranking ‘health of your athletes,’ as a top priority, IFs are not addressing all aspects of athlete health. In comparison with 2012, there was a significant decrease in priority for IFs is ‘health of the general population’.
Conclusion Despite the widespread knowledge of the importance of the promotion of physical activity (sport) on global health, the decreasing priority and programming of the IFs on physical activity promotion is concerning. Although IFs have prioritised the protection of the health of elite athletes, there are gaps in programming demonstrating that IFs are missing important areas of athlete health. Improving recreational athlete health programming could also benefit population health as well as improve IF fan base and sport participation.
- Health promotion
- prevention
- sports injury
- non-communicable disease
- elite athletes
Statistics from Altmetric.com
Introduction
Athlete performances at the Olympic Games and World Championships thrill audiences globally. The quest to be ‘citius, altius, fortius’ (faster, higher, stronger), as embodied in the Olympic motto, has motivated athletes since the inaugural modern Olympic Games in 1896. Elite athlete performance is associated, by its very nature, with an elevated risk of injury and/or illness.1 It is, therefore, incumbent on all involved with sport, and in particular its international sports federations (IFs), to take steps to protect athlete health.2 In that regard, Fuller and Drawer outlined a theoretical framework to facilitate IF risk management in sport.3 Athlete health protection is also the cornerstone of the Olympic Movement Medical Code4 and is embedded in the Olympic Charter in the Mission and Role of the IOC (#9).5 Documents such as these clearly support the role and the obligation of the IFs to protect athlete health.
The Olympic Charter also supports the protection of athlete health (Article 26–1.8)5 and then goes one step further in identifying the role of the IF in the promotion of sport for all (#12)5—⇓that is, for elite athletes and for those who participate in sport recreationally. According to the WHO, insufficient physical activity (PA) is the fourth leading risk factor for non-communicable diseases (NCDs) such as cardiovascular disease, diabetes and the metabolic syndrome.6 Furthermore, physical inactivity in children can lead to an increase in the risk of hypertension, diabetes, fractures, sports injuries and obesity.7 As one of the gatekeepers of PA, sport therefore has the ability to play an active role in improving global health through the prevention of NCDs. In 2003, the United Nations Inter-Agency Task Force on Sport for Development and Peace published a paper that identified the role of sport in improving both the quality and quantity of life through the reduction of NCDs.8 Two consensus statements by the IOC have been published in this field: one on the Fitness and Health of Children, which identifies the importance of sport as a tool for promoting PA in this population7 and the second on the Prevention of Non-Communicable Diseases, which outlines a prevention strategy aimed at motivating the sport community to action.9 The WHO and the IOC signed a memorandum of understanding in 2010 to collaborate in addressing the rising prevalence of NCDs.10 A publication of the IFs’ opinions and activities in promoting health in their athletes and in the general population by Mountjoy and Junge reported that the IFs perceive the field of global health promotion to be of low priority and that only the Fédération Internationale de Natation (FINA) and the FIFA of the 35 participating IFs had programmes to promote PA.11 It is arguable that the IFs leadership role in PA promotion is just as great, if not greater, than that of governments and NGOs, as the very reason for the existence of IFs is to organise and promote their respective sports around the world.
It is apparent that both athlete health protection and the promotion of PA to improve global health should be important responsibilities of the IFs, and the work of FINA and FIFA Medical Assessment and Research Centre (F-MARC) illustrates that the IFs have the capability to effectively promote PA. The objectives of the present study were to identify the current areas of priority and activity for IFs with respect to athlete health and safety and global health and to evaluate for changes in comparison with 2012. The results are meant to direct the activities of the Association of Summer Olympic International Federations (ASOIF) Medical and Science Consultative Group and to influence the planning and priorities of the IFs and the IOC Medical and Scientific Commission.
Methods
The 28 IFs on the programme of the Summer Olympic Games (table 1) were requested to answer a survey on their priorities and programming regarding athlete and global health. The study was designed and supervised by the authors, while the facilitation and technical implementation of the online survey was supported by PriceWaterhouseCoopers (PWC). An introductory email from ASOIF was sent to the IF president, secretary general and medical chairperson containing explanatory instructions and access information to the survey. An online survey format was chosen to provide a user-friendly interface that ensured data accuracy and to allow the respondents the flexibility to complete the questionnaire at their own pace. The online platform also enabled multiple users within an IF to complete the questionnaire and facilitated efficiency in the management of the survey process. Confidentiality of the data was maintained through the use of a password-protected access link and data storage system created by PWC. The study was conducted during a 6-week period from March to April 2016. Email prompts to encourage participation were sent as required.
