Article Text

Abstract
Objective To determine the effectiveness of conservative treatment (CT) on pain and function in patients with patellar tendinopathy (PT) compared with minimal intervention (MI) or other invasive intervention, or in addition to decline eccentric squat.
Methods Searches were performed in MEDLINE, Embase, Cochrane, PEDro, SPORTDiscus, CINAHL and AMED databases. All randomised trials that evaluated CT (any intervention not involving invasive procedures or medication) in individuals with PT were included. Two reviewers screened studies, extracted data and assessed risk of bias of all included studies. Where suitable, meta-analyses were conducted; we assessed certainty of the evidence using GRADE methodology.
Results When compared with MI, CT did not improve pain (weighted mean difference (WMD) −2.6, 95% CI −6.5 to 1.2) or function (WMD 1.8, 95% CI −2.4 to 6.1) in the short-term (up to 3 months) follow-up. When compared with invasive intervention, CT did not improve pain (WMD 0.7, 95% CI −0.1 to 1.4) or function (WMD −6.6, 95% CI −13.3 to 0.2) in the short-term follow-up. No overall effects were found for combined CT (when a conservative intervention was added to decline eccentric squat) on pain (WMD −0.5, 95% CI −1.4 to 0.4) or function (WMD −2.3, 95 % –9.1 to 4.6) at short-term follow-up. Single studies showed an effect on pain with iontophoresis at short-term follow-up (d = 2.42) or dry needling at medium/long-term follow-up (d = 1.17) and function with exercise intervention at medium/long-term follow-up (over 3 months) (d = 0.83).
Summary/Conclusion Our estimates of treatment effect have only low to very low certainty evidence to support them. This field of sports medicine/sports physiotherapy urgently needs larger, high-quality studies with pain and function among the potential primary outcomes.
- injury
- tendon
- intervention
- knee
Statistics from Altmetric.com
What is already known?
Patellar tendinopathy responds slowly to conservative interventions; clinicians find it is challenging to manage, especially during the athletic season.
What are the main findings?
There is low to very low certainty evidence to support the short-term and medium/long-term effects of exercise, dry needling and iontophoresis as treatments for patellar tendinopathy.
As there have been major methods’ limitations in randomised controlled trials of conservative treatment for patellar tendinopathy, well-designed randomised controlled trials are needed.
Introduction
Patellar tendinopathy (PT) is characterised by pain and dysfunction of the patellar tendon.1–8 Many treatments have been described and prolonged rehabilitation is often necessary.9–13 Common management of PT includes load control, medication, adequate monitoring to detect a deteriorating tendon, and modification of musculoskeletal factors that influence biomechanics and loading.10–16
Conservative treatments (CTs) play a major role in the treatment of PT and are commonly defined as any form of non-invasive treatment (ie, excluding injections and surgery).17 Previous systematic reviews on PT have evaluated the effectiveness of individual CT or combinations of CT with an invasive treatment;16 18–22 however, these reviews do not properly inform clinical practice on which CT is recommended for PT management16 18–22 as they all suffer from serious methodological limitations. In addition, since the publication of these reviews,15 16 18 19 22 new high-quality randomised controlled trials (RCTs) have been published which may provide different insights for PT management.23–25
The aim of the current systematic review of RCTs was to investigate the effect of individual types of CT on pain and function in patients with PT compared with minimal intervention (MI) or other intervention (OI). We also investigated the effect of combining various CTs and the effect of adding a CT to decline eccentric squat. Where possible, meta-analysis of outcome data on pain and function was performed, and the certainty of the evidence was assessed using The Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology.
