Article Text

Abstract
Background: The mechanism that causes pain in chronic Achilles tendinosis is not known. However, high resolution colour Doppler ultrasound has shown that neovascularisation may be involved.
Objective: To investigate if sclerosing the neovessels would affect the level of tendon pain.
Methods: The effect of colour Doppler ultrasound guided injection of a sclerosing agent, polidocanol, against neovessels was studied in 10 patients (seven men and three women, mean age 55 years) with painful chronic mid-portion Achilles tendinosis.
Results: Eight patients were satisfied with the results of treatment. There was significantly reduced pain during activity (reported on a visual analogue scale (VAS)) and no remaining neovascularisation after an average of two injections. Two patients were not satisfied, and neovascularisation remained. At the six month follow up, the same eight patients remained satisfied and could perform Achilles tendon loading activities as desired. Their VAS score had decreased from 74 before treatment to 8 (p<0.01).
Conclusions: Sclerosing neovessels appears to be an effective treatment for painful chronic Achilles tendinosis, suggesting that neovessels play a key part in causing chronic tendon pain.
- Achilles tendinosis
- pain
- ultrasonography
- neovessels
- sclerosis
Statistics from Altmetric.com
Chronic Achilles tendinosis is a relatively common painful condition with unknown cause and pathogenesis.1,2 It is generally difficult to treat.1–4 It was thought that chemical inflammation was present in this condition, but we have confirmed its absence in the chronic stage using microdialysis techniques.5 The source of pain and the mechanisms have not been scientifically clarified.3–7
Both prospective and randomised studies of painful eccentric calf muscle training have provided promising short term treatment outcomes.8,9 The mechanism underpinning the good clinical results achieved is not known. Using colour Doppler ultrasound, the same researchers showed neovascularisation in the area, with changes in all tendons with chronic Achilles tendinosis, but not in pain free normal tendons.10 In this study, passive dorsiflexion of the ankle stopped the flow in these vessels (neovascularisation). Dorsiflexion of the ankle is repeatedly performed during an eccentric calf muscle training regimen. Taken together, these findings led to the hypothesis that the vessels, and possibly also the nerves accompanying the vessels, were involved in the pain mechanisms in chronic painful Achilles tendinosis. We decided that, if this hypothesis were correct, sclerosing the neovessels would reduce pain in chronic Achilles tendinosis. Sclerosis is widely used for treating varicose veins and telangiectasia. We chose the sclerosing agent polidocanol because it has been widely used, has few side effects, and is a registered drug.11–13 It was originally developed as a local anaesthetic.
The aim of the study was to see if ultrasound guided sclerosis of the neovessels in chronic painful Achilles tendinosis would result in less tendon pain six months after study entry.
MATERIALS AND METHODS
The investigation was approved by the ethical committee of the medical faculty of the University of Umeå.
Ten patients (seven men and three women) took part. The mean age was 55 years (range 43–74), and the mean weight was 88 kg (range 63–130). The mean duration of symptoms was 16.5 months (range 4–45).
All patients had a painful thickening in the mid-portion of the tendon. In all of them, clinical findings corresponded to the ultrasonographic findings of an area with localised widening, irregular fibre structure, hypoechoic areas, and neovascularisation 2–6 cm from the calcaneal insertion.
Five patients had been treated with non-steroidal anti-inflammatory drugs, and one patient with two corticosteroid injections. Seven patients had tried eccentric calf muscle training without any effect.
Walking was the main physical activity of eight of the patients, one patient did light jogging, and one patient was a recreational golfer.
Ultrasound guided sclerosis
The examinations were performed with high resolution grey scale ultrasound with the aid of colour Doppler (Acuson Segoia; Siemens). A linear multifrequency (8–13 MHz) probe was used. The pathological changes in the painful thickened Achilles tendon were registered. Colour Doppler was used to diagnose the neovascularisation and to find the entrance of the vessels into the tendon. The contralateral non-painful tendon was also examined.
Polidocanol (5 mg/ml) was used as the sclerosing agent. The active substance is an aliphatic non-ionised nitrogen free surface anaesthetic. Before the treatment, the skin was washed with a solution of chlorhexidine and alcohol. The skin was then covered with sterile paper with a hole revealing only the middle part of the Achilles tendon. Polidocanol was injected with a 0.7 × 50 mm needle connected to a 2 ml syringe. As polidocanol is also a local anaesthetic, there was no need for anaesthesia before the injection.
Polidocanol was injected against the vessels entering the Achilles tendon from the ventral side of the tendon. The injection was performed dynamically; linear high resolution ultrasound ensured injection into or close to the vessels. The ultrasound probe was held on the dorsal side of the Achilles tendon parallel with the fibres. The injection was always from the medial side of the tendon to minimise the risk of contact with the sural nerve (fig 1). It was necessary to use colour Doppler to identify these small vessels (fig 2).

