Article Text

Abstract
A number of different methodological approaches have been used to describe the inciting event for sports injuries. These include interviews of injured athletes, analysis of video recordings of actual injuries, clinical studies (clinical findings of joint damage are studied to understand the injury mechanism, mainly through plain radiography, magnetic resonance imaging, arthroscopy, and computed tomography scans), in vivo studies (ligament strain or forces are measured to understand ligament loading patterns), cadaver studies, mathematical modelling and simulation of injury situations, and measurement/estimation from “close to injury” situations. In rare cases, injuries have even occurred during biomechanical experiments. This review describes each research approach and assesses its strengths and weaknesses in contributing to the understanding and prevention of sports injuries.
- BIAD, boot induced anterior drawer
- ACL, anterior cruciate ligament
- CT, computed tomography
- MRI, magnetic resonance imaging
- anterior cruciate ligament
- injury biomechanics
- epidemiology
- prevention
- research methods
Statistics from Altmetric.com
- BIAD, boot induced anterior drawer
- ACL, anterior cruciate ligament
- CT, computed tomography
- MRI, magnetic resonance imaging
Research on injury prevention has been described by van Mechelen et al1 as a step by step process, in which information on the causes of injury is systematically collected and used to develop potentially effective intervention methods. One important goal is to map the different extrinsic and intrinsic risk factors that contribute to the susceptibility of an athlete to injury, as described by Meeuwisse.2 However, to develop specific injury prevention methods for a particular injury type in a given sport, it is important to describe the inciting event or mechanism of injury, as outlined by Bahr and Krosshaug.3 The latter conclude that a precise description of the inciting event is a key component to understanding the causes of any particular injury type in a given sport and emphasise the need to expand the traditional biomechanical approach to describing the inciting event. Although it may be important to have an exact and detailed biomechanical description of the injury, this is not always sufficient to develop effective prevention methods. According to Bahr and Krosshaug,3 a complete description of the mechanisms for a particular injury type in a given sport needs to account for the events leading to the injury situation (playing situation, player and opponent behaviour), as well as to include a description of whole body and joint biomechanics at the time of injury. Furthermore, to address the potential for prevention, the information on injury mechanism must be considered in a model that also considers how internal and external risk factors can modify injury risk.
The different components of the inciting event are not completely independent. Characteristics of the sports situation and athlete/opponent behaviour will of course influence whole body biomechanics as well as the joint or tissue specific loading. However, they represent different areas at which preventive measures can be introduced to reduce the risk of injury. If, for instance, freestyle skiers are injured in the landing after a specific trick, it would be possible to change the rules—for example, prohibit the specific trick—or to change the course profile—for example, remove the mogul in which they land. Alternatively, it could be possible to develop improved boot-binding release systems, but this would require a detailed biomechanical description of the injury mechanism.
A number of different methodological approaches have been used to describe the inciting event (fig 1). These include interviews of injured athletes, analysis of video recordings of actual injuries, clinical studies (in which the clinical findings on joint damage are studied to understand the injury mechanism, mainly through plain radiography, magnetic resonance imaging (MRI), arthroscopy, or computed tomography (CT) scans), in vivo studies (ligament strain or forces are measured to understand ligament loading patterns), cadaver studies, mathematical modelling and simulation of injury situations, or measurement/estimation from “close to injury” situations. In rare cases, injuries have even occurred during biomechanical experiments. The purpose of this review is therefore to describe and assess strengths and weaknesses of each of these research approaches to address how each of the methods can provide knowledge on the mechanisms of injury in sport that can be used to develop methods for prevention.