Methods
Search strategy and inclusion criteria
Electronic search strategies were designed to identify published RCTs investigating any CT for PT on Medical Literature Analysis and Retrieval System Online (MEDLINE), Embase, Cochrane, Physiotherapy Evidence Database (PEDro), SPORTDiscus (bibliographic database for sports and sports medicine research), The Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Allied and Complementary Medicine Database (AMED) databases. Search strategies were conducted on 13 February 2019 and no language or date restrictions applied. Descriptors used in the search strategy were related to ‘randomised controlled trials’, ‘patellar tendinopathy’ and ‘conservative treatment’ (detailed searches are presented in online supplementary appendix 1). These descriptors were intentionally broad to increase sensitivity of the search strategy and include studies on all potential treatments of interest. For the purpose of this review, ‘conservative treatment’ was defined as any intervention that did not involve an invasive procedure (injection/surgery) and/or medication. ‘Patellar tendinopathy’ was defined as persistent pain in the patellar tendon for at least 1 month during sports practice or physical activity in people aged 18 years or older (whether or not confirmed through a radiological exam).23 26
Supplemental material
Trials were eligible for inclusion if they directly compared CT to minimal intervention (MI) (ie, no intervention, placebo) or invasive interventions. Trials investigating the additional effect of CT combined with decline eccentric squat were also eligible, provided the comparison group included only decline eccentric squat and placebo. Trials comparing different CTs with each other were excluded. The primary outcomes of interest were pain (eg, Visual Analogue Scale/VAS) and function (eg, Victorian Institute of Sport Assessment-Patella/VISA-P and Kujala Scales). Short-term follow-up was defined as up to 3 months after baseline, and medium/long-term follow-up was defined as over 3 months after baseline. The review protocol was prospectively registered at PROSPERO (International prospective register of systematic reviews - ie, CRD42017072082).
Study selection
After removing duplicates, two independent reviewers (LDMM and GB) screened all titles and abstracts identified by the search strategy for eligibility and identified potentially eligible studies. Then, the same reviewers assessed all potentially relevant full texts, and RCTs fulfilling the inclusion criteria were included in the review. A third reviewer (VCO) resolved between-reviewer discrepancies in two studies.27 28 These potential full texts were excluded because they did not investigate PT. If any systematic reviews on the treatment of PT were identified during the screening process, the reference lists were screened to identify any further RCTs.
Methodological quality
Two independent reviewers (LDMM and GB) independently assessed risk of bias of all included trials using the 11-point (0–10) PEDro (Scale (http://www.pedro.org.au/), and a third reviewer (VCO) resolved any between-reviewer discrepancies. Where available, scores that were already available on the PEDro database were used.
Data extraction
Characteristics of all included trials (ie, setting, participants, intervention, comparator, outcome, follow-up) were extracted independently by two reviewers (LDMM and GB), with a third reviewer (VCO) resolving potential discrepancies. Means, SDs and sample sizes for pain and function were extracted for each group at short-term and medium/long-term follow-up. When more than one follow-up was available, we considered those closest to the end of the intervention as the short-term, and closest to 12 months after baseline as the medium/long-term follow-up of interest. When trials compared more than one CT (wired and wireless patch iontophoresis;23 eccentric exercises and heavy slow resistance training26) with a comparator of interest (sham treatment;23 corticosteroids injections),23 26 26 we combined outcome data from the investigated CTs, following Cochrane recommendations.29 The calculations used for these outcomes according to the recommendations, are detailed in online supplementary appendix 2.
Data analysis
Outcome data were transformed to common 0–10 and 0–100 point scales for pain and function, respectively. Where possible outcome data were pooled and heterogeneity was assessed using the I2 statistic, with scores less than 50% indicating low heterogeneity.30 For pooling, a fixed-effects model was used where I2 was less than 50%, and a random-effects model was used when I2 was over 50%. Pooled data are presented in forest plots through weighted mean differences (WMDs) with 95% CIs for CT overall, as well as for specific CTs. Individual study data are presented in forest plots using mean differences (MDs) and 95% CIs. Estimated effect sizes were calculated using Cohen’s benchmarks: d>0.2 for small effects; d>0.5 for medium effects; and d>0.8 for large effects.30 31 All analyses were conducted using Comprehensive Meta-Analysis software, V.2.2.04 (Biostat, Englewood, New Jersey, USA).
