Article Text

Abstract
Aim—To provide an understanding of the current concepts in the natural history, pathophysiology, diagnosis, and treatment of spondylolysis based on the available medical literature.
Methods—Articles were selected for review by the following methods: (a) MEDLINE searches with review of abstracts to select relevant articles; (b) review of multiple textbooks considered likely to contain information on spondylolysis; (c) review of references in articles identified by (a) and (b). Over 125 articles were ultimately reviewed fully. Publications were selected for inclusion in this article on the basis of perceived scientific and historical merit, particularly as thought to be relevant to achieving the stated purpose of this review. As no controlled clinical trials were identified, this could not be used as an inclusion criterion.
Conclusions—Isthmic spondylolysis is considered to represent a fatigue fracture of the pars interarticularis of the neural arch. There is a relatively high incidence of radiographically identified spondylolysis in the general population, but the vast majority of these lesions probably occur without associated symptoms. Symptomatic pars lesions appear to be particularly a clinical problem in adolescents, especially adolescent athletes. The optimal diagnostic and treatment algorithms are not well identified in the current literature. Multiple imaging studies may have a role in the diagnosis of a pars lesion, and treatment seems likely to require at least relative rest and physical rehabilitation with consideration of bracing or, rarely, surgical intervention depending on the clinical context.
- spondylolysis
- spondylolisthesis
- spine
- back
- neural arch
- pars interarticularis
Statistics from Altmetric.com
Spondylolysis can be defined as a defect in the pars interarticularis of the vertebral arch. This defect is seen relatively often in radiographic studies and may either occur asymptomatically or be associated with significant low back pain (LBP). Painful lesions of the pars are particularly a clinical problem in adolescent athletes. Spondylolysis and spondylolisthesis, a related condition defined by the forward displacement of one vertebral body to the one subjacent to it, were classified by Wiltse et al1 in 1976 as follows: Type I: dysplastic—congenital abnormalities of L5 or the upper sacrum allow anterior displacement of L5 on the sacrum. Type II: isthmic—a lesion in the pars interarticularis occurs. This is subclassified as (a) lytic, representing a fatigue fracture of the pars, (b) elongated but intact pars, and (c) acute fracture. Type III: degenerative—secondary to long standing intersegmental instability with associated remodelling of the articular processes. Type IV: traumatic—acute fractures in vertebral arch other than the pars. Type V: pathological—due to generalised or focal bone disease affecting the vertebral arch.
Isthmic (type II) spondylolysis is the type predominantly discussed here as it represents the primary pathology in clinical lesions of the pars in adolescents with symptomatic pars lesions.
Epidemiology and natural history
The incidence of spondylolysis in the caucasian population has been reported to be about 3–6%.2–4 Roche and Rowe4 studied 4200 cadaveric spines and found an overall incidence of 4.2%. This varied within subgroups of the population, however, with rates of 6.4% for caucasian males, 2.8% for African-American males, 2.3% for caucasian females, and 1.1% for African-American females. There was no significant change in these rates with increasing age from 20 to 80 years old. Other authors have similarly noted males being affected two to three times as often as females.2,3 The vast majority of spondylitic defects occur at L5 (85–95%), with L4 being the next most commonly affected level (5–15%), and more proximal lumbar levels being affected much less often.2–8 Many studies have shown a strong association between pars defects and the presence of spina bifida occulta.3,4,8–10 Radiographically visualised spondylolysis is associated with spondylolisthesis about 25% of the time.3,11
In an important study that provides some insight into the natural history of spondylolysis, Fredrickson et al3 prospectively studied 500 first grade students with plain radiographs and performed several smaller studies within their population. They found an overall incidence of spondylolysis of 4.4% at age six. This increased to 5.2% by age 12 and 6% by adulthood. Family members of those affected had a much higher rate of spondylolysis than the population as a whole. They also studied 500 newborns with plain radiographs and found no cases of spondylolysis. Generally no cases of spondylolysis are reported in otherwise healthy newborns, and it is the general agreement of many authors that most cases probably occur in the early school age years.1,3,12–14 The overwhelming majority of these cases are asymptomatic.3 Interestingly, Rosenburg et al15 studied 143 adults who had never walked and found that none of them had a pars defect on plain radiographs, although the views obtained were limited in some patients. This, along with the study of Fredrickson et al,3 seem to support the idea that a pars lesion is the result of repetitive stress to this region, an issue relevant to the assessment of athletes with spondylolysis and considered in more detail below.
