Article Text

Abstract
Objectives The risk of graft revision following ACL reconstruction may depend on the sport type the individuals are engaged in. The purpose of this study was to report the ACL graft revision rate in alpine skiers, football and handball players.
Materials and methods Primary ACL reconstructions and graft revision data from 2004 to December 2016 were obtained from the Norwegian Cruciate Ligament Registry. The graft survival rates were calculated for individuals in each of the three sport types, for bone patellar tendon bone (BPTB) and hamstring tendons (HT) grafts separately, and related to age at primary operation and sex.
Results A total of 711 grafts in 14 201 primary ACL reconstructions were revised (5.0%) after median 6 years, 3.8% in alpine skiers, 5.0% in soccer and 6.1% in handball players (p<0.001). Adjusted Cox regression showed similar ACL graft survival rates in the three groups. The HR for graft revision was 5 times higher for individuals aged ≤18 years than for those aged ≥35 years (p<0.001). The corresponding HR for graft type was 1.8 times higher for HT than for BPTB grafts (p<0.001), but 2.8 times higher for individuals aged ≤18 years (p<0.001). The 12 years survival of BPTB grafts was 96% compared with 93% for HT grafts (p <0.001).
Conclusion The revision rate for ACL grafts was similar among alpine skiers, football and handball players, and the results support the use of BPTB grafts in young athletes with closed growth zones in the knee.
Study design Cohort study; level of evidence, 2.
- acl reconstructions
- reoperations
- sex
- sport
Statistics from Altmetric.com
Introduction
The Norwegian Cruciate Ligament Registry (NCLR) was established in 2004 to identify the results of different surgical procedures, grafts and graft fixation devices.1 2 Registration rates are close to 90%.1 3 Rupture of the ACL is common in sport activities and in younger age groups, and it is usually surgically treated with ACL reconstruction using tendon grafts.4 The bone patellar tendon bone (BPTB) and hamstring tendons (HT) are the most commonly used grafts in Scandinavia.4 5 Most athletes return to their sport after ACL reconstruction, and many may injure the same knee again and sustain an ACL graft rupture or an ACL rupture of the contralateral knee.6 An ACL graft failure is a serious injury since the outcome of ACL revision surgery is inferior compared with that of primary ACL reconstruction.7 8 The risk of ACL graft tear has been reported to be much higher for young female football players compared with other female athletes of the same age group with 11% vs 1% graft failure after a mean follow-up of 5.7 years, but the other female athletes did not include handball players.9 High ACL graft failure rates for children and adolescents who return to sport (13% graft rupture after mean 6.5 years) have been reported in a systematic review and meta-analysis.10 In rugby players, the ACL graft failure was 16% after a 5-year follow-up period.11 The risk of ACL graft tear may be associated with the type of activity the athletes are engaged in.4 Football, handball and alpine skiing are very popular sports in Norway, and a preliminary ACL registry study presented at the 16th ESSKA Congress in 2014 showed that the risk of revision for ACL graft failure was lower for those who had suffered their injury in alpine skiing which is an individual sport compared with those who had been injured in the team sports such as football and handball.12 The purpose of the present study was to extend the ACL registry study with four more years and adjust the data for age, sex, graft type and time periods to assess the absolute risk, and factors influencing ACL graft revision in the three sport types. The working hypothesis was that graft revision would be lower in alpine skiers than in football and handball players.
Methods
Study design
Data including primary ACL reconstructions and revisions with a secondary ACL reconstruction were obtained from NCLR including the period June 2004 when the registry was established through to December 2016. A total of 21 446 primary ACL reconstructions were recorded in the period. The largest number (66%) sustained their injury in football (39%), handball (14%) and alpine skiing (13%), and only these were included in the present study. The primary ACL reconstruction was performed with BPTB and HT grafts in 99% of the patients, and the distribution of the two grafts in the three sport groups were similar (table 1). Several graft fixation methods were used in the period, but they are not included in this study. The revisions defined as a secondary ACL reconstruction were calculated in per cent and as HRs for each of the three sports, for age at the primary operation and sex, for BPTB and HT grafts separately and for time periods.