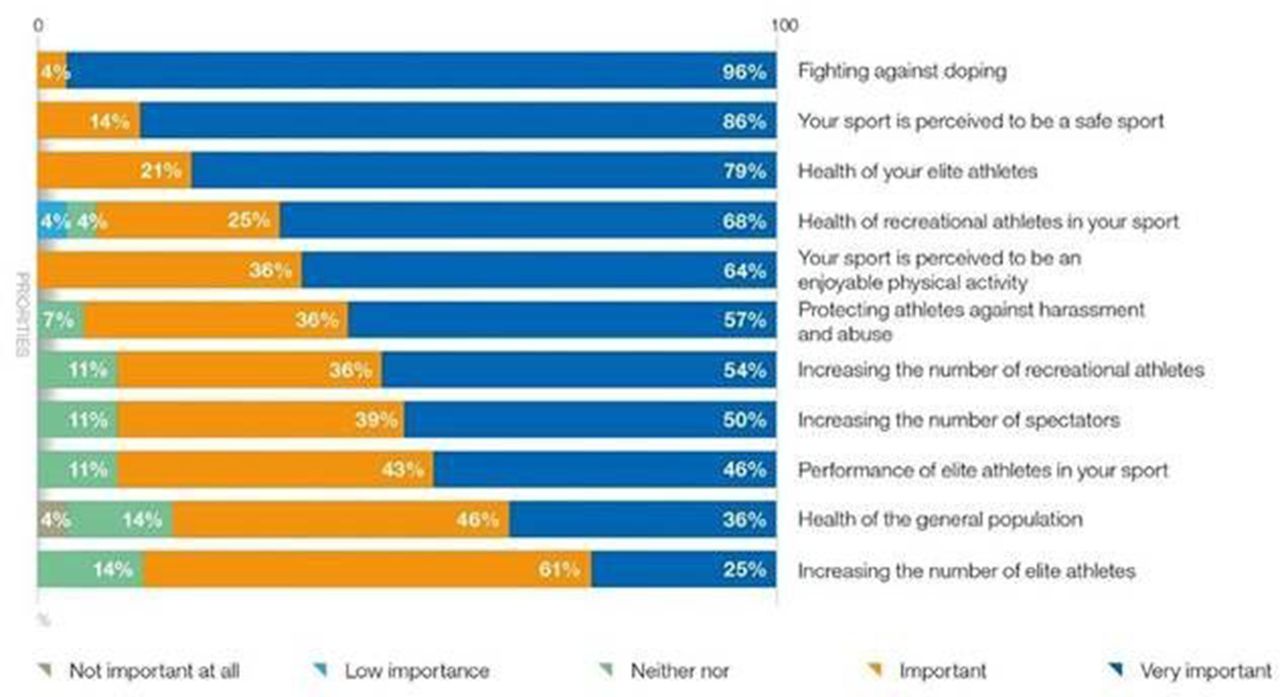
Following an introduction, demographic data were recorded to ensure respondent authenticity and to facilitate corroboration of the data as needed. The content of the survey was based on a survey conducted in 2012 by Mountjoy and Junge to facilitate a comparison of IF priorities and programming over time.11 The survey was composed of two parts: the first part asked the IFs to report the importance of 11 health-related topics on a f5-point Likert scale and to rank three of those topics in priority of importance (figure 1). The second part of the survey asked the IFs to identify programmes, guidelines or research activities in 27 health-related topics (figure 2). The complete survey can be found in appendix 1 (online version). The details of IFs were obtained from their official web-based home pages as well as the olympic.org website. Contingency tables were created for match-paired IFs (2012 and 2016 responses). The McNemar’s test for paired nominal data was used to test for statistical significance. Significance was accepted at p<0.05. All analyses were performed using SAS V.9.3 for Windows.
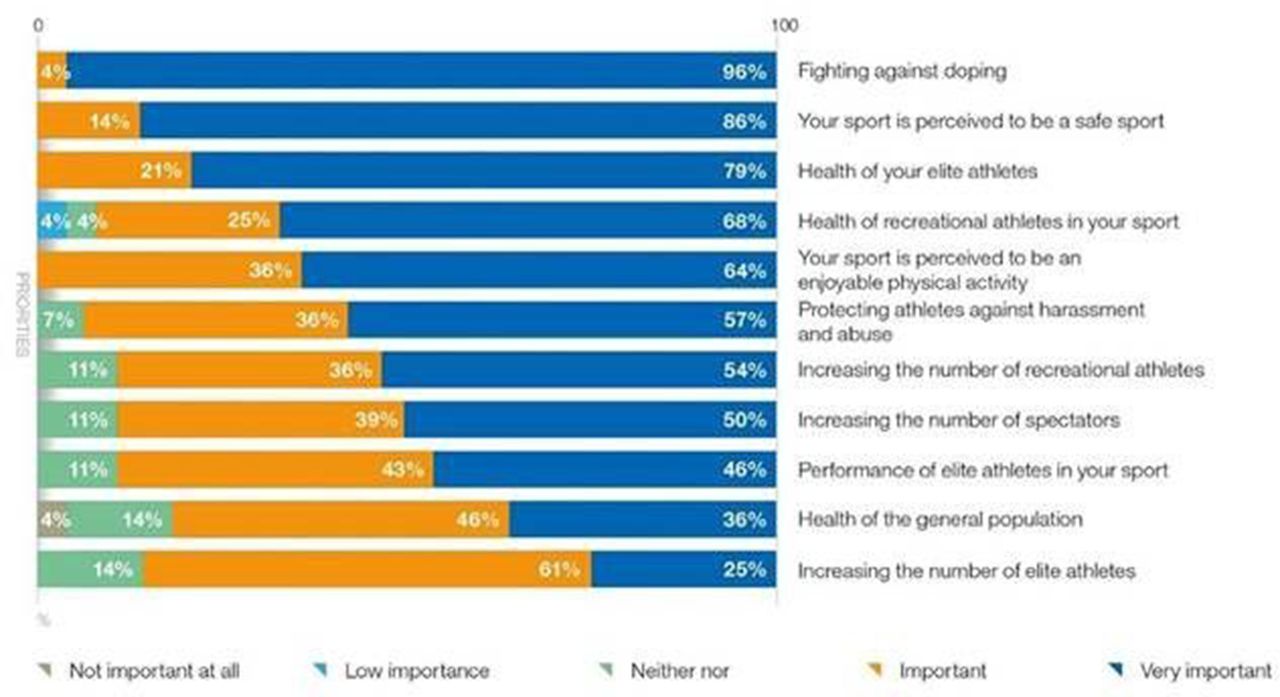
Importance of health priorities for the international sports federations.

Percentage of international sports federation health-related programmes, guidelines or research activities.
Characteristics of international sports federations (IFs) participating in the Olympic Games (OG) in 2016
Results
Response rate and characteristics of the IFs
The characteristics of the 28 participating summer IFs are illustrated in table 1. The IFs range in size from 110 member national federations (Union Internationale de Pentathlon Moderne) to 222 (International Table Tennis Federation). Over 500 athletes participated in each of five IFs’ sports (International Association of Athletics Federation (IAAF), FINA, World Rowing—Federation Internationale des Societes D’Aviron, Union Cycliste Internationale and FIFA) at the Olympic Games in 2016, totalling 47% of the athlete participation. The most recently added sports to the Summer Olympic Games programme are World Rugby (WR) and Golf (IGF), which reappeared in the Olympic Sport Program in Rio de Janeiro in 2016. Six IFs represent team sports, and 21 IFs are individual sports; one IF (FINA) has both individual and team sport athletes. All 28 summer IFs responded to the survey indicating a response rate of 100%.
Health priorities of the IFs
The IFs’ ratings of the perceived importance of the 11 health-related topics can be found in figure 1. While 96% of IFs identified the ‘fight against doping’ as the highest priority, in the overall ranking, it was ranked second in perceived importance behind ‘your sport is perceived to be a safe sport’. The third-ranked topic was ‘the health of your elite athletes’. The three lowest priorities of the IFs were ‘increasing the number of elite athletes’, ‘health of the general population’ and ‘performance of elite athletes in your sport’. ‘Protecting athletes against harassment and abuse’ was identified by one IF as their third-ranking priority.
IF ranking of identified health priorities
IFs health-related programmes/guidelines/research activities
Figure 2 demonstrates the IF programmes, guidelines or research activities of various health-related topics. Only one IF stated that it has no health-related programmes/guidelines/research activities. The most common health-related activities were ‘injury prevention by regulation for equipment/venues’ and ‘first aid/minimum safety standards at events’, each of which was reported by 93% of IFs. These were closely followed by ‘injury surveillance during IF championships’ (85%) and ‘implementation of the Olympic Movement Medical Code’ (70%). The least common activities of the IFs were ‘technology based health risks’ (15%), ‘prevention of chronic disease in the general population’ (11%) and ‘relative energy deficiency in sport’ (7%).
The number of activities reported by each IF ranged between 2 and 23, with most IFs identifying a total of 11 activities. Two IFs stated that they conducted ‘other activities’, but only one IF recorded the activity, which was ‘education of team staff’. One of the least common activities was ‘prevention of chronic disease in the general population’, which was specified by only two IFs.
A comparison of IF health priorities and activities since 2012
An analysis was completed to determine changes in IF health-related priorities and activities since 2012 in comparison with a similar study conducted by Mountjoy and Junge.11 There was a decrease in priority of the following four non-elite athlete health-related topics: ‘image as an enjoyable physical activity’, ‘health of recreational athletes in your sport’, ‘increasing the number of recreational athletes’ and ‘increasing the number of spectators’. The only parameter, however, that showed a statistically significant decrease was the ‘health of the general population’ (p≤0.01).
In the 2016 survey, 12 new health-related topics were added to part 2 of the questionnaire addressing IF programmes, guidelines and research activities in comparison to the 2012 survey. Only two of these topics (‘implementation of the Olympic Movement Medical Code’ and ‘nutritional supplementation use’) were implemented by more than 50% of the IFs. ‘Relative Energy Deficiency in Sport (RED-S)’ and ‘technology based health risks’ were the two health-related topics with the lowest activity of the IFs (see table 3).
Number and percentage of international sports federations (IFs) with newly added IF health-related programmes, guidelines or research activities
Figure 3 demonstrates the changes in IF health-related programmes, guidelines and/or research activities between 2012 and 2016. There is a positive trend or increase in IF athlete health-related activities such as ‘first aid/minimum safety standards at events’, ‘return to play after injury’ and ‘post elite-career management’. Conversely, there were fewer programmes in ‘injury prevention by exercise programs’, ‘prevention of chronic disease in general population’ and ‘injury prevention by Fair Play campaigns’.

{kind=link}
{kind=link}
{kind=link}
The percentage change in the number of IF with health-related programmes, guidelines and/or research activities from 2012 to 2016. IF, international sports federation.
Discussion
Study limitations
This study was intentionally designed to target Summer Olympic IFs, thus the results and their implications are limited to this cohort. Inclusion of both Winter Olympic IFs and non-Olympic IFs would provide a broader understanding of IF health-related priorities and activities. Inherent in survey methodology is the risk of self-report bias. In addition, this study did not evaluate the quality of the reported activities/programmes and the reasons for any changes in those activities/programmes since 2012 as this analysis was outside the scope of the study.
Elite athlete health protection
As in 2012, most IFs were active in the area of elite athlete health protection. The ‘fight against doping’ was the highest priority for IFs, which is not unexpected as being a signatory to the World Anti-Doping Code is a prerequisite for participation in the Olympic Games. The IFs also reported high activity in several elite athlete-related topics such as ‘injury prevention by regulation’, ‘first aid/minimum standards at events’ and ‘injury surveillance during events’. The trend analysis over time demonstrates that IFs have increased programming for their elite athletes since 2012 in the areas of ‘first aid’, ‘return to play after injury’ and ‘post elite career management’. These findings demonstrate that Summer Olympic IFs understand and take action in relation to their responsibility to protect athlete health.2
However, despite this improvement in elite athlete health programming, the comparison of IF activity between 2012 and 2016 reveals a decrease in elite athlete health-related programmes relating to ‘elite athlete mental health’, ‘injury surveillance at IF events’, ‘environmental conditions’, ‘nutrition/hydration’ and ‘injury prevention by Fair Play campaigns’. This shows that IFs could be doing more to protect elite athlete health. The need for (as an example) mental healthcare is demonstrated by a recent prospective study by Gouttebarge et al in football, which reported a prevalence of 12% for symptoms of mental distress and 37% for anxiety and/or depression.12 Other important elite athlete health-related topics that have been identified in the scientific literature as important parameters in elite athlete health that are identified in this study as being of low priority for IFs include ‘eating disorders’13, ‘protection from harassment and abuse’14 and ‘Relative Energy Deficiency in Sport (RED-S)’15. Furthermore, although 24 IFs reported that they undertook programmes in ‘injury surveillance during IF championships’, only six IFs have published their results (IAAF,16 FINA,17 FIFA,18 WR,19 International Handball Federation,20 Federation International de Volleyball21 and despite 19 IFs reporting ‘pre-participation medical examinations’, only one IF published their activity (FIFA).22
Promotion of sport for the improvement of global health
‘Health of the general population’ was identified as the second lowest priority for the IFs, and only three IFs identified activities directed towards ‘Prevention of chronic diseases in the general population’. Of these three IFs, only two IFs have programmes that address the public health crisis of NCDs caused by physical inactivity: F-MARC’s 11 for Health23 24 and FINA’s Swimming for All-Swimming for Life.25 F-MARC’s 11 for Health programme pairs football-based activities with health initiatives addressing PA promotion and education about healthy behaviours related to both communicable and non-communicable diseases. This programme has been successfully implemented around the world to school-aged children.23 24 FINA’s Swimming for All-Swimming for Life programme has a dual benefit in that it has the potential to save lives through drowning prevention and to improve the quality and quantity of life through the promotion of PA and the subsequent reduction of NCDs. A learn-to-swim programme has been developed and is being implemented globally in collaboration with Unesco in all five FINA member continental federations.25
One finding in this study that is of particular concern is the statistically significant decrease in IF priority in ‘health of general population’ between 2012 and 2016, particularly in light of the recommendation of the 2012 study on IF health activities by Mountjoy and Junge that ‘International Federations should use the unique chance to contribute to the health of the general population by the promotion of physical activity through their sport’.11 It appears that the recommendation has not been heeded. IFs have an obligation to develop ‘sport for all’, as mandated through the IOC Consensus Statement on the Fitness and Health of Young People,7 by Recommendation #51 of the Olympic Movement in Society Congress held in Copenhagen, 200926 and more recently by the IOC President, Mr Thomas Bach, in the introduction to the Olympic Agenda 202027:
[The Olympic Movement] has an interest and a responsibility to get the couch potatoes off the couch. Only children playing sport can be future athletes. Only children playing sport can enjoy the educational and health values of sport.
Furthermore, ‘increasing the number of recreational athletes’ was of low importance for the IFs (ranking 9 out of 12). This is a surprising finding, as the sustainability of a sport is dependent on the number of participants. Increasing the number of recreational athletes would also benefit global health through the promotion of PA to this section of the population.
Call to action
According to the WHO, NCDs cause approximately 38 million deaths annually, mainly in low-income and middle-income countries; over 40% of these deaths (16 million) occur before the age of 70 years. Physical inactivity alone is responsible for around 3.2 million deaths per year.6 28 PA has the power to reduce these numbers through its many health benefits, such as the reduction of prevalence of cardiovascular disease, cancers of the colon and breast, chronic respiratory diseases, diabetes, depression, obesity and osteoporosis with subsequent fractures of the hip and vertebral column.6 Despite the ethical responsibility and the integral role that sport has in relation to the promotion of PA for the health of the general population, the fact that IFs have decreased their priorities and programming in this area is concerning. In response to this result, the ASOIF Medical and Scientific Consultative Group developed a strategy to stimulate a change in knowledge and behaviour of the IFs and to inspire and motivate the political leadership of the IFs to action.
In November 2016, ASOIF, in collaboration with Sport Accord Convention, held an IF Forum in Lausanne Switzerland, entitled ‘The Power of Sport to Drive World Health’. The attendees included presidents, secretary generals and medical commission chairpersons of the IFs from ASOIF, Association of International Olympic Winter Federations, Association of IOC Recognised International Sport Federation and Alliance of Independent Recognised Members of Sport. In total, there were 324 participants. The first part of the programme addressed ‘Safe Sport’, which focused on the improvement of elite athlete health, highlighting areas identified in this study that were reported as low priority by the IFs, such as athlete mental health, protection from harassment and abuse, Fair Play programmes and rule changes based on sport-specific science. The second part of the programme addressed ‘Sport for Health’ outlining the science on the health risks of physical inactivity along with the role of sport in mitigating these risks. A workshop followed these plenary sessions in which the participants identified potential solutions to collectively address the global health crisis. An action plan to promote sport as a tool to increase PA with the goal of creating a positive, long-lasting legacy through the improvement of global health was developed. This action plan comprises three steps, and is in compliance with the Olympic Agenda 2020 initiative through the implementation of strategies to enhance accessibility of sport for all.
