Article Text

Abstract
Objectives: To examine (a) return to competitive sport within 12 months of anterior cruciate ligament (ACL) reconstruction, (b) maintenance of competitive participation at follow up, and (c) the relation of the level of sports activity and competitive participation at follow up to subjective functional assessments. Also to address the incidence of continued competitive participation despite notable functional problems with the operated knee at 12 months and follow up.
Methods: All patients were competitive athletes before injury and had undergone ACL reconstruction by the transtibial endoscopic technique with either a bone-patellar tendon-bone or a multiple looped hamstring autograft. Evaluation was carried out a mean of 43 months (range 24–73) after surgery by a postal questionnaire in which the Cincinnati sports activity scale (CSAS) and Cincinnati sports function scales were presented in conjunction with closed questions on change in competitive level and the presence of complaints.
Results: Of 109 selected patients, 77 (71%) responded. At follow up, 62 of 77 patients (81%) reported that they had returned to competition within 12 months of surgery. Within the same time frame, 55 of the above 62 patients (89%) also claimed to have returned to the level at which they were competing before injury (or higher). At follow up, 30 of the above 55 patients (54%) reported to still be competing at this high level. Twelve of the above 55 patients (22%) also admitted to major problems with the operated knee at that time. The overall incidence of patients competing despite major functional impairment in the operated knee was 13 of 62 (21%) at 12 months and six of 47 (13%) at follow up. Thirty eight patients (49%) were active in sport at least four times a week at follow up (CSAS level 1), and, using Spearman’s rank correlation between CSAS scores and total sports function scores, r was calculated to be 0.44. Competitive and male patients had higher total sports function scores at follow up than non-competitive (p = 0.005) and female (p = 0.02) patients respectively.
Conclusions: The reported return to competition at the previous level, both within 12 months and at follow up, was high but as expected considering the standard of treatment, patient selection, and study exclusion criteria. Patients with few functional complaints maintained a high level of sporting activity, even after discontinuing competitive participation.
- anterior cruciate ligament
- athlete
- comeback
- functional assessment
- rehabilitation
- ACL, anterior cruciate ligand
- CSAS, Cincinnati sports activity scale
- CSFS, Cincinnati sports function scales
Statistics from Altmetric.com
- ACL, anterior cruciate ligand
- CSAS, Cincinnati sports activity scale
- CSFS, Cincinnati sports function scales
After the clinical diagnosis of an anterior cruciate ligament (ACL) rupture in a competitive athlete, reconstructive surgery is indicated primarily by the patient’s motivation to return to (a) competition at the previous level or (b) an athletic lifestyle involving functionally challenging activities that were previously impossible because of the ACL deficiency.1–4 Although return to competition and maintenance of an athletic lifestyle may be considered to overlap, they should be assessed separately in competitive athletes.
The successful return to competition at the previous level will for most athletes require the near absence of functional limitations. However, some continue to participate in functionally challenging activities, and even compete at a high level despite major functional complaints. Competing with such problems increases the risk of secondary injury,5 resulting in accelerated deterioration of knee function and progression of osteoarthritis.5,6 No adequate attempts have been made to identify the incidence of such behaviour, which should influence clinicians’ consideration of outcomes in terms of sports activity parameters.
Outcome data for heterogeneous samples of athletes receiving standardised treatment are scarce, and studies are needed to identify appropriate outcome variables. Interestingly, there is a lack of correlation between objective measurements of static stability and subjective assessment of functional limitations after reconstructive ACL surgery.7–9 Subjective functional assessments should be presented as outcome principal variables after ACL reconstruction, and the tools for such assessments should be tailored to assess the principal activities of interest to the patients.
Widespread use of tools with a lack of functional variables combined with objective measurements of static stability has introduced concerns about their validity with regard to outcomes in competitive athletes.5,10,11 The Cincinnati knee rating system is a comprehensive set of tools for assessing functional outcomes after knee ligament surgery and has been adequately tested for reliability, validity, and responsiveness.12,13 We therefore based our investigation on this system.
The primary objectives of our investigation were to examine the return to and maintenance of competitive participation, and the relation of sports activity and competitive participation to subjective functional assessments at follow up. An additional objective was to address the incidence of competitive participation despite appreciable functional problems in the operated knee.