Demographics and crude data of alpine skiers, football and handball players at primary ACL reconstruction and at ACL graft revision. median with IQR (Q1–Q3)
Statistical analyses
The results are presented as mean, median, IQR (Q1–Q3), 95% CI and revision rates (percentage of secondary ACL reconstruction for various groups over time). Pearson’s χ2 test and Kruskal-Wallis test for independent samples were used to evaluate statistical differences in demographic data.
Kaplan-Meier survival analyses were performed with first ACL graft revision for any reason as end point. Information about deaths and emigrations were obtained from the National Population Register. The survival of the ACL grafts in patients who had died or emigrated without revision was censored at the date of death or emigration. All other patients were censored at the end of the study at 31 December 2016.
A Cox regression model was used to calculate the possible association between sport type and revision. HRs were represented with 95% CI and p values relative to alpine skiing, men, BPTB, age ≤18 years and the time period 2004–2007 as reference categories. Both unadjusted (crude) and adjusted multivariable Cox regression models were used. In the unadjusted analysis, the effect of sport categories were studied separately. Adjustment for potential confounding was performed. The model included the variables age, sex, type of graft and time period for the primary operation. We chose to use age as a categorical variable since its influence was not continuous. The stratification into age groups were performed to underline the fact that alpine skiers were older than football and handball players at the primary ACL reconstruction. The choice of year span was based on four groups with approximately the same number of operations in each group. The time periods were 2004–2007, 2008–2010, 2011–2013 and 2014–2016 with about the same amount of operations in each of the