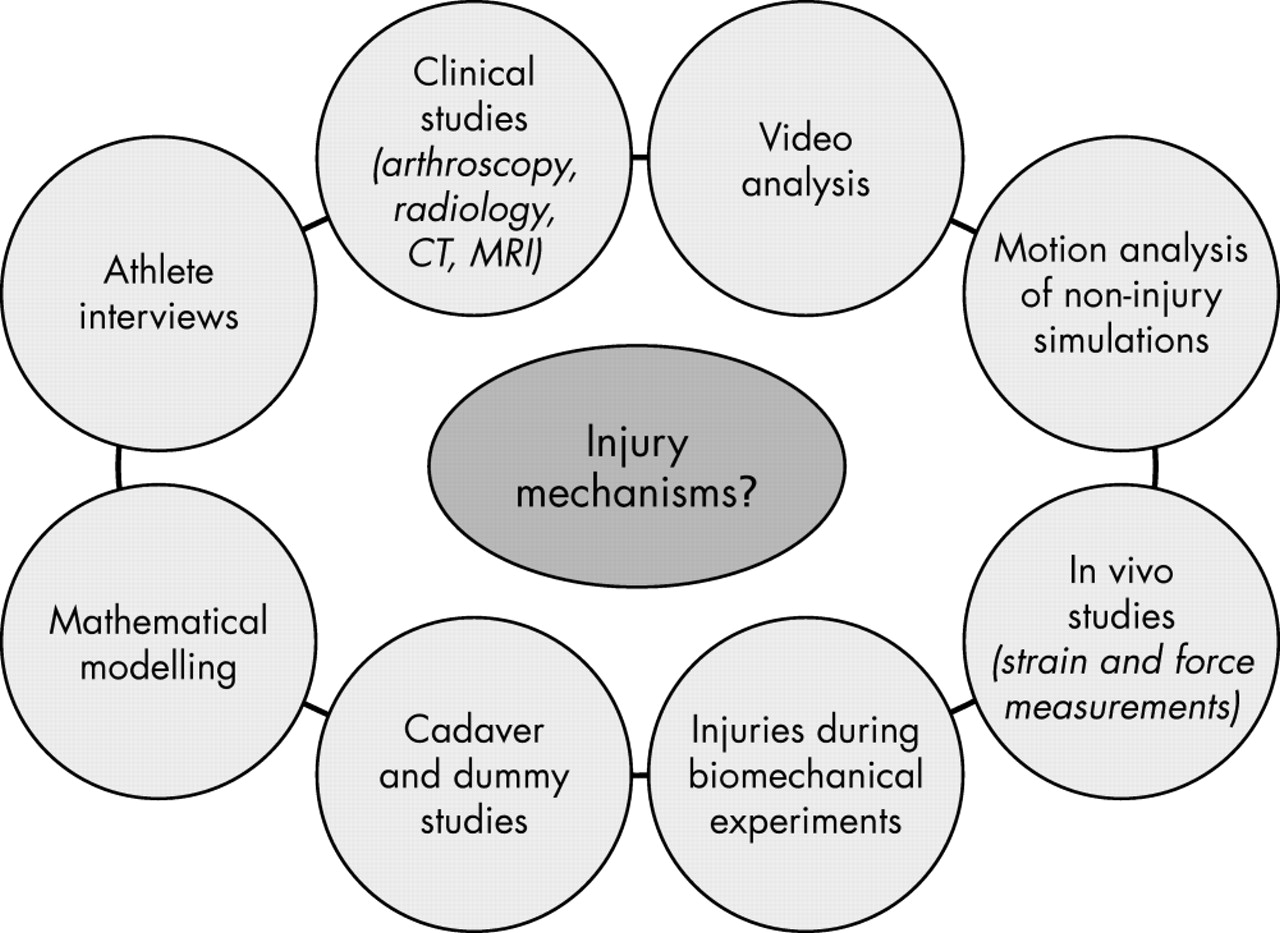
Research approaches to describe the mechanisms of injuries in sports.
ATHLETE INTERVIEWS
One of the most commonly used approaches in studying injury mechanisms is the description of the injury as reported by the athlete, coach, medical personnel, or others who witnessed the accident.4 We will term this approach “athlete interviews,” even if it is not always the athlete who is actually interviewed.4–14 The advantage of using this approach is that it is relatively easy to obtain data—for example, through a personal interview or a questionnaire. Information on injury mechanisms is therefore often collected as part of routine injury surveillance systems, by which it is possible to gather data on a large number of injured athletes. Such systems have been established in various sports, such as the National College Athletic Association (NCAA) Injury Surveillance System for US collegiate sports5 and similar systems in professional Australian rules football6 and professional football at the national team level (FIFA),7 international club level (UEFA),8 and national club level in various countries.9,15,16 Furthermore, a number of the injury surveillance systems established in alpine skiing resorts also routinely collect information on injury mechanisms.10,17,18
To use anterior cruciate ligament (ACL) injuries as an example, one important question is whether these occur without opponent contact or result from opponent contact. There are a number of examples of epidemiological studies that attempt to answer this question. For example, Arendt and Dick5 performed a five year evaluation of ACL injuries in collegiate men’s and women’s football (soccer) and basketball programmes using the NCAA Injury Surveillance System. They concluded on the basis of 367 cases that non-contact mechanisms were the primary cause of ACL injury for both sexes, but that the non-contact to contact ratio was higher in women than men (4:1 v 2:1 in basketball and 1.7:1 v 1:1 in football respectively). In two prospective cohort studies from Norwegian team handball with a total of 112 cases, Myklebust et al13,14 reported a non-contact to contact ratio of 16:1, and Strand et al19 reported a 2:1 ratio in a retrospective case series of 144 team handball players undergoing surgery for a suspected ACL injury.
The studies mentioned here and their widely differing results illustrate one of the limitations of the athlete interview approach—that is, the lack of precise definitions of the categories used when reporting data. Although it may seem intuitively easy to distinguish between contact and non-contact mechanisms, there is no universally accepted definition for these terms. Direct contact with the knee—for example, a hit to the lateral side of the knee—clearly falls into the contact category. Conversely, injuries without any form of opponent contact must be classified as non-contact. However, it is not clear how the question would be interpreted by a player who was pushed in the back or held by his shirt just before or at the time of injury. In fact, the papers mentioned did not report the definitions used. Olsen et al20 later suggested discrimination between injuries with direct contact (direct blow to the lower extremity of the injured player; thigh, knee, or lower leg), indirect contact (where the injured player is held, hit, or pushed in a body region other than the lower extremity), and non-contact (where there is no contact with other players). Depending on the results, the distinction between indirect and direct contact mechanisms could have important implications for prevention. This example illustrates the need to clearly explain to the athlete (or other person) completing the injury form the definitions used, and to detail the definitions used when reporting the results of the study.