The sclerosing procedure. Note the position of the probe covered with a sterile rubber cover and the position of the injection needle on the medial side of the Achilles tendon.
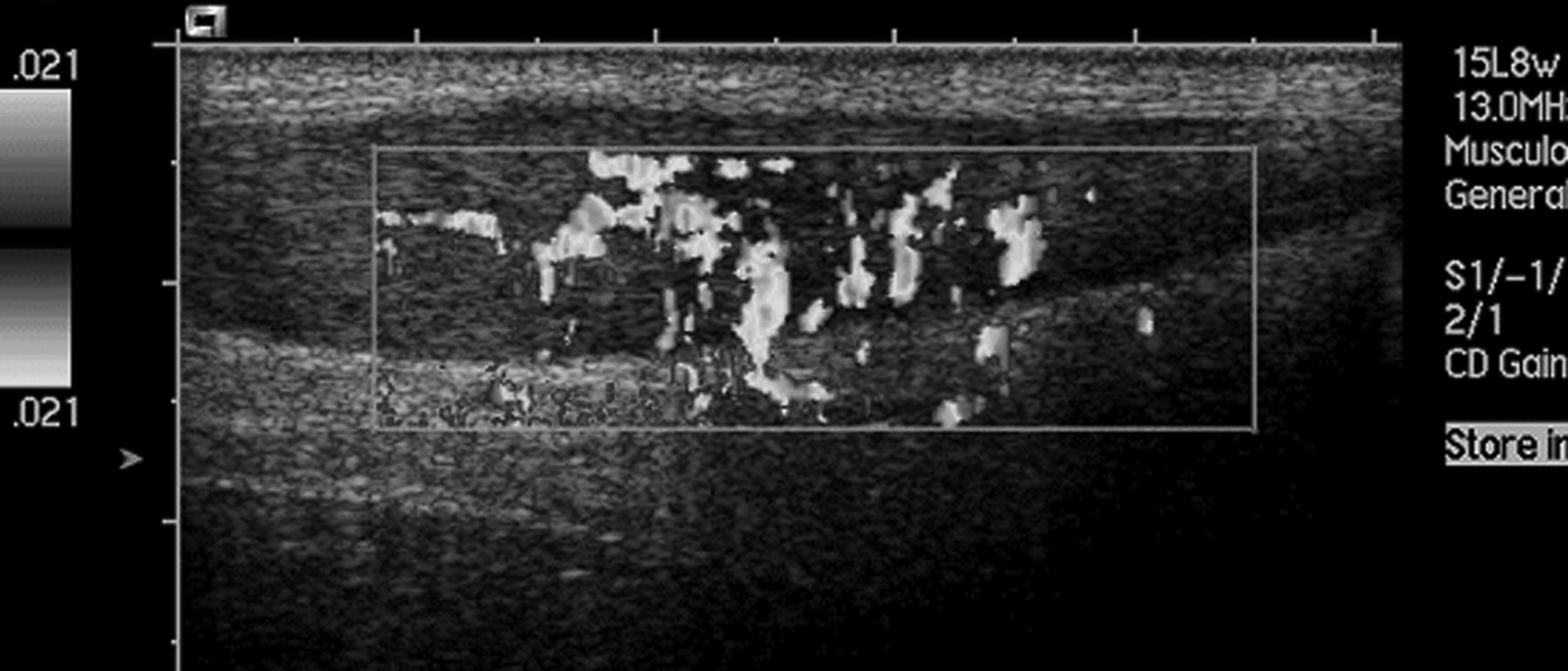
Neovascularisation in chronic Achilles tendinosis. Longitudinal ultrasound scan. Thickened and irregular tendon. Colour Doppler is presented; the neovessels are the coloured structures inside and at the ventral side of the Achilles tendon. The colour figure can be found at www.bjsportmed.com.
It was possible to place the tip of the needle into or close to the vessels entering the Achilles tendon. When the tip of the needle was positioned correctly, a small amount of polidocanol was gradually injected until all vessels were closed. Altogether 2–4 ml was injected. It was possible to observe the immediate effect of the injection (fig 3). If the position of the needle was correct (inside or very close to the vessel), the circulation stopped briefly. The injections were continued until the circulation had stopped in all the vessels in the region of the pathology.

{kind=link}
{kind=link}
{kind=link}
The same tendon as in fig 2 immediately after injection of polidocanol. There is no remaining circulation in the neovessels in the Achilles tendon. The colour figure can be found at www.bjsportmed.com.
All patients were free of pain immediately after the injection (local anaesthetic effect), but the symptoms returned after a few hours.
The patients were allowed free activity such as walking, cycling, and light jogging the day after treatment.