Two independent reviewers (LDMM and HL) assessed the certainty of the current evidence using GRADE methodology.32 In the current review, evidence started at high certainty and was downgraded by one level for imprecision when the analysed sample was <300 participants (serious imprecision was downgraded by two levels); and by one level for risk of bias when the mean PEDro Score was <5 out of 10. Investigation of publication bias was not possible due to the small number of included trials.33 Between-reviewer discrepancies were resolved by a third investigator (VCO).
Sensitivity analyses were planned to investigate whether methodological quality, sample characteristics and physical activity level impacted on the estimated effects; however, the small number of included trials limited our analyses to methodological quality only.
Results
Characteristics of included trials
After removal of duplicates, we identified 6845 references and screened them. Nine RCTs were included in the review. The main reasons for exclusion of potential full texts (n=90) were a non-randomised design (n=45); no CT as intervention (n=23); or no PT according to the employed definition (n=13). The flow of trials through the review is presented in figure 1.
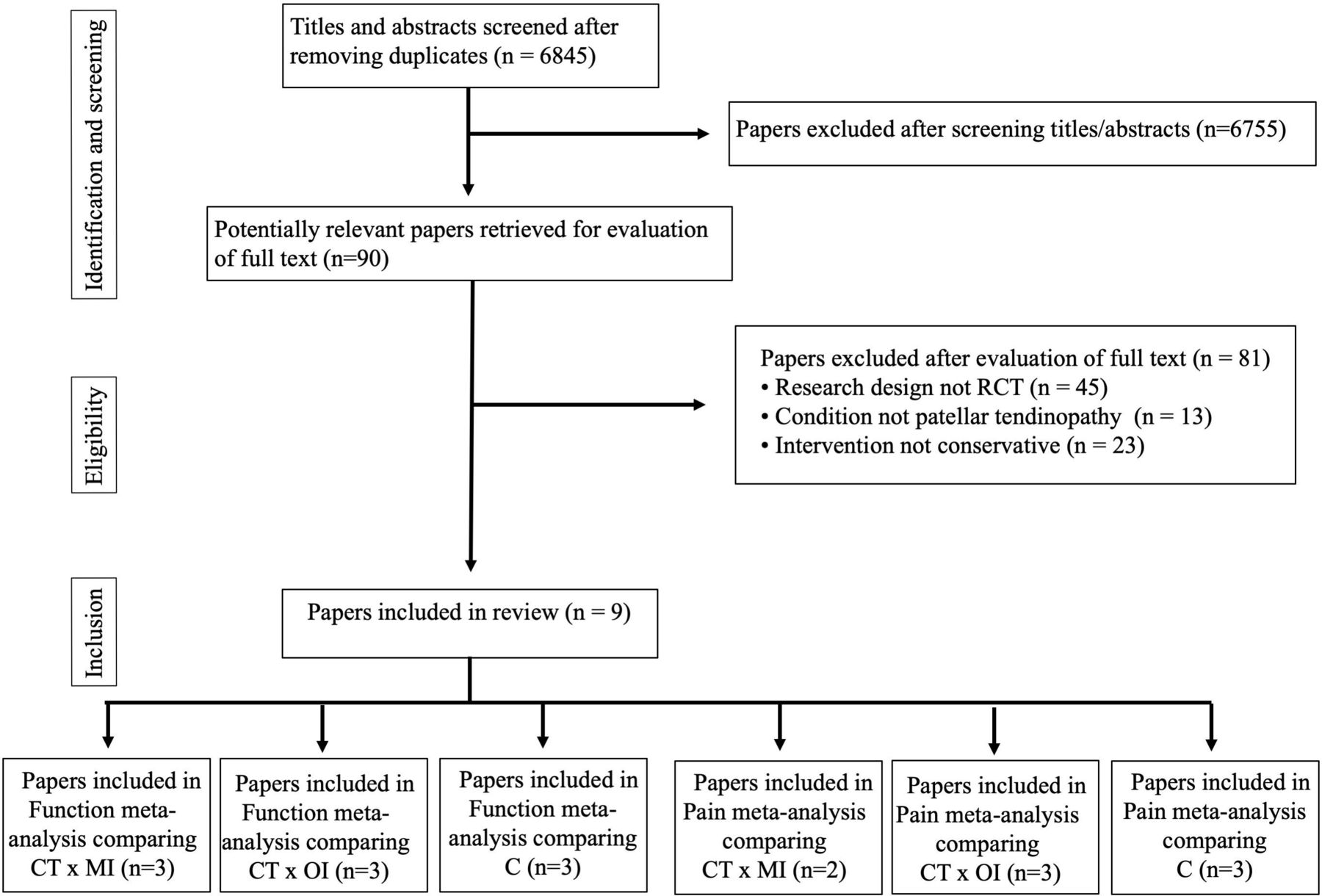
Flow of studies through the review. n, sample size; LDMM and GB, authors; RCT, randomised controlled trial; CT, conservative treatment; MI, minimal intervention; OI, other intervention; C, combined.