As there was (coincidentally) a fairly even distribution of the sexes in the study sample, sex differences are examined in some key outcome variables.
Although previous studies have looked at return to competition14–17 and level of activity8,17,18 at follow up, these evaluations were based on heterogeneous samples of athletes subjected to assorted surgical and rehabilitative techniques. Furthermore, previous studies have not specifically investigated the maintenance of competitive participation or focused adequately on the incidence of competitive participation despite appreciable functional complaints in the operated knee.
METHODS
Patients
Patients were retrospectively identified from surgical logbooks dating from January 1994 to February 1998 and selected according to the criteria listed in table 1. Of the 109 patients selected, 77 (71%) responded within two months.
Inclusion and exclusion criteria
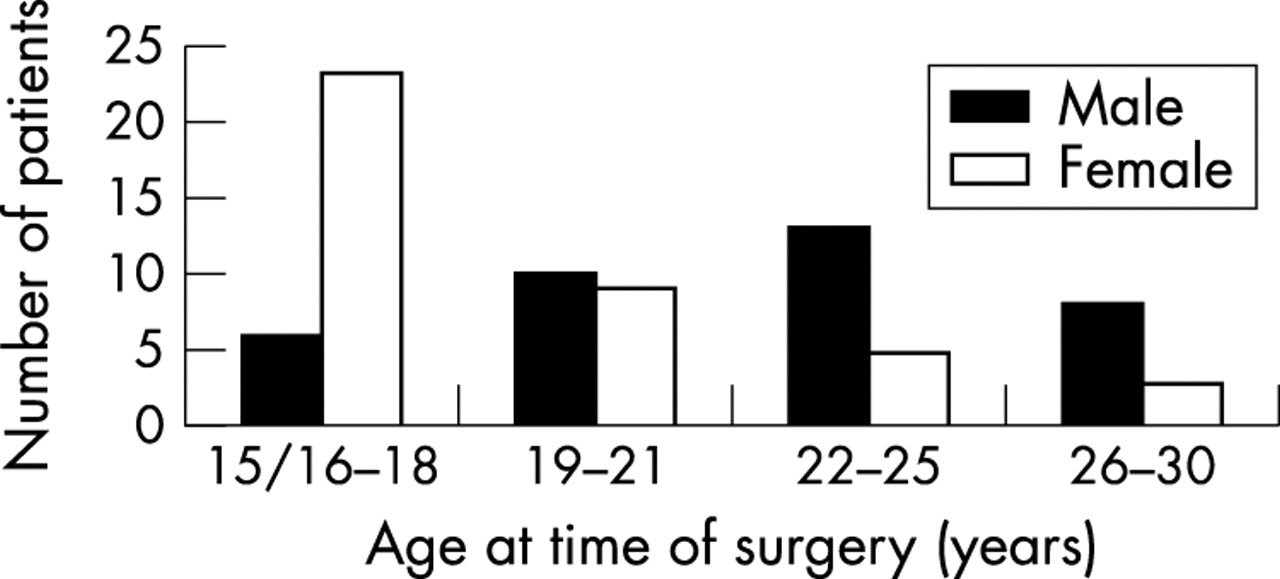
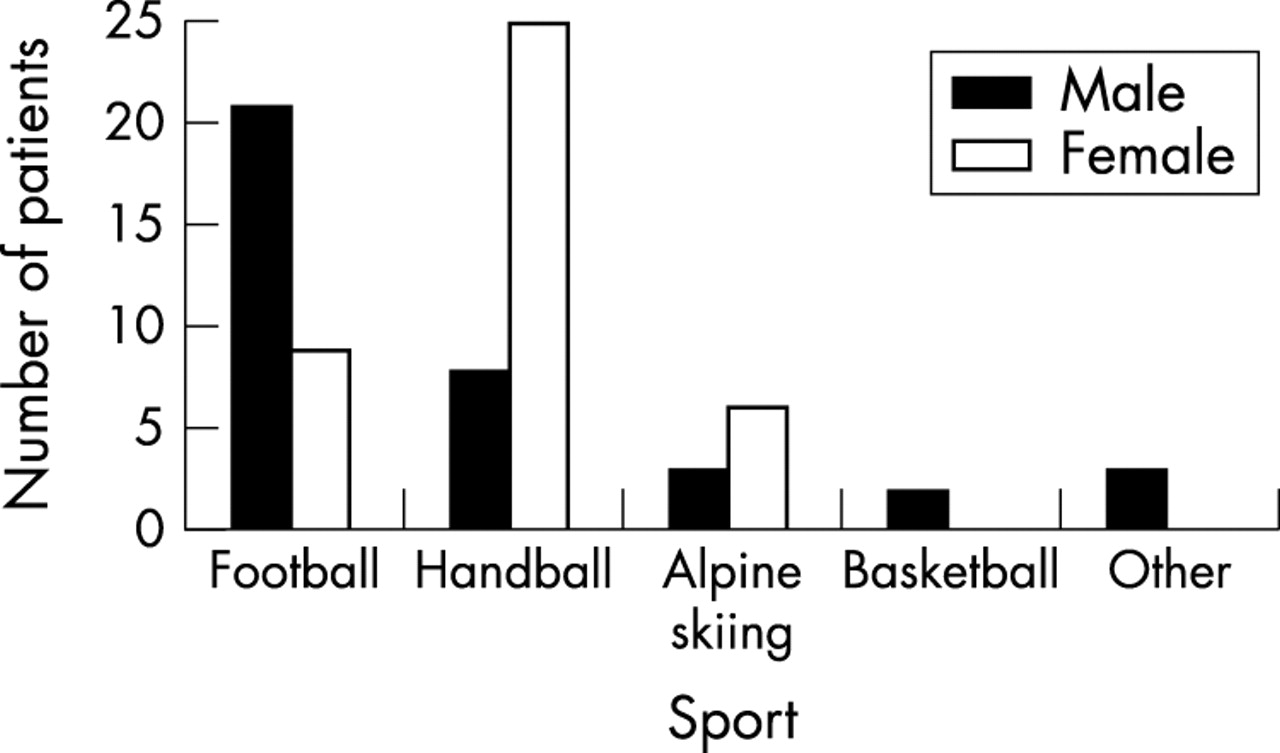
Table 2 summarises the key descriptors of this sample. The sample composition, in terms of the patients’ age and sex, illustrated in fig 1, is similar to that observed in the epidemiological study of ACL injuries in a similar population by Bjordal et al.16 Compared with female patients, male patients were older at the time of surgery (p = 0.0005), generally had more sporting experience (p = 0.005), and were competing at a higher level before injury (p = 0.002). Female patients had surgery significantly longer after injury (p = 0.001). Figure 2 shows the distribution of the sample according to the sport played at the time of injury. Five patients had suffered concomitant injuries to the medial collateral ligament, and these lesions were managed non-surgically by wearing a brace.19 Cartilage abnormality or evident concomitant