Outcome measures
At study entry, follow ups, and the final measurement (six months), the same experienced radiologist (LÖ) assessed neovascularisation as 0, 1+, 2+, 3+, 4+ according to the appearance of vessels inside the tendons. When no vessels were visible, the estimation was 0. When there were one or two small vessels mostly in the anterior part of the tendon, the estimation was 1+. When there were several irregular vessels throughout the tendon, the estimation was 2+ to 4+.
We also assessed Achilles tendon pain during activity at baseline, follow ups, and at six months. Using a visual analogue scale (VAS) for pain, the patients recorded the amount of pain during activity (walking or jogging) on a 100 mm long pain scale: no pain was recorded as 0 and severe pain as 100. Patient satisfaction with the result of treatment was also recorded, defined as satisfied or not satisfied. Results were evaluated before and after each treatment.
RESULTS
The mean VAS score before treatment was 74 (range 39–89), and neovascularisation was estimated as 3+ or 4+ in most tendons (table 1).
Results of sclerosing treatment in 10 patients with painful chronic Achilles tendinosis
Colour Doppler showed numerous small irregular vessels inside the tendon with tendinosis (localised widening with irregular fibre structure and hypoechoic areas). The vessels were entering from the fat pad anterior to the Achilles tendon. At the first investigation, the contralateral normal tendon was investigated and found to be thin with a regular fibre structure and without any hypoechoic areas or vessels.
Follow up
The patients were assessed clinically and by ultrasound after three to six weeks. If the Achilles tendon was still painful and neovascularisation was still present, the treatment was repeated. In the successful cases, one to four (mean two) injections were given, until there was no pain and no detectable circulation inside the tendon.
At the six month follow up (table 1), eight of the patients were satisfied with the results of treatment, and two were not. The mean VAS score after treatment (last injection) was 8.4 (range 0–29) in the former, and 71 (70 and 72) in the latter. Neovascularisation was reduced to 0 or 1+ in the eight satisfied patients, and in the two not satisfied there was no change (3+ and 4+). The two patients with persisting neovascularisation were those with a high VAS score.
There was no obvious change in thickness or structure of the Achilles tendon during the short term follow up.
There were no side effects of the treatment.
DISCUSSION
In this pilot study, sclerosing the neovessels in patients with painful chronic mid-portion Achilles tendinosis significantly diminished tendon pain during activity at six months follow up. The characteristic morphological findings in chronic Achilles tendinosis are irregular fibre structure and arrangement, high concentrations of glycosaminoglycans, and vessel ingrowth.14,15 Achilles tendinosis is most often associated with tendon pain during loading activities such as walking and jogging, but the mechanism that underpins the pain is not known. Tendon biopsy and microdialysis have shown that there is no chemical inflammation in the chronic stage of this condition.5,6 We have recently shown the presence of localised neovascularisation in 28 consecutive patients with painful chronic Achilles tendinosis, but not in 20 pain free normal Achilles tendons,10 indicating that neovascularisation may be part of the pain mechanism. The results of the present study confirm the probable importance of neovascularisation in mid-portion tendinosis. Sclerosing the vessels in the pathologically changed Achilles tendons significantly decreased pain and allowed the patients to return to pain free tendon loading activity. Colour Doppler ultrasound findings correlated well with reduced pain from the Achilles tendon. Patients with no remaining neovascularisation in the Achilles tendon had no pain during activity, but patients with unchanged neovascularisation still had pain during activity.
Our study does not show precisely why tendon pain is diminished by this treatment. However, tendons became pain free and heel raises on one leg could be performed without pain immediately after the treatment, but the pain returned within six hours. This pain free period is probably the result of the local anaesthetic effect of polidocanol, and, as only the area with neovessels was injected, this strongly indicates that this area is the source of pain. In the eight successfully treated patients, the pain gradually disappeared, in two patients after one injection and in six patients after two to four injections. Polidocanol has a selective effect in the vascular intima causing thrombosis of the vessel. It also has an effect if injected extravascularly. This is important when very small vessels are sclerosed. Polidocanol may also sclerose nerves adjacent to the neovessels, either directly (by destruction) or indirectly (by ischaemia). Further investigation of the mechanism of pain reduction by polidocanol injection is required. Polidocanol has been widely used as a sclerosing agent, with good clinical results in the treatment of varicose veins in the legs and oesophagus, haemorrhoids, telangiectasis, and gastroduodenal lesions.11–13
Take home message
Refractory Achilles tendon pain was reduced by injection of polidocanol to sclerose neovascularisation. Controlled trials are needed to test this new treatment further.
Although these data are potentially very important for treatment of tendinopathies, conclusions must remain tempered until further data are collected. The main limitations of this study are that there is no control group and that patients were not blinded to what they perceived as a new treatment.
