Article Text

Abstract
Aim: To conduct a detailed analysis of ankle sprains sustained in English professional football over two competitive seasons.
Methods: Club medical staff at 91 professional football clubs annotated player injuries. A specific injury audit questionnaire was used together with a weekly form that documented each club’s current injury status.
Results: Completed injury records for the two competitive seasons were obtained from 87% and 76% of the participating clubs. Ankle ligament sprains accounted for 11% of the total injuries over the two seasons, with over three quarters (77%) of sprains involving the lateral ligament complex. A total of 12 138 days and 2033 matches were missed because of ankle sprains. More sprains were caused by contact mechanisms than non-contact mechanisms (59% v 39%) except in goalkeepers who sustained more non-contact sprains (21% v 79%, p<0.01). Ankle sprains were most often observed during tackles (54%). More ankle sprains were sustained in matches than in training (66% v 33%), with nearly half (48%) observed during the last third of each half of matches. A total of 44% of sprains occurred during the first three months of the season. A high number of players (32%) who sustained ankle sprains were wearing some form of external support. The recurrence rate for ankle sprains was 9% (see methodology for definition of reinjury).
Conclusion: Ankle ligament sprains are common in football usually involving the lateral ligament complex. The high rate of occurrence and recurrence indicates that prevention is of paramount importance.
- ankle
- football
- injury
- sprain
- ATFL, anterior talofibular ligament
- CFL, calcaneofibular ligament
Statistics from Altmetric.com
Ankle sprains (especially those involving the lateral ligament complex) have often been reported as the most common injuries in sport.1–6 It has been suggested that such injuries are usually sustained in sports involving running,2 cutting,2 jumping,2,7 and contact with other players,8,9 and this partly explains the high incidence of ankle sprains in football.10–12 Ankle sprains in this population have been reported to have a high recurrence rate.11,13–15
The findings of the initial Football Association Audit of Injuries study were consistent with these findings.16 Over two seasons, the authors observed that 17% of all injuries were to the ankle, the same figure being reported by Ekstrand and Gillquist.11 Ekstrand and Tropp13 found that ankle sprains comprised 19% of all injuries. Sandelin et al17 observed that 75% of ankle injuries were ligament sprains (mostly lateral ligament complex), whereas Hawkins et al16 reported this figure to be 67% (80% being to the lateral ligament complex). Hawkins et al16 found that a total of 76% of ligament sprains that recurred during the same season were to the ankle. Given the high incidence of ankle sprains, the authors suggested that prevention and rehabilitation of ligament sprains warranted further investigation.
As a follow up to the initial study, the aim of this study was to undertake a detailed analysis of the data on ankle sprains. Information on incidence, time lost, mechanism of injury, use of external support, and timing of ankle sprains could help to suggest the best methods of preventing and rehabilitating such injuries.
METHODS
Player injuries were prospectively reported from July 1997 through to the end of May 1999 inclusive. A total of 91 of the 92 football clubs from the English football leagues (Premier and Football League) committed themselves to the project. Injuries were recorded by club physiotherapists and/or doctors on a specific player injury audit questionnaire designed for this study. Injury audit questionnaires for players who had returned to full training/competition during a particular week were returned weekly together, with a form indicating which players had been absent and the number of days and competitive matches each had missed that week. Before the study, medical staff from clubs attended a briefing day and were issued with guidance notes on how to complete the questionnaires. Only professional players with a squad number were involved in the study. Participants were asked to complete a consent form, and each club provided details of their squad at the beginning of each season. Table 1 presents the information obtained. New players who joined the club were included, and players leaving clubs were omitted from the study if they did not stay within one of the four English leagues.
Division, playing position, and age distribution of the cohort at the beginning of the study
A recordable injury was defined as one sustained during training or competition and which prevented the injured player from participating in normal training or competition for more than 48 hours (not including the day of the injury). Injuries unrelated to football were not included, nor was any absence resulting from illness. Injuries acquired during international duty were included because details of such injuries were generally reported back to club medical staff. The severity of each injury was defined as slight, minor, moderate, or major depending on whether the player was absent from training or competition for two to three days, four to seven days, one to four weeks, or more than four weeks, respectively. Reinjury was defined as an injury of the same nature and location involving the same player in the same season. The dominant foot was defined as the predominant foot used for kicking a ball.
