Article Text

Abstract
Objective: To determine whether quantified, auditable records of functional rehabilitation can be generated using subjective assessments of players’ performance in fitness tests routinely used in professional football.
Method: Ten sequential test elements grouped into three phases (fitness, ball and match skills, match pace football) were used to monitor players’ functional recovery from injury. Physiotherapists subjectively assessed players’ performance in each test element using a six point subjective rating scale. Satisfactory performance in each element of the assessment programme added 10% to the injured player’s recovery score. Daily recovery scores for injured players were recorded against the time spent in functional rehabilitation.
Results: Rehabilitation data for 118 injuries sustained by 55 players over two seasons were recorded. The average time in functional rehabilitation depended on the time spent in pre-functional rehabilitation and the nature and location of injury. Benchmark functional rehabilitation curves (y = mln(x) + c) were developed for thigh (n = 15) and lower leg (n = 8) muscle strains and knee (n = 7) and ankle (n = 9) ligament sprains (R2 = 0.95–0.98).
Conclusions: A structured, quantified rehabilitation programme based on routine fitness and skills exercises and a graded subjective assessment of performance provides an auditable record of a player’s functional recovery from a range of lower limb injuries and a transparent exit point from rehabilitation. The proposed method provides a permanent record of the functional rehabilitation of players’ injuries and evidence based data to support management’s return to play decisions.
- football
- functional
- rehabilitation
- injury severity
- return to play
Statistics from Altmetric.com
Injury is a major risk for professional athletes, and for athletes returning to competition after injury the risk is even greater. Those in charge of these athletes therefore have a responsibility to implement risk management strategies1 that will minimise the incidence and consequences of injury2 and ensure that injured athletes are effectively rehabilitated. A football player’s overall rehabilitation can be divided into two stages: pre-functional (treatment and recovery) and functional.3 Pre-functional rehabilitation begins with the immediate treatment of an injury through PRICE therapy (protection, rest, ice, compression, and elevation), immobilisation, and the use of non-steroidal anti-inflammatory drugs.4 The injury is progressively mobilised during treatment using non-weight-bearing and partial weight-bearing exercises5,6 in order to recover range of movement,7 muscular strength, and power.8 Functional rehabilitation, which involves full weight-bearing and sport specific exercises, begins when the team doctor considers that pre-functional treatment of the player’s injury has been successfully completed.4
In most occupations, an employee sustaining an injury at work is rehabilitated by doctors acting independently of the employer, and the employee’s own doctor normally determines when he or she is fit to return to work. However, in professional team sports, medical personnel employed by the club usually carry out the rehabilitation of injured players, and sometimes non-medical personnel employed by the club are involved in return to play decisions.9 This situation creates an ethical dilemma because, if personnel employed by the club make decisions on when injured players return to full team training and competition, these decisions could be influenced by short term commercial interests, which may conflict with players’ longer term health interests. In this context, Waddington and Roderick10 (p 118) commented: “if the team doctor and physiotherapist are agents of the club, how can they simultaneously act as agents for, and on behalf of, the individual player as patient?”
A consensus statement11 identified criteria that should be confirmed at a satisfactory level before an injured athlete returns to play; these criteria included the status of anatomical and functional healing and the restoration of sports specific skills. The statement, however, did not identify what a satisfactory level was or how it should be determined. A number of systems have been developed for the assessment of clinical outcome from treatment of knee injuries,12 of which the Cincinnati knee rating system,13 comprising two subjective scales—the Cincinnati sports activity scale and the Cincinnati sports function scale—appears to be the most appropriate for sports participation. The Cincinnati sports activity scale defines four frequencies of sports participation (none; 1–3 times/month; 1–3 times/week; 4–7 times/week) and three levels of intensity for each frequency of participation (no running/twisting/jumping; running/twisting/turning; jumping/hard pivoting/cutting). The Cincinnati sports function scale defines three types of sports activity (straight running; jumping/landing on affected leg; hard twists/cuts/pivots) and four levels of performance for each activity (not able to do; definite limitations/half speed; some limitation/guarding; fully competitive). Although these scales have been tested on patients returning to competitive sports after major injuries,13,14 they are not designed for the day to day assessment of rehabilitating professional athletes. Beardmore et al9 reported that New Zealand rugby union players were not always subjected to fitness tests before their return to play and stated (p 28): “it seems that rugby union has been placing greater emphasis on clinical recovery and anatomical healing than the ability of an injured part to withstand the stresses and demands of the sport”. A survey of English professional football showed that, although most clubs provided adequate medical facilities and personnel to rehabilitate injured players,15 the provision of an evidence based, auditable trail of a club’s return to play criteria for injured players was not an essential element of the rehabilitation process.
The incidence of injury in professional football is high16 (competition: 17–36 per 1000 player-hours; training: 1.5–6.5 per 1000 player-hours), with strains, sprains, and haematomas of the lower limb the most common acute injuries.17–20 The average severity of injuries ranges from 15 to 24 days,18–20 and recurrences account for 20–25% of injuries.16 Football is a physically demanding sport which involves activities such as running, jumping, turning, passing, shooting, heading, and tackling, with players covering 5–17 km per game.21,22 These activities place great demands on muscles, tendons, ligaments, cartilage, and bone, and, if these tissues are overloaded beyond their capacity to adapt, an injury will occur. Training therefore focuses on improving the body’s ability to withstand stresses during these critical activities by using aerobic and anaerobic exercises to develop fitness and football specific activities to extend ball and match skills.21,23–26
Enforced inactivity through injury reduces players’ physiological capabilities.27 Therefore functional rehabilitation programmes are designed so that players regain their pre-injury levels of fitness. Functional outcome measurement should quantify players’ performance capabilities and verify that an appropriate exit point from rehabilitation has been reached. Ekstrand28advocated a controlled rehabilitation process with players regaining full range of movement, coordination, and at least 90% of their muscle strength before returning to team training and competition. Unfortunately, return to play criteria at most clubs are not transparent. Fuller and Hawkins29 (p 149) proposed that physiological profiles of players could be used as benchmarks against which to assess players’ rehabilitation and “to provide records to demonstrate that players have been passed fit and have not been subjected to undue risk by an early return to play”.