four periods. HT dominated the first three periods and BPTB the latter. The initial analysis of the proportional hazard assumption of the Cox regression model was by inspection of log-log plots. The proportional hazard assumption of the Cox regression model was assessed by inspection of Schoenfeld residuals and found reasonable. Variables known to be possible confounders based on previous studies were included in the Cox regression model. All tests were two-sided and the statistical significance level was set at 0.05. We found 5.2% bilateral procedures in our material (alpine skiing 3%, football 5.2% and handball 7.2%). Statistical analyses were performed using IBM SPSS Statistics, V.24 (IBM, Armonk, New York, USA) and R V.3.4.1 (The R Foundation, Vienna, Austria).
Results
Characteristics related to secondary ACL reconstruction
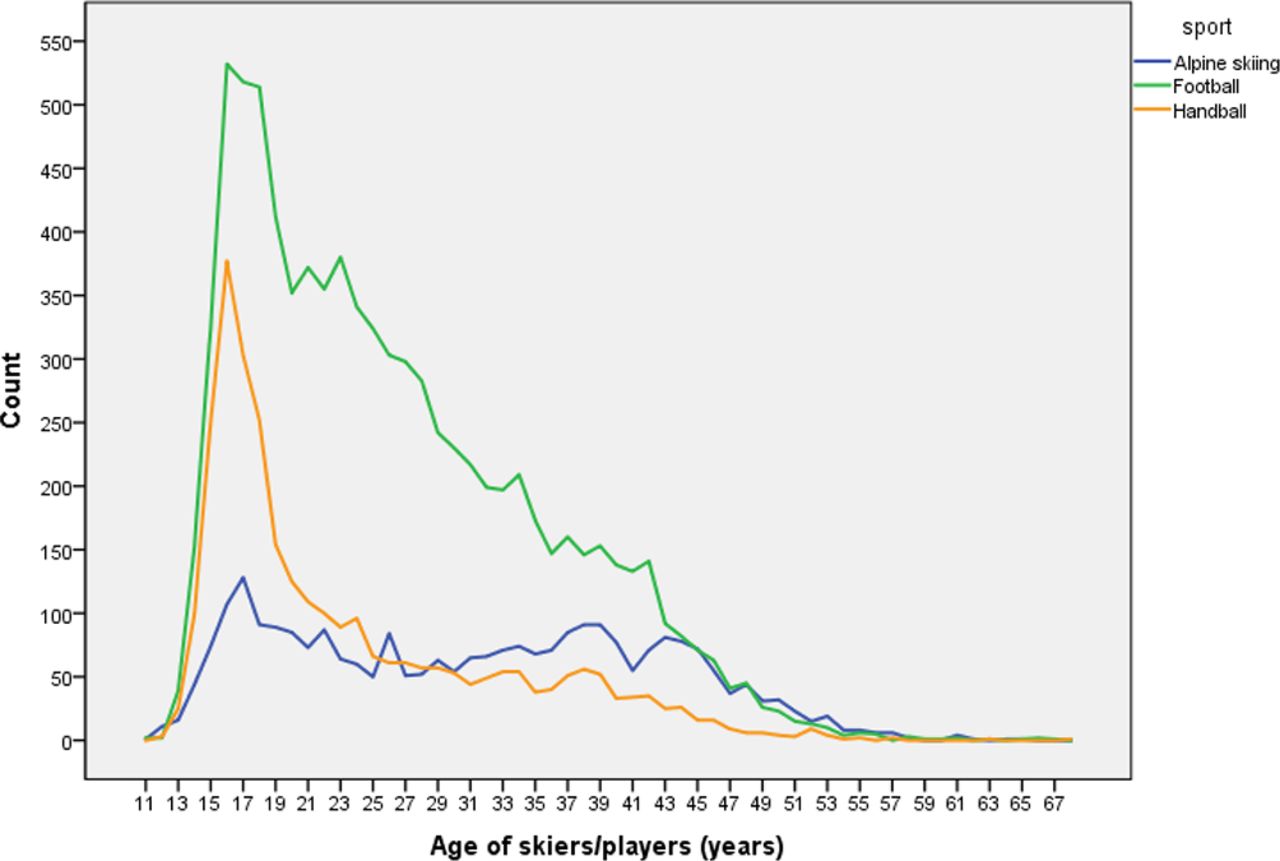
A total of 711 graft failures (5.0%) were revised with a secondary ACL reconstruction within the three sport categories. The crude graft revision rate was lower for alpine skiers than for football and handball players (p<0.001) (table 1). Almost half of the primary ACL reconstructions were performed in females, but the percentage of females was much higher among handball players than among football players and alpine skiers (p<0.001). The reverse was observed for football players (p<0.001) (table 1). Corresponding sex distribution was observed for ACL graft revisions (p<0.001) (table 1). A larger share of football and handball players was teenagers compared with alpine skiers (figure 1). The median age at revision was significantly lower than the median age at the primary ACL reconstruction in the three sports as a group (p<0.001). This was observed both for alpine skiers and football players, but not for handball players (table 1). About 16% of the graft revisions occurred within 1 year, and almost half (45%) within 2 years after the ACL reconstruction.