Data were analysed using SPSS (Chicago, Illinois, USA). Descriptive and comparative data are presented. The χ2 significance test was used to investigate differences, and significance was accepted at p<0.05 level. All players agreed to participate in the study, and there were no drop outs during the study period.
RESULTS
Of the 91 clubs starting the study, completed injury records for the entirety of the 1997/1998 and 1998/1999 competitive seasons were attained from 87% and 76% respectively. During the study period, 1011 ankle injuries were documented, comprising 17% of the 6030 total number of injuries sustained over the two seasons
Table 2 displays the nature of all ankle injuries. Ankle ligament injuries (sprains) accounted for 11% of the total injuries sustained over the two seasons. There was no significant difference between the incidence of dominant and non-dominant ankle sprains based on expected values (56% v 42%). No significant differences in the incidence of ankle sprains between Premier, 1st, 2nd, and 3rd divisions were observed.
Nature of ankle injuries
Table 3 shows the medical classification of ankle sprains. Most involved injury to some portion of the lateral ligament complex, that is the anterior talofibular, calcaneofibular, and posterior talofibular ligaments (77%).
Medical classification of ankle ligament injuries
Table 4 shows the diagnostic investigations performed on ankle sprains. Only six players underwent some form of surgery, and 19 players had injections.
Diagnostic investigation of ankle sprains
One third of ankle sprains were sustained during training and two thirds during matches; there was no significant difference between the observed and expected incidence of ankle sprains based on the percentage of total match and training injuries reported. Player to player contact was responsible for 59% of injuries, and 39% were non-contact injuries. Tackling (36%) and being tackled (18%) were the most common mechanisms of sustaining an ankle sprain. Figure 1 displays the non-contact mechanisms of ankle sprains: 77% of non-contact sprains were caused during landing, twisting and turning, and running. Ankle sprains in goalkeepers were the result of significantly more non-contact mechanisms of injury than contact mechanisms (79% v 21%, p<0.01). The most common mechanisms of injury for this position were landing (36%), twisting/turning (21%), and diving (10%).
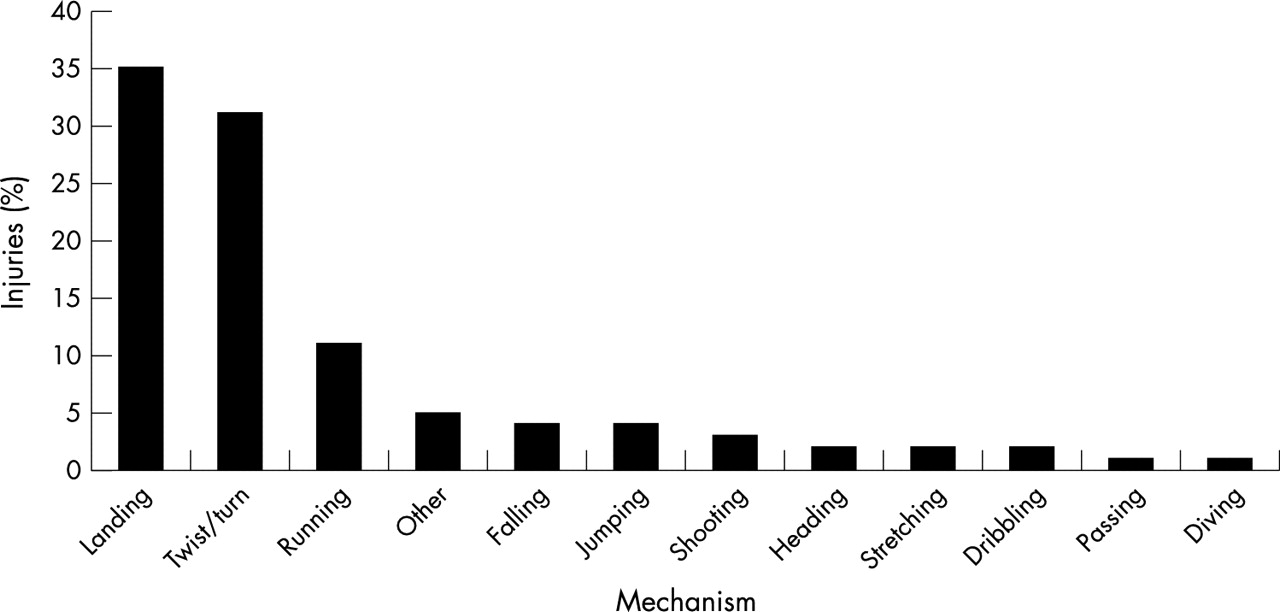
Mechanism of non-contact ankle sprains.