cartilage damage was recorded in four patients, and 16 patients had meniscal lesions. Complete graft failure within the first 12 months occurred in one patient. All basic data, except general sports experience, were collected from the patients’ journals and the surgical reports. Non-responders were not significantly different from the responders in terms of these variables.
Key characteristics of the subjects studied

Frequency distribution according to sex and age at the time of surgery.

Frequency distribution according to sport at the time of the injury.
Treatment
All patients had an arthroscopically assisted reconstruction of the ACL, with an ipsilateral autologous bone-patellar tendon-bone graft (67 patients) or multiple looped hamstring tendon graft (10 patients). Two experienced surgeons performed all of the procedures and provided standardised follow up. All patients had extensive rehabilitation before the operation, and the rehabilitation after the operation followed the modern, accelerated protocol of Shelbourne and coworkers.20–22
Evaluation
The mean time from surgery to follow up was 43 months (range 24–73). At one month, contactable non-responders were encouraged by telephone to respond. Follow up evaluation was by a postal questionnaire which was completed individually by the patients. The questionnaire was constructed around the Cincinnati sports activity scale (CSAS; fig 3) and Cincinnati sports function scales (CSFS; fig 4).13 These scales were presented in conjunction with closed questions on change in level of competitive participation from before the injury, as well as the presence of notable symptoms 12 months after surgery and at follow up. Figure 5 presents the options provided for answering these questions. Table 3 summarises the structure and contents of the questionnaire.