-
Isthmic spondylolysis is found in about 4–6% of the population
-
The vast majority of radiographically evident pars defects develop during early childhood without symptoms
-
Spondylolysis occurs more often in adolescent athletes than is noted in the general population and is particularly a clinical problem in this population
The incidence of spondylolysis seems to be higher in the young athletic population than in the general population. Jackson et al10 studied 100 young female gymnasts using plain radiographs and found spondylolysis in 11%, representing an almost fivefold increase compared with the rate of 2.3% for the general caucasian female population in the study noted above by Roche and Rowe.4 In a review of 1430 radiographs on adolescent athletes (most of whom were likely to have had LBP), Rossi6 noted a roughly 15% incidence of spondylolysis for the group as a whole. Divers, weight lifters, wrestlers, and gymnasts had disproportionately higher rates within this group. In a recent review of 3152 elite Spanish athletes, Soler and Calderon7 found a slightly lower overall rate of 8.02% for the group as a whole. They also noted higher rates of spondylolysis in gymnasts and weight lifters, with throwing track and field athletes and rowers also showing particularly high incidence. Micheli and Wood16 compared adolescents presenting to a sports medicine clinic with LBP with a control population of adults with LBP and found that 47% of the adolescents had spondylolysis compared with only 5% of the adults. Other authors have similarly noted higher than normal rates of spondylolysis in gymnasts17, football players,18,19 and a variety of other athletes.12,20–23
Progressive spondylolisthesis is one of the primary concerns in patients with pars defects. Overall, the risk of progression of spondylolysis with or without low grade spondylolisthesis to a more significant slip is small. However, the literature in this regard is lacking as no standard is used to define what degree of slip progression is significant. Frennered et al24 followed 47 patients under the age of 16 with symptomatic spondylolysis or low grade spondylolisthesis for a mean of seven years. The initial degree of slip was 9–14%. In only two (4%) of their patients did the degree of slip progress ⩾20% over the follow up period. They found no radiographic or clinical correlates with the risk of slip progression. Danielson et al9 similarly reported that only 3% of their 311 patients (mean age 16.2 years) had a slip progression of greater than 20% over an average period of 3.8 years. They also found no clear predictive variables associated with slip progression, including the presence of spina bifida occulta. Blackburne et al25 found that 12 of 79 patients had a slip progression of 10% or greater over a follow up period of 1–10 or more years, but four of these patients only progressed 10% and two had presented with slips of 100%. None of their patients who presented with a slip of less than 30% progressed to a slip beyond 30%. Progressive slip was predominantly noted during the adolescent growth spurt and was associated with the presence of spinal bifida occulta in this study.25 Sietsalo et al26 followed 272 children and adolescents with spondylolisthesis and found that 23% had more than 10% progression over a mean follow up of 15.8 years. Their group had a relatively large degree of slip at the time of diagnosis (37.8% mean), and the only predictive variable identified was an increased tendency to progress with an initial slip of greater than 20%. The tendency to progress was more apparent in the age groups correlating with the growth spurt of puberty. Although spina bifida occulta was associated with more severe slips, its presence was of no statistical value in predicting progression in this study.26 In her study of 255 patients followed for at least 20 years, Saraste27 noted a mean slip progression of 4 mm with only 11% of adolescents and 5% of adults progressing more than 10 mm. Fredrickson et al3 also noted that progression was uncommon in general and they did not see progression in any patient after the age of 16. There was no significant difference in the risk for slip progression for females compared with males in the many studies mentioned above,9,24,26 although several authors noted that the initial slip on presentation was greater in females.9,26,28
Muschik et al29 specifically assessed the risk of slip progression in child and adolescent athletes. They found similar numbers to those reported for the general population, with 12% of their patients showing a slip progression of more than 10% over an average follow up of 4.8 years. Only one of their 86 patients progressed more than 20%, and 9% of their patients actually showed a partial reversal of displacement on follow up. The initial degree of slip for all patients was 10.1%. They found no significant relation between the presence of spina bifida occulta and progression, but they did note an increased tendency to progress during the early growth spurt of puberty. All of their athletes remained asymptomatic during the follow up period, and they felt that there was no increased risk for progression with active sports participation. Frennered et al24 also noted no correlation between athletic training and slip, progression of slip, or pain.
Pathophysiology
The lesion of the pars interarticularis in spondylolysis is generally considered to result from mechanical stress to that portion of the neural arch.14,22,30–34 Wiltse et al14 suggested that most cases of isthmic spondylolysis should be considered fatigue fractures caused by repetitive load and stress rather than a single traumatic event, although a single traumatic event may result in completion of the fracture already developing. Farfan et al33 hypothesised that a single event leads to the initial microfracture in the pars, with progressive fracture occurring as the result of repetitive overload. Similarly, many authors have felt that the increased rate of spondylolysis in athletes is related to the increased forces in the lumbar spine associated with various athletic activities.5,6,10,21,22,30
Several authors have looked at the effects of mechanical loading on the pars interarticularis. In a modelling experiment, Dietrich and Kurowski32 found that the greatest loads with flexion/extension movements occur at L5/S1 and that the highest mechanical stresses occur at the region of the pars interarticularis. Cyron and Hutton31 performed cyclic loading on the inferior articular processes of cadaveric lumbar vertebrae simulating shear force. They found that this type of load pattern resulted in pars fractures in 55 of 74 vertebrae studied and felt this clearly showed the vulnerability of the pars to repetitive loading. Their study also suggested that the strength of the neural arch increases up to the fourth or fifth decade of life, and they hypothesised that this may be a factor in the low incidence of acute pars fractures in older people. In a second study, they found that the vertebrae that did not fracture with their protocol had a greater cross sectional area of cortical bone in the pars than a random population sample.35 Cyron and Hutton felt that the genetic predisposition for spondylolysis may be related to a possible genetic tendency for relative cortical bone density at the pars.c2.