All nine included trials were published in English between 2005 and 2018. Three out of nine trials investigated athletes with PT,26 34 35 two included physically active participants with PT24 35 and four trials enrolled patients with PT without reporting any information on sports participation.23 25 36 37 Pain was assessed in eight;23–26 34 36–38 function was assessed in all nine included trials.23–26 34–38 Pain was assessed with a 0–10 Visual Analogue Scale,25 36–38 the 0–100 millimetre scale (transformed to a 0–10 scale)26 or with pressure sensitivity (kilograms transformed to a 0–10 scale).23 For pain, higher scores indicated worse symptoms. Function was assessed with the 0–100 VISA-P Questionnaire24–26 34–38 and the 0–100 Kujala Scale,23 with higher scores indicating better function.
Two of the included trials compared one CT with MI or OI,23 38 three compared CT with invasive treatment,25 26 34 and three investigated the effect of a CT added to decline eccentric squat.24 36 37 Three trials23 35 37 reported only short-term effects (ie, ≤3 months after baseline) and six trials24–26 34 36 38 investigated short-term and medium/long-term (ie, >3 months after baseline) effects. Characteristics of included trials and transformed outcome data are presented in table 1 and online supplementary appendix 3, respectively.
Characteristics of the included trials (n=9)
Methodological quality of included trials
The methodological quality of the included trials ranged from 1 to 9 points on the 0–10 PEDro Scale (table 2). All trials reported random allocation and 66.7% (n=6) scored above 5 points out of 10 on the PEDro Scale. The main reasons for poor methodological quality were a lack of therapist blinding (n=6, 66.7%), lack of outcome assessor blinding (n=5, 55.6%) and absence of intention-to-treat analysis (n=5, 55.6%).
Methodological quality of the included studies using PEDro Scale
Effectiveness of CT on pain and function in people with PT
The overall effect of CTs (combining all CTs as a common intervention) for PT are reported below. We considered first trials that investigated 1 CT against MI followed by OI, then trials which investigated the effect of a CT added to decline eccentric squat (combined conservative intervention) (figures 2 and 3). Finally, we reported separate analyses of specific CTs.

Pooled results of conservative treatment compared with minimal intervention or other intervention and in addition to decline eccentric squat on pain at short-term or medium/long-term follow-up in individuals with patellar tendinopathy. Left side favours conservative intervention.

{kind=link}
{kind=link}
{kind=link}
Pooled results of conservative treatment compared with minimal intervention or other intervention and in addition to decline eccentric squat on function at short-term or medium/long-term follow-up in individuals with patellar tendinopathy. Right side favours conservative intervention.
Effectiveness of combining all CTS as a common intervention versus MI
When compared with MI, estimates showed little to no effect of all combined CTs (iontophoresis and extracorporeal shockwave therapy (ESWT)) on pain (two trials,23 38 n=51 (combined CTs) and n=37 (MI)). WMD was −2.6 (95% CI −6.5 to 1.2) at short-term follow-up and MD was −0.2 (95% CI −1.5 to 1.1) at medium/long-term follow-up (see figure 2). The evidence was downgraded to low certainty due to imprecision at both short-term and medium/long-term follow-up.