The aims of the present research were to determine whether quantified, auditable records of injured players’ functional rehabilitation could be generated using subjective assessments of players’ performance in fitness tests routinely used in professional football and to assess whether benchmark functional rehabilitation curves could be generated for the most common lower limb injuries.
METHOD
A cohort of 55 professional football players employed by a club competing in the English Premiership during the 2001/02 and 2002/03 seasons gave written consent to take part in the study. The club’s medical team included a full time doctor and four full time physiotherapists, of which three were chartered physiotherapists. At least one of the medical team was always available to provide treatment for players injured during training and competition. Injuries were recorded in accordance with the protocols prescribed by the Football Association.20 An injury was defined19 as “any injury that prevented a player from taking a full part in training activities typically planned for the day and/or match play not including the day on which the injury was sustained”. An injury was reported as a recurrence based on the judgment of the clinician assessing the injury, taking into account the individual structure injured and the player’s previous medical history associated with this structure. Absences due to illness and non-football related medical conditions were not included in the study. Match and training exposures were recorded for each player, and incidences of injury, together with 95% confidence intervals, were reported as the number of injuries per 1000 player-hours of exposure.
During rehabilitation, players typically received four hours of treatment a day, seven days a week, from the medical staff. Players progressed from the pre-functional to the functional stage of rehabilitation when they were pain-free, the team doctor confirmed tissue healing was complete, and they were capable of undertaking full weight-bearing exercises.3,30 During functional rehabilitation, players were assigned to one of the club’s physiotherapists, who were responsible for players’ rehabilitation programmes and daily assessments. The functional stage of the rehabilitation programme comprised 10 sequential test elements grouped into three phases:
-
Phase I, fitness elements: F.1, endurance; F.2, speed-endurance; F.3, speed; F.4, power; F.5, agility.
-
Phase II, ball and match skill elements: S.1, basic ball skills (short passing, kicking, half volleying, volleying); S.2, advanced ball skills (long passing, kicking, half volleying, volleying); S.3, basic match skills (dribbling, tackling, heading, juggling); S.4, advanced match skills (crossing, shooting, ball control, defending).
-
Phase III, match pace football element: M.1.
A range of individual exercises, described by Bangsbo,21 Rosch et al,24 and Hawkins,25 was used for each of the fitness and skills elements. These exercises were used routinely by the club for team fitness and skills training, and each player’s benchmark performance in the exercises was measured at the beginning, during, and end of the season using the performance criteria specified in these publications.21,24,25 Player performance in an exercise was assessed during functional rehabilitation by the responsible physiotherapist using a subjective six point scale that took into account the player’s normal uninjured capabilities: 0, player unable to continue; 1, poor; 2, moderate; 3, good; 4, very good; 5, excellent (equated to the player’s benchmark standard when uninjured). Physiotherapists involved in the assessments discussed and agreed the subjective six point assessment criteria for all lower limb injuries for each element of the functional rehabilitation programme and worked together in various combinations before the start of the study to optimise the consistency of the assessments. All physiotherapists agreed that the minimum acceptable assessment score in each exercise was 3, and that the following levels of performance were required to achieve the score. In the fitness elements, players must: complete the exercise pain-free with no evidence of swelling at the injury location on completion of the exercise; experience no discomfort when moving in all directions and at all speeds; and complete the exercise with a normal gait pattern. In the skills elements, players must: maintain concentration and coordination; achieve adequate ball control and timing; and remain pain-free for the duration of the exercise. During the match pace football element, players must complete all normal match activities at normal match speed and remain pain-free throughout the assessment period.
In phases I and II, players were required to achieve an assessment score of ⩾3 in two exercises from the range of exercises available for each element. Players progressed to phase II of the rehabilitation programme when they had successfully completed all elements of phase I, and to phase III when they had successfully completed all elements of phase II. Satisfactory completion of each exercise achieved a player recovery score of 5% in phases I and II and a recovery score of 10% on completion of the single match pace element in phase III; players were considered to be fit to return to normal team training and competition when they had achieved a 100% recovery score. If the responsible physiotherapist was uncertain as to the level of performance of a player in any exercise, a second opinion was sought from another physiotherapist, and a consensus level of performance was agreed.
The number of days a player spent receiving treatment before starting functional rehabilitation and the player’s daily recovery scores during functional rehabilitation were recorded by the player’s responsible physiotherapist. Benchmark functional rehabilitation curves were generated by averaging appropriate—for example, thigh muscle strains, knee ligament sprains—daily recovery scores and plotting these values against the number of days of functional rehabilitation received.
RESULTS
A total of 118 injuries (match, 63; training, 55), of which seven were recurrences, and 43 932 player-hours of exposure (match, 2622; training, 41 310) were recorded over the two seasons: this equated to incidences of 24 (18–30) injuries/1000 player-match-hours and 1.3 (1.0–1.6) injuries/1000 player-training-hours. A total of 2367 player-days (pre-functional, 1451; functional, 916) were spent in rehabilitation, which corresponded to an average injury severity of 20.1 days (pre-functional, 12.3; functional, 7.8).
