Article Text

Abstract
The ligamentous, osseous, musculotendinous, and neural structures at the postero-medial side of the elbow are at risk for various injuries in overhead athletes. The combination of valgus and extension overload during overhead activities results in tensile forces along the medial stabilising structures, with compression on the lateral compartment and shear stress posteriorly. The combination of tensile forces medially and shear forces posteriorly can result in ulnar collateral ligament (UCL) tears, flexor–pronator mass injuries, neuritis of the ulnar nerve, posterior impingement, and olecranon stress fractures. Most symptomatic conditions of the overhead athlete can be treated conservatively initially. In cases where conservative treatment is unsuccessful surgical intervention is indicated. Recent advances in arthroscopic surgical techniques and ligamentous reconstruction ensure that the prognosis for return to pre-injury level is good.
- AOL, anterior oblique ligament
- POL, posterior oblique ligament
- UCL, ulnar collateral ligament
- elbow
- athlete
- instability
Statistics from Altmetric.com
The increase in the number of participants in overhead sports as baseball, tennis, football, and volleyball has resulted in a sharp rise in the incidence of elbow injuries in recent decades. The magnitude of forces across the elbow during overhead throwing and tennis strokes can produce tremendous valgus and extension overload in some players. This combination of valgus and extension often leads to acute or chronic injury of the elbow. Tensile forces are generated along the medial stabilising structures, with compression on the lateral compartment and shear stresses posteriorly.
Common injuries encountered at the medial elbow include ulnar collateral ligament (UCL) tears, flexor-pronator mass tendinosis or tears, and ulnar neuritis. In the posterior compartment, posterior impingement can be seen, with or without loose bodies and olecranon stress fractures. Laterally, overload may results in chondromalacia of the radiocapitellar joint with or without loose body production.
The purpose of this article is to review current knowledge on the diagnosis and non-operative and operative treatment of postero-medial elbow problems in adult athletes. For appropriate treatment of elbow problems in athletes, a thorough understanding of both anatomy and biomechanics is necessary. Thus the anatomy and biomechanics of the elbow are briefly reviewed.
ANATOMY AND BIOMECHANICS
In the normal elbow joint, stability is maintained by a combination of joint congruity, capsuloligamentous integrity, and balanced intact musculature. The olecranon and olecranon fossa articulation as well as the radio-capitella joint provide primary stability at less than 20° or more than 120° degrees of elbow flexion. In between, stability is provided by soft tissue constraints, mainly the UCL.1,2
The UCL complex consists of an anterior oblique ligament (AOL), posterior oblique ligament (POL) and a transverse band (fig 1). This transverse band is also known as Coopers ligament and originates and inserts on the ulna. It does not provide stability. The AOL has been shown to be the most important soft tissue constraint to valgus instability of the elbow and is the strongest and stiffest of the collateral ligaments of the elbow, with an average failure load of 260 N.2,3

Ulnar collateral ligament (UCL) complex. 1 = anterior oblique ligament (AOL); 2 = posterior oblique ligament (POL); 3 = transverse band.
The mean length of the AOL is 27.1 mm and of the POL, 24.2 mm; the mean widths are about 4.7 mm and 5.3 mm, respectively.4–8 The AOL originates from the inferior edge of the medial epicondyle and inserts on the medial aspect of the coronoid process of the ulna. The flexor carpi ulnaris muscle, pronator teres, and flexor digitorum superficialis predominantly form the musculo-tendinous unit overlying the AOL; all three muscles are considered to contribute to medial support.9 While the flexor carpi ulnaris lies directly over the AOL, the flexor digitorum superficialis has fibres originating in the AOL.
During a throwing motion—in baseball for example—the elbow moves during late cocking and acceleration phases from 110° to 20° of flexion with velocities up to 3000°/s.10 This combination of valgus forces and rapid extension results in tensile forces along the medial side, compression on the lateral portion of the elbow, and shear forces in the posterior compartment. This combination is called “valgus extension overload” syndrome and forms the basic pathological model behind most injuries in the athlete’s elbow.
INSUFFICIENCY OF UCL
Rupture of the UCL resulting from overhand throwing has been described extensively in athletes.11–17 Most affected individuals are high level baseball pitchers, though the earliest recognition of this injury was in javelin throwers. Reports of comparable injuries in other athletes such as rock climbers, tennis players, and handball goalkeepers are rare. Findings in acute medial collateral ligament injury are moderate to severe elbow pain, acute onset of pain during throwing, a popping sensation during throwing, medial ecchymosis, and acute ulnar nerve symptoms. Chronic overuse of the elbow in athletes—the most common presentation of UCL insufficiency in the athlete—can also result in progressive attenuation of the UCL leading to ligamentous insufficiency even in the absence of a singular catastrophic episode of ligament failure. Some athletes report a previous severe injury, suggestive of acute ligament rupture which was not diagnosed or where definitive treatment was not carried out. Commonly, however, athletes may note a history of recurrent elbow pain after or during throwing, without a specific injury, and finally present after an acute episode of pain during throwing—an “acute on chronic” presentation. These athletes present with tenderness over the medial aspect of the elbow, especially during the late cocking or early acceleration phases of throwing, and postero-medial pain.