Furthermore, the categorisation of injury mechanisms into predefined descriptions may result in incomplete or even erroneous interpretation—for example, if the categories are created to fit with a specific theory on the injury mechanism. Interestingly, in one study21 on ACL injuries in which the description of the injury mechanism was written down as stated by the patients, 17 different injury mechanisms were reported, whereas normally the number of categories is much fewer. Unfortunately, injury mechanism descriptions based on the athlete interview approach commonly use widely different terminology; categories and definitions are rarely provided and sometimes it seems somewhat arbitrary which variables are reported. There are examples of papers on ACL injury mechanisms that report on the sporting situation11,13,14,19,22 and others even report on detailed joint kinematics.23–25
Such detailed descriptions should be interpreted with caution if based on athlete interviews alone. One important limitation of the athlete interview approach is the ability of injured players to comprehend and recall what actually took place when they were injured. Injuries usually happen quickly and often involve several players, opponents, and teammates. It is therefore difficult to determine to what extent the injured athlete or the witnesses are able to assess the playing situation and, perhaps even more difficult, the biomechanical aspects of the injury mechanism. The description given may not even be the athlete’s own interpretation of the event, but be influenced by what he was told by others witnessing the event, his coach, parents, or teammates. It may be argued that a major injury is a landmark event in the life of an athlete. Even so, our recollection of a situation often changes with time, and recall bias is another possible source of error.26 In addition, the description may be “filtered” by the person completing the injury form, and the record may reflect his interpretation of the description—for instance, in the case of an athletic trainer or doctor taking notes for the medical record.
In other words, there are significant methodological limitations that must be borne in mind when interpreting the results from studies based on questionnaire data. It could even be argued that it is not possible to collect accurate and detailed information on injury mechanisms using this approach, thus limiting the ability to develop preventive measures.
However, for some injury types and sports where playing actions and injury mechanisms are easily categorised and the injury mechanisms are consistent, questionnaire data may provide an accurate description of the mechanisms, at least for the playing (sports) situation and athlete/opponent behaviour. For example, questionnaire studies from volleyball have clearly documented the mechanisms for ankle sprains. These mainly occur at the net as the result of landing on the foot of an opponent or a teammate after blocking or attacking.27 About half of all ankle sprains occur when a blocker lands on the opposing attacker’s foot, and about one quarter result from a player landing on his/her teammate’s foot when landing from a two or three man block. This information on the injury mechanisms was successfully used as the basis for an intervention study focusing on exercises to teach correct approach, take off, and landing technique when blocking or attacking.28 This example shows that data from athlete interviews can be important for developing prevention methods.
CLINICAL STUDIES
Another approach to understanding the mechanism of injury is to analyse the pathology of the injury and associated damage. For instance, MRI or CT scans of the head can diagnose the location of brain and skull damage accurately, and thereby form the basis for an estimate of the location and direction of the forces causing the observed damage. In the case of an ACL injury, the use of radiography,29 MRI,29,30 CT,31 or arthroscopy32 to obtain a detailed description of the pathology—for example, associated injury to the menisci or collateral ligaments, or localised cartilage injury, or bone bruises—can be used to predict the injury mechanisms. MRI studies after ACL injuries have reported a high prevalence of osseous contusions on the lateral femoral condyle and posterolateral injury of the tibia and soft tissue.29,33,34 On the basis of these findings, as well as the high prevalence of osseous contusion directly over the terminal sulcus of the lateral femoral condyle, Speer et al29 stated that valgus must have been a part of the injury mechanism, and suggested three different models to explain the pathological findings: (a) pivot shift injury of the posterolateral tibial rim and meniscus; (b) hyperextension injury of the anterolateral tibial rim and meniscus; (c) reduction after pivot shift event of the anterolateral tibial rim and meniscus. Studies investigating the associated joint damage after ACL injury may indeed be helpful in generating new hypotheses, and possibly rejecting others. However, the paper of Speer et al also illustrates that it is not possible to determine reliably the sequence of events leading to the observed findings on the basis of such studies alone. The essential question—and main limitation of clinical studies in general—is whether the damage occurs before, during, or as a result of the ACL rupture.
Another limitation of many of the studies using this approach to date is that they do not provide any other information about the injury situations causing the injuries, or are based on mixed samples of athletes from different sports and performance levels. This makes the pathology reported even more difficult to interpret. An exception is the study of Ferretti et al,35 a retrospective report on the surgical findings in 52 volleyball players with ACL injuries. This study also provided information about playing position, what sports specific action the players were performing when injured, as well as kinematics and stance phase. Serious injury to the medial collateral ligament was found in seven cases, indicating valgus loading. However, in 34 cases the only macroscopic injury visible was ACL rupture.
Although exact descriptions of joint pathology can be obtained from arthroscopy, MRI, and other imaging studies, an accurate prediction of the detailed joint biomechanics leading to injury is difficult. Information on joint biomechanics alone may not be sufficient to develop ideas for prevention. Therefore it may be that the most important role of data from clinical examinations is that they can be used to support or contradict observations from other methods, such as interviews of the injured athlete or analysis of video tapes of the incident. This requires a prospective approach in which data from all three methods are collected in a standardised way.
VIDEO ANALYSIS
Today, sport is an entertainment industry, and most major international and national competitions and leagues are taped and televised, in some cases even at the youth level. This represents an excellent opportunity to collect videotapes of sports injuries and analyse their mechanisms.