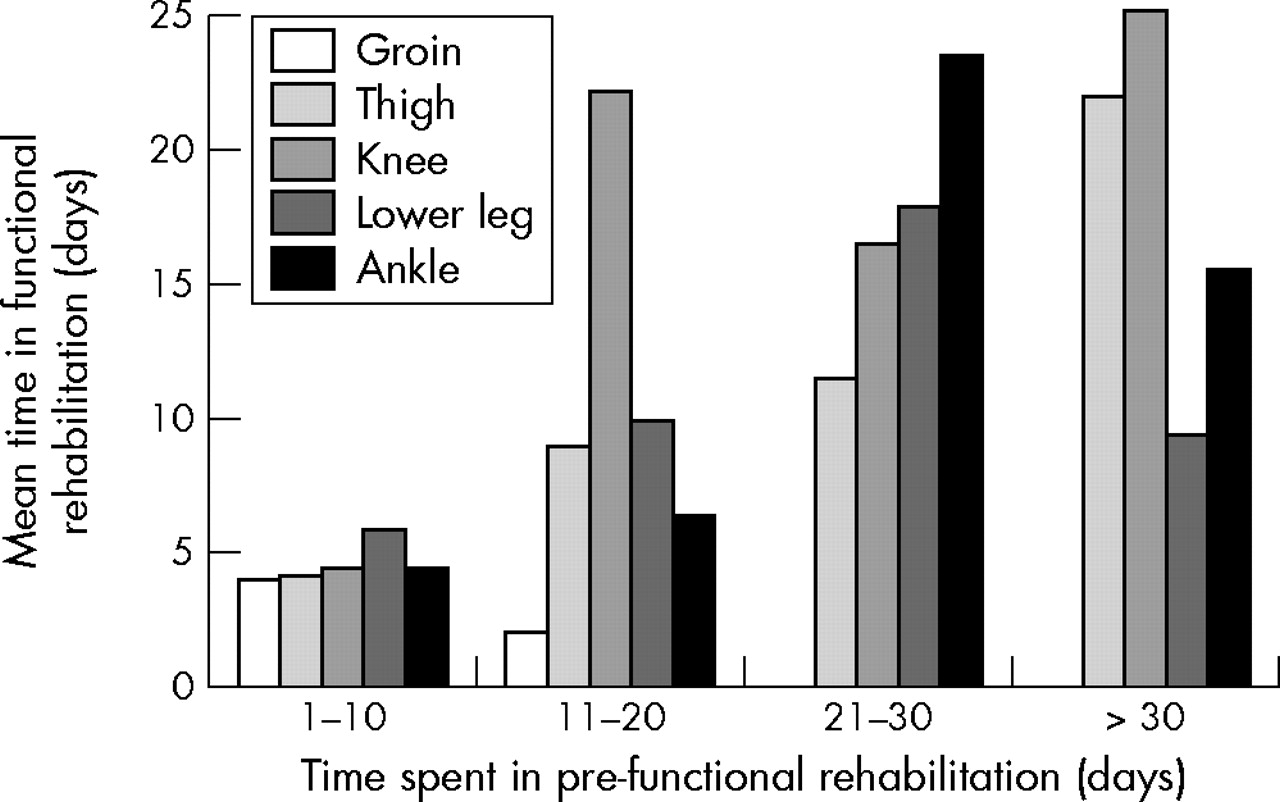
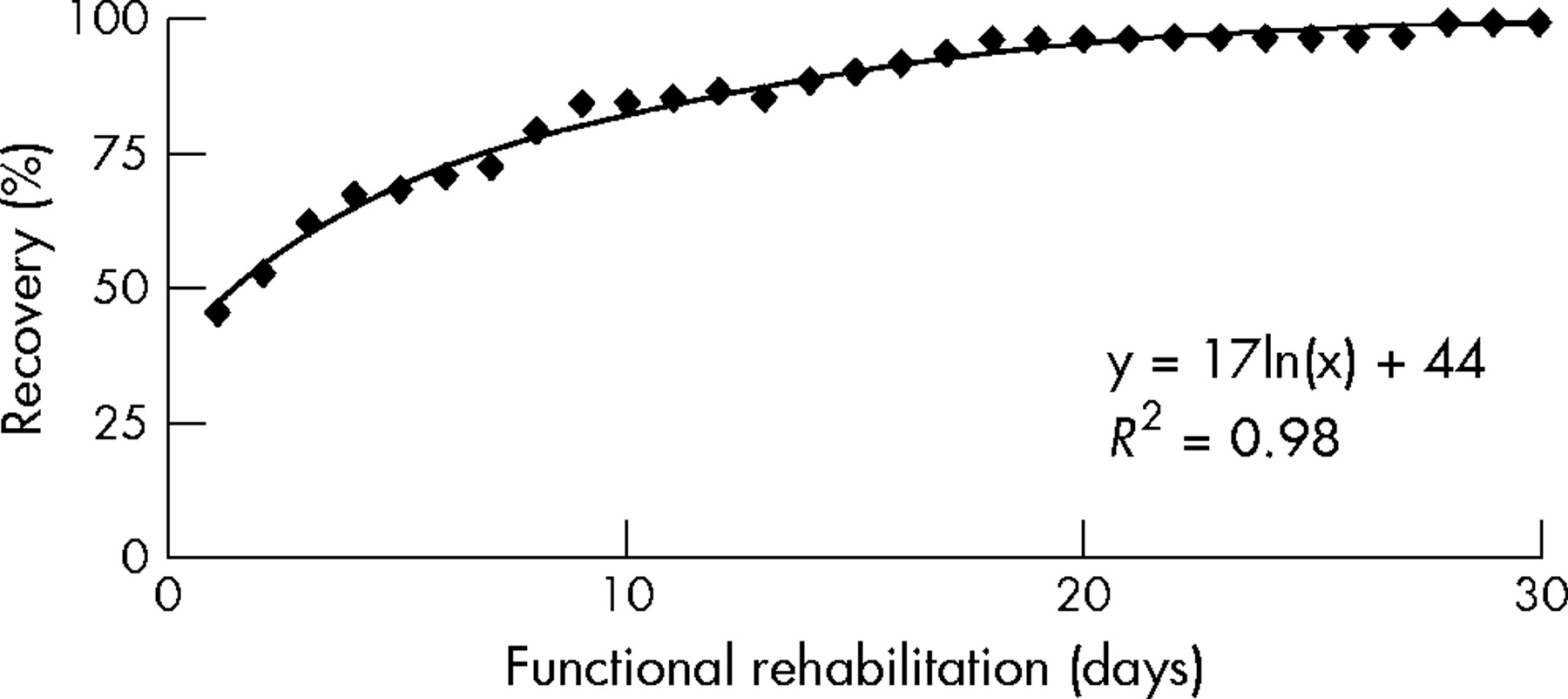
The number of injuries and the average time that players spent in pre-functional and functional rehabilitation as functions of the nature, location, and diagnosis of injuries are shown in table 1 and as functions of age, activity, playing position, and previous injury in table 2. Figure 1 shows the relation between the times spent in functional and pre-functional rehabilitation for all injuries. Figures 2 and 3 show the equivalent information for lower limb injuries as functions of the nature and location of injuries respectively. Figures 4–7 show the benchmark functional rehabilitation curves for injuries requiring one week or more of pre-functional rehabilitation for thigh muscle strains (11 hamstring; four rectus femoris), lower leg muscle strains (eight gastrocnemius), knee ligament sprains (five medial; one lateral; one patella), and ankle ligament sprains (nine lateral) respectively. The best fit curve and correlation coefficient (R2) are displayed on each graph.
