Article Text

Abstract
Objective: To investigate the effect of different sodium concentrations in replacement fluids on haematological variables and endurance performance during prolonged exercise.
Methods: Thirteen female endurance athletes completed three four hour runs on a 400 m track. Environmental conditions differed between the three trials: 5.3°C and snow (trial 1), 19.0°C and sunny weather (trial 2), 13.9°C and precipitation (trial 3). They consumed 1 litre of fluid an hour during the trials with randomised intake of fluids: one trial (H) with high sodium concentration (680 mg/l), one trial (L) with low sodium concentration (410 mg/l), and one trial with only water (W). Before and after the trials, subjects were weighed and blood samples were taken for analysis of [Na+]plasma, packed cell volume, and mean corpuscular volume.
Results: The mean (SD) decrease in [Na+]plasma over the whole trial was significantly (p<0.001) less in trial H (2.5 (2.5) mmol/l) than in trial W (6.2 (2.1) mmol/l). Mild hyponatraemia ([Na+]plasma = 130–135 mmol/l) was observed in only six women (46%) in trial H compared with nine (69%) in trial L, and 12 (92%) in trial W. Two subjects (17%) in trial W developed severe hyponatraemia ([Na+]plasma<130 mmol/l). No significant differences were found in performance or haematological variables with the three different fluids. There was no significant correlation between[Na+]plasma after the run and performance. There was a significant correlation between changes in [Na+]plasma and changes in body weight.
Conclusions: Exercise induced hyponatraemia in women is likely to develop from fluid overload during prolonged exercise. This can be minimised by the use of replacement fluids of high sodium concentration. Sodium replacement of at least 680 mg/h is recommended for women in a state of fluid overload during endurance exercise of four hours. However, higher [Na+]plasma after the run and smaller decreases in [Na+]plasma during the trials were no indication of better performance over four hours.
- hyponatraemia
- fluid replacement
- endurance
- women
- running
Statistics from Altmetric.com
It is well known that adequate fluid replacement during exercise is important to replace sweat loss. In this way, exercise capacity is maintained by avoiding dehydration and a decline in thermoregulation.1 As there is increasing evidence that hyponatraemia is one of the most common and most serious complications during prolonged exercise,2–4 we aimed to study sodium replacement during exercise. We chose a study population of female athletes because hyponatraemia is more common in women.2,3 Speedy and Noakes5 even considered that female sex is one of the main risk factors without knowing the underlying causes.
There are two theories on the cause of exercise induced hyponatraemia. One suggests that there are massive unreplaced sodium losses in sweat associated with dehydration.6 The second proposes that hyponatraemia develops from fluid overload in athletes who drink excessively. This causes dilutional hyponatraemia2,3,7 and prevents weight loss8 or even causes weight gain2,3 in hyponatraemic athletes immediately after long races. All studies have described an inverse relation between changes in body weight and [Na+]plasma2,7,9 during ultradistance exercise. Both this observation and the appreciable water loss7 during recovery support the theory of fluid overload.
For shorter distances, the American College of Sports Medicine recommends a fluid intake of 0.6–1.2 litres/h.10 Burke11 suggested a fluid intake of 0.5–1 litre/h in ultradistance events, and Noakes12 proposed the consumption of 0.5 litre/h for less competitive athletes during prolonged exercise. It is difficult to give specific recommendations because there are interindividual differences in water loss, which also depend on weather conditions.4,9,10,13 Vrijens and Rehrer14 found a significant inverse correlation between rates of change in [Na+]plasma and exercise time.
The aim of this study was to investigate the effect of different sodium concentrations in the replacement fluids consumed during prolonged exercise on haematological variables and endurance performance.
METHODS
Consent for our study was obtained from the local ethics committee. All 13 participants were informed about the procedures of this study and each gave written consent before participation. They were well trained, healthy female runners. All had participated in several long distance races (half marathon, marathon, 100 km races, or ultrarunning). The median age was 39.6 years (range 22–53), and the mean weight was 57.7 kg (range 52.1–64.4). They performed no exercise on the day before the trials. Each participant recorded their intake of food and drink during the 24 hours before the first trial. Participants were asked to replicate their intake for trials 2 and 3. Nutrition protocols were checked before each trial. Menstrual cycle and urinary output of the participants were not recorded.