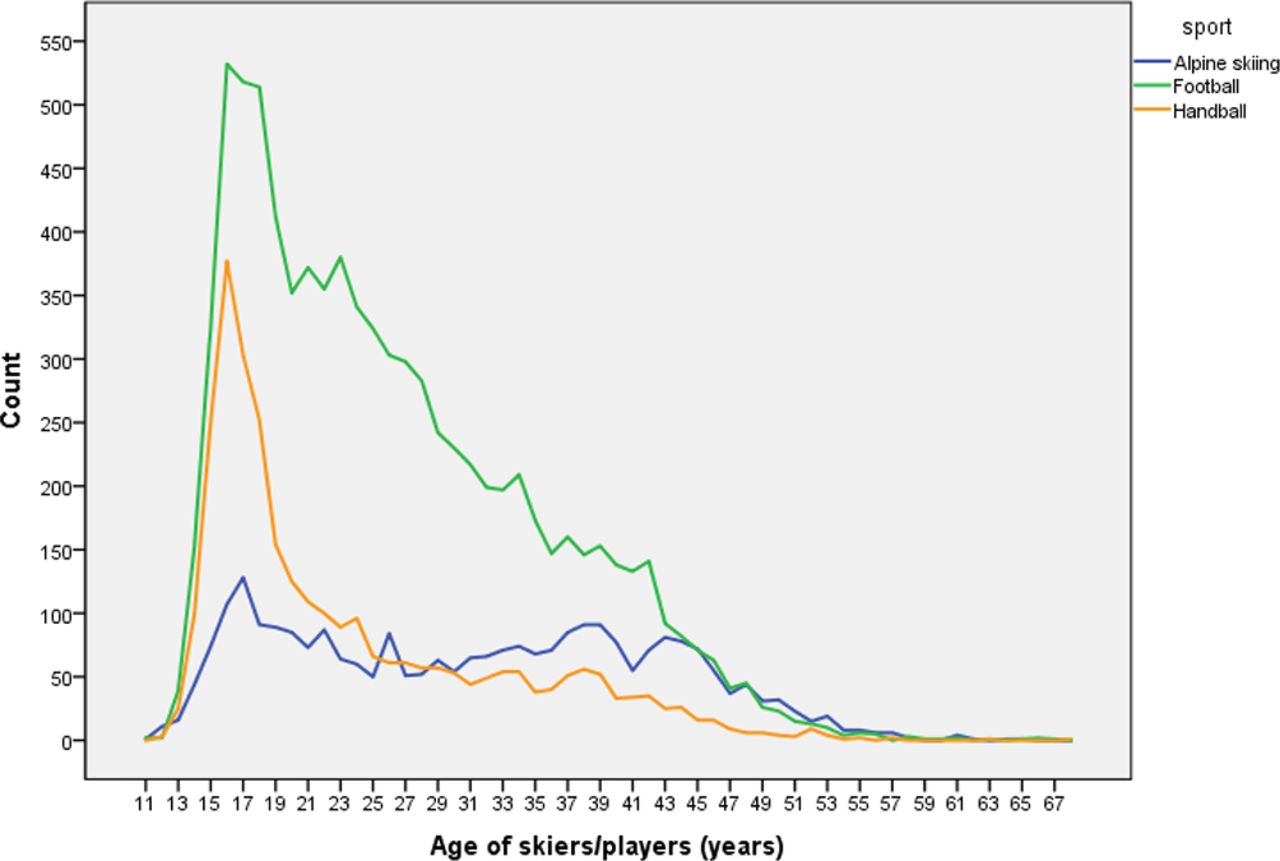
Age distribution of alpine skiers, football and handball players at the primary ACL reconstruction.
The median follow-up time was 6.0 years (Q1–Q3: 2.9–8.8), 4.4 years (Q1–Q3: 1.6–9.0) for BPTB grafts and 6.4 years (Q1–Q3 4.0–8.9) for HT grafts (p<0.001).
The crude revision rate for BPTB grafts was 2.7% after median 4.4 years compared with 6.8% for HT grafts after median 6.4 years (p<0.001).
The median time to revision was 2.6 years (Q1–Q3: 1.5–4.7) for BPTB grafts and 2.1 years (Q1–Q3: 1.2–3.6) for HT grafts (p=0.035).