Length of time in pre-functional and functional rehabilitation as a function of nature, location, and diagnosis of injury
Length of time in pre-functional and functional rehabilitation as a function of risk factors (n = 118)

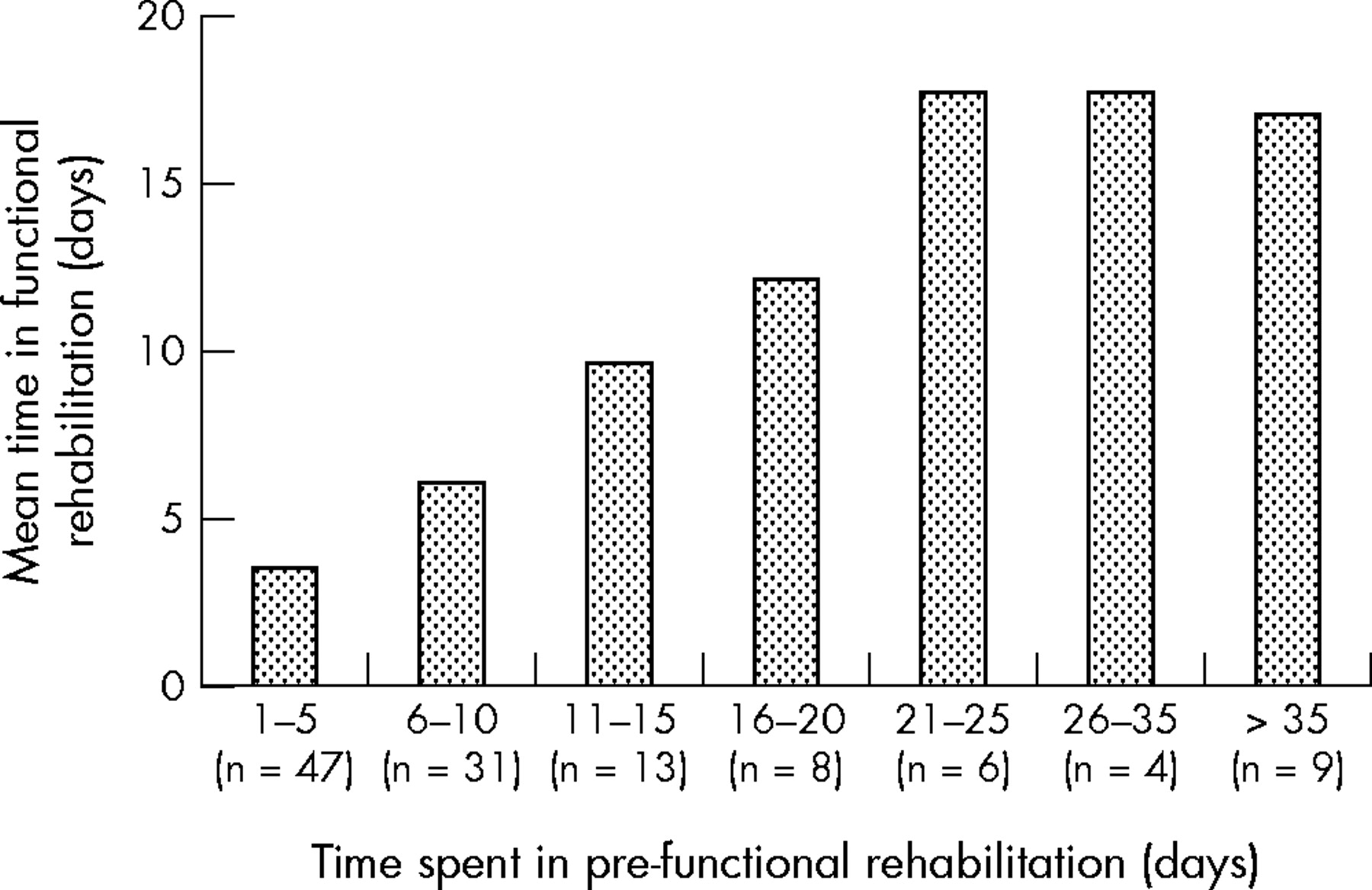
Mean time in functional rehabilitation for all injuries (n = 118) as a function of time spent in pre-functional rehabilitation.

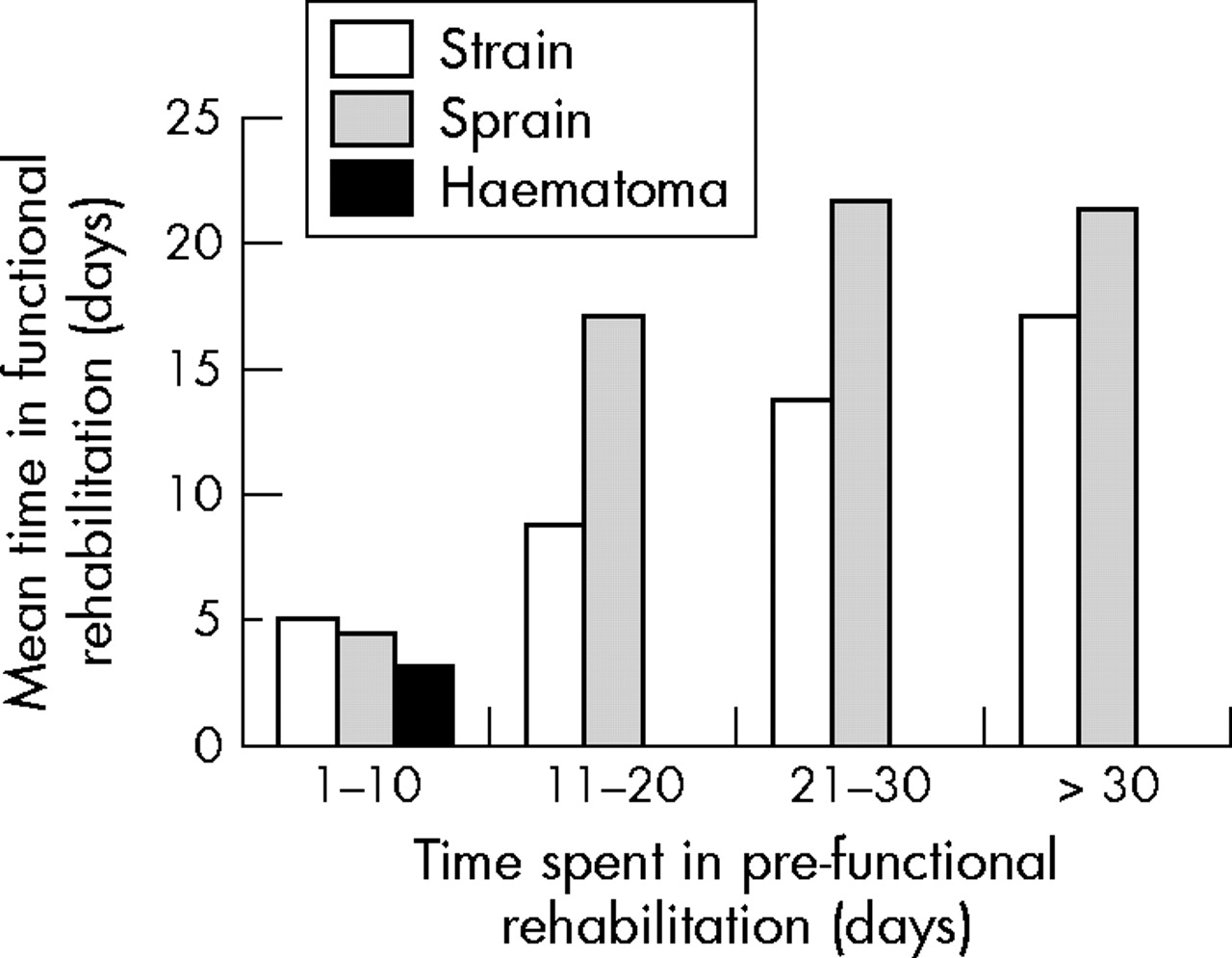
Mean time in functional rehabilitation for lower limb injuries as a function of the