Using a different approach to assess the mechanical vulnerability of the pars, Sagi et al36 performed microscopic analysis of human fetal spines. They noted an uneven distribution of trabeculation and cortication in the region of the pars in the lower lumbar vertebrae. They thought that this may create a potential stress riser in the region of the pars, leaving that region vulnerable to repetitive stress. Their findings were also thought to suggest the possibility of a congenital anomaly in this region leaving a person particularly predisposed to the development of isthmic spondylolysis. This, along with the biomechanical and epidemiological studies described above, would seem to support the concept of Wiltse et al14 that isthmic spondylolysis represents a fatigue fracture of the pars related to repetitive stress.
Clinical presentation
There is little in the way of formal study of the clinical presentation of spondylolysis and related findings on physical examination. As noted above, most people found to have spondylolysis radiographically develop the lesion without symptoms.3 The clinical presentation of symptomatic spondylolysis is described by many authors as a complaint of focal low back, with radiation of pain into the buttock or proximal lower extremities noted occasionally.12,13,16,20,30,37 The onset of pain can be gradual or start after an acute injury, and mild symptoms can be present for some time with an acute worsening after a particular event.12,14 Some authors feel that activities involving lumbar spinal extension or rotation may particularly increase symptoms.7,14,37,38 Physical examination is often thought to show a hyperlordotic posture with tight hamstrings.37,39 The only possible pathognomonic finding noted in the literature is reproduction of pain by performing the one legged hyperextension manoeuvre (the patient stands on one leg and leans backwards), with unilateral lesions often resulting in pain when standing on the ipsilateral leg.14,30,37,39 Clearly, this manoeuvre may stress spinal structures other than the pars, and, as with any clinical exam finding, the results of this manoeuvre should be assessed in the context of the overall clinical picture. Neurological examination in isolated spondylolysis should generally be normal, with radicular findings suggestive of alternative or additional pathology.
Diagnostic imaging
The radiographic visualisation of a pars lesion is clearly essential in establishing a diagnosis of symptomatic spondylolysis. Many imaging modalities may play a role in the identification of a symptomatic pars lesion. Most studies on spondylolysis have used plain radiography, and much of the literature on the prevalence of spondylolysis is based solely on plain radiography, the large scale cadaveric study of Roche and Rowe4 being a notable exception. With the advent of newer imaging techniques, many of the more recent studies include the use of nuclear imaging, computed