When compared with MI, estimates also showed little to no effect of all combined CTs (iontophoresis and ESWT) on function (three trials,23 35 38 n=61 (combined CTs) and 47 (MI)). The WMD was 1.8 (95% CI −2.4 to 6.1) at short-term follow-up and MD was −2.2 (95% CI −11.8 to 7.4) at medium/long-term follow-up (see figure 3). The evidence was downgraded two levels to very low certainty at short-term follow-up due to serious imprecision (pooling <300 participants) and risk of bias (PEDro Score <5). At medium/long-term follow-up the evidence was only of low certainty due to serious imprecision (see online supplementary appendix 4 for all GRADE assessments).
Effectiveness of combining all CTs as a common intervention versus OI (invasive treatment)
When compared with invasive treatment (corticosteroid injections and platelet-rich plasma (PRP)), estimates showed little to no effect of all combined CTs (dry needling, exercise and ESWT) on pain (three trials,25 26 34 n=60 (combined CTs) and 44 (OI)). WMD was 0.7 (95% CI −0.1 to 1.4) at short-term follow-up and MD was −0.4 (95% CI −2.6 to 1.8) at medium/long-term follow-up (see figure 2). The evidence was also considered to be of low certainty for pain at short-term and medium/long-term follow-up (downgraded due to imprecision).
When compared with invasive treatment (corticosteroid injections and PRP), estimates also showed little to no effect of all combined CTs (dry needling, ESWT and exercise) on function (three trials,25 26 34 n=60 (combined CTs) and 44 (OI)). WMD was −6.6 (95% CI −13.3 to 0.2) at short-term follow-up and MD was 5.9 (95% CI −17.1 to 29.0) at medium/long-term follow-up (see figure 3). The evidence was of low certainty at short-term and medium/long-term follow-up (downgraded due to imprecision).
Effectiveness of adding a CT to decline eccentric squat (combined CT)
Combined CTs of three trials24 36 37 (decline eccentric squat + ESWT24 and glyceryl trinitrate patch36 and low-intensity pulsed US37) showed little to no effect on pain at short term follow-up (n=51 (combined CTs) and 61 (control)) when compared with sham treatment plus decline eccentric squat. Combined CTs of two trials24 36 (decline eccentric squat + ESWT24 and glyceryl trinitrate patch36) showed little to no effect on pain at medium/long-term follow-up (n=37 (combined CTs) and 45 (control)) when compared with sham treatment plus decline eccentric squat. WMD was −0.5 (95% CI −1.4 to 0.4) at short-term follow-up and MD was −0.6 (95% CI −1.6 to 0.4) at medium/long-term follow-up (see figure 2). Evidence was of low certainty for pain at short-term and medium/long-term follow-up due to imprecision.
When we analysed the effect of our combining CTs of three different trials24 36 37 (decline eccentric squat + ESWT24 and glyceryl trinitrate patch36 and low-intensity pulsed US37) there was little to no effect on function (n=51 (combined CTs) and 61 (control)) when compared with sham treatment plus decline eccentric squat. Combined CTs of two trials24 36 (decline eccentric squat + ESWT24 and glyceryl trinitrate patch36) showed little to no effect on function (n=37 (combined CTs) and 45 (control)) when compared with sham treatment plus decline eccentric squat. WMD was −2.3 (95% CI −9.1 to 4.6) at short-term follow-up and WMD was −6.8 (95% CI −14.4 to 0.8) at medium/long-term follow-up (see figure 3). Evidence was considered to be of low certainty for function at short-term follow-up and medium/long-term follow-up due to imprecision.
Effectiveness of specific CT for PT versus MI
When compared with MI, one trial estimated the effect of combined groups of wired and wireless iontophoresis on pain.23 Wireless (n=10) and wired (n=11) iontophoresis were applied to patients with PT and compared with sham iontophoresis (n=10).23 MD was −4.6 points on the 0–10 pain scale (95% CI −6.0 to −3.2) at short-term follow-up, indicating a large effect (d=−2.4). The evidence was considered of very low certainty (downgraded two levels due to serious imprecision and risk of bias, PEDro Score of 4 out of 10).