nature of injury (strain: n = 51; sprain: n = 32; haematoma: n = 15) and the time spent in pre-functional rehabilitation.
Mean time in functional rehabilitation for lower limb injuries as a function of injury location (groin: n = 11; thigh: n = 37; knee: n = 12; lower leg: n = 16; ankle: n = 26) and the time spent in pre-functional rehabilitation.

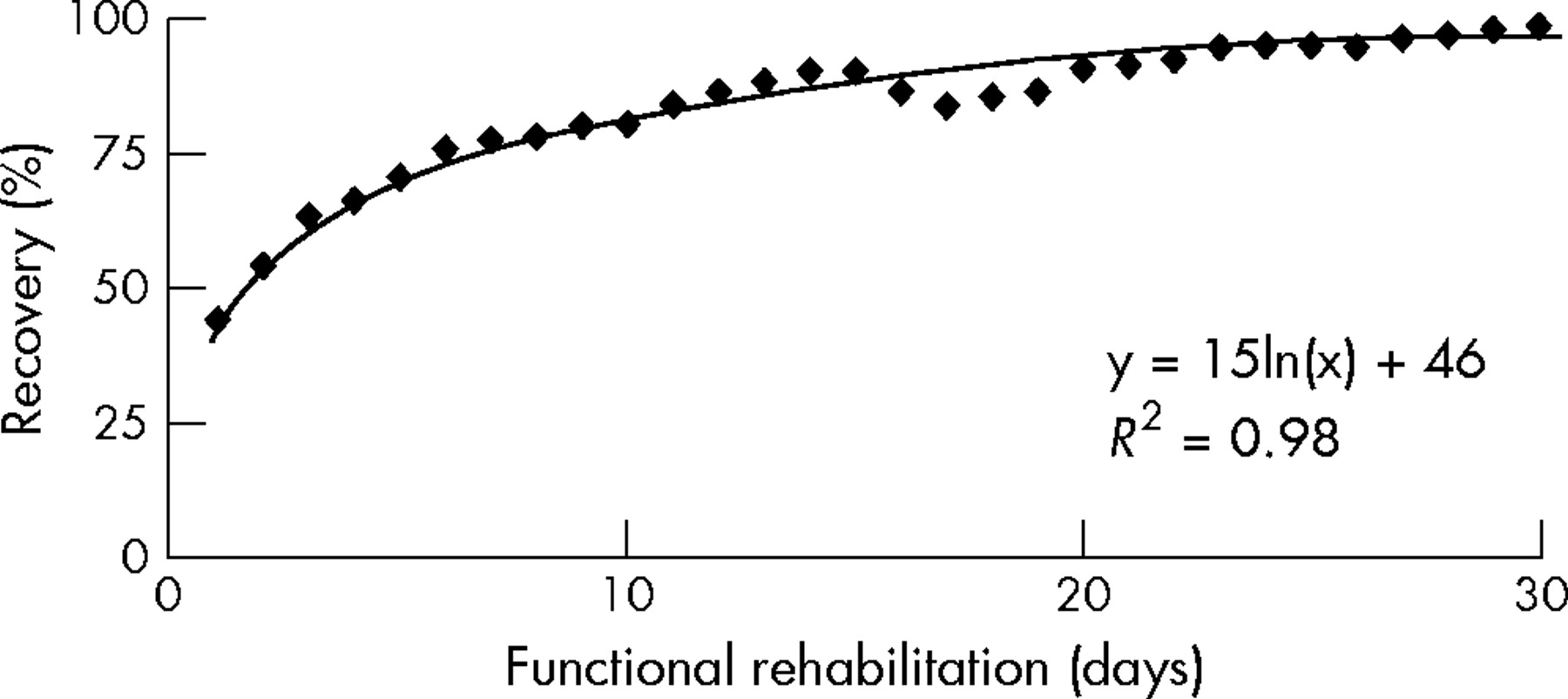
Benchmark functional rehabilitation curve for thigh muscle strains requiring one week or more pre-functional rehabilitation (n = 15).