Surprisingly, until recently, very few researchers have used systematic analysis of video tapes of incidents to analyse injury mechanisms, despite the fact that the first video analysis study was published by Silver and Gill more than 15 years ago on serious cervical spine injury in rugby.36 To determine whether a change in the laws of the game was necessary or whether the existing laws were adequate to prevent neck injuries in rugby, their research was carried out by video recording several games of rugby and analysing the games later in slow motion to determine how injuries occurred. They found that most of the injuries occurred in the ruck and maul situation, and concluded that they were not due to bad luck but were caused by irresponsible actions. The laws of the game were being broken and not being enforced, indicating that stricter officiating could perhaps prevent injuries. Another early study using this approach is that of Ettlinger et al37 on ACL injuries in alpine skiing. They used kinematic information collected from videotapes of recreational skiers and described the “phantom foot” injury mechanism as the typical movement pattern resulting in injury. They even used this information to educate skiers on how to avoid dangerous behaviour, and were able to reduce the rate of ACL injuries by 62% among professional skiing instructors and ski patrols using a video based “awareness training” programme.
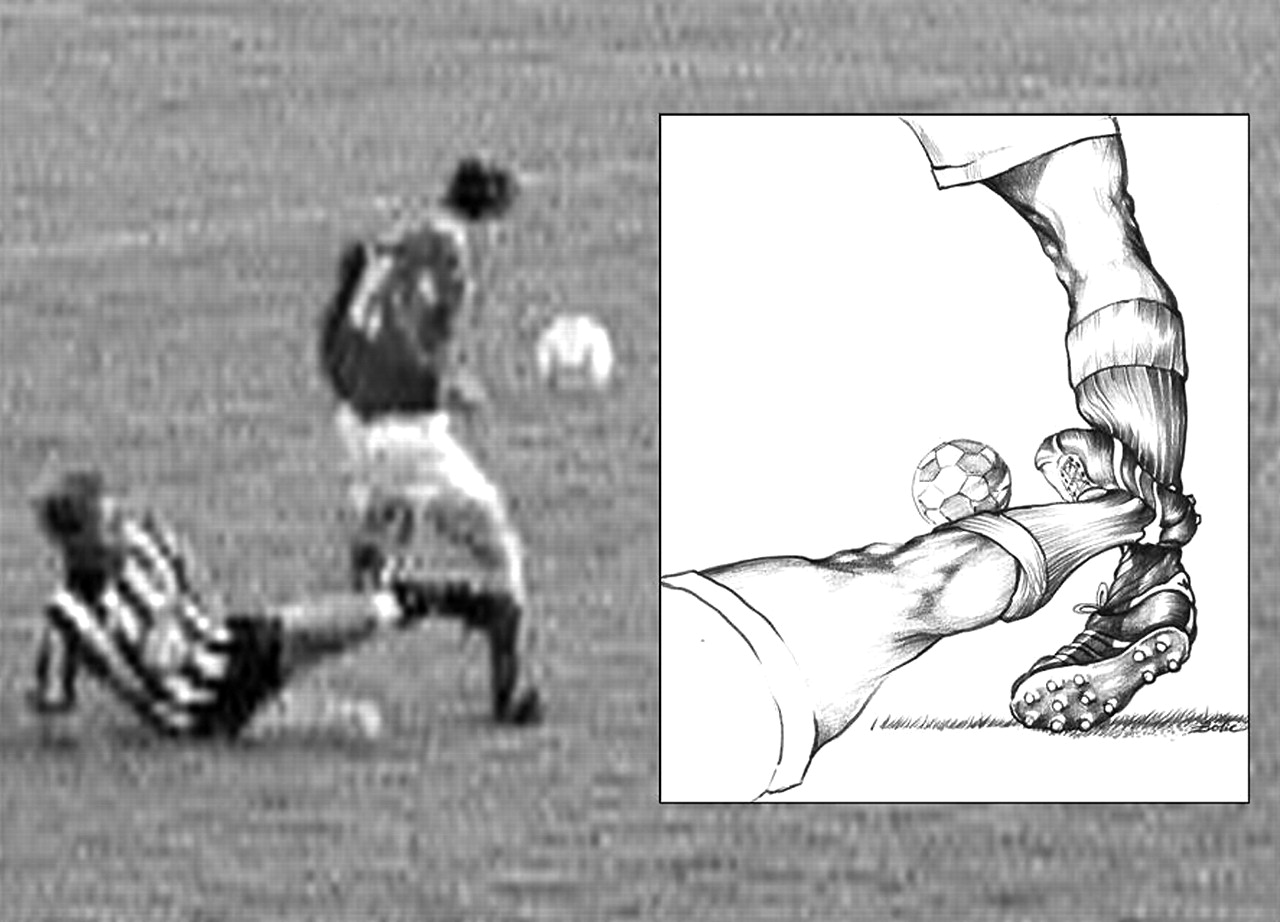
Both of these early studies illustrate that systematic video analysis of injuries can potentially contribute information on the sports situation and athlete movement patterns, which can be used directly to prevent injuries. Recently, there has been a surge of papers using a similar approach to study the mechanisms of different injury types in several sports.9,15,20,38–48 Our group9,15,38–41 and others44–48 have used video analysis to study the mechanisms of football injuries in a series of studies. These studies have mainly focused on describing the playing situation, athlete-opponent interaction, and refereeing, confirming results from questionnaire studies pointing to tackling duels and heading duels as high risk situations. Arnason et al15 point to an interesting observation: that the exposed player’s attention appeared to be focused away from the opponent challenging him for ball possession in 93% of the cases. However, a video based intervention study using “awareness training” modelled on the study of Ettlinger et al37 did not affect injury risk.49 Until now, whole body or joint biomechanics have been studied to a lesser degree in football injuries, but two recent studies by Andersen et al have examined the mechanisms of ankle9 (fig 2) and head41 injuries. For ankle injuries, the joint kinematics showed mostly supination trauma as expected. However, several of the incidents were triggered by an external medial force of the ankle (late tackle from the side) which brought the player out of balance, causing unexpected foot motion just before landing. This illustrates the importance of describing not only the joint specific biomechanics, but also the playing situation leading up to the injury. Similarly, another study showed that the most common injury mechanism for head injuries was elbow to head contact in heading duels.41 The study suggested that the elbow was used actively at or above shoulder level. Thus both of these studies suggest that stricter rule enforcement or even changes in the laws of the game could lead to a reduced risk of injury.9,41

Illustration of the main injury mechanisms observed from systematic video analysis of anterior cruciate ligament injuries in team handball, a plant and cut movement with the knee close to extension resulting in a valgus-external rotation collapse of the push off knee.20 Illustration reproduced with permission from Oslo Sports Trauma Research Center/T. Bolic.