tomography (CT), and/or magnetic resonance imaging (MRI). The data derived from older studies using only plain radiography need to be interpreted with caution, as clearly many cases of spondylolysis identified by some of the newer imaging techniques are not noted concurrently on plain films. This difference may alter the way we view the natural history and treatment of spondylolysis. As the various imaging modalities all have slightly different anatomical and physiological correlates, it also may not be safe to assume that the results of studies on spondylolysis using one imaging technique are necessarily transferable to a population with pars lesions identified using a different type of imaging. These issues need to be borne in mind when considering the role of the various imaging modalities in the diagnosis of spondylolysis. Although there has been no direct comparison of the available imaging studies as they relate to clinical outcome and treatment, multiple imaging modalities may be useful in any given patient.
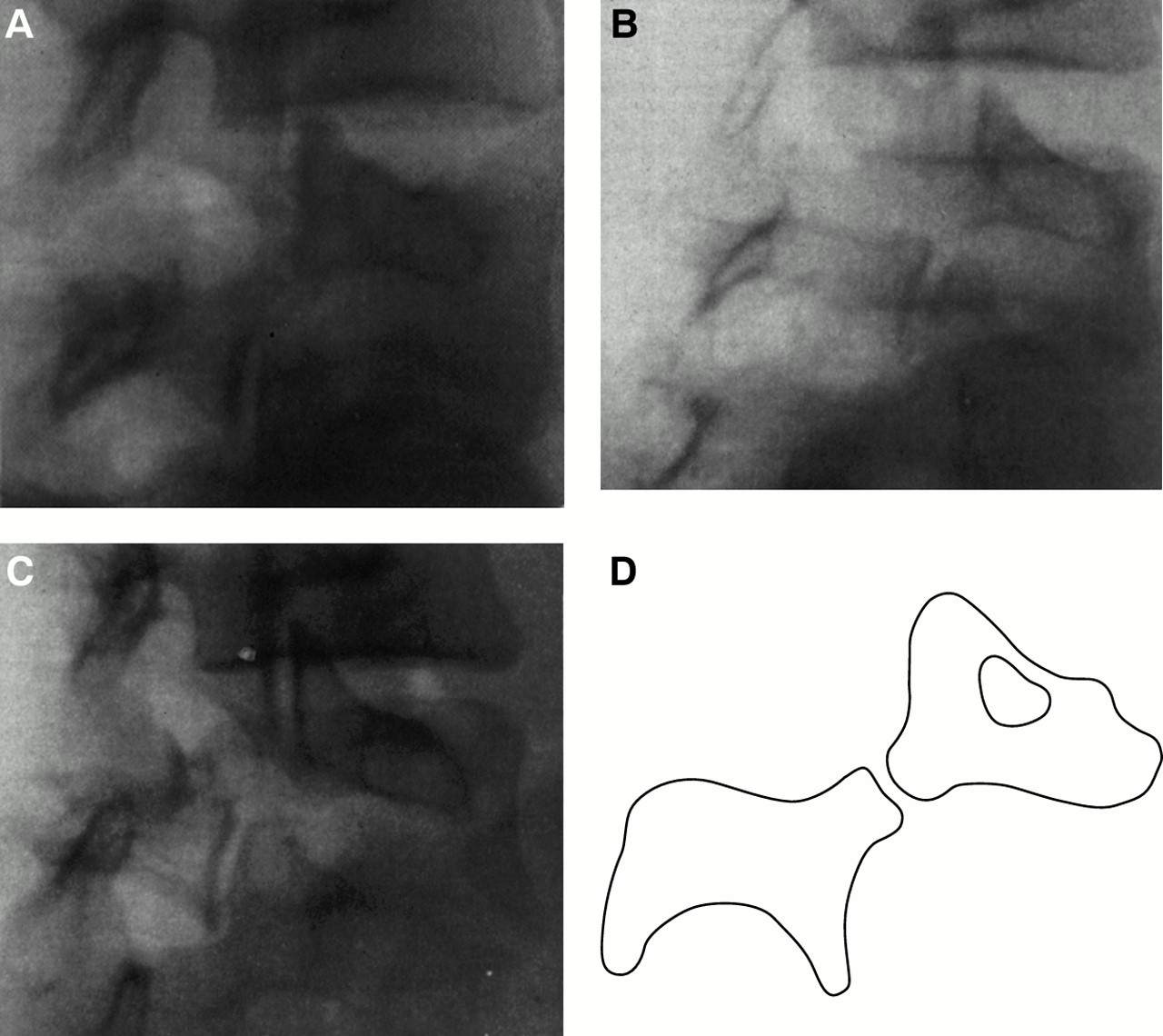
Plain radiography has been an important diagnostic tool for spondylolysis for some time (figs 1A–C and 2A,B). The defect in isthmic spondylolysis is visualised as a lucency in the region of the pars interarticularis. The lesion is commonly described as having the appearance of a collar or a broken neck on the “Scotty dog” seen in lateral oblique radiographs (fig 1D). Visualising a defect in the pars on plain radiographs can be difficult, however, and often requires multiple views of the lumbosacral spine. Using anteroposterior, lateral, and lateral oblique views, both Libson et al11 and Amato et al2 found that about 19% of the pars defects identified were seen only on the lateral oblique views. Amato et al2 also used a spot lateral view of the lumbosacral junction and a 30° up-angled anteroposterior view, and found that an additional 3.5% of defects were identified only on these two views. The single most sensitive view in this study was the lateral spot view of the lumbosacral junction, which disclosed the lesion in 84% of their cases.
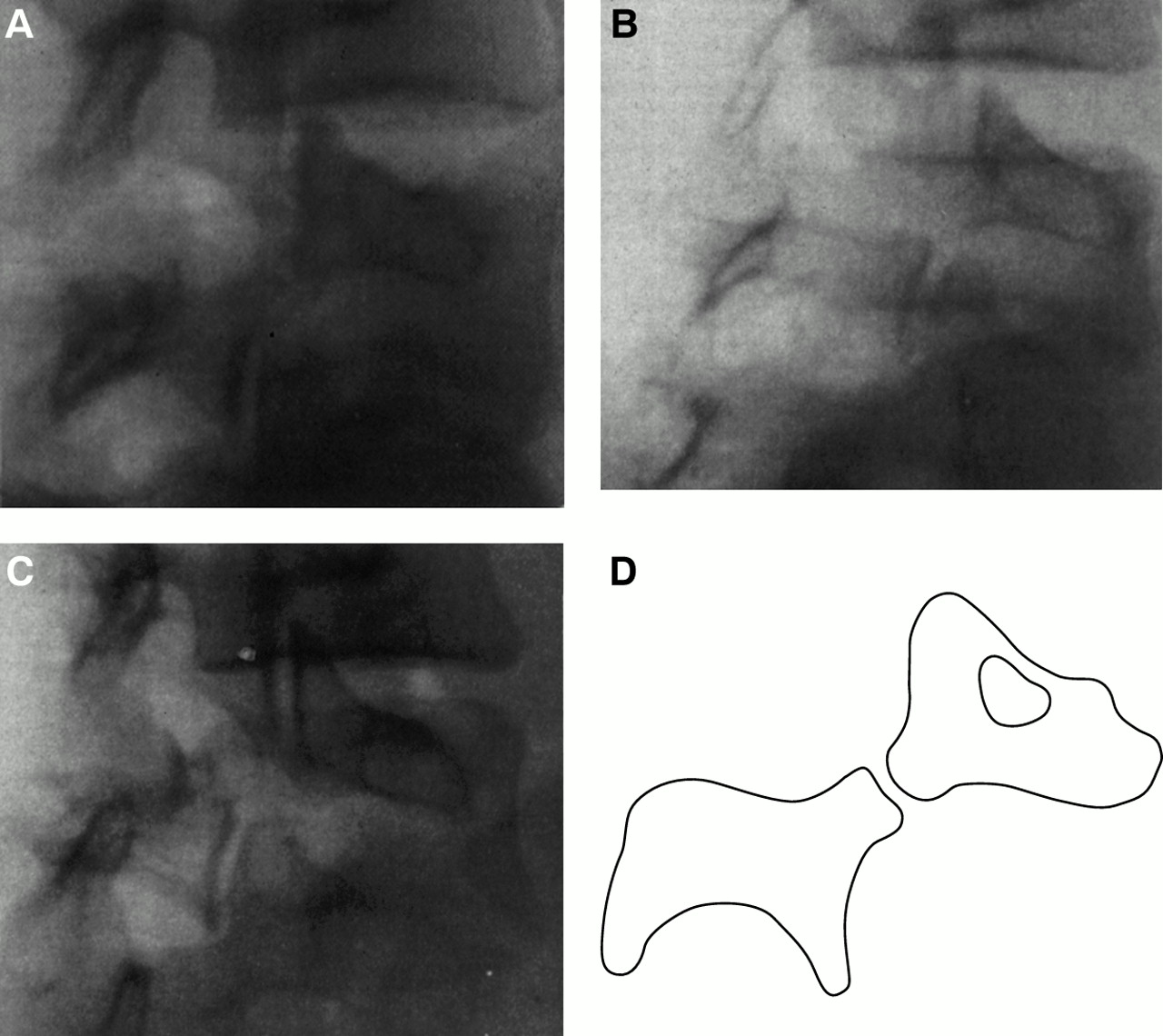
(A) Lateral oblique radiograph showing an early stage pars fracture; (B) lateral oblique radiograph showing a progressive stage pars fracture; (C) lateral oblique radiograph showing a terminal stage pars fracture; (D) line drawing from (A) showing the “Scotty dog” with a disruption in its “neck,” representing a fracture in the pars interarticularis. (A)–(C) taken with permission from Morita et al.58

(A) Anteroposterior radiograph of 12 year old athlete with low back pain showing spina bifida occulta of L5 (note incomplete formation of the posterior neural arch). (B) Lateral oblique radiograph of the same patient showing a possible pars fracture at L5.