The total number of days that players were absent over the two seasons was 12 138, and a total of 2033 matches were missed. A total of 83% of the ankle sprains required players to miss one month or less.
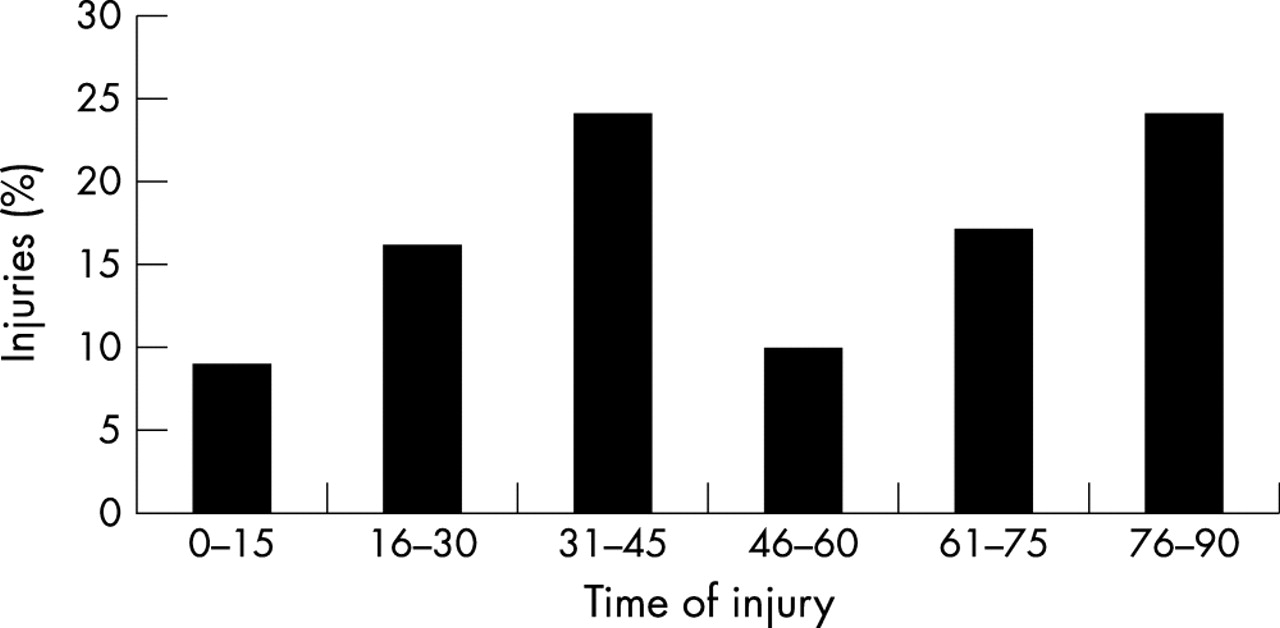
Figure 2 shows the timing of match injuries. A total of 48% of injuries were sustained during the last third of the first and second halves of the match. There was no significant difference between the number of ankle sprains sustained in the first and second halves of matches. There was no significant difference between the timing of contact and non-contact ankle sprains during matches or training.