Although video analysis has the potential to be a more detailed and reliable way of analysing injury mechanism than athlete interviews, current methods for estimating kinematics from uncalibrated video sequences are inadequate.50 Therefore, the video analysis approach has been more useful for describing the playing situation and athlete/opponent movements than detailed joint biomechanics, although a new model based, image matching technique has recently been described.50 To date, studies on the mechanisms for ACL injuries have only used simple visual inspection to extract joint kinematic information from video sequences (fig 3).20,37,42,51 This could potentially represent a significant source of error, as it is not known to what extent it is possible to interpret segment attitudes and estimate joint angles in three planes simply through visual inspection. Finally, these methods cannot produce continuous estimates of joint angles and positions, which are necessary for a detailed biomechanical analysis of the injury mechanisms—for example, joint angle time histories, velocities, and accelerations. In contrast, methods have been developed to estimate impact biomechanics for head injuries.43,52–54 McIntosh et al52 examined video tapes from head impacts that resulted in concussion in Australian rules football and rugby to obtain estimates of closing speed and head impact energy. Using a similar approach, Pellman et al43 later studied cases of concussions and significant head injuries from National Football League games to estimate the speed of impact from the game films. From these estimates, the situations were reconstructed in the laboratory using helmeted dummies to accurately measure the dynamics involved. In helmeted sports, it could even be possible to build accelerometers into the helmet to measure impact biomechanics directly in injury and non-injury situations and compare these data with the analysis of video recordings of the same incidents.
{kind=link}
{kind=link}
{kind=link}
Typical mechanism for lateral ligament injury in football as observed from systematic video analysis: opponent contact to the medial side of the leg, causing the player to put weight on an inverted ankle.9 Illustration reproduced with permission from Oslo Sports Trauma Research Center/T. Bolic.
An obvious limitation of the video analysis approach is the quality of the video recording—for example, the image quality, the resolution of the athlete of interest, and the number of views available. It is not known to what degree a two or three camera recording improves the kinematics estimate from visual inspection. However, a recent study by Krosshaug and Bahr50 indicates that additional camera views increase the accuracy of a model based, image matching technique for extracting human motion from uncalibrated video images. In addition, the viewing angle relative to the athlete will determine what variables are most reliable.50 An important challenge is to determine the exact point of injury. In studies of ACL injuries, one report claims that the “precise point of injury” could be determined,51 whereas another stated that finding the exact moment of ACL disruption was impossible.42
Another limitation, which must be kept in mind when interpreting the results, is that not all of the injuries reported by team medical personnel can be identified on the game tapes. In fact, about half of all injuries in football can be found on video.15,39 The proportion of identified incidents ranges from all of the head injuries, about half of ankle and knee injuries, but only one third of hamstring strains. For example, hamstring strains may be difficult to study because they are mainly non-contact in nature. They probably result from sprinting, turning, or rapid increases in speed, which not always result in immediate and obvious disability to the player or take place in camera view near the ball. For the injury types for which a significant proportion of the injuries cannot be found on the tapes, it is possible that the injury mechanisms for the missing injuries differ from the recorded ones—for example, they are non-contact and less “spectacular.” This also means that studies based on video analysis alone,46,55 without reliable medical information from the same matches, must be interpreted with caution. The completeness and diagnostic accuracy of the medical information is an important factor to consider when planning a video study.
Video analysis is a relatively new field, and most studies report sparsely on the methods used to standardise and assess the quality of the video analysis. In a study of ACL injuries in European team handball, Olsen et al20 used a group of three experts, who independently described the injury mechanisms based on a standardised form with predetermined variables and categories. Although the accuracy is not known, a comparison between the examiners showed that the reliability was good. They also verified that their sample of prospectively collected videos was representative, by comparing the descriptions of injury mechanisms obtained from interviews of a larger sample of athletes, including those that were captured on video.
However, a range of potential selection biases can result from the availability of video tapes. The video approach is more likely to be used for matches played by elite professional athletes, where TV coverage is regular, and less likely in amateur, female, and youth sports. However, in a study on rugby headgear at the youth level by McIntosh et al,56 as part of the study protocol they established a system to video record a representative sample of games to study the injury mechanisms. Moreover, training videos are often not available, and the injury mechanisms in training and match play may differ, as we would expect there to be less aggressive and foul play in training. Finally, most video analysis studies only describe events and situations leading to injury. Unless there is a representative control sample of non-injury situations, it cannot be determined if the characteristics of the injury situations are different from what normally takes place without resulting in injury. The assessment of the non-injury situations should, if possible, be carried out in a blinded fashion, although this may be difficult in some cases—for example, for ACL injuries—where an obvious valgus collapse follows many of the ruptures.20
In conclusion, analysis of video recordings of actual injuries can provide detailed descriptions of the mechanisms of sports injuries. However, studies must be planned to obtain representative video samples, and the accuracy of the methods can be questioned, especially the ability to describe detailed joint biomechanics.