The trials consisted of four hours of running and started at 10 30 am on three successive Saturdays. They took place on the same 400 m track in spring at an altitude of 510 m above sea level. Table 1 shows the weather conditions. The subjects were asked to run as many kilometres as possible during these four hours.
Weather conditions/ambient air temperatures
We provided three liquids of different sodium concentrations (table 2). A sample of each liquid was taken before each trial to check the sodium concentration. To minimise other variables that might affect performance, the intake of carbohydrates was kept constant in trials L and W. In trial H, 10 g more carbohydrate was consumed during the four hours because of the different composition of the original products (table 2). To adjust the energy intake in trials H and W to that in trial L, set rations of semisolid carbohydrates were given to subjects in the former (table 2). Subjects were allotted randomly to three groups (n = 5 + 5 + 3) in which the liquids were consumed in different orders.
Composition and amount of liquids/semisolids during one trial
Subjects consumed 0.33 litre of the fluids and semisolids immediately before and every 20 minutes during the trials, which resulted in an intake of 1 litre/h during the trial. They did not consume anything after the trials until they had been weighed and blood samples taken.
The subjects were weighed without shoes on and wearing the same dry clothing before and after the trials using the same scales (accuracy ± 100 g; Rowenta, Vernon, France) on a level hard surface. Blood samples were collected by routine venepuncture within 30 minutes before and after the trials. They were taken with the subject seated and were analysed within 24 hours. All reagents were stored at 4°C within 45 minutes of sample collection. Electrolytes were assayed after centrifugation (Integra 700 analyser; ion-selective electrodes; Roche, Reinach, Switzerland). Haematological assays were carried out on EDTA anticoagulated samples (Advia 120 analyser; Bayer, Zurich, Switzerland).
Residuals of measured variables were calculated to test for normal distribution, in which case analysis of variance was applicable, otherwise the Kruskal-Wallis test was used. An analysis of variance was performed with regard to [Na+]plasma before the run for the three liquids and trials to ensure comparable starting conditions. Analyses of variance were performed to detect significant differences in changes in [Na+]plasma, weight, packed cell volume, mean corpuscular volume (MCV), and performance for the three liquids and trials. Bonferroni post hoc tests were performed for statistically significant analyses of variance.
Linear correlation coefficients were calculated for various measured variables. Significance was set at p<0.05. Mild hyponatraemia was defined as [Na+]plasma = 130–135 mmol/l, and severe hyponatraemia as [Na+]plasma<130 mmol/l.
RESULTS
In trial H, [Na+]plasma decreased in 10 subjects (77%). Seven subjects (54%) were normonatraemic, and mild hyponatraemia was observed in six subjects (46%). One subject showed no change and two showed an increase in [Na+]plasma (1 mmol/l; 2 mmol/l), which means that 23% showed no decrease in [Na+]plasma at all.
In trial L, 12 women (92%) had lower [Na+]plasma after running. The one subject showing an increase in [Na+]plasma was hyponatraemic before the trial ([Na+]plasma = 134 mmol/l). Nine subjects (69%) developed mild hyponatraemia.
[Na+]plasma decreased in all subjects in trial W. Mild hyponatraemia was found in 12 subjects (92%), and one subject had a [Na+]plasma of 135 mmol/l. Two subjects (17%) had a [Na+]plasma of 129 mmol/l, which is considered severe hyponatraemia (table 3). Although they were severely hyponatraemic, they did not have any clinical symptoms of hyponatraemia.