In conclusion, colour Doppler ultrasound guided sclerosis of neovessels in patients with painful chronic mid-portion Achilles tendinosis is safe and reasonably simple to perform in the radiology room. Although limited by the absence of patient blinding or a control group, these preliminary findings are promising, as patients had significantly reduced pain during tendon loading activities. The data point to neovascularisation as a potential cause of tendon pain. We have started appropriately controlled and blinded randomised studies to evaluate further the effects of this type of treatment.
REFERENCES
Commentary
This paper describes a truly innovative treatment for chronic tendon pain that has the potential to have a major health impact. However, the data are preliminary and must be interpreted with caution until supported by further studies. The authors have an excellent track record in trials of treatments for tendon problems,1 innovative techniques to measure bone and tendon physiology,2,3 and tendon imaging.4 Their work contributes to the panoply of ground breaking tendon research from Scandinavian countries such as Finland,5 Denmark,6–10 and Norway11 as well as Sweden.12–15
The paper reflects a major paradigm shift in the treatment of tendinopathy and mirrors a changing view about tendon pathology and physiology that I will briefly review. Traditionally, doctors have addressed the supposed inflammatory component of tendon injuries, but fortunately this approach is falling by the wayside.16 Strengthening exercises have also been used to treat tendinopathy for almost 20 years,17 albeit with a recent modification that the patient may need to accept a period of significant tendon pain while undertaking heavy eccentric exercise treatment.18,19
Noticing that pain during heel drop training was not associated with failure of the exercise treatment, researchers raised questions about the role of pain in tendon healing and what structures mediated tendon pain and tendon healing.9,20–22 Answers to such questions required a novel method of measuring the intratendinous biochemical milieu. The current authors had previously used in vivo microdialysis in bone,2 and the Sports Medicine Research Unit9 were making significant breakthroughs in understanding peritendinous tissue physiology.9,10,23
Håkan Alfredson, an orthopaedic surgeon scientist, was the first to use microdialysis within the tendon itself.20 He sampled the Achilles, lateral elbow, and patellar tendons in various patients with longstanding tendon pain, as well as in some intrepid and, until then, asymptomatic volunteers.24 The patients had low levels of inflammatory markers (prostaglandin E2) and unexpectedly high levels of glutamate compared with controls.3 Whether or not glutamate is central in tendon pain, or is merely a byproduct of tendon pathology (tendinosis), remains to be elucidated.15 Continuing in their search for where the pain of tendinopathy comes from, the Umea researchers then targeted tendon neovascularisation, a key feature of tendinosis.25–27 They reported that neovascularisation was a prominent feature on ultrasonography of painful Achilles tendons, but not in those that were pain free.4 Although this does not prove cause and effect, it appears to have provided the momentum to move from investigative to interventional radiology. In what may prove to be a masterstroke in management of tendinopathy, Öhberg and colleagues then obliterated the neovasculature using a sclerosing agent, polidocanol, as reported in this paper.
The authors will agree that, although excitement is justified, the sagacious critic will reserve judgment. Data such as these do not, by any means, constitute conclusive evidence. The authors point out that this study must be followed by appropriately blinded and controlled clinical trials. Many new medical treatments have soared rapidly on the “treatment enthusiasm curve” only to crash in the wake of appropriately designed follow up studies. Nevertheless, given the suboptimal present outcome of patients with Achilles tendinopathy,5 this new treatment has the potential to fill a definite clinical need.
Apart from its potential therapeutic importance, this paper provides interesting new data from which to consider the question: where does the pain come from in tendinopathy?9,20–22 One component of tendinosis (neovascularisation) was successfully treated, and the pain largely disappeared. Does this provide a mechanism explaining the success of longitudinal percutaneous tenotomy?28 Given the intermediate time course of recovery, there is much scope for research into the pathophysiology that underpins this clinical improvement. Non-invasive techniques such as in vivo microdialysis and near infrared spectroscopy,8 as well as tendon core biopsy techniques,29 give the tendon physiologist new scope. This paper also provides impetus for colour Doppler studies of pain free, but ultrasonographically abnormal, tendons for neovascularisation.30 Such tendons are common in sportspeople.31,32
A final clinical caution relates to adverse effects, as it must with any new treatment. Polidocanol has been trialled as a venous sclerosant in bleeding peptic ulcer33 and in skin varicosities.34 Its generally benign reputation was rocked by one (reversible) cardiac arrest after injection into a right limb vein.35 Another practical issue is acceptance of polidocanol by national drug licensing authorities for this new indication.
I know that the authors of this paper are not yet claiming to have cured all tendinopathies, but they deserve enormous credit for inventing a practical, biologically plausible, and at present, promising, treatment that may become a household name—polidocanol. Their challenge, and one I am sure they have already started to address, is to test this promising innovation in rigorously designed clinical trials.