Relationships adjusted for confounders
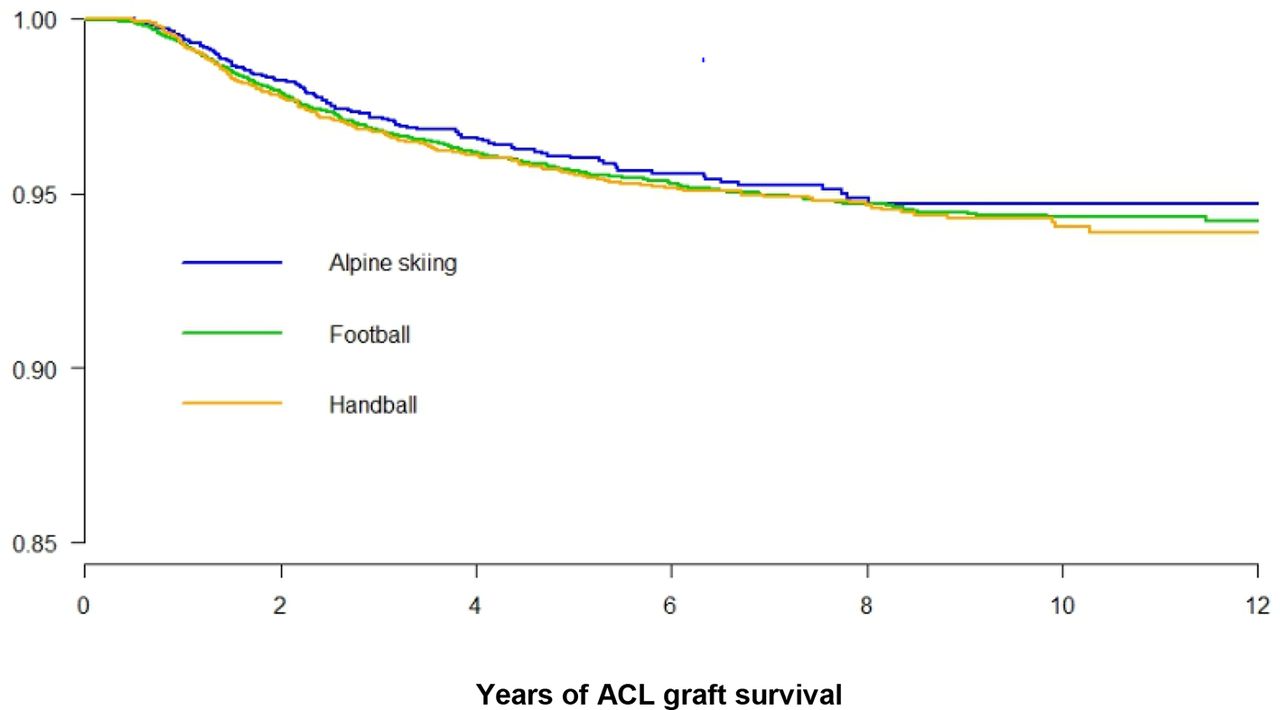
When the Kaplan-Meier graft survival plot was adjusted for age, sex, graft type and time periods, the ACL graft survival in alpine skiers, handball and football players did not differ. The revision rate increased with increasing follow-up time and was about 6% after 10 years (figure 2). The adjusted HR for ACL graft revision for individuals aged ≤18 years was 5 times higher than those aged ≥35 years (p<0.001) (table 2), being 10% and 2% respectively after 6 years.

Cox regression survival curves for ACL grafts in alpine skiers, football and handball players adjusted for age, sex, graft type and time period.
HRs for ACL graft revision in alpine skiers, football and handball players evaluated in a multivariate Cox regression model adjusted for sports category, sex, graft type (bone patellar tendon bone (BPTB) and hamstring tendon (HT) grafts), age and time period for the primary ACL reconstruction
HR for graft revision was 1.8 times higher for HT than BPTB grafts (p<0.001), 1.4 times higher in the time period 2011–2013 compared with 2004–2007 (p=0.001) and similar for females and males (table 2). For individuals aged ≤18 years, the adjusted HR for graft rupture was 2.8 times higher for HT than for BPTB grafts (p<0.001) (table 3).