Effect of specific CT for PT versus invasive treatment
One trial23 combined groups performing eccentric squats (n=12) and heavy-slow resistance exercises (n=13) and compared this to a group receiving US-guided injections of 40 mg/mL methylprednisolone in 0.5 mL lidocaine (1%) (n=12).26 The MD was 17.5 points on the 0–100 function scale (95% CI 5.0 to 30.0) at medium/long-term follow-up in favour of exercise, indicating a large effect size (d=0.8). The evidence was of low certainty (downgraded due to serious imprecision) but indicates that exercise may have a potential effect on function at medium/long-term follow-up when compared with corticosteroid injections.
One trial34 compared the effect of ESWT (n=23) with PRP injections (n=23) on pain and function at medium/long-term follow-up. MDs were, respectively 1.7 points on the pain scale (95% CI 0.5 to 2.9) and −13.7 points on the function scale (95% CI −22.8 to −4.6) at medium/long-term follow-up in favour of PRP. Effect sizes indicate large effects for pain (d=0.82) and function (d=−0.87) for PRP. The evidence, which was of low certainty (downgraded due to imprecision), indicates that PRP may improve function and pain at medium/long-term follow-up compared with ESWT.
One trial estimated the effect of dry needling on pain (n=12) compared with PRP injections (n=9).25 MD was −1.4 points on the 0–10 pain scale (95% CI −2.7 to −0.1) in favour of dry needling at medium/long-term follow-up, indicating a large effect (d=1.2). The evidence, which was of low certainty (downgraded due to imprecision), indicates that dry needling may have a large effect on pain at medium/long-term follow-up compared with PRP.
Sensitivity analysis
We used sensitivity analyses to investigate the impact of poor methodological quality on the primary analyses. One trial with a PEDro Score of 1/10 was removed from the primary analysis of CT compared with MI at short-term follow-up for function.35 The resulting estimate of effect was 0.9 (95% CI −7.4 to 9.1) which was slightly smaller than the original estimate, though still not statistically significant in favour of either group (see figure 3).
Discussion
In this systematic review of RCTs, we investigated the effects of CT on pain and function in patients with PT compared with minimal and invasive treatments, or in addition to decline eccentric squat. It appears that overall CT has little to no effect on pain and function compared with MI, invasive treatment or combined treatments. We found that in individual trials that reported positive effects (ie, exercise, dry needling and iontophoresis), the evidence was of only low to very low certainty evidence due to imprecision (ie, small sample sizes) and poor methodological quality.
Overall CTs (iontophoresis and ESWT) showed little to no effect on pain and function at short-term or medium/long-term follow-up when compared with MIs (sham). Moreover, little to no effects were found for combined CTs (ESWT, GTN patch and ultrasound plus decline eccentric squat) on pain and function at short-term or medium/long-term follow-up when compared with sham. These findings are in contrast to those from other systematic reviews on CT for PT. Van Rijn et al 39 pooled three studies and found that eccentric training alone or a combination of eccentric training and ESWT, were more likely to achieve clinical improvement when compared with ESWT alone or a combination of topical glyceryl trinitrate patch, eccentric training and placebo treatment. Mani-Babu et al 19 showed limited evidence for ESWT with alternative non-operative treatments (non-steroidal anti-inflammatory drugs, physical therapy and exercise) and effects similar to patellar tenotomy surgery for medium/long-term PT. These contradictory results can be partly attributed to different inclusion criteria adopted in the systematic reviews. For instance, Mani-Babu19 compared two different CTs (ESWT vs drugs) and the current review did not aim to compare effects of different CTs, but compared CTs with MI (ie, no intervention, placebo) or invasive interventions.