The limitations of plain radiography arise, in part, from the orientation of the plane of the defect. To be visualised optimally on plain radiography, the defect should ideally be aligned tangentially to the radiological beam. As the lesion in spondylolysis does not lie within any of the primary orthogonal planes, it may not be aligned well with any of the standard radiological views.40,41 Saifuddin et al41 used CT scans of 69 spondylitic defects to assess the orientation of the pars lesions and found wide variation between individuals, with only 32% of the lesions aligned within 15° of the 45° lateral oblique plane. The authors concluded that standard 45° lateral oblique views alone are not reliable in identifying the presence of a pars defect, and their findings support the contention of other authors that multiple views are needed for optimal visualisation of pars defects on plain films.2,40
The problem of the limited sensitivity of plain radiography has become more apparent in several studies using radionuclide imaging, particularly single photon emission computed tomography (SPECT), and this type of imaging has been shown to offer many advantages over isolated plain radiographs (figs 3 and 4). In 1981, Jackson et al42 reported on the use of bone scan for identifying pars lesions in young athletes. They studied 37 consecutive athletes younger than 20 with focal lumbar pain and a clinical history suggestive of a pars lesion. All of these patients underwent initial evaluation with bone scan and plain films. They found increased uptake in the posterior elements in 25 of these patients, and seven of these 25 patients had no evidence of a pars defect on plain films. All seven ultimately returned to unrestricted activity without recurrent symptoms after conservative treatment. In six of the seven, the bone scan was normalised on follow up, while the other patient showed a considerable reduction in uptake compared with the original scan. The authors noted that patients with both a positive bone scan and positive radiographs or those with bilateral areas of increased uptake on initial bone scan tended to fare worse clinically. Elliot et al43 similarly reported a patient series assessed by bone scan and plain radiography. They found that two of their nine patients with positive bone scans had normal radiographs and that nine patients with spondylolysis on plain radiographs had normal bone scans. They felt that a bone scan could potentially identify pars lesions before they appeared on plain radiographs and that a negative bone scan with positive plain films made it unlikely that the pars lesion was causing symptoms. Lowe et al44 also thought that a bone scan was useful in identifying painful pars lesions noted on plain radiographs based on their study of 23 military recruits with spondylolysis on plain films. All 10 of their patients who had recent LBP had positive bone scans, while all of the asymptomatic individuals had negative bone scans.

Planar bone scan, posterior view, of the patient in fig 2 showing a mild increase posteriorly on the left at L5.