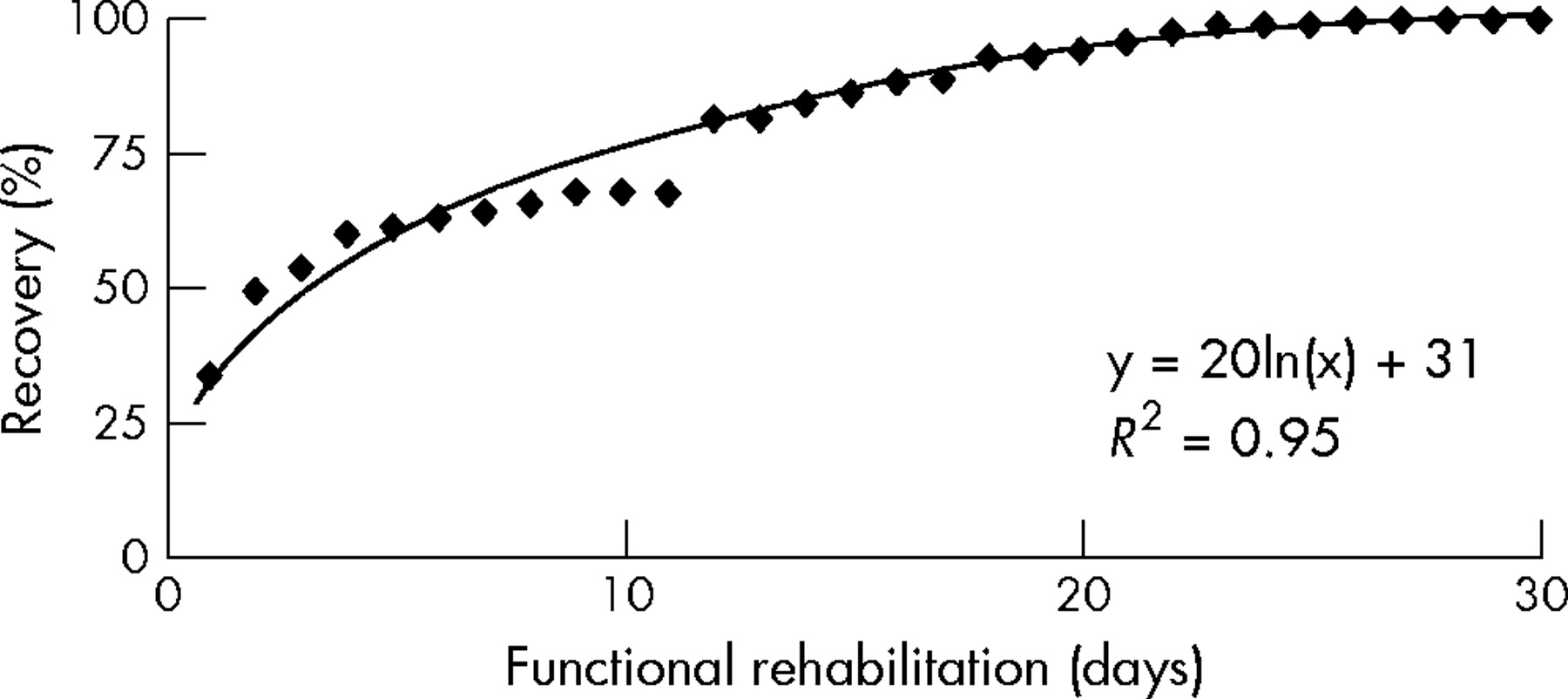
Benchmark functional rehabilitation curve for lower leg muscle strains requiring one week or more pre-functional rehabilitation (n = 8).

Benchmark functional rehabilitation curve for knee ligament sprains requiring one week or more pre-functional rehabilitation (n = 7).
Benchmark functional rehabilitation curve for ankle ligament sprains requiring one week or more pre-functional rehabilitation (n = 9).
Figure 8 shows the functional rehabilitation record of a 34 year old first team player who sustained a gastrocnemius muscle strain in the first league match of the season; the player required seven days pre-functional rehabilitation. Figure 9 records the functional rehabilitation record of a 19 year old reserve team player who sustained a rectus femoris muscle strain in training at the beginning of the season; the player required 13 days pre-functional rehabilitation. During functional rehabilitation, the player suffered from tonsillitis (days 4–9) and a period of lethargy (days 17 and 18). Figure 10 shows the functional rehabilitation records for two players who sustained knee medial ligament sprains. Player A, who had sustained six injuries over the preceding 18 month period and had returned to competition the previous week after a fractured bone in a foot, was a 26 year old first team player; the player required 46 days pre-functional rehabilitation. Player B, who had been injury-free over the preceding 18 month period, was a 20 year old reserve team player; the player required 17 days pre-functional rehabilitation.
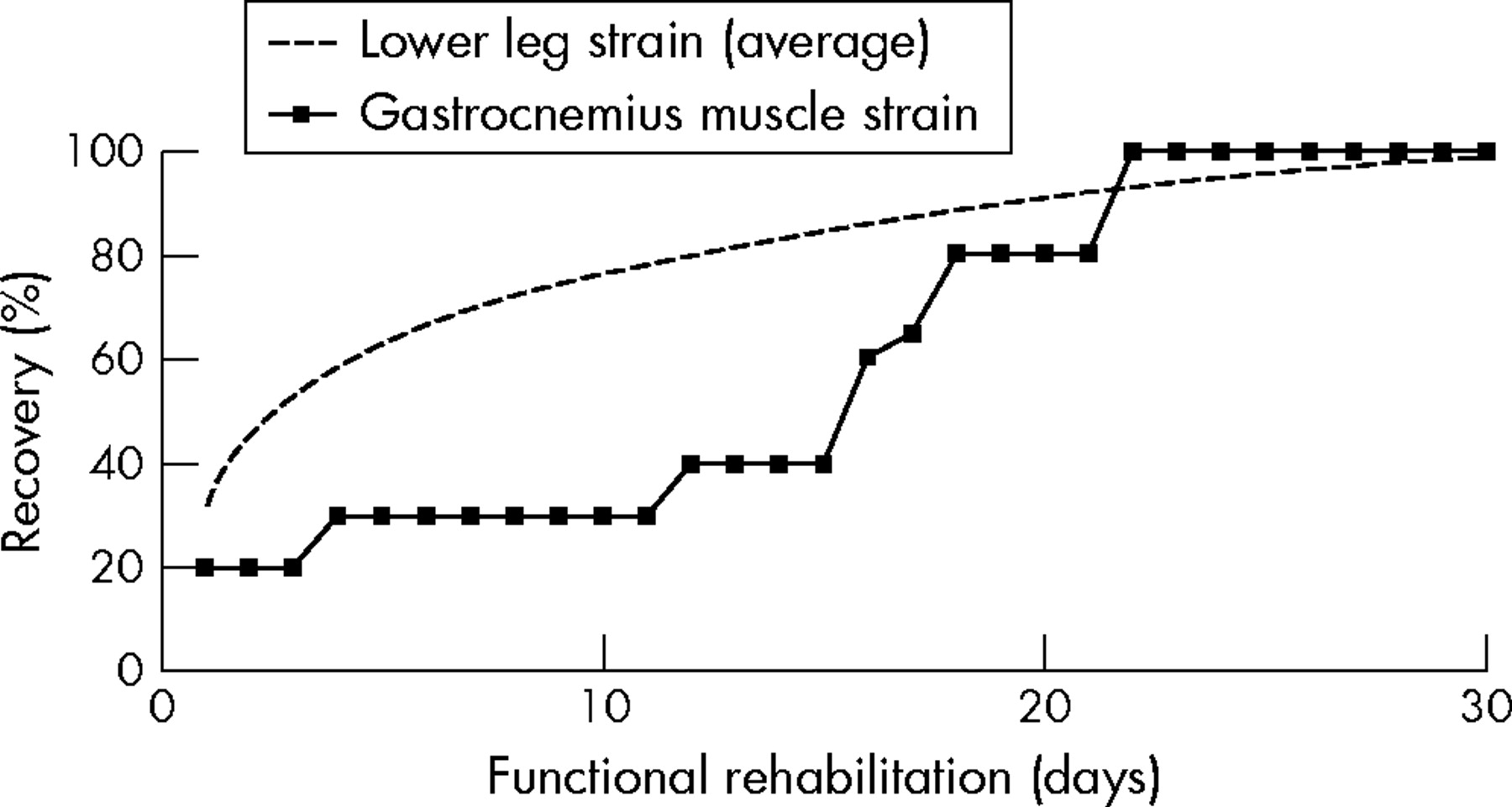
Individual functional rehabilitation records for a player sustaining a lower leg muscle (gastrocnemius) strain and a subsequent recurrence.
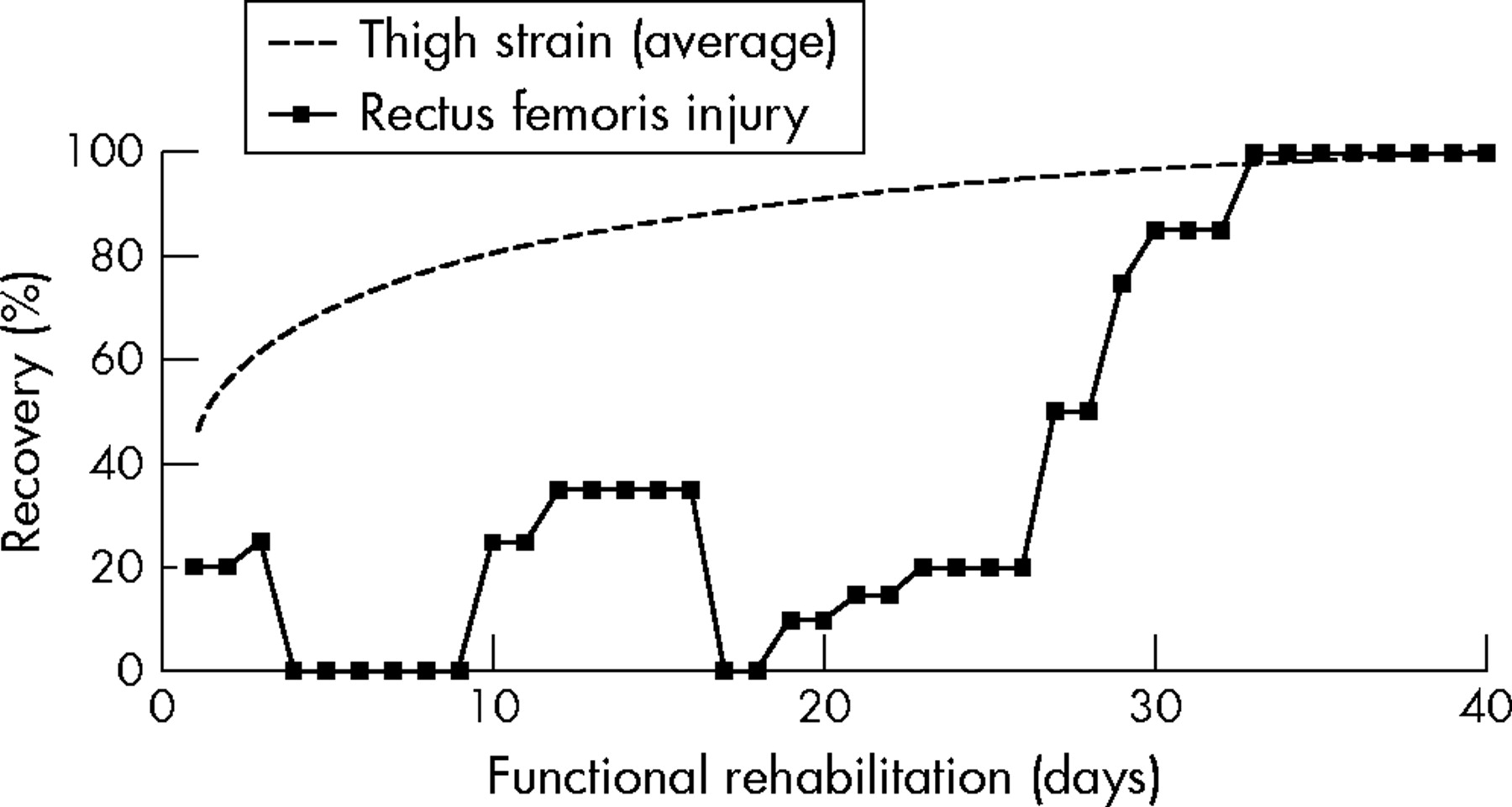
Individual functional rehabilitation record for a player suffering illness during the functional rehabilitation of a rectus femoris muscle strain.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual functional rehabilitation records for two players suffering knee medial ligament sprains.
DISCUSSION
The nature, incidence, and severity of injuries recorded in this study were within the ranges reported previously in English professional football.19,20 The injury patterns were therefore judged to be typical of those encountered by professional players in England. Recurrences were lower than previously reported, but this may reflect a benefit of the quantified rehabilitation procedure. Players’ age, playing position, and activity at the time of injury and whether the injury was new or recurrent (table 2) had no significant effect on the times spent in the pre-functional and functional stages of rehabilitation.
What is already known on this topic
-
Injured professional athletes often return to play without completing a structured rehabilitation programme
-
Return to play criteria used by clubs are often not transparent
What this study adds
-
Quantified transparent records of functional rehabilitation from injury were produced for individual players, which provided evidence based data to support management’s return to play decisions
-
Benchmark functional rehabilitation curves were derived for common lower limb injuries
The structure of the functional rehabilitation programme was typical of that used in English football: the range of exercises employed provided day to day variety and maintained players’ interest throughout their functional rehabilitation. This approach enabled rehabilitating players to demonstrate that they had re-established the aerobic and anaerobic capabilities and football specific skills required for a return to training and competition. Rehabilitation was dependent on the nature and location of the injury sustained (table 1), with groin strains requiring the least and knee ligament injuries the most time for pre-functional and functional rehabilitation. The pre-functional stage of rehabilitation generally represents a period of inactivity for injured players; Bangsbo27 (p 60) stated: “A prolonged period of inactivity, e.g. during recovery from injury, will considerably weaken the muscles. The length of time required to regain strength depends on the duration of the inactivity period.” The increasing time required for functional rehabilitation as the length of time in pre-functional rehabilitation increased supported this view (fig 1).
The rating system was based on similar principles to those adopted for the Cincinnati knee rating system,13 as it provided a range of functional assessment levels and a graded scale of performance at each level. The procedure, however, was fundamentally different, as it provided an ongoing auditable assessment of a player’s recovery from injury rather than providing a single assessment of the player’s final capabilities. Recovery curves offer other benefits. For example, they enable a player’s rehabilitation to be reviewed if a recurrence occurs, allow the success of different rehabilitation strategies to be assessed, and provide the medical team with transparent, auditable evidence of whether a player was fit to return to play.
Benchmark recovery curves for injuries requiring one week or more pre-functional rehabilitation were developed to reflect the general dependence of functional rehabilitation on the nature and location of injuries. Injuries of this severity result in players missing at least one match, so they command a significant time commitment from the physiotherapists during functional rehabilitation. The four benchmark recovery curves (thigh and lower leg muscle strains and knee and ankle ligament sprains) correlated well (R2 0.95–0.98) with logarithmic equations (y = mln(x) + c). Only one of the 11 groin muscle (adductor) strains recorded required one week or more of pre-functional rehabilitation, and therefore a benchmark recovery curve was not constructed for this type of injury. The benchmark recovery curves provide standards against which to assess the rehabilitation of individual players and to make interclub comparisons of the effectiveness of rehabilitation strategies.
The three examples of functional rehabilitation illustrate various benefits of the process. The first example (fig 8) was a player who progressed to functional rehabilitation after just seven days compared with the average 12 days required for this type of injury (table 1); the player then struggled for some time to achieve satisfactory standards of performance in the speed, power, and agility fitness elements. Subsequent investigations identified that this player had understated the severity of his injury because, having sustained an injury early in the season, he was concerned that, if he lost his place to a younger player, he would find it difficult to regain his place. As one of the club’s older players, he was concerned that his contract would not be renewed at the end of the season if he failed to command a first team place. The early progression to functional rehabilitation had resulted in the player still experiencing pain, and this had inhibited his ability to achieve adequate performances in the more progressive fitness tests.
In the second example (fig 9), the player underwent a normal period of pre-functional rehabilitation before progressing to functional rehabilitation. The player progressed through the early endurance and speed-endurance fitness tests, but a six day period of illness (tonsillitis) meant he was unable to continue. On returning from illness, the player quickly recovered his previous level of performance, but was concerned about his recovery from tonsillitis and reported a general feeling of lethargy. On day 17, the club’s doctor arranged a series of blood tests for the player. When these tests were returned negative on day 18, the player’s concerns were allayed and his rehabilitation then progressed smoothly to full recovery.
The third example (fig 10) illustrates the differences that can occur in the rehabilitation of apparently similar injuries. Player B’s recovery was straightforward and closely followed the benchmark for knee ligament sprains. Player A, however, took five weeks before he could achieve acceptable levels of performance in the speed, power, and agility elements. Subsequent investigation identified that player A’s slower recovery was caused by the cumulative effects of the player’s previous six injuries on his general fitness and, in particular, by the exceptionally long period of inactivity required for the pre-functional rehabilitation of the current medial ligament injury, which had followed closely on from an eight week period of rehabilitation for a fractured bone in the foot.
The results show that a structured, quantified rehabilitation programme based on routine functional exercises and a graded subjective assessment of performance can provide auditable records29 of players’ recoveries from lower limb injuries and a transparent exit point31 from the rehabilitation programme. Further studies are required, however, to confirm its general utility. The rehabilitation records allow players to view their daily progress32 against benchmark standards and enable physiotherapists to develop realistic motivational targets for players throughout their rehabilitation.33 The quantified approach to functional rehabilitation benefits clubs by providing a permanent record of the rehabilitation of every injury and evidence based data to support management return to play decisions.29 The general principle of quantified functional rehabilitation proposed here could be equally applied to other injuries and sports if appropriate sport specific exercises are incorporated into the programme.
REFERENCES
Commentary
This paper provides a fascinating theory on the management of injury in professional sport. The use of objective measures to assess ability to return to play provides an original concept to assist practical decision making on a daily basis. The objective assessment provides the means by which simple and meaningful information can be effectively communicated and shared between members of an athlete’s support team. More importantly, agreement is more likely to be forthcoming and transparent between individuals when challenging decisions need to be made on return to play. The use of sports specific field assessment will face scrutiny with respect to scientific rigour, but, if used in association with other “tools”, the process will be reinforced and contextualised for the environment. The process and system developed will provide a practical, meaningful, and useable tool for the support team that can fit into their core role without significantly impinging on the daily demands of their job. The development of robust protocol and return to play characteristics will take time to evolve in a sport, as more data will be required to support decisions made. However, this process should become the benchmark for the management of any injury rehabilitation and return to play for all sports.
Footnotes
-
Competing interests: none declared