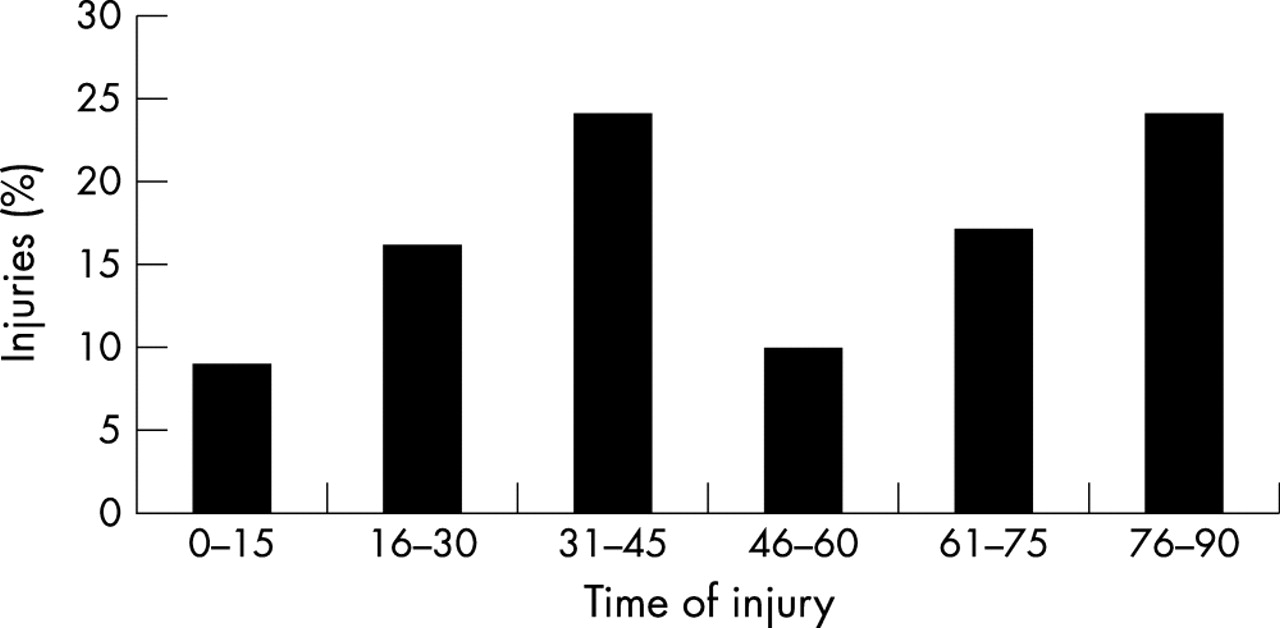
Timing of ankle sprains sustained during match play.
Figure 3 shows the number of ankle sprains during each month of the season. During the first three months of the season, 44% of ankle injuries were sustained (p<0.01).

{kind=link}
{kind=link}
{kind=link}
Month in which injury occurred: ankle sprains and all injuries.
Table 5 shows the number of players wearing external support to the ankle. In 32% of injuries, players had been wearing some form of external support.
Type of external support worn by players who sustained ankle sprains
The reinjury rate for ankle sprains was 9%, whereas the average reinjury rate for all injuries was 7%. Although not significant, there were more non-contact reinjuries than initial injuries (47% v 39%). The average number of training days missed and the average number of matches missed per ankle sprain for reinjuries and initial injuries did not differ significantly (19 days and four matches v 18 days and three matches).
DISCUSSION
Of all the injuries sustained over the two seasons, ankle injuries were responsible for 11%. This figure is lower than most other studies, with figures of 15%,18 22%,12 and 32%19 being reported. The differences in injury definition and methodology18,20,21 makes comparison between studies difficult and may help explain differences in the results. For example, some studies record injury rate per 1000 hours. However, in this study, the exposure of players to training and matches was not measured, therefore injury rate could only be reported in absolute terms. Also, we did not include any injuries where players missed training for less than 48 hours, whereas other studies have used the definition that an injury is any incident that causes a player to miss the next scheduled game or practice.11–13 On consultation with doctors and physiotherapists working in professional football, it was felt that the definition used in the present study was more appropriate. It should also be noted that the results of this study are based on the diagnoses of individual club medical personnel, which may vary from practitioner to practitioner.