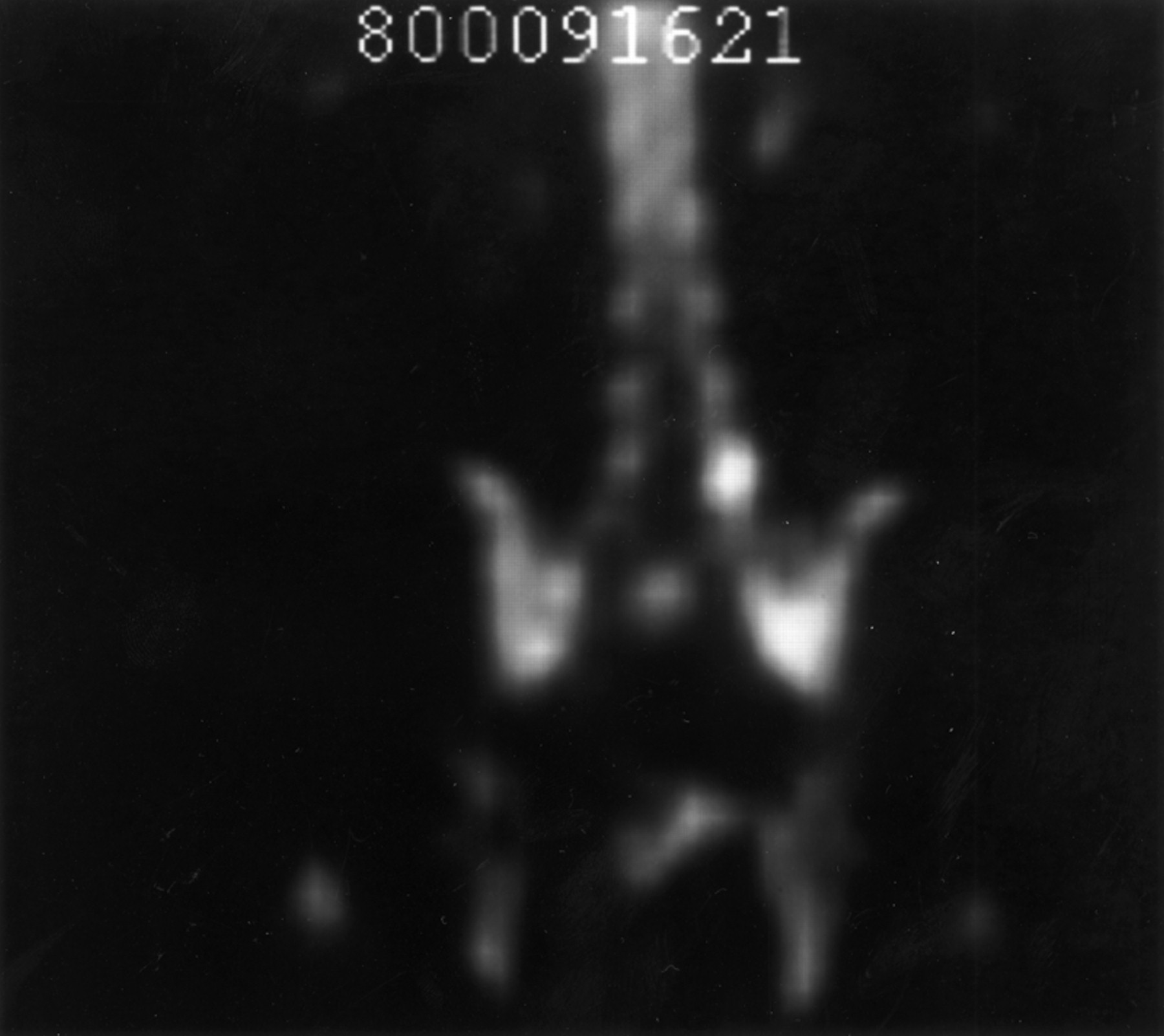
Single photon emission computed tomography (SPECT) imaging, anterior view, of the patient in figs 2 and 3 showing a clear increase in the left posterior neural arch of L5.
-
About 20% of pars defects seen on plain radiography are identified on lateral oblique views only
-
SPECT and CT have been shown to be more sensitive for identifying pars lesions than plain radiography in several studies
-
MRI may also be more sensitive than plain films but needs further study
Although planar bone scan appears to be more sensitive for detecting pars lesions than plain films, several studies have suggested that SPECT is more sensitive than both. In 1988, Bodner et al45 compared plain radiography with planar bone scan and SPECT. They studied 15 patients between 10 and 23 years old presenting with LBP. Ten of these patients had findings consistent with a posterior element lesion on the SPECT scan, but only five had a positive bone scan and only three had positive plain films. Bellah et al46 reported a similar comparative study and also found SPECT to be more sensitive than both planar bone scan and plain films. They studied 162 patients (mean age 16.4 years) and found that 91 patients had an abnormality on SPECT whereas planar bone scan only detected 32 of these cases. Of 56 patients who had negative radiographs (including some assessed with CT), 25 had a pars lesion on SPECT. Planar bone scan identified only nine of these 25 additional lesions. SPECT was notably negative in five patients with pars lesions identified on plain films or CT. Several of the abnormalities identified on SPECT were proved to represent spinal pathology other than spondylolysis, including infection and osteoid osteoma. This raises an important point about SPECT and radionuclide imaging in general. Although these modalities may present increased sensitivity in detecting pars lesions compared with plain radiography, they are not necessarily highly specific for this. Other imaging modalities, such as CT and MRI, may be required in a patient with a positive SPECT to fully clarify the diagnosis.
As mentioned above, the studies by Elliot et al43 and Lowe et al44 suggested that radionuclide imaging may be helpful in identifying symptomatic pars lesions. Studies on SPECT provide additional support for this concept. Collier et al47 studied 19 patients with a pars defect on radiography and found that all six of their asymptomatic patients had negative SPECT results whereas 11 of 13 diagnosed clinically to have symptomatic defects had positive SPECT results. Lusins et al48 found a propensity for SPECT to be positive in patients with spondylolysis and a recent injury compared with patients with spondylolysis and more long standing symptoms. Raby and Mathews49 compared the results of SPECT scanning with clinical outcome following surgery for spondylolysis. They found that the patients who became pain free after surgery all had positive SPECT scans before the operation, whereas those with continued symptoms had negative scans.