Questionnaire structure and contents

Cincinnati sports activity scale. Reproduced, with permission, from Barber-Westin et al.13 The scale consists of 12 scores distributed across four levels. The three scores at each level correspond to three intensities of force to which the lower extremities are subjected, and the level indicates the frequency of participation in that type of activity.

Cincinnati sports function scales. Reproduced, with permission, from Barber-Westin et al.13

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Question on change in level of competitive participation compared with before the injury.
The term “competitive level” is defined by the classification of the competitions in which the athlete was participating, rather than performances at this competitive level.
Statistical analysis
Interval and ratio scale data were analysed using parametric statistical tools. Differences between groups were assessed using Student’s t test. Central tendency and spread in data are indicated by the mean followed by the standard deviation or the confidence interval.
Ordinal or categorical data were analysed using non-parametric statistical tools; in the assessment of differences between groups in terms of categorical outcomes, the χ2 test was used, and the Mann-Whitney U test was used in the assessment of differences in CSAS and CSFS scores.
Spearman’s rank correlation coefficients were used to assess quantitative relations between CSAS and CSFS total scores. Central tendency and spread in data are indicated by the median as well as the mean followed by the standard deviation. Statistical significance was set at p<0.05
RESULTS
Return to competition
Table 4 summarises the competitive status of the patients 12 months after surgery and at follow up compared with before the injury. There were no significant differences between male and female patients in terms of return to competition at 12 months, whether the overall return (p = 0.33) or return to the levels achieved before injury (and higher) (p = 0.59) were assessed.
Competitive status 12 months after surgery and at follow up
Maintenance of competitive participation
At follow up, the number of competitive patients had decreased significantly from 12 months (p = 0.013), as had the proportion of competitive patients competing at the level achieved before injury (p<0.001). Of the 62 patients that were competitive at 12 months, 46 were still competing at follow up. Of the 43 patients who were competing at their previous level without substantial functional problems at 12 months, 23 (52%) were still competing at the same level at follow up, seven (16%) had stopped competing for unrelated reasons, and three (7%) had developed functional problems that resulted in their retirement from competitive sport.
Assessment of functional limitation and (general) sports activity at follow up
Table 5 gives the frequency distribution of scores on the CSAS at follow up. Table 6 gives measures of spread and central tendency in the CSFS. Most patients scored themselves at CSAS levels 1 and 2 (69 of 77 (90%)), and most of these (38 of 69 (55%)) gave themselves the top score at their given level; men did so more often than women (24 of 35 (69%) v 14 of 34 (41%); p = 0.04). Table 7 gives Spearman’s rank correlation coefficients between sports activity scores and sports function scores at follow up. Competitive patients and male patients had significantly higher overall sports function scores at follow up than did not competitive (p = 0.005) and female patients (p = 0.02) respectively. Patients who were not competitive at follow up and reported having major impairment had significantly lower overall sports function scores (at follow up) than did those who were not competitive for other (unrelated) reasons (p<0.0001). The reduction, from 12 months to follow up, in the proportion of patients with problems with the operated knee who were competing at their previous level was not significant (p = 0.43).
Distribution of CSAS scores at follow up
Spread and central tendency of Cincinnati sports function scales scores at follow up
Spearman’s rank correlation coefficients between Cincinnati sports activity scale and Cincinnati sports function scales total scores at follow up
Incidence of continued competitive participation despite functional impairment of the operated knee
Table 4 gives these results.
The significance of the increased proportion of patients that were not competitive because of functional impairment from 12 months to follow up is not possible to assess in a meaningful way because of the small numbers.
DISCUSSION
The apparent lack of outcome data with appropriate outcome measures for competitive athletes prompted this investigation. Little emphasis has previously been placed on the immediate return to and maintenance of competitive participation, although these are important objectives for competitive athletes. In addition, investigators have typically presented results from samples that included chronic cases (surgery more than 12 months after injury), older patients (>35 years), and patients with pre-existing knee pathology.