HRs for revision of bone patellar tendon bone (BPTB) and hamstring tendon (HT) grafts in alpine skiers, football and handball players related to age (years) evaluated in a Cox regression model adjusted for sport category, sex and time period for the primary ACL reconstruction
The adjusted graft survival was significantly higher for BPTB than for HT grafts already after 1-year follow-up with a 12-year survival of 96% for BPTB and 93% for HT grafts (p<0.001) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Cox regression survival curves with 95% CI for bone patellar tendon bone (BPTB) and hamstring tendon (HT) ACL grafts adjusted for age, sex, type of activity (sport) and time period.
Discussion
ACL graft survival and revision rates
This study showed similar ACL graft survival for alpine skiers, football and handball players after adjustment of the data for age at primary operation, sex, type of graft and time periods, and the working hypothesis was rejected.
The ACL graft revision rate was 5% after 6 years, in agreement with other studies from the Scandinavian4 5 13 and Kaiser Permanente registries.14 The revision rates in the registries are lower than reported from studies of competitive athletes,9–11 possibly since many of the ACL reconstructions in the registries are performed in recreational athletes with a lower activity level than competitive athletes. The revision rate in this study was about 6% after 10 years. Hettrich et al 15 reported a revision rate of 7.7% after 6 years and Risberg et al 16 of 8% after mean 17.8 years. Females are reported to be more at risk for ACL injuries,17 18 but the ACL graft revision rates were similar for both genders in this study, in agreement with previous reports from the Scandinavian registries including ACL reconstructions related to all sports and other activities.4 5 13
Sixteen per cent of the graft revisions occurred within 1 year after the ACL reconstruction. Athletes should therefore not return to sport too early after the surgery since the reinjure rate is reported to be significantly reduced by 51% for each month return to level one sport was delayed until 9 months after surgery.19
Most of the ACL reconstructions in Norway (66%) were performed in alpine skiers, football and handball players. This calls for ACL injury prevention. Effective ACL injury preventive training programme have been reported for both for football20 and handball players17 and alpine skiers.21 ACL injury prevention measures are also important since the outcome of ACL revision surgery is inferior to that of primary ACL reconstructions.7 8 22–25
Influence of age on ACL graft failure
Age is an important risk factor for ACL graft failure with highest risk for the younger age groups,4 5 26 and the median age at revision was significantly lower than the median age at the primary ACL reconstruction except in handball players where the median age at the primary ACL reconstruction was only 20 years. This is in agreement with ACL graft revision being more frequent in the younger age groups. It may also play a role that many young athletes want a quick graft revision to return to sport on the same level and regain a place in the team. Alpine skiers had a higher median age at the primary ACL reconstruction and less were teenagers than observed in handball and football players. This may explain the lower revision rate among alpine skiers compared with the two other sport groups observed in the crude data, especially since the graft revision rate was 5 times higher for persons aged ≤18 years than those aged ≥35 years in this study.