We found that a sprain was, by far, the most common type of injury to the ankle (67%). Ankle sprains most often involved the lateral ligament complex (77%). Lewin12 also found the lateral ligament to be the most commonly injured structure (67%). This may be because of the relative shortness of the medial malleolus and the natural tendency for the ankle to go into inversion rather than eversion.5 We observed involvement of the anterior talofibular ligament (ATFL) in 73% of cases. Other authors have also found the ATFL to be the most commonly sprained ligament,6 with Sitler et al22 reporting that 66% of the ligamentous injuries of the ankle were to the ATFL. A possible reason for the high incidence of injury to the ATFL could be that it has a lower load to failure than the calcaneofibular ligament (CFL).2 Clanton and Porter23 quoted values of 138 N and 345 N for the ATFL and CFL respectively. Secondly, in plantarflexion, the ATFL is relatively taut, whereas the CFL is relatively loose; in dorsiflexion, the converse is true.23 This would fit with the common mechanism of injury to the lateral ligament, which typically involves the foot and ankle just at the moment of loading with a plantarflexion and inversion force.23–27
Injuries to the medial or deltoid complex accounted for only 14% of ankle sprains. Clanton and Porter23 stated that medial ligament complex injuries occur in 10% of all ankle sprains; however, their review of ankle sprains included many different sports. It is hardly surprising that the incidence of medial ligament complex sprains in our study was higher than 10% given that the demands of soccer include kicking with the inside of the foot and ankle as well as receiving tackles to this area.
This study shows that the anterior and posterior tibiofibular ligament and interosseous membrane were injured in 4% of sprains. These structures generally constitute the syndesmosis of the ankle making this value comparable to that of Renström and Konradsen,27 who reported a 3% incidence for isolated syndesmosis injuries.
In our study, 11% (77) of ankle sprains were diagnostically investigated, mostly by x ray examinations (59). According to the Ottawa strategy for ankle injuries,28 radiographs should be taken if there is bone tenderness at the tip or posterior aspect of the lateral malleolus, at the tip or posterior aspect of the medial malleolus, at the navicular tuberosity or base of the fifth metatarsal, or if the patient is unable to weight bear immediately after the injury and at the initial examination. This system can then be used to reduce the use of radiographs.
A low number of players (6) had surgery for their ankle sprains. This may be because functional non-operative treatment is the accepted choice for grade I and grade II ankle sprains.27 In the case of grade III sprains, the treatment is less clear—that is, whether to immobilise in a cast, to operate, or to allow early controlled mobilisation. Kuwada9 stated that, when conservative measures have been exhausted and the patient is not satisfied with his or her condition, surgical correction is a reliable and viable treatment.
Our results show that more ankle injuries were sustained to the dominant side than the non-dominant side, although the difference was not significant based on expected incidence. Other studies have shown significant differences.11,29,30 It could be expected that most sprains would be to the dominant side, as the main mechanisms of injury discussed previously generally involve the dominant leg.
More contact than non-contact mechanisms of injury were observed (59% v 39%). Árnason et al18 also found contact ankle sprains to be more common than non-contact (69% v 31%). Similarly they found that “tacklings”, which presumably includes tackling and being tackled, to be the major mechanism of injury (62%); in comparison, we observed this value to be 54%. Non-contact mechanisms were most commonly landing, twisting and turning, and running. The only positional variation in mechanism of injury was that goalkeepers sustained significantly more non-contact injuries (namely twisting and turning, landing, and diving). This would correlate with the functional profile of a goalkeeper as they are regularly performing these activities as part of their positional requirements. The mechanism of injury is vital from the point of view of functional rehabilitation programmes and in devising strategies for the prevention of reinjury. It has been suggested that athletes be trained and rehabilitated in potential positions of injury.26,31 If this principle is applied to football, activities involving jumping, landing, cutting and turning, and running could be performed during late stage rehabilitation and preventive protocols to maximise ankle stability during such manoeuvres. Contact positions of injury can also be used, but as this generally involves tackling, it may be more difficult to simulate and control safely. Laskowski et al32 stated that sport specific training is crucial in regaining proprioception to “hard wire the proprioceptive pathways and solidify a neuromuscular engram specific to these activities.”