On physical examination the joint must be tested for valgus instability in 30° and 70° of flexion. Biomechanical studies show that the UCL provides the greatest contribution to valgus elbow stability at 70° of elbow flexion. Safran et al18 found that neutral rotation is the best forearm position to reveal valgus laxity. Comparison with the uninvolved elbow should always be undertaken to differentiate between physiological and pathological laxity. The degree of laxity is often underestimated. However, not just the degree of laxity but also the quality of the end point must be assessed. In patients with insufficiency of the UCL. In patients with insufficiency of the UCL, two tests have been found to be particularly useful. First is the moving valgus stress test (fig 2A). In this test, a valgus stress is applied to the elbow while the shoulder is abducted and externally rotated. The elbow is then taken through a range of flexion and extension. Pain is reproduced within the arc or 80° to 120°. A second useful test is the modified milking manoeuvre (fig 2B). The patient’s elbow is flexed to 70° and the examiner uses one hand to palpate the UCL and medial joint line while the other hand is used to apply a valgus stress to the patient’s elbow by pulling down on the patient’s thumb. The diagnosis is confirmed by positive magnetic resonance imaging (MRI), dynamic stress radiographs, dynamic ultrasonography, or a positive valgus test under anaesthesia.19,20 Stress radiographs, often felt to be the gold standard in the assessment of UCL injury, have proven inconsistent. Safran has also recently presented the use of an arthrometer to evaluate valgus stability of the elbow and found this to be more sensitive than stress radiographs in detecting UCL injury.21 MRI can contribute to decision making in medial instability, with a sensitivity of 57% and a specificity of 100% for UCL injury.22,23 MRI arthrography appears to improve the sensitivity of detection of UCL tears.16

(A) The moving valgus stren test described by O’Driscoll; (B) The modified “milking manoeuvre” as described by Safran to detect insufficiency of the UCL; opening of the medial joint line can be palpated during valgus stress.
Conservative treatment of isolated UCL injury consists of short immobilisation in a long arm cast or placement in a hinged elbow brace to control initial pain and inflammation while reducing valgus forces to the elbow, followed by an intensive exercise programme and avoidance of valgus load for three to six months. In non-throwing athletes or low demand individuals, a conservative regimen has acceptable results. Athletes involved in high demand throwing sports respond less well to non-operative treatment.24,25 Rettig et al reported a 42% success rate of non-operative treatment in throwing athletes with UCL injuries.26 Persistent symptomatic instability after non-operative treatment is an indication for reconstruction. Most reports describe a technique that includes a free tendon graft placed in bone tunnels in the humerus and ulna.27–29 Although good results were reported, the technique is technically demanding and the risk of fracture, especially of the ulnar tunnel, is a concern. Recently, a simplified docking technique was described on the humeral side, using palmaris tendon.30,31 Jobe et al reported a follow up study in 71 athletes with valgus instability. Fourteen had a direct repair of the ligament, and 56 had a reconstruction of the ligament using the Jobe technique with a free palmaris tendon graft. The result was excellent or good in 10 of the 14 patients in the repair group and in 45 of the reconstruction group. Seven of the 14 who had direct repair returned to the previous level of participation in their sport. Fifteen patients had postoperative ulnar neuropathy, This was transient in six, and the other nine had an additional operation for the neuropathy. Rohrbough et al, who first described the humeral docking technique, had excellent results in 33 of 36 cases.30
FLEXOR-PRONATOR TENDINOSIS OR RUPTURE
Flexor-pronator tendinosis is much less common than its lateral counterpart, the latter occurring seven to 20 times more often. While flexor-pronator tendinosis is commonly called golfer’s elbow, this tendinosis is much more common than tennis elbow in high level tennis players. Improper throwing or tennis technique, poor conditioning, and fatigue can all lead to inflammation of the flexor-pronator mass. The pronator teres and flexor carpi radialis have been identified as the most common sites for pathological changes.32,33 Tenderness is usually distal and lateral to the medial epicondyle; resistant wrist flexion and forearm pronation exacerbate pain.
In throwing athletes and tennis players, acute muscle tears have also been described.34 Both injuries generally respond well to non-operative treatment with active rest, physical therapy, and gradual return to athletic activities. Cortisone injections may be beneficial as an adjunct, to reduce the pain sufficiently to undertaken physical therapy or home exercises.