LABORATORY MOTION ANALYSIS
In contrast, the strength of laboratory motion analysis is that it is possible to estimate kinetics and kinematics with much greater precision than is possible from analysing video recordings. However, injuries cannot be replicated in the laboratory for obvious reasons, and studies using motion analysis are therefore generally designed to mimic typical injury situations. For example, several laboratory studies have recently investigated side step cutting or jump landings in relation to non-contact ACL injuries.57–61 They have aimed to study factors believed to be important in the different causation hypotheses—for example, by comparing knee flexion angles,62–66 electromyographic activation patterns,63,65,67 or net joint kinetics between men and women.58,59,68,69 However, although it is possible to quantify the motion patterns for movements that are assumed to be similar to the situations in which injuries mainly occur,5,20 it is difficult to predict to what extent the joint dynamics are in fact comparable. Unfortunately, laboratory and game biomechanics have not so far been compared. However, in order to create more “match-like” situations, different research groups have tried to simulate the game setting—for example, by introducing unexpected cutting61,70 a static defender,57 or catching a ball while landing.71 All of these factors proved to increase joint loading, indicating that there are indeed significant differences between controlled laboratory trials and match situations that may lead to injury.
There are also other problems associated with traditional motion analysis techniques, which introduce errors in the estimates—for example, skin movement artefacts,72,73 identification of bony landmarks,74 and signal noise.75,76 Key variables related to ACL injury mechanisms such as knee internal/external rotation and rotation moments have proved to be unreliable in high impact sporting motion.72 Similarly, tibia to femur translation in a sporting event is too small to be measured with available imaging techniques based on surface markers.72 Also, the standard net joint kinetics approaches, without the additional use of, for example, sophisticated mathematical models or results from cadaver studies, is incapable of estimating ACL force. Interpretation of the results is therefore troublesome in the sense that it is difficult to predict to what extent, if at all, the observed mechanics exposes the athlete to increased risk of injury.
One approach to assessing the relation between a particular movement pattern (as measured through laboratory analysis) and injury risk is to couple motion analysis with a prospective registration of injuries. One could even introduce an intervention programme designed to change biomechanics and reduce injury risk. Hewett et al77 observed a significant decrease in peak forces and knee adduction/abduction moments in a group of 11 female volleyball players before and after four weeks of plyometric training. The same group later applied this programme to a group of 366 female high school athletes and found that knee injury risk was reduced, indicating that reducing peak landing forces or varus/valgus loading is effective in preventing knee injuries.78 Further support for this hypothesis can be found in a recent prospective study among 205 female high school athletes, which shows that athletes who ruptured their ACL during the subsequent season displayed appreciably different knee posture and loading (greater abduction angle and moment, higher ground reaction force) in a pre-season laboratory jump/landing task compared with those who did not.60 Although this is not a study of the injury mechanisms per se, it establishes increased dynamic valgus and high abduction loads as risk factors for injury among female athletes. In this way, it supports the valgus mechanism described by Olsen et al20 from video analysis of ACL injuries in team handball. Taken together, these studies show that laboratory motion analysis can provide relevant information for understanding the mechanisms of sports injury.
IN VIVO STRAIN/FORCE MEASUREMENTS
In vivo studies of strain or forces represent another approach that can provide useful information on tissue loading in situations with similar characteristics to injury situations, and thus perhaps also relevant for injury. Some of the most utilised methods are strain gauges—for example, the Differential Variable Reluctance Transducer79—and buckle transducers80 or fibre optic sensors81 for measuring force. Lately, non-invasive methods such as ultrasonography82 and MRI83 have also shown their potential.
However, owing to the technical challenges,79 the ability to perform sport specific movements using invasive techniques is at present limited. In addition, non-invasive studies are limited in that they cannot be applied in a sport relevant situation. In vivo studies have therefore generally focused on, for example, muscle-tendon biomechanics and rehabilitation, rather than injury mechanism research. An exception is the study by Cerulli et al,84 in which ACL strain was measured in an athlete performing a one legged maximal jump on to a force plate. However, methodological limitations—for example, impingement problems84 preventing the athlete from extending the knee, and wiring, preventing more than one step—prevent this from reflecting the real sporting situation. This was also indicated by their findings, as the maximal strain was only slightly higher than measured while the athlete was standing still on one leg.
INJURIES DURING BIOMECHANICAL EXPERIMENTS
For obvious ethical reasons, one cannot replicate injury situations in a experimental study on live subjects. In a few rare cases,85,86 accidental sports injuries have occurred during research experiments. In a study set up to assess the biomechanics of weight lifting, Zernicke et al85 videoed an Olympic weightlifter rupturing his patellar tendon in a clean and jerk. Net joint kinetics were determined, and the tensile loading of the patellar tendon before and during tendon trauma could be estimated. It was concluded that the maximal tendon stress was considerably greater in sporting situations than in a static setting. In the study of Barone et al,86 kinematic input to a simulation model was collected at the landing from a jump on a ski slope. The researchers intended, from the motion obtained, to simulate the so called boot induced anterior drawer (BIAD) injury mechanism. Unfortunately, one of the skiers accidentally tore his ACL during one of the landings in a typical BIAD injury. It was then possible to evaluate electromyographic signals as well as the kinematics and provide a much more precise description of the injury mechanism than otherwise would be possible. The results showed that the injury seemed to take place at a much later stage than expected.