According to Hawkins et al,16 the impact of an injury on a club can be considered in relation to its severity and the number of potential competitive matches missed. We observed that 12 138 days and 2033 matches were missed because of ankle sprains, which equates to an average of 18 days and three games missed per sprain. Ekstrand and Gillquist30 reported that players were absent from practice on average for four weeks after an ankle sprain, but the number of players in their study was much smaller than in the present one. In this study, 83% of ankle sprains had a rehabilitation period of less than one month. This suggests that most ankle sprains are not severe, and it is the incidence rather than severity of ankle sprains that makes them problematic injuries. It also suggests that the rehabilitation period was rather short, which may explain the higher than expected reinjury rate for ankle sprains compared with total injuries (9% v 7%), as the injury may not have had enough time to heal completely. Houglum33 stressed the importance of understanding the phases and timing of healing for appropriate, efficient, and effective rehabilitation. There is no uniform consensus on how long injured ligaments take to reach normal tensile strength; figures range from 16 weeks to 40–50 weeks for a return to 85–95% of normal tensile strength.33 With periods of rehabilitation being much shorter than the duration of ligament healing, players may have returned to full function without full tensile strength of the ligament. Applying stress to collagen in the maturation phase helps to organise the collagen fibres, enhancing the strength of the scar.33 This may present a case for continuing treatment of the ligament during the maturation and remodelling stage even when the player has returned to full training. This would ensure that the ligament regains as much strength and organisation as possible.
Konradsen et al34 monitored changes in ankle eversion strength and sensorimotor control functions after acute ankle inversion injury. They found that 12 weeks after the injury, an increased error in accuracy of ankle position was still present compared with the healthy ankle. It took six weeks for normalisation of eversion strength. These findings justify continued proprioceptive and strength type training even after players have returned to play. Tropp et al35 recommended wobble board training after return to play to prevent reinjury. This training may also help to avoid the development of chronic ankle joint instability (especially functional instability), ankle instability being common among athletes.2,4,35
More injuries were sustained during matches than in training (66% v 33%). Árnason et al18 also reported a higher injury rate for matches, but the difference was much greater (4.4 v 0.1 per 1000 hours equating to 98% v 2%). This correlates with the increased number of contact mechanisms, as more contact injuries would be expected during games.18 Nearly half (48%) of ankle sprains sustained during games occurred during the last one third of each half. This pattern was observed by Hawkins et al16 for all injuries, with the authors citing Gleeson et al36 who suggested that the risk of ligamentous injury may be increased by increases in electromechanical delay and anterior tibiofemoral displacement. This emphasises the importance of endurance training in ankle rehabilitation to avoid fatigue at the end of each half. It may also present a case for preventive training programmes when players are more fatigued—that is, at the end of training sessions. However, this requires further research, as other studies have found ankle injuries to be evenly distributed throughout games.11,37
The timing of injuries throughout the season is also important; 44% of ankle injuries were sustained during the first three months of the season, considerably more than expected. The importance of structured neuromuscular coordination and proprioceptive training during the closed season and preseason months is emphasised, as the number of ankle sprains peak in August and September. In their systematic review on the prevention of ankle sprains, Thacker et al20 emphasised the importance of conditioning of the ankle before the competitive season and during the course of the season, with emphasis on ankle strength and proprioception. According to Gauffin et al38 postural sway and the pattern for postural correction were improved by wobble board training.
Ankle sprains are commonly known as recurrent injuries, with 56%,19 75%,39 and 69%18 of sprains involving players with a previous history of ankle sprain. The problem with comparing these data with our own is that this study only recorded injuries over two seasons and therefore the past medical history of the players is not known—that is, if they sustained an ankle sprain in previous years. Also, the studies cited above have not recorded how they defined and measured previous injury. Of the 677 injuries recorded over the two seasons in this study, 57 were reinjuries, (9%). Although not significant, it was found that those players sustaining recurrent injuries missed on average more training days and matches than those with first time injuries (18 v 19 days, three v four matches). Missing four matches instead of three may not be significant in terms of statistics, but in terms of football, it is crucial that players, especially “first choice” ones, miss as few matches possible.
More non-contact mechanisms were responsible for reinjuries than initial injuries (47% v 39%). Nielsen and Yde19 described a characteristic pattern of major trauma causing the initial injury, with minor trauma (for instance during running) being responsible for the reinjury. Ekstrand and Gillquist39 reported that many major injuries were preceded by minor injuries; they suggested that this may be due to impairment of timing and neuromuscular coordination. Árnason et al37 suggested that reinjuries were caused by lack of preventive measures and inadequate rehabilitation. Controlled rehabilitation and strict adherence to directions for resumption of play should therefore be insisted upon. It may also help to have preinjury or normative measures of ankle strength and proprioception as a component of player functional profiles. The objective measures could then be used to help decide when the player is fully fit. Waddington and Shepherd26 suggested measuring postural sway as a prediction of injury risk. Athletes in the “higher injury incidence zone” would then carry out a specifically designed functional training programme to potentially reduce the risk of ankle injury.