Comparison of BPTB and HT grafts
BPTB was previously the most common graft for ACL reconstruction in Norway, but HT grafts increased gradually and peaked to 84% in NCLR in 2010, declining to 77% in 2012,5 to 56% in 2014 and to 34% in 2016.27 The reduced use of HT grafts during the last years in Norway is probably related to the higher revision rate of HT than BPTB grafts.4 5 Several studies have compared ACL reconstruction with BPTB and HT grafts and found similar clinical outcome, but more postoperative anterior knee pain and more stable knees have been reported with BPTB grafts, and reduced knee flexion strength with HT grafts. 28–33 Most studies report similar revision rates for BPTB and HT grafts, but Leys et al 34 have reported a rupture rate of 8% for BPTB grafts and 17% for hamstrings grafts in a group of 180 patients 15 years postoperatively. This difference was not statistically significant (p=0.07). It is therefore necessary with larger number of patients found in review and registry studies to show that the graft failure rate is almost twice as high for HP grafts as for BPTB grafts.4 5 13 14 30 35 This is confirmed in the present study that have a longer follow-up time than previous studies from the Scandinavian registries.4 5 13 The reasons for the higher revision rate of HT than BPTB grafts are not clear, but the size of the HT graft may be a factor with higher failure rates for grafts with smaller diameters.36 Also the loss of the protection of hamstrings strength for the ACL graft may play a role.37 The graft revision rate in the present study was 1.8 times higher for HT than for BPTB grafts (p<0.001), but 2.8 times higher for individuals aged ≤18 years (p<0.001). This is in agreement with the findings of Persson et al,5 and young age may also play a role for the higher revision rate of HT compared with BPTB grafts. BPTB may, however induce growth disturbances in patients with open growth zones in the knee, and HT grafts are usually used in the youngest patients.38
The HR for ACL revision was 1.4 times higher in the period 2011–2013 compared with the period 2004–2007 (p=0.001). This may be related to the much higher use of HT grafts than BPTB grafts in the years prior to and in the period 2011–2013 than in later years.5 27
Nearly half the ACL graft revisions occurred within 2 years. The median time to revision was 2.1–2.6 years after the primary ACL reconstruction since the patients usually are subjected to a conservative treatment programme with muscle strengthening before reoperation.39 For elite athletes similar but more intense programmes are used.
Strength and weaknesses of the study
The strength of this registry study is the high number of patients and the accuracy of recordings in NCLR compared with the Norwegian hospital records.1 3 The weakness is that clinical data are missing, that patients recorded in 2016 have shorter follow-up time than 1 year and that the recorded graft revision rate for the three sports probably had been higher with a longer follow-up time. Another weakness is the difference in follow-up time between BPTB and HT grafts, but this is partly compensated for by the Kaplan-Meyer survival analyses and Cox regression adjustment. We were not able to present ACL reconstruction and graft revision rates per 100 000 person years in the three sport types due to lack of data regarding how many of the Norwegian population are alpine skiers, football and handball players. Calculations of such rates would provide more accurate information of the risk for ACL reconstruction and graft revision in the three sports and enable us to compare the Norwegian rates with those from similar studies.
The most important weakness is that only graft failures revised with a new ACL reconstruction have been recorded. Since several graft failures are treated conservatively with a muscle rehabilitation programme, the real graft failure rates are probably higher than reported in this paper.
Conclusion
The ACL graft revision rate was similar in alpine skiing and the team sports football and handball, and 5% after 6 years follow-up. The revision rate decreased with increasing age at the primary operation being 10% for individuals aged ≤18 years and only 2% for those aged ≥35 years. The HR for revision of HT grafts was 1.8 times higher than for BPTB grafts, but 2.8 times higher for youth aged ≤18 years. This supports the use of BPTB grafts in this age group if the growth zones in the knee are closed.
What are the findings?
During 6-year follow-up, 5% underwent ACL graft revision.
The graft revision rates were similar among alpine skiers, football players and also handball players when the data were adjusted for age at the primary operation, sex and graft type.
The revision rate after 6 years was 10% for individuals aged ≤18 years, but only 2% for those aged ≥35 years, and 2.8 times higher for hamstring tendons (HT) than bone patellar tendon bone (BPTB) grafts for those aged ≤18 years.
How might it impact on clinical practice in the near future?
The data can inform shared decision making when young athletes with closed growth zones in the knee are considering BPTB grafts or HT grafts for ACL reconstruction.
Acknowledgments
The authors would like to thank LP Granan MD PhD and the Norwegian Cruciate Ligament Registry for providing the data for the study, and Norwegian orthopedic surgeons for providing data from their ACL patients to the registry.
References
Footnotes
Contributors AE and SH planned the study in agreement with LE. AE and SH made the initial analyses of the data. AMF extended the data collection, did the statistical analyses and made the figures. AE wrote the first draft of the paper, and all authors contributed to the final manuscript.
Funding Martina Hansens Hospital is thanked for paying for coloured figures in the article.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. All data relevant to the study are included in the article or uploaded as supplementary information.