Of course, studies in this category are both rare and undesired. We must therefore consider other approaches for gaining insight into the injury mechanisms. However, although it is difficult to draw general definite conclusions from such single-case studies, they do provide extremely valuable insight into the injury mechanisms when they do occur.
CADAVER AND DUMMY STUDIES
Cadaver studies investigating the anatomy and function of joints and ligaments are numerous.87–89 A common approach has been to measure the kinematics before and after cutting one or more ligaments of, for example, the knee.90,91 From such studies, gross estimates of ligament function can be obtained, classifying the ligaments into “primary restraints” and “secondary restraints”, depending on their effect on joint angular or translational motion. It is also possible to mimic the assumed injury mechanism and load an intact cadaver joint to failure, to see if the mechanism produces the intended pathology. A technically more sophisticated approach is the use of strain gauges or force transducers to assess ligament function under different loading conditions. The classic study of Markolf et al92 of combined loads that generated high ACL forces has provided valuable insight into ACL function. Similarly, Berns et al93 also studied combined loading, but measured strain instead of force. Bahr et al94 measured the forces in the anterior talofibular ligament and calcaneofibular ligament as well as the motion in the tibiotalar and subtalar joints during aggressive loading, using buckle transducers. The results confirmed that the anterior talofibular ligament acts as the primary restraint in inversion, during which injuries typically occur.
Although these studies are important in understanding ligament function, their value in injury mechanism research is limited, as lower loads cannot be extrapolated to failure level with confidence.93 Unfortunately, the validity of cadaver studies is also often hampered by the fact that specimens are old and/or not representative of an athletic population.95 In addition, the freezing and thawing process reduces the ultimate load of the tissue.96
In most studies, muscular support is lacking, although some cadaver studies has also simulated muscle forces in, for example, the quadriceps and/or hamstrings.97–99 DeMorat et al98 recently conducted a controlled cadaver study in which it was demonstrated that aggressive quadriceps loading in 20° flexion could actually take the ACL to failure, by applying a 4500 N force within one second. A mean anterior displacement of 19.5 mm was measured during the violent quadriceps contractions, and more than half of the knees sustained gross ACL injury at the femoral insertion level. Unfortunately, even in studies in which muscle forces are simulated, the actual muscle force patterns that contribute to the joint dynamics in a real injury situation are unknown, and would probably be difficult to reproduce in such a set up even if they were known.
Another approach used in sports injury research is the use of dummies or physical models, which are well known in car crash testing. Such dummies—for example, the Hybrid III family of dummies—have excellent biofidelity, and can be instrumented with, for example, load sensors and accelerometers.100 As mentioned above, this approach has been used in laboratory research on the mechanisms for head injury43 and to test protective equipment such as helmets.101 As dummies are passive—that is, they lack muscles—the types of injuries that can be investigated using this approach are obviously limited. Nevertheless, in those situations in which the assumptions are met, dummy studies have proven useful.
MATHEMATICAL MODELLING
Sophisticated mathematical modelling and estimation of “close to injury situations” or simulation of injury situations has become increasingly popular. Some models take into account whole body dynamics,102–104 whereas others model only, for example, the knee joint105 or different aspects of the ACL.106 Through such models, it is possible to establish the relation between, for example, the measured kinematics, ground reaction forces, and ACL force.104 Hence, motion analysis using the traditional inverse dynamics approach can be taken to the next level with such approaches, although the challenges are significant.
The advantage of the simulation approach is that one can study different injury mechanisms in a computer environment, thus avoiding any hazard to athletes. Depending on the models, one can study cause-effect relations, for example, between neuromuscular control and knee loading,102 or intercondylar geometry and ACL impingement.105
McLean et al107 developed a three dimensional simulation model for side stepping that could predict body kinematics, ground reaction force, and three dimensional joint forces and moments with relatively good accuracy. Anterior-posterior force could also be calculated from this model. In their next study,102 Monte Carlo simulations of neuromuscularly perturbed motion were performed based on data from 10 male and 10 female subjects. It was found that the mean estimates of peak anterior drawer force were never positive—that is, the ACL was not loaded in the recorded situations, and also rarely in the simulations. As stated by McLean et al, because the muscle activation patterns in the model were not measured but predicted, it is expected that for individual muscles they will not perfectly resemble the true activations. An alternative approach could have been to use (scaled) electromyography as input.108,109 Another shortcoming in this model was the lack of realistic modelling of joint contact surface—for example, tibial plateau slope—which has been shown to be important for ACL loading.103
Owing to the complexity of anatomy and neuromuscular control, a sophisticated mathematical simulation model will necessarily have to rely on assumptions and simplifications to deal with the inherent undeterministic nature of the equations describing the dynamics. Because of this, a more complex model may be able to reproduce the measured kinematics more precisely, but the ability to predict new—for example, injury producing—situations may possibly suffer.102
The fact that an injury model nearly always needs to be validated, either in a non-injury situation or in vitro, clearly adds a degree of uncertainty to its use. Still, the biggest challenge is probably how to verify that the simulated injury pattern actually resembles what is experienced in real life. This is illustrated well with the experiment of Barone et al.86 If the injury had not occurred during their BIAD experiment, chances are that a “solution” not present in the real world could have been found, because the observed injury kinematics differed significantly from all the other non-injury ski jump landings.