Like radionuclide imaging, CT scan has been shown to be more sensitive than plain radiography in visualising pars lesions (fig 5).40,41,50,51 Congeni et al50 compared CT with plain films and radionuclide imaging. They studied 40 young athletes with LBP, negative plain films, and a presumptive diagnosis of spondylolysis based on a positive bone scan or SPECT. They found pars lesions on CT in 34 of these patients, with 18 appearing chronic and 16 with signs of acute or healing fractures. Six patients with positive scintigraphy had no clear fracture on CT, including several with stress reactions and one with an avulsion fracture of an apophyseal joint. Both standard axial views and reverse angle gantry CT images were used for this study, and the authors noted that some lesions were seen more clearly with the axial views, whereas others were better clarified on the reverse angle gantry views. This study raises several key issues. CT was clearly more sensitive than plain radiography. In addition, it was more specific than scintigraphy. CT can reveal more detail about the nature and origin of a bony defect than can SPECT, and has the added advantage of showing other spinal pathology, such as a disc herniation, not identified with radionuclide imaging. The relative sensitivities of CT and SPECT are not fully clear. Congeni et al50 interpreted their finding of six patients with negative CT and positive radionuclide imaging as showing a 15% false positive rate for radionuclide imaging. It could also be that some of these cases represented false negatives for CT. The true relation between the two will be difficult to assess without a controlled trial, and it may be best to think of them as complementary tests, each showing a different aspect of the anatomic and physiological state of the bone.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Computed tomography scan of the patient in figs 2–4 showing a fracture in the left pars interarticularis (arrow). There is also sclerosis, but no fracture, in the right pars.
Although less well studied than CT and radionuclide imaging, MRI may also play a role in the diagnosis of spondylolysis. Its use for visualising the pars was somewhat problematical in early studies, but more recent work with improved technical approaches has proved more useful. Udeshi and Reeves52 studied sagittal thin slice MRI (3 mm slice thickness for T1 sequences and 4 mm for T2) for the recognition of normal pars. With T1 imaging, they could identify that 95% of the lumbar spine pars studied did not have a pars defect. However, only 75% of the pars studied appeared truly “normal”. T2 imaging was somewhat less sensitive in both regards. Campbell and Grainger53 also found that only 74% of the pars visualised on 3 mm sagittal T1 cuts were clearly normal, but this improved to 93% with the addition of reverse angle oblique axial T1 images and sagittal three dimensional gradient echo DESS (dual echo at steady state) images. MRI clearly offers advantages in terms of visualising other types of pathology present in the lumbar spine and may have the potential for identifying stress lesions early in their clinical course.40,54 The lack of ionising radiation with MRI may also make it a particularly desirable modality for studying pars lesions,40 especially in the female adolescent population. However, it should be noted that MRI, like CT, does not assess whether a bony lesion is metabolically active. Overall, the role of MRI in the diagnosis and treatment of spondylolysis is not yet clear in the available literature.
Treatment
Treatment for spondylolysis has been studied using a variety of diagnostic standards, therapeutic interventions, and outcome measures. The lack of consensus on these issues and the lack of any large scale controlled clinical trials on the diagnosis and management of spondylolysis make it difficult to define an optimal treatment algorithm. The recent advances in imaging technology also limit the practical utility of older studies based on plain radiography for diagnosis and follow up. Several recent studies that attempt to stratify patients on the basis of radiographic appearance of the pars lesion also complicate patient assessment as there may be clinical subgroups that should be managed differently. Although the comprehensive answers to questions on the treatment of spondylolysis await further study, currently available studies on treatment are discussed below.
In a widely referenced study, Steiner and Micheli55 assessed bony healing and clinical outcome in 67 patients with spondylolysis or low grade spondylolisthesis who were treated with an anti-lordotic modified Boston brace. All the patients were diagnosed and followed using plain radiography, and 25 of them underwent a planar bone scan. They followed a treatment regimen of brace use for 23 hours a day for six months followed by a six month weaning period and physical therapy during which athletic participation in the brace was allowed provided that no symptoms were present. Twelve of these patients showed evidence of bony healing, with the earliest changes appearing at four months, and 78% had good to excellent clinical results including full return to activity and no brace use. The overall rate of healing improved to 25% when patients with only spondylolysis were considered. This study is somewhat limited by the relatively small size, lack of controls, and the reliance on plain radiography for assessment of healing.