Haematological variables and their changes, absolute performance and changes in body weight for the three trials and liquids
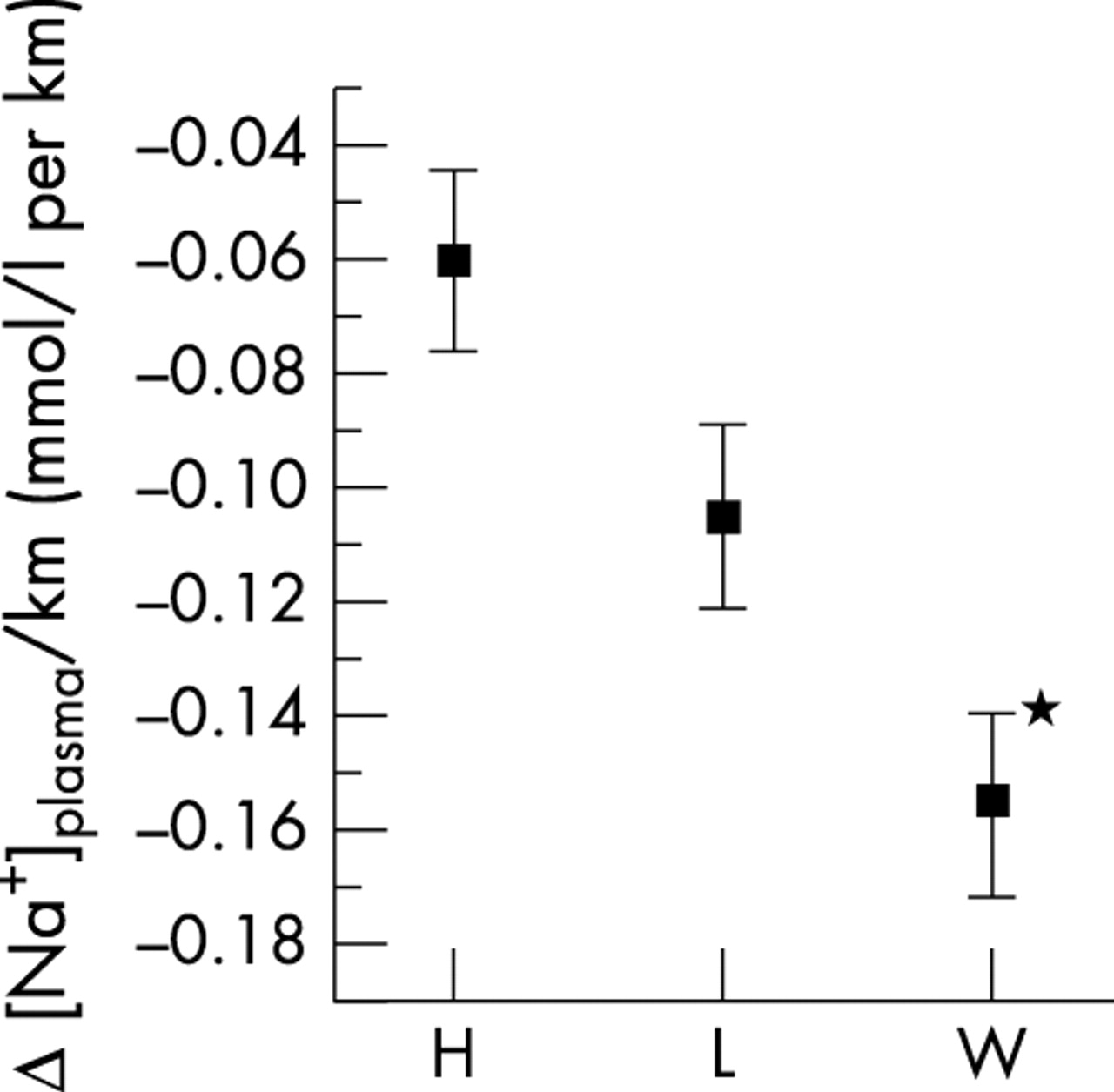
The differences in the change in [Na+]plasma and [Na+]plasma/km were significantly smaller in trial H than trial W (table 3, figs 1 and 2). [Na+]plasma was significantly higher after the run in trial H than trial W (table 3) (Bonferroni post hoc test). [Na+]plasma after the run and changes in [Na+]plasma and [Na+]plasma/km did not differ for the three fluids (analysis of variance).

Changes in [Na+]plasma over a four hour run when fluids of high (H) or low (L) sodium concentration or water (W) were consumed. Means (SD) are shown. *Significantly different from W.