Flexor-pronator mass tendinosis unresponsive to a well managed non-operative programme for at least six months is an indication for surgical treatment after exclusion of any other pathological causes, especially UCL insufficiency. Results after surgery show an improvement of elbow function in 90% of all cases, with >95% returning to sports activities.33 However, if there is concomitant ulnar nerve symptoms, the success rate is only 40–50%.
ULNAR NEURITIS
Ulnar neuritis around the elbow can be the result of compression or traction from valgus stress and can be seen as an isolated injury or in combination with UCL insufficiency or chronic flexor-pronator mass tendinosis. Compression can occur because of a tight cubital tunnel, osteophytes from the ulno-humeral joint, muscle hypertrophy, or subluxation of the nerve. Subluxation of the nerve should be distinguished from a hypertrophic part of the medial head of the triceps snapping over the medial epicondyle during flexion.34 In the throwing athlete the initial presentation of ulnar neuritis may be pain along the medial joint line associated with dysaesthesias, paraesthesias, or even anaesthesia in the little finger and the ulnar half of the ring finger. Baseball pitchers will complain of loss of ball control. The paraesthesias usually occur early and precede motor weakness in general. Motor weakness can result in early fatigue in the hand of the athlete or difficulty with the performance of complex hand tasks or clumsiness. On physical examination the cervical spine is assessed and provocative manoeuvres to rule out the thoracic outlet syndrome should be carried out. A systematic examination of the elbow is necessary to detect osteoarthritis, valgus instability, flexion contracture, and injury to the flexor-pronator mass. Tenderness along the cubital tunnel may be present and full flexion of the elbow, in combination with full extension of the wrist for three minutes, may provoke ulnar nerve symptoms.35 The degree of sensory and motor changes can vary depending on the severity and duration of ulnar nerve compression. Conservative treatment with rest and cessation of sports activities can be tried; however, the success rate in athletes is probably lower than in the general population, especially if it is associated with insufficiency of UCL. Surgical intervention is indicated in case of progressive muscle weakness, persistent muscle weakness for more than four months, chronic neuropathy, or failure of a non-surgical regimen.35–37
POSTERIOR IMPINGEMENT
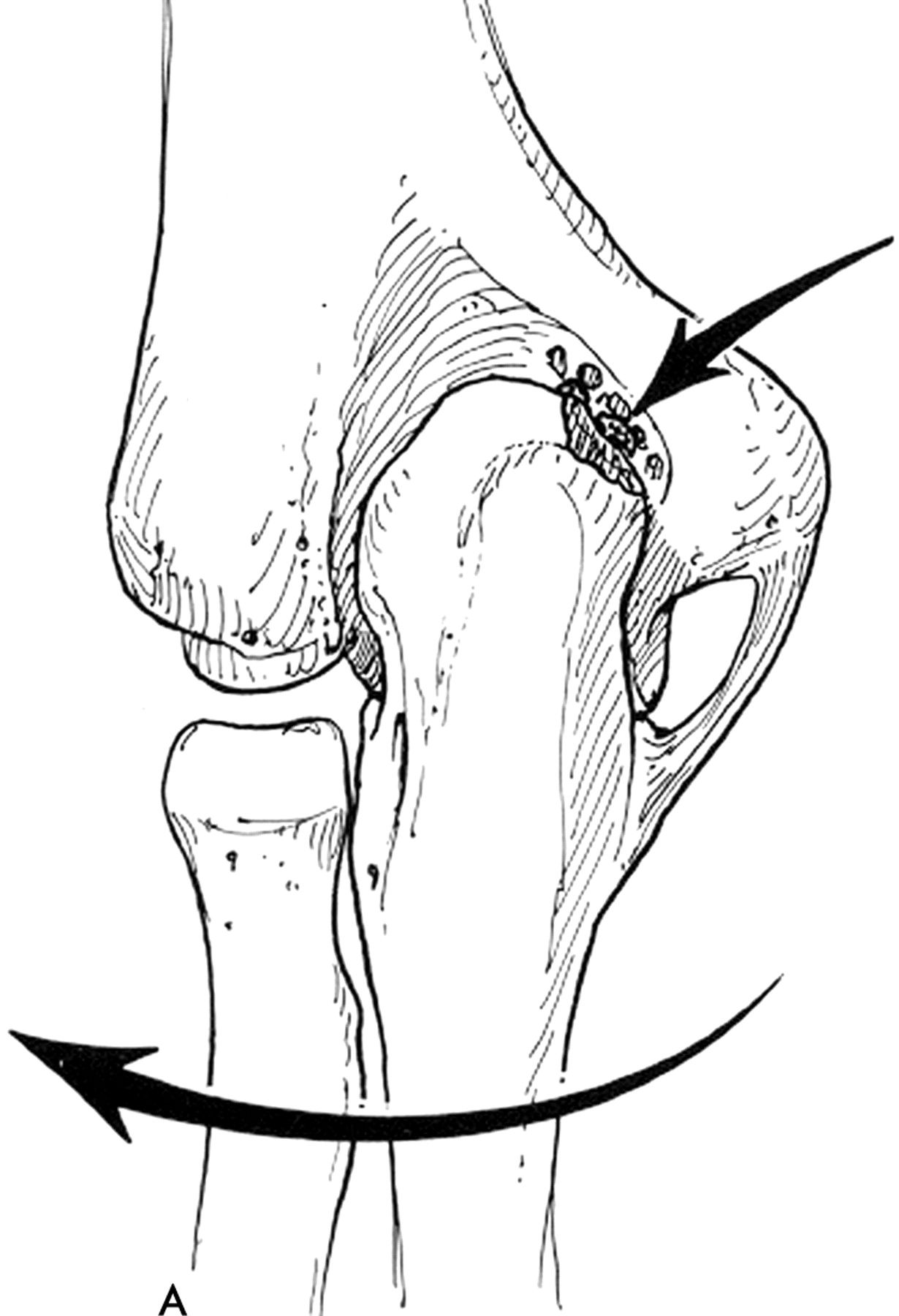
Posterior impingement of the elbow is an uncommon disorder in the general population; however, it is usually seen in patients who overuse their elbow during specific sporting activities such as overhead throwing or tennis.38,39 This problem is caused by repetitive combined hyperextension, valgus, and supination of the elbow, resulting in a mechanical abutment of bony or soft tissues in the posterior fossa of the elbow (fig 3). The resultant soft tissue swelling, loose bodies, or osteophyte formation, or combinations of these, together with abutment may result in symptoms in the posterior side of the elbow.38–40 The athlete complains of pain posteriorly, joint effusion, locking, crepitus, and a decrease in range of motion, most notably an extension deficit. If conservative treatment of posterior impingement fails, arthroscopy of the elbow can be successful.39,40

