Article Text

Abstract
Objectives We describe the medical services provided and report the injuries and illnesses that occurred at the eighth Asian Winter Games 2017.
Methods A total of 2010 athletes and team officials from 32 National Olympic Committees and 2 guest countries attended this event; medical services were provided for 16 days. Medical data (medical care and physiotherapy) were collected for the same period by the organising committee for athletes and non-athletes (team officials, workforce, media and spectators) and recorded on the electronic medical record system at the medical rooms in the venues and the team residences.
Results We recorded 745 medical encounters (medical care, 443; physiotherapy, 302), of which 549 (74%) were among athletes. There were 214 injuries as well as 144 illnesses and other medical conditions. Of the 1164 athletes, 549 (47%) utilised the services. Ice hockey, snowboarding and alpine skiing had high rate of medical encounters. More than half of the delegations were not accompanied by team doctor, and rate of medical encounters was high in these teams. The vast majority of patients transferred to hospital for further care were mostly athletes (n=36 out of 41), mostly alpine skiers and ice hockey players.
Conclusion Injuries and illnesses varied depending on NOC medical staffing and sport events. These data will serve organisers of medical and physiotherapy services in the Asian Winter Games and similar large events.
- sports injury
- medical service
- epidemiology
- surveillance
- illness
Statistics from Altmetric.com
What are the findings?
This is the first report detailing the medical services and injuries and illnesses reported in the Asian Winter Games.
Among the 2010 athletes and team officials, there were 214 injuries and 144 illnesses during the games.
47% of athletes utilised the services of the medical care and physiotherapy.
41 patients were transferred to hospital; the sports most represented were alpine skiers and then ice hockey players.
How might it impact on clinical practice in the future?
We identify of high-risk disciplines among winter sports events.
As more than half of the participating countries were not accompanied by team doctors, and these National Olympic Committees utilised the medical services to a large degree, these data help facilitation in organising effective medical and physiotherapy services in future big sports events.
Introduction
The Asian Games are organised by the Olympic Council of Asia (OCA), which has 45 National Olympic Committees (NOC). As its affiliates, apart from its flagship quadrennial Asian Games, the OCA also provides for a Youth Games, an Indoor and Martial Arts Games, Beach Games and the Winter Games. The concept of the Asian Winter Games (AWG) was initiated in 1984 to promote and develop winter sports and facilitate its development and improving the related skills in Asia. The first AWG was held in Sapporo in 1986, which also hosted the AWG in 1990 and the Winter Olympic Games in 1972.
Since its inception, the number of participants in the AWG has been increasing. The AWG is a unique international sports event where athletes from various countries participate including even those with tropical climates with no winters. Hence, the level of all athletes’ sports skills varies in the AWG, compared with other international competitions such as the Olympic Games or the world championships. Also, not all NOCs are accompanied by their medical staffs.
In general, injuries reported in winter sports are categorised by injury mechanism, location, type, incidence and severity.1–3 Winter sports pose a potential risk of severe trauma causing permanent disorders or death because of high-energy injury mechanisms as well as being open to specific medical conditions associated with cold climates. The eighth AWG Organising Committee (SAWGOC) established medical and first-aid centres at venues to provide medical services to athletes, other games personnel and spectators. This was done in compliance with the Olympic Council of Asia’s Guidelines for Medical Services and under the supervision of its Medical and Anti-Doping Commission.4 This study aimed to describe medical services provided by the 2017 AWG and report injuries and illnesses occurred therein. To the best of our knowledge, this is the first report that compiles data about medical issues encountered in the AWGs.
Methods
Participants and sports events
The eighth AWG was held from 19 to 26 February 2017 in Sapporo and Obihiro (speed skating), Japan. A total of 2010 athletes and team officials from various countries participated in the AWG. These represented 32 NOCs, including guest teams from Australia and New Zealand. Overall, 1164 athletes participated in 11 sports disciplines and 64 events held at 12 venues. The 11 disciplines were as follows: Alpine skiing, cross-country skiing, ski jumping, freestyle skiing, snowboard (skiing), speed skating, short track speed skating, figure skating, biathlon, ice hockey and curling. Out of the 32 participating NOCs and guest teams, a total of 15 NOCs were accompanied by their team doctors to the AWG.
Medical committee and antidoping commission
The members of the Local Organising Committee’s Medical Committee comprised medical representatives of the Japanese Olympic Committee, Japan Anti-Doping Agency, National Sports Federations and a local medical university which served as the central facility providing medical services to the event. The medical committee and SAWGOC Medical and Sanitary Affairs Section together with the OCA Medical Committee planned and established the medical services programme.
Medical services and EMR
As medical services were provided for 16 days (from 12 to 27 February 2017), medical statistics were collected for the same period. This period commenced with the opening of the athlete village and ended 2 days after the closing ceremony.
In this study, we obtained medical records related to daily medical treatment and smooth transfer to designated hospitals by using the electronic medical record (EMR; Fuji Xerox Co, Ltd, Japan) system. As computers preinstalled with the EMR system were set up at each medical room of the venues, the medical head office could refer and collect medical data immediately using the Cloud storage. The EMR system facilitated organising all medical details, which helped medical personnel to follow-up an encounter at the medical rooms.
Designated hospitals and medical rooms
In both host and co-host cities of the event, 37 designated hospitals and dental clinics were selected based on the number of medical services and geographical advantage. In particular, three large general hospitals, including a university hospital, a city general hospital and a private general hospital, were prepared to receive emergency cases and severe injuries and illnesses. The medical treatment in the designated hospitals and onsite medical treatment centres was provided free of charge during the event for accreditation card holders, known collectively as ‘the games family’.
Furthermore, medical rooms were prepared at each athlete village hotel, headquarter hotel, main media centre, competition venue and the opening and closing ceremony venue. We allocated physicians at the medical rooms in those official hotels, orthopaedic surgeons at the venue medical rooms and emergency physicians at the opening and closing ceremony venue medical rooms. At the medical rooms, we prepared an emergency kit including an automated external defibrillator (AED) and basic medicines or equipment for injuries and illnesses. Doctors at the medical rooms examined patients and prescribed drugs or applied splints when needed. A dentist and a physiotherapist were allocated in addition to a doctor and a nurse at the medical rooms of the ice hockey venues. While non-urgent patients were treated at the medical rooms, a direct transportation service was provided for emergency patients. When further examination was needed such as image examination or blood test, patients were transferred to the designated hospitals. Before the games, workshops were held for medical personnel to explain the medical system and process of medical cares including treatment in emergencies at the venues. The total number of registered medical staffs was 707 for the medical rooms and the venues. The details of the medical staffs are shown in table 1.
Numbers of staff for the medical rooms and the venues
Medical command centre
Medical Command Center organised medical issues during the games. This Center consisted of the members of the medical committee, SAWGOC Medical and Sanitary Affairs Section and the OCA Medical Committee. The main role of the Command Centre was to check the condition of all the medical rooms. The Center also dealt with issues arose from games facilities. Moreover, when the transfer was required with a patient, it was immediately reported to the Command Center by the administrator in the medical rooms. In each of these situations, a member from the Command Center went to the designated hospital to take over following duties.
Physiotherapy and athletic training
The physiotherapy service was arranged in three medical rooms at athlete hotels and six competition venue medical rooms for ice hockey, Alpine skiing, freestyle skiing and figure skating. The forms of physiotherapy provided were as follows: exercises, stretching, mobilisation, therapeutic massage, cold therapy, heat therapy, electrotherapy, ultrasound, laser and taping. In addition, athletic training rooms in a gymnasium were created in the central athlete hotel area to support conditioning and maintenance issues; this athletic training room was operated by an athletic trainer in cooperation with a physiotherapist.
Data analysis
Medical staffs
Cumulative total number of participated staffs was summarised by category.
Medical encounters
All medical encounters (medical care and physiotherapy) treated in our medical rooms were recorded on the EMR system. Distribution of medical encounters was analysed by date and accreditation category: including NOC (athletes and team officials), media, spectators and others. The category ‘others’ included OCA family, volunteers and SAWGOC staffs. The data of patients were also summarised by injuries and illnesses or facilities (athlete village hotels, competition venues and non-competition venues). Non-competition venues included the headquarter hotel, the main media centre and the opening and closing ceremony venues. Patients transferred to hospitals for further care were sorted by category and sport. Medical encounters of athletes were separately summarised. They were sorted by NOC size (over or below 100 participating athletes) and NOC with or without team doctors.
Physiotherapy and athletic training visitors were summarised by athletes or non-athletes, facilities or prescriptions. The physiotherapy prescriptions were divided into three categories; exercise and manual procedure (exercises, stretching, mobilisation, therapeutic massage), modalities (cold therapy, heat therapy, electrotherapy, ultrasound, laser) and taping. Athletes used the training room with or without the support services of our athletic trainers.
Medical encounters of athletes were farther analysed. They were divided according to their NOCs with or without their team doctor. The casualty rates by sport were calculated.
Results
Medical staffs
A total of 1550 medical staffs participated in this event for the medical rooms and the venues. The details of the participated staffs are shown in table 1.
Distribution of medical encounters
The event recorded 745 encounters (medical care, 443; physiotherapy, 302) visits.
Figure 1 shows the daily distribution of medical encounters during the 16 days of the medical services provided. Competitions started on day 8 and ended on day 15. A peak of the medical encounters recorded occurred on day 9 and high numbers of encounters could be entered until day 14.
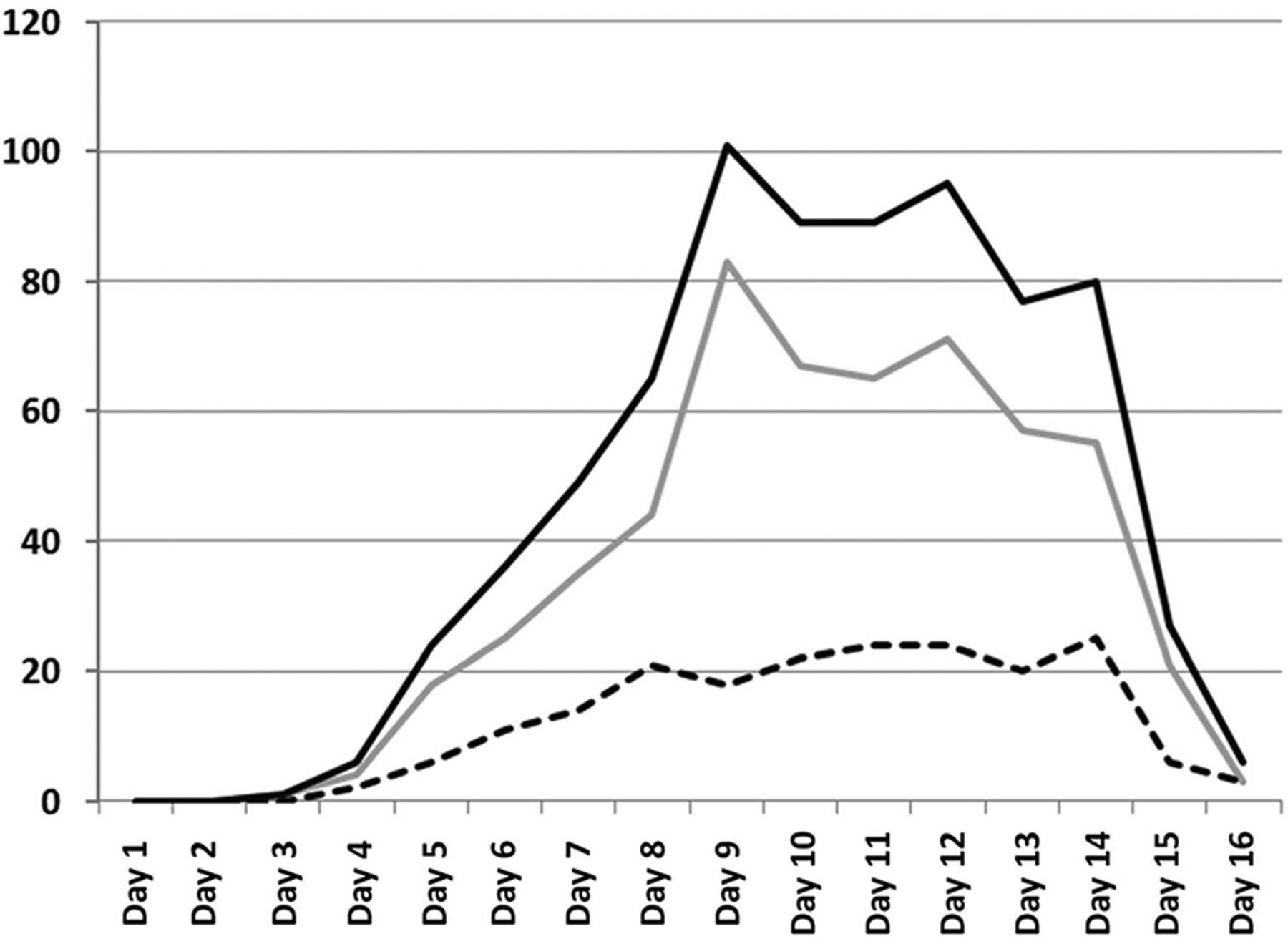
Daily distribution of medical encounters. Grey line, athletes; dotted line, non-athletes; black line, total number.
Distributed by accreditation category, athletes formed the largest group, accounting for 73.7% (549 out of 745 medical encounters), followed by team officials at 12.5% (93), media 0.3% (2), spectators at 1.9% (14) and others at 11.3% (87).
Medical care, physiotherapy and athletic training
The number of visits encountered for medical care was 443, of which athletes constituted 295 encounters (67%). The most common reason for seeking medical care during the AWG was injuries (214), followed by illnesses (144) and others (85). The body part most featured among the number of injuries was lower extremity (table 2). The summarised data of patients by facilities is shown in table 3. A total of 589 medical encounters (medical care, 309; physiotherapy, 280) were recorded at the medical rooms in the athlete village hotels.
Number of encounters for medical care by injury, illness and their category
Number of encounters for medical care treated in the medical rooms according to facilities
The summarised number of physiotherapy and athletic training visitors by athletes or non-athletes and facilities is shown in table 4. The number of people visiting physiotherapists and the training room was 302 and 1148, respectively. The number of physiotherapy prescriptions was as follows: 251 of exercise and manual procedure, 218 of modalities and 90 of taping.
Number of physiotherapy and athletic training encounters
Hospital transferred encounters
The number of patients transferred to hospitals for further care was 41 (athletes, 36; OCA families, 3; team official, 1; other, 1). The rate of transferred patients was 9% (41 of 443 medical cares). Of note, one team official was hospitalised for a brief period. The event reported no case of surgery, severe infectious diseases or death.
Medical encounters of athletes
During the event 549 athletes utilised the services (medical care, 295; physiotherapy, 254) (table 5). This was the cumulative total number, and when this number was divided by the total number of the participated athletes (1164), it was 47.2%. NOCs with a size of over 100 participating athletes exhibited a lower ratio (number of medical encounters/number of athletes) compared with smaller size NOCs. Among the 15 NOCs having own team doctors to take care of 913 athletes in total, the number of medical encounters was 314, which generated a rate of 34.4%, much lower than the comparable rate of 93.6% for those NOCs without having own doctors (table 5).
Distribution of athlete medical encounters between NOC with/without team doctor
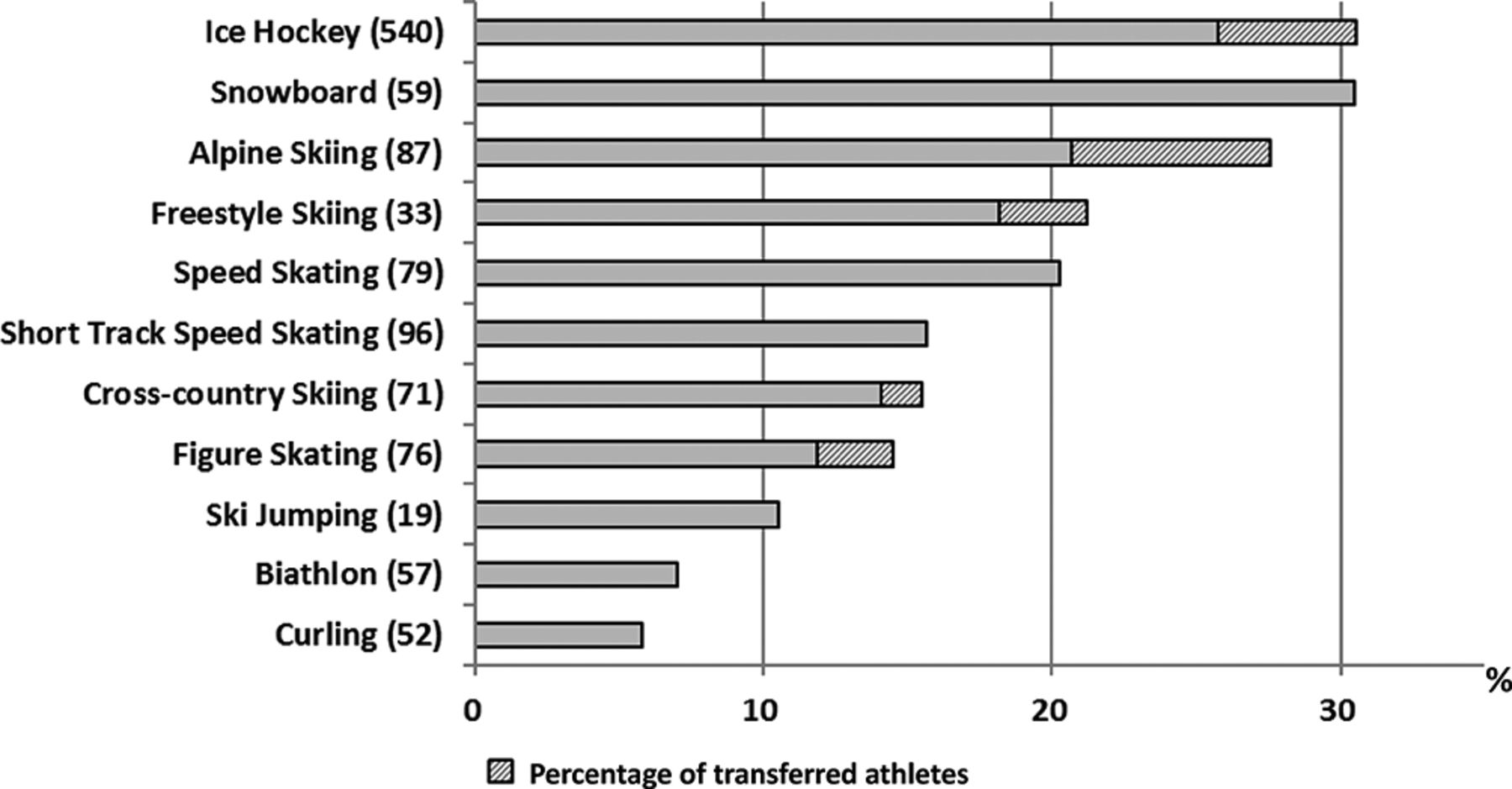
Medical encounters (injury and illness) by sport discipline are shown in figure 2. Of the 540 ice hockey athletes, 165 (30.6%) visited our medical rooms. Snowboard and alpine skiing athletes also showed a high proportion of attendance (30.5% and 27.6%, respectively). A total number of 36 athletes from ice hockey (n=26), alpine skiing (n=6), freestyle skiing (n=1), cross-country skiing (n=1) and figure skating (n=2) were transferred to hospitals for further care. The main reason for athlete referrals to hospital was trauma including contusion, joint sprain, fracture and two cases of concussion. Two cases were except trauma, one was acute gastroenteritis and another was vertigo.
{kind=link}
{kind=link}
Medical encounters (injury and illness) and transferred to referral hospitals by sport discipline. Number of participants is shown within parenthesis (note: five athletes entered two events).
Discussion
To the best of our knowledge, this is the first report detailing the medical services and injuries and illnesses reported in the AWGs. The 2017 Sapporo Asian Winter Games hosted 2010 participants from 32 countries and 2 guest countries, and >1500 (cumulative number) medical staff members worked for this event to provide best medical service for the participants and their accompanied staff, including media and spectators. The SAWGOC diligently established a large number of medical and first-aid facilities and designated local medical institutions as referral hospitals to provide medical and first-aid services to all participants and spectators in the event.
Injuries and illnesses in international winter sports events and medical demands in the AWG
Lately, some international sporting events have reported the statistics concerning injury and illness during the event. For instance, the Vancouver 2010 Winter Olympic Games5 reported 287 injuries and 185 illnesses among 2567 athletes from 82 NOCs. The incidence rate of medical issues was 11.2 injuries and 7.2 illnesses per 100 registered athletes. In addition, the Sochi 2014 Winter Olympic Games hosted 2780 athletes from 88 NOCs over an 18 day event,6 and reported 391 injuries and 249 illnesses, with an incidence rate of 14 injuries and 8.9 illnesses per 100 athletes. Of note, these data were not entirely comparable with our study (15.5 injuries and 6.8 illnesses per 100 registered athletes when expressed in the same way as the previous studies). In the Olympic Games, IOC medical commission asked NOCs’ head physicians to daily report the occurrence of newly sustained injuries and illnesses on a standardised reporting form. In this study, we did not include cases treated by only NOC doctors. Hence, the actual number of injuries and illnesses could have been higher in the Sapporo AWG.
As described earlier, the AWG is a unique sports event because of the diversity of athletes that participate in the same event. More than half of the NOCs participated in this event without an accompanied team doctor. The rate of medical encounters was high in these groups, and the number of encounters was also negatively related to NOC size.
Furthermore, AWG’s physiotherapy services focused on injury treatment and rehabilitation and supporting athletes’ performance. We had a large number of patients needing physical therapy during the event, likely because not all NOCs were accompanied by their physiotherapists or athletic trainers. This fact underlines the need and demands on a well-functioning physiotherapy service in the AWG.
Severe and transfer cases in winter sports events
One of the crucial missions of medical services in sports events is to establish transportation and treatment system for severe cases. The reported rates of transportation to a hospital by an ambulance in the Winter Olympic Games were 1.5% in the Calgary 1998, 3.2% in the Salt Lake City 2002 and 2.8% in the Torino 2006.7–9 In the Sapporo AWG, the rate of transferred patients was 9.3%. The highest rate of transferred athletes was alpine skiers, followed by ice hockey players. The medical emergency system covered these disciplines and could thereby treat all the transferred athletes appropriately. The risk of injuries varied among sports events, and these data might be useful when preparing medical services and systems for emergency cases.
Conclusion
Athletes and team officials formed the largest group for medical encounters recorded. More than half of the participating countries were not accompanied by team doctors, and these NOCs utilised the medical services to a large degree. Injuries and illnesses varied depending on NOC medical staffing and sport events. We recommend to further compiling data on medical care and service in the AWG to better facilitate the organising of medical and physiotherapy services in the AWG and similar large events.
Acknowledgments
The authors thank the OCA Medical Committee and Anti-Doping Commission for its guidance, support and supervision during the preparatory phase as well as the competition period. A special appreciation to the following members who were in Sapporo at Games Time: Dr Jegathesan (chairman), Ms NaS, Dr Mohammad Razi, Dr Sultan Al Busaidi, Dr Xie Minhao, Dr Young Soo JIN, Ms Yuan Hong, Dr Kamal Al Hadidi, Dr Aminath Noordin, Ms Juliet Quisiquisi and Dr Makato Ueki. They also would like to thank the Olympic Council of Asia (OCA) for its kind permission to use the data collected and to publish this paper.
Footnotes
Contributors KW and TA: gathered the data. SA, KF, HS, TO, TI, HS and MK: analysed the data. KW and MK: wrote the initial drafts. KW: revised the initial drafts. MJ and NS: revised the manuscript. TA, SA, KF, HS, TO, TI, HS and MK: ensure the accuracy of the data and the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval The design of this study was approved by the Olympic Council of Asia.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data for this study were obtained from the original data preserved in The 8th Asian Winter Games Organising Committee.