Our study showed that 32% of players were wearing some form of ankle support when they sustained an injury. This appears remarkably high given that this is often considered to be a form of prevention of ankle sprains.14,29,31,40 The question must be posed as to why so many players were wearing an ankle support. Perhaps it was for prophylactic reasons to prevent initial injury or because of mechanical and or functional instability from a previous injury. The high number of injuries in taped ankles may be explained if the players involved had a history of ankle sprain, because the risk of reinjuring a previously sprained ankle is high. Some players are keen to return to training without reaching full fitness and may request to have their ankle strapped in the hope that this will provide extra support and protection from reinjury. This may also help to explain the high number of players sustaining injury even with an ankle support. This study did not record how many players were wearing an ankle support and who did not sustain an injury. This, along with more detail on the ankle supports used (for example the method of application, skill of applicant, and the type of joint support used), would be required to draw further conclusions. A discussion on the effectiveness of joint support for the ankle joint as a preventive tool in football is beyond the scope of this paper, although it is an issue that undoubtedly requires further investigation.
As the lateral ligament ankle sprain is so common in football, prevention of initial and recurrent injuries is of paramount importance. Methods of preventing contact ankle sprains have previously been suggested. These include rules to control and minimise unnecessary or hazardous contact with other players and appropriate officiating to ensure compliance with event rules.20 These may in practice be very difficult to implement, and so more practical interventions such as the education of coaches and players to minimise contact in training sessions and the wearing of an ankle guard component of shin guards are recommended. None of these factors have been subject to rigorous scientific review, but common sense suggests that they would be useful in the prevention of such injuries. Ekstrand and Gillquist39 recommended that coaches emphasise injury prevention and that athletes be taught basic principles of injury prevention. Other suggestions for the prevention of ankle sprains include adequate maintenance of pitches and training surfaces.39 This is a plausible suggestion because it has been reported that one of the risk factors for ankle injury is an uneven surface.5 Complete rehabilitation and preseason ankle conditioning (involving functional stimulus to both proprioceptive and muscular control systems closely related to the action that overloads the system in the first instance) have already been suggested. The use of external support in the prevention of ankle sprains has yet to be validated. However, both taping and braces have been shown to prevent ankle sprains in football players.14,29,41 The design selected for some of these studies may form a basis for questioning the validity of the results.7
Take home message
Ankle sprains are common in football and usually involve the lateral ligament. Their frequent occurrence and recurrence indicates that preventive strategies such as functional profiles (including normative and preinjury measures of ankle stability), effective rehabilitation, preseason conditioning of the ankle, and education of coaches and players are of paramount importance.
As a component of long term planning of athlete development, Bayli42 emphasised the importance of mastering eye-foot coordination and balance at an early age (6–10 years). If such fundamentals are not mastered early in an athlete’s career, his or her ability to move to a higher level of sporting achievement will be limited. This so called “window of opportunity” could also be used as a long term injury prevention strategy by educating coaches to introduce proprioceptive and coordination activities at this early age.
Ankle sprains (especially those involving the lateral ligament) are common injuries in football. It is the frequency and risk of reinjury rather than severity (time missed) that makes these injuries problematic. Emphasis is therefore on prevention through the use of functional profiles (including normative and preinjury measures of ankle stability), adequate rehabilitation, preseason conditioning of the ankle, and education of coaches and players.
Acknowledgments
We acknowledge the financial support given by The Professional Footballers’ Association together with the support of The League Managers Association, The Premier League, and The Football League, and the commitment of the medical practitioners working at professional football clubs in England and Wales. We also gratefully acknowledge the contributions made by the members of the Project Consultative Committee Working Group, namely Mr R Myles Gibson (Chairman), Dr C Cowie, Dr M Waller, Mr G Lewin, and Mr A Jones.