{kind=link}
{kind=link}
Changes in [Na+]plasma/km over a four hour run when fluids of high (H) or low (L) sodium concentration or water (W) were consumed. Means (SD) are shown. *Significantly different from H.
Performance was significantly better in trials 2 and 3 than in trial 1. Weight gain was significantly larger in trial 1 than in trial 2. Packed cell volume and MCV fell significantly less in trial 1 than in trial 2 (table 3) (Bonferroni post hoc test). Performance, weight, packed cell volume, and MCV did not vary with intake of the three different liquids (analysis of variance).
All subjects in trial H, 12 (92%) in trial L, and 11 (85%) in trial W gained weight. Weight loss was observed in one subject in trial L (0.2%) and in two in trial W (0.8% and 0.2%). Packed cell volume and MCV decreased in 10 subjects (77%; table 3).
There were significant correlations between changes in [Na+]plasma and changes in weight (r = −0.353; p<0.02) and also between [Na+]plasma after the run and changes in weight (r = −0.291; p<0.04). The correlation between performance and change in weight was also significant (r = −0.364; p<0.03).
DISCUSSION
The most important result of this study is that, in female endurance athletes, a decline in [Na+]plasma can be minimised or even avoided in a situation of fluid overload during exercise by consuming fluids of high sodium concentration. No subject in trial H had severe hyponatraemia, and the decrease in [Na+]plasma was smaller than in trial W after four hours of running. Differences in [Na+]plasma between trials H and L were not significant, but in trial L the incidence of hyponatraemia was higher (fig 1, table 3).
Our subjects drank 1 litre of liquid an hour, about the maximum generally recommended.4,9,10,13 This fact and our results showing weight gain suggest that fluid overload was the cause of hyponatraemia in 69% of our subjects.13 Several reasons have been suggested for the failure to excrete the fluid overload: abnormalities in renal function, elevated levels of antidiuretic hormones, limitations in intestinal absorption, retained fluid in the gastrointestinal tract, or a combination of these or other factors.5,7,14,15 Maughan et al16 suggested that acute restoration of fluid balance after exercise induced fluid loss is not affected by the normal menstrual cycle in healthy untrained eumenorrhoeic young women. However, we cannot exclude the possibility that cyclical neuroendocrine variations during the menstrual cycle influenced the excretion of fluid and/or sodium in our subjects.
With regard to fluid storage, we expected a decrease in packed cell volume and [Na+]plasma and an increase in MCV and body weight as a consequence of fluid overload as observed in the state of hypotonic hyperhydration. We recorded no significant differences in packed cell volume and body weight change after ingestion of any of the three liquids. This suggests that the increase in plasma volume was no larger in trial H than trials L and W, even though the subjects showed significantly smaller decreases in [Na+]plasma (fig 1). Changes in MCV did not show a fluid shift into the intracellular compartment (table 3). Therefore it is not possible to conclude from our results in which compartment the fluid was stored.
From these results and the fact that most of our subjects complained about indigestion when consuming the fluid of high sodium concentration, it is possible that there is an ingestion limit for fluid and/or sodium. As there were fewest complaints on consumption of the fluid of low sodium concentration, it is possible that the semisolid carbohydrates provided had an effect on fluid shifts.
Our findings support those found in two papers by Sanders et al,17,18 who showed that replacement of sodium was only beneficial if the total fluid loss was replaced. However, our results should be interpreted with caution as it has not been shown yet whether weight changes are an exact indirect measure of changes in fluid status, as already questioned by Speedy et al.3
Differences in decreases in [Na+]plasma and [Na+]plasma/km were not significant between trials 1, 2, and 3, but they were significant for the different liquids: decreases were less in trial H than in trial W. This suggests that decreases in [Na+]plasma were more influenced by the type of fluid than by the ambient temperature (table 3).
Ingestion of sodium did not have any significant effect on performance (table 3), as shown in other studies.14,19 Performance in trials 2 and 3 was better than in trial 1, showing that ambient temperature had more influence on performance than sodium concentration in the replacement fluids and may have confounded the results (table 3). The lack of significance may be related to the large variability in performance in our subjects, whose exercise time may have been too short to result in hyponatraemia in this special case of fluid overload because hyponatraemia has often been observed in female runners during ironman triathlons lasting more than 10 hours.2,3
When we related [Na+]plasma to weight change, we observed that the decrease in [Na+]plasma was larger in trial W than in trial H. Weight changes in trials H, L, and W were not significant (table 3). Therefore consumption, at the same rate, of fluid of different sodium concentrations did not significantly alter changes in body weight and hence fluid status.
How much sodium do runners need during prolonged exercise to prevent hyponatraemia? Zapf et al20 calculated a sodium intake of 730 mg/h to keep [Na+]plasma constant. Barr et al1 observed that decreases in [Na+]plasma did not change significantly when 1.1 litre/h of a liquid containing 650 mg sodium/l was provided rather than the same amount in the form of water. Vrijens and Rehrer14 found smaller decreases in [Na+]plasma when subjects drank 1.2 litres of a sodium-containing sports drink (410 mg/l) an hour compared with water. Our control product (trial L) also contained 410 mg sodium/l and our results support their findings. We also showed that decreases in [Na+]plasma can be minimised or even avoided by taking fluids containing even more sodium than our control product (trial L), but the differences were not significant.
The pathogenesis of hyponatraemia is still uncertain, and recommendations on intake depend on many variables.5 However, on the basis of our results, we recommend sodium replacement of at least 680 mg/h for endurance exercise of four hours or more in women who are in a state of fluid overload to minimise the risk of hyponatraemia.
Furthermore we recommend a fluid intake of less than 1 litre/h for women during prolonged exercise because consuming 1 litre/h during a four hour run was sufficient to cause fluid overload in most of the subjects in our study.
Further research is needed to investigate both ingestion limitation and the fluid composition that would result in fewest side effects and medical complications and produce improved performance. The actual physiological mechanisms by which the risk of developing hyponatraemia is minimised by intake of fluids of high sodium concentration have yet to be established.
Take home message
Consumption of 1 litre of fluid an hour during a four hour run is sufficient to cause fluid overload in women during prolonged exercise. In such cases of fluid overload, sodium replacement is important. We recommend sodium replacement at 680 mg/h for women to minimise the risk of developing hyponatraemia.
Acknowledgments
This study was supported by ECR Pharma GmbH, Hünenberg, Switzerland. We thank our subjects and the laboratory of the Swiss Paraplegic Centre in Nottwil for their contributions.
REFERENCES
Commentary 1
This research furthers our knowledge of plasma sodium balance as influenced by beverage intake and composition during exercise. It supports previous research showing that the addition of sodium to a beverage is beneficial, reducing the decrease in plasma sodium concentration often observed with exercise when fluid ingestion is equal to or greater than fluid losses.1 Both studies also show an inverse correlation between body weight change and plasma sodium concentration. It appears that fluid retention and lack of compensatory urinary output may play a role in the development of hyponatraemia. Although a fluid overload was given in this study, it appears that this is not necessary to elicit a decrease in plasma sodium and that the lack of appropriate fluid output is central to the development of hyponatraemia.
References
Commentary 2
One of the questions always asked in any discussion on exercise associated hyponatraemia is about the role of sodium supplementation in the prevention of hyponatraemia (despite there being no published data implicating sodium losses in the causes of hyponatraemia). To date, there is very little published research that helps to answer these questions. This paper therefore represents an important contribution to our knowledge on this controversial subject. The data confirm that an intake of 1 litre/h in female endurance athletes leads to fluid overload and sometimes hyponatraemia also (despite 1 litre/h being within commonly accepted guidelines for fluid replacement in endurance exercise). The second important finding is that, in this situation of fluid overload, sodium supplementation may reduce the fall in serum sodium concentration. This suggests a potential role for sodium supplementation in the prevention of hyponatraemia when an athlete is drinking excessively. Further research is needed to investigate the role of sodium supplementation in ultradistance exercise in athletes maintaining neutral fluid balance, and also in the field situation of an actual race.