Return to competition
The high rate of return to competition 12 months after surgery was expected, given the study inclusion criteria, the accelerated rehabilitation schedule, and the high motivation of the patients to achieve this objective. The latter is also reflected by the high proportion who managed to return to the competitive level achieved before injury. Although sex differences for return to competition within 12 months were not significant, the somewhat higher results for the male patients were in accordance with experience and were expected given the findings of Bjordal et al,16 who assessed outcomes in a similar population.
The sex differences can largely be attributed to the lower age of the female patients and the lower proportion of elite female athletes in the sample. For younger athletes, unresolved educational and/or occupational issues are more likely to present attractive “unrelated reasons” for discontinuing competitive participation.
Considering the rehabilitation schedule and the high motivation of the patients, a return to competitive sport at the previous level within 12 months is a realistic objective, and these results support this. Their motivation was discussed with patients before surgery, and the lack of such motivation resulted in exclusion from the study.
It may be argued that the athletes’ accuracy of recall of their status at 12 months is questionable. However, with an accelerated rehabilitation schedule, this is the time frame within which most competitive athletes will aim/expect to achieve a satisfactory return to competitive sports after an uncomplicated ACL reconstruction.
Maintenance of competitive participation
We considered maintenance of competitive status to be important. It is worth emphasising that two thirds of patients who discontinued their competitive career did so for reasons other than the injury. The lower maintenance for patients who managed the initial return to competition at their previous level was expected, given the greater demands (in general) of maintaining a competitive career at a high level and because any functional limitations would be magnified on return to the previous competitive level, compared with a lower competitive level (regardless of the previous level).
Incidence of patients continuing competitive participation despite functional impairment
The incidence was somewhat lower than expected from experience. The higher incidence reported 12 months after surgery than at follow up is probably part of a natural pattern of trial of functional capacity, but the small sample size makes this observation difficult to assess.
Notably, few of the patients who reported competing despite problems at 12 months were similarly competitive at follow up. The return to competitive status should be considered in the light of the incidence of such behaviour, although its significance, in particular over short periods, is largely unknown. One may hypothesise that the typical behaviour involves accepting some degree of discomfort and pain during the initial return to competitive activity; later the condition will either improve, allowing the level of competitive participation to be maintained, or deteriorate, forcing the patient to adjust his/her competitive participation, or even retire from competitive participation altogether.
Because of the small sample size, the significance of the relative reduction in the incidence from 12 months to follow up was difficult to assess. However, one may hypothesise that the typical behaviour involves accepting some degree of discomfort and pain during the initial return to competitive activity; later the condition will either improve, allowing the level of competitive participation to be maintained, or deteriorate, forcing the patient to adjust his/her competitive participation, or to choose to retire from competitive participation (in that particular sport) altogether.
Functional limitations and sports activity at follow up
Like other studies using similar surgical techniques and rehabilitative approach,16,22,23 the great majority of patients, by reporting very few functional limitations, perceived the outcome as satisfactory. In common with the study by Wiger et al,17 the high activity levels maintained by patients at follow up supported the validity of their subjective assessments of their functional limitations.
Patients may reduce their activity levels for many reasons other than functional impairment, reducing the relation between actual sports activity and the subjective rating of functional limitation. It was encouraging that patients who had discontinued competitive participation for reasons other than problems with the operated knee reported maintaining a highly athletic lifestyle, both in terms of the type of activity and frequency at follow up, indicating that surgery had in fact been appropriately performed in these patients.
Patients with major knee problems at follow up had a lower CSAS score mode, reflecting the reduced intensity of sports activity compared with that of those without such problems, which is logical.
We have not focused on the changes in sports activity and degree of functional limitation relative to the time from surgery to follow up, principally because of the small and somewhat unevenly distributed sample. The progressive changes in functional and sports activity variables for patients with major functional impairment, or with concomitant lesions at the time of surgery, would require a substantially longer follow up period and prospective study design.
The principal limitation of our study was the small sample size, which limited the scope for data analysis. Appropriate selection of patients, continued use of validated tools for assessment, and, preferably, data collection in a prospective fashion should reduce the ambiguity of results in future studies. Although the satisfactory outcomes of surgery in this population were as expected, appropriate outcome measures should be audited and discussed in a factual context rather than inferred from experience.