Action plan for IF promotion of global health
Planning
Develop partnerships with
other IFs
governments: education, health, infrastructure (sport facilities)
non-governmental organisations
WHO/Unesco/Unicef
media
industry/business
Adaptation of the IF sports for various ages, physical abilities and cultures
Adoption and adaption of existing programmes
Implementation
raise awareness through education programmes
development of an event legacy programme to engage physical activity in host cities
engage national federations in dissemination and implementation
provision of sport equipment
dissemination in schools, public places, communities in crisis
promotional strategy through
social media
athlete role models
major event signage
partnerships with broadcasting
programme branding
Evaluation
monitor and evaluate programme uptake, sustainability and efficacy of health benefits.
The IF Forum concluded with a ‘Declaration’ identifying their commitment and intention:
Global health initiative through sport:
We, the International Federations, recognise and acknowledge our responsibility to promote health; for our athletes and for the global population.
Through collaborative action, and partnerships with non-sport entities, we will develop, implement and evaluate the effectiveness of programs to promote health through the Power of Sport.
Conclusion
While it is encouraging to see the increase in IFs’ prioritisation of some aspects of the health of the elite athlete, focus should be given to all aspects of protection and promotion of athlete health both during and after retirement from sport. A more robust and comprehensive athlete health programme would ultimately result in longer athlete retention (eg, through reduced attrition due to injury) and improvement in sport performance.
The IFs did not identify recreational athlete health as a priority. Attention to this large group of individuals worldwide would benefit sport through the increase in healthy participating athletes as well as the fan base and sport market.
IFs have an obligation to develop and promote sport for all and are in a unique position to positively influence global health through the promotion of their sport to counteract the epidemic of physical inactivity and subsequent reduction in the prevalence of NCDs. The barriers to IF promotion of health in both the elite athlete and global populations should be identified, and effective solutions should be developed to deliver IF programmes that improve both athlete and global health. With vision and intent, funding and partnership, sport can have a positive impact on the global epidemic of NCDs through the promotion of PA.
What are the findings?
International sport federations (IFs) are aware of and are actively working to protect many aspects of elite athlete health. However, IFs are not addressing several important components of athlete health.
Despite the knowledge of the importance of physical activity in the promotion of global health, and the IFs’ responsibility to encourage and promote sport for all, the IFs’ priority and programming in this area has significantly decreased since 2012.
IFs have committed through a joint Declaration and Action Plan to address their role in the promotion of physical activity to improve global health through sport.
How might it impact on clinical practice in the future?
International Sport Federations will commence programing in areas of athlete health not being addressed.
International Sport Federatoins will develop research programs to develop evidence based information to better inform rule changes for athlete safety.
International Sport Federations will recognize their role in promoting global health, and will develop programs accordingly.
Acknowledgments
The authors appreciate the cooperation of the IFs and their medical representatives who responded to the survey providing the data for this project. We also gratefully acknowledge the assistance of ASOIF in the implementation of the survey and the invited guest speakers who shared their expertise at the IF Forum in Lausanne, November 2016.
’The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd and its Licensees to permit this article (if accepted) to be published in Journal (British Journal of Sports Medicine) editions and any other BMJPGL products to exploit all subsidiary rights, as set out in our licence (http://bjsm.bmjjournals.com/misc/ifora/licenceform.shtml).
References
Footnotes
Twitter @margo.mountjoy @asoif
Contributors MM: first author, substantial contributions to conception and design, data collection, interpretation of results, drafting and revising the manuscript and final version to be published. AC: second author, analysis and interpretation of data, drafting and revising the manuscript and final approval of the version to be published. RB, JD, LE, SM and JM: substantial contributions to implementation, revising the manuscript and approval of final version to be published.
Funding ASOIF provided assistance with the survey implementation through the support of PWC.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There is no unpublished data from the study.