ASSESSING THE EVIDENCE
As seen from the description of the various research approaches, evidence relevant for understanding the mechanisms of sports injury can be obtained from widely different methods and study designs. Therefore the traditional evidence hierarchy110 cannot be applied in this setting. Important insight can be gained from studying the events preceding (for example, the velocity at impact, the playing situation), at (for example, the loads), or after (for example, the associated joint damage to the knee) the point of injury. In addition, we can learn from similar situations that did not lead to injury—for example, by studying the loading patterns in a side step cutting manoeuvre in the laboratory or in a match situation. Laboratory studies generally have better potential for accurate measurements, but it is difficult to predict to what extent the results are valid for actual injury situations. It is also necessary to expand the traditional biomechanical approach to describing the inciting event, if the objective is to prevent injuries.3 A complete description of the mechanisms for a particular injury type in a given sport needs to account for the events leading to the injury situation (playing situation, player and opponent behaviour), as well as to include a description of whole body and joint biomechanics at the time of injury.3
It is obvious from the different research approaches used that no single method exists that can provide a complete description of the injury mechanisms in sport. Consider as an example a popular hypothesis for non-contact ACL injuries in ball/team sports: the quadriceps drawer hypothesis.111 According to this, the patellar tendon force acts as an anterior drawer that may rupture the ACL. This hypothesis is built on several underlying premises:
-
force is transmitted through the patellar tendon as the ACL ruptures;
-
the patellar tendon angle to the long axis of the tibia results in an anterior force on the tibia when the tendon is loaded;
-
the patellar shear force must be larger than the ultimate ACL strength plus other forces acting as agonists with the ACL;
-
the loading rate must be such that the ligament rather than the bone fails.112
These premises can be studied with different approaches. For instance, through cadaver experiments92 and in vivo studies,113 we know that knee flexion must be approximately 30° or less to enable anterior shear forces through the patellar tendon from a quadriceps contraction. Although the precision may limit the usefulness of athlete interviews or video analysis, it is possible to obtain important information on key factors—for example, flexion angle estimates.20,42,51 To achieve greater accuracy, laboratory studies can be used to measure joint angles,59,65,69 muscle activation patterns,114,115 and joint loading.57–59,69,116 However, as it is not known how well such experiments correspond to the actual injury situations, at what point an injury would occur, or even how ACL loading relates to the estimated net joint kinetics, the validity of evidence from such studies can be questioned. Cadaver studies, on the other hand, can examine directly how the ACL is influenced by the quadriceps force, as shown by, for example, DeMorat et al.98 However, the relevance of this study to actual non-contact ACL injuries was questioned, as a mathematical modelling approach showed that the experimental set up did not replicate the dynamics involved in a sporting situation.102 Mathematical models can potentially test all the implicated premises. However, again their relevance can be questioned, as such methods rest on data obtained in the laboratory as input for the simulations. If this is the case, the simulations may also be substantially different from what is actually occurring in a real injury situation. Mathematical models must also be extensively validated before their results are of value, which can be achieved using one or more of the categories: cadaver studies, motion analysis studies, and in vivo studies.
What is already known on this topic
Sports injury mechanisms cannot be studied using direct experimental techniques. Other possible approaches are: athlete interviews; clinical studies (radiography, MRI, and CT); video analysis; laboratory motion analysis; in vivo strain/force measurements; injuries during biomechanical experiments; cadaver and dummy studies; mathematical modelling.
What this study adds
-
A complete description of the mechanisms for a particular injury type in a given sport needs to account for the events leading to the injury situation (playing situation, player and opponent behaviour), as well as include a description of whole body and joint biomechanics leading up to, and at the time of, the injury.
-
For most injury types, as no single research approach is adequate in terms of validity, accuracy, and completeness of information provided, it is necessary to combine a number of different approaches to describe the mechanisms fully.
This example is used to illustrate why, in many cases, it is necessary to combine different approaches to provide results that are both valid and accurate. Combining evidence from separate studies using different approaches is valuable, but differences in the experimental set up or study design may prevent comparison of the findings from one study with those of another. However, there are examples of studies that have successfully combined different approaches in one study. As previously mentioned, Pellman et al43 in their study on head injuries in American football achieved greater validity and accuracy by combining video analysis and a dummy study, than if such studies were performed separately. Likewise, Olsen et al20 combined athlete interviews and video analysis to increase the validity of the video analysis. Unfortunately, clinical or MRI findings of additional knee joint damage that could provide further information to interpret loading patterns were not reported in this, nor in any of the other studies that included video analysis.
RECOMMENDATIONS
Injury mechanisms can be described using different research approaches with a focus on different elements of the inciting event, and suggestions for preventive measures may originate from each category. It is therefore important to investigate all aspects of the injury mechanism. We have reviewed eight different research approaches to the study of the mechanisms of injuries in sport, each with its possibilities and limitations. For most injury types, one research approach alone will not be sufficient to describe all aspects of the injury situation, and it is therefore necessary to combine a number of different research approaches to describe the mechanisms fully. For example, relevant combinations of research approaches that could provide a broader and more precise understanding could be combining athlete interviews, video analysis, and clinical studies, or combining video analysis and cadaver/dummy/mathematical simulation studies.
REFERENCES
Footnotes
-
Competing interests: none declared