Blanda et al5 reported on a similar study of 82 athletes with spondylolysis and/or spondylolisthesis. The diagnosis was based on plain radiography or bone scan with plain radiography for follow up, and treatment consisted of activity restriction, bracing, and physical therapy. Unlike Steiner and Micheli,55 however, they used a brace to maintain lordosis, worn full time for two to six months until the patient was pain free with daily activity and spinal extension. The results of this study were similar to those of Steiner and Micheli,55 with 96% of the patients with only spondylolysis having good or excellent clinical results and 37% of these patients showing radiographic union, although these included 15 patients who underwent surgery after failing non-operative treatment. This study is again limited by the lack of controls, size, and reliance on plain radiography and bone scan. The different treatment strategies in these two studies showing similar clinical results particularly highlights the need for controlled trials and a better understanding of the natural history of symptomatic spondylolysis, as it is not clear where the true treatment effect lies. In one additional study on bony healing, Daniel et al56 assessed healing in a young military population with spondylolysis and found lower rates of healing by plain radiography than the two studies above despite activity restriction and three months of bracing. This study may be affected somewhat by the relatively short follow up time to the final radiographs (three or four months) and by the overall age of the population (21 years), which was significantly older than the patients in the other two studies discussed above (both with a mean age of about 16 years).5,55
In order to gain a better understanding of healing rates and patient stratification, Morita et al57,58 and Katoh et al59 attempted to assess the relation between bony healing and the radiographic stage of the pars lesion. They classified the pars lesions into early, progressive, and terminal stages on the basis of either plain radiography (fig 1A–C) or CT and found much higher healing rates in early stage lesions with very little or no healing in terminal stage defects.58,59 Morita et al58 studied 185 adolescents with spondylolysis. Plain radiography or CT was used for diagnosis and follow up, and treatment consisted of activity restriction, bracing with a non-specified “conventional lumbar corset” for three to six weeks followed by the use of an extension limiting corset for three to six months, with rehabilitation once healing had occurred. Healing was noted in 73% of the early stage, 38.5% of the progressive stage, and none of the terminal defects. Katoh et al59 studied 134 patients under 18 who were diagnosed with spondylolysis by plain radiography. All were subsequently evaluated by CT before and after treatment, and treatment consisted of relative rest only (S Katoh, personal communication). Healing was noted in 62% of the early stage defects while none of the terminal defects healed. Clinical outcome was not reported for these studies. Both of these studies, as well as the study by Blanda et al5 found much higher healing rates for unilateral pars defects than for bilateral lesions.
-
Most patients with symptomatic spondylolysis do well with conservative care
-
Many pars lesions may heal with conservative care, particularly early stage unilateral defects
-
Osseous healing is not necessary to achieve an excellent clinical outcome with full return to activities, although it would seem desirable to achieve this where possible
-
There are no published controlled trials on treatment for spondylolysis
Surgical treatment for spondylolysis has generally been reserved for patients who fail to respond to conservative treatment. It is reported to be required in about 9–15% of cases of spondylolysis and/or low grade spondylolisthesis.5,55 Indications for surgical intervention include progressive slip, intractable pain, development of neurological deficits, and segmental instability associated with pain.13,30 Surgery is generally not required to control pain.42 There are case reports of patients being treated with external electrical stimulation after conservative treatment had failed, who then went on to show bony healing.60,61 The role of this technique in the overall management of patients with spondylolysis is certainly not well defined, however.
Conclusions
Spondylolysis is a relatively common radiographic finding that predominantly develops during early childhood without any associated symptoms but may be a significant cause of pain in certain people, particularly adolescent athletes involved in sports with repetitive spinal motions. The pars lesion is probably a fatigue fracture caused by repetitive stress imposed by physical activity. Although the pars defect can often be identified by plain radiography, radionuclide imaging (particularly SPECT), CT, and possibly MRI may be needed to identify and stage a pars lesion or to exclude other spinal pathology that may be present. Most patients have excellent clinical outcomes with conservative care, although there is limited long term follow up of athletes suffering pars lesions in adolescence. Actual healing of the pars lesion seems more likely to occur in unilateral defects and in lesions with earlier appearing radiological characteristics.5,58,59 Bony healing has been shown to occur with rigid,5,55 soft,57,58 or no bracing,42,59 and excellent clinical outcomes can be achieved in the absence of fracture healing.5,55 These varied approaches and outcomes make it difficult to define clearly the role of bracing, and rigid bracing does not seem to be mandatory for the appropriate management of adolescent athletes with symptomatic spondylolysis. One common thread to most treatment approaches to spondylolysis is relative rest and the avoidance of activities associated with increased pain. This may well be the central aspect of treatment, with the primary goal of early stage treatment being minimisation of the biomechanical forces responsible for the propagation of the stress reaction in the pars. Clearly, further clinical study of spondylolysis is needed, particularly longitudinal studies to enhance our understanding of the natural history of this disorder and controlled clinical trials to study the type and extent of treatment necessary to optimise patient outcomes. This need would include comparative assessment of the different imaging methods available, with an emphasis on their use in enhancing patient identification, treatment stratification, and outcome. It is our current opinion that treatment should proceed on an individual basis after a careful assessment of the patient's overall status and identification of concrete treatment goals.
True or false?
-
It is rare to see a pars defect on plain radiograph that is not a significant source of pain.
-
Isthmic spondylolysis generally represents a congenital pars defect unrelated to physical activity or biomechanical factors.
-
SPECT appears to be highly sensitive for the presence of an acute pars lesion, although its specificity for this type of lesion is probably less than some other imaging modalities.
Multiple choice questions
-
In studies on healing of pars lesions with conservative care, terminal stage sclerotic lesions have been found to heal with what frequency?
-
73%
-
38.5%
-
25%
-
0%
-
-
The increased rate of spondylolysis with certain sports is believed to be related to which of the following?
-
Participation of smaller athletes
-
Repetitive extension, flexion, and rotational forces in the lumbar spine
-
High velocity collision in contact sports
-
Excessive rest
-
True or false?—answers
(T = true; F = false)
p 415: Standaert CJ, Herring SA. Spondylolysis: a critical review
(1) F; (2) F; (3) T.
Multiple choice--answers
p 415: Standaert CJ, Herring SA. Spondylolysis: a critical review
1 (d); 2 (b).