Moreover, overall CTs (ie, dry needling, ESWT and exercise) resulted in little to no difference in pain and function at short-term and medium/long-term follow-up compared with OIs (ie, corticosteroid injections and PRP). PRP and corticosteroid injections are interventions aimed at reducing pain and improving the healing of various tissues.37 Di Matteo,40 however, indicated a paucity of high-level evidence regarding the application of PRP in PT treatment. In addition, the International Olympic Committee stated that for each individual a risk/benefit analysis should be performed before embarking on this therapeutic modality.41 One of the trials26 included in this systematic review indicated that corticosteroid injections had good short-term but poor medium/long-term clinical effects on PT. While further trials are needed to investigate the effect of PRP and corticosteroid injections, there is a need to focus on potential harms from these invasive treatments in order to contribute to clinical decision-making.42
By combining different CTs in the same analysis to give an ‘overall’ effect, the statistical power is increased at the expense of diluting the effect of specific treatments. However, when we analysed individual trials on CT for PT, there was only very low certainty evidence showing that iontophoresis had an effect on pain at short-term follow-up compared with sham treatment.23 Although this finding is supported by a previous study showing that analgesic treatments43 could temporarily accomplish this purpose, other studies advocate that effects will not be maintained in the latter stages of treatment when the tendon is again loaded.44 We did not identify any trials that investigated medium/long-term effects of iontophoresis treatment on pain. In a further study included in this review, dry needling revealed greater effects on pain at medium/long-term follow-up compared with PRP.25 Dry needling (trigger-point therapy) is proposed to have an analgesic and mechanical effect on the tendon45 that contributes to tensile force enhancement and medium/long-term effects.46 This mechanical effect on the tendon may be different to when ESWT is applied, as one study found no effect on function or pain at medium/long-term follow-up compared with PRP.18 Our results indicated that dry needling had better medium/long-term effects than PRP, however, this is based on low certainty evidence meaning that further research is very likely to have an effect on this estimate and may change it.
The results of the current review suggest that exercise could contribute to PT treatment, as it had an effect on function at medium/long-term follow-up compared with US-guided injections of methylprednisolone and lidocaine. Lee47 identified that tendon stiffness diminished by 15% and strain increased after 12 weeks of eccentric exercise (single-leg decline squats) among in-season athletes with PT. Scattone-Silva48 revealed that landing with greater trunk flexion promotes an immediate decrease of patellar tendon force in elite jumping athletes. Considering that PT aetiology involves tendon overload,49 clinicians should consider improving biomechanics and prioritising local interventions (to modify mechanical properties of the tendon) and more general exercises (to enhance kinetic chain energy flow) in rehabilitation when dealing with patients with PT.
Our results identified only low to very low certainty evidence to support CTs. These results indicate that the treatment of PT remains challenging and that further research on CTs is warranted to determine whether they are effective in reducing pain or improving function. It is important that future trials on treatments for PT include (1) Proper outcome definitions (including long-term pain and dysfunction—over 6 months) and inclusion criteria for PT such as younger participants and better specify the participant’s physical practice profile. (2) Patient-reported outcome measures such as absence from training and games. (3) Adequate sample sizes. (4) A long-term follow-up over 12 months.
This is the first systematic review to rigorously evaluate the methods of included trials of CT for PT and apply the GRADE system to the quality of evidence. This field is mired by low to very low certainty evidence. Previous systematic reviews were limited to a few databases with language restrictions,22 and some reviews19 22 included non-randomised studies without considering the increased risk of bias due to confounding in these studies. None of the previous reviews performed a meta-analysis or considered how small sample sizes in the primary studies were related to the certainty of the evidence available. In some cases, we combined all conservative modalities into one analysis. Our approach increases the sample size and gives an overall picture of heterogeneity across studies. One strength of the review is that we excluded trials that compared CT with other CTs because they do not answer our research question. Despite only nine trials being included for meta-analysis, we have shown the true effect of CT for PT treatment. The small number of trials and their methods’ limitations resulted in imprecise estimates.
Conclusion
There is low to very low certainty evidence that iontophoresis (up to 3 months follow-up) and dry needling (when follow-up was carried out at 6 months) may reduce pain in PT. There is low certainty evidence that exercise improves individuals’ function with follow-up at 6 months. To know whether and which CTs are effective for patients with PT, larger studies at low risk of bias are needed.
References
Footnotes
Correction notice This article has been corrected since it published Online First. The second author's name has been updated.
Contributors LDMM, HL, GB, VCO selected the trials and conducted the analysis. LDMM, HL, GB, VCO, JZ, NH interpreted the data and reviewed drafts.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.