Valgus-extension overload resulting in posteromedial impingement.
Posterior impingement can also be associated with ligamentous instability of the elbow, especially UCL insufficiency. UCL insufficiency allows for greater shear force and posterior impingement.41 Radiographs, especially an axial view, may be helpful to detect osteophytes on the olecranon or on the borders of the posterior fossa. Computed tomography (CT) can be used to evaluate the posterior compartment for osteophytes. However, MRI with intra-articular contrast is more sensitive (the sensitivity for posterior soft tissue or loose bodies is nearly 90%).39 Sonography can be used, and stress radiographs may be carried out to document ligamentous laxity or rupture.40–43 Treatment for posterior impingement starts with conservative measures such as physiotherapy and non-steroidal anti-inflammatory drugs, in combination with rest, ice, compression, and elevation. Sometimes steroid injections can give some relief from pain, especially if there is soft tissue swelling causing impingement. If conservative treatment fails, arthroscopic or open debridement is the primary treatment option for posterior impingement of the elbow. In the largest available series documenting elbow arthroscopy; Reddy et al reported 187 arthroscopies done in 172 patients. The most common diagnosis was posterior impingement (51%), followed by loose bodies (31%) and degenerative joint disease (22%). Laxity of the UCL was seen in 6% of cases. Although 68 patients were lost to follow up, they reported 49% excellent, 36% good, 11% average, and 4% poor results, based on the modified Figgie score. There were three transient complications, one related to the ulnar nerve.42 There are few publications on arthroscopic treatment of posterior impingement. In 1997, Fideler et al showed excellent results in 113 professional baseball players treated arthroscopically for posterior impingement and loose bodies; 74% returned to their preoperative level of sports.38 Bradley et al showed that after two years, six patients with posterior impingement treated arthroscopically had either an excellent or a good result. In this study, only athletes with posterior impingement were included. Patients who had underlying arthrofibrosis of the elbow were excluded, as were unstable elbows. The latter were treated by a stabilising operation first.39 Andrews cautioned that those who underwent partial olecranon excision for posterior impingement did not have universally excellent results; 42% of his patients required a second operation, several undergoing UCL reconstruction. It is unclear whether removal of the osteophytes and some of the olecranon uncovered UCL insufficiency or resulted in increased strain on the UCL, making is susceptible to rupture when the athlete returned to throwing.43,44 As a result of Andrews’s work and cadaver research, it is recommended that only the osteophyte and no native olecranon should be removed.45–47
OLECRANON STRESS FRACTURES
Stress fracture of the olecranon can be the result of repetitive microtrauma against the olecranon fossa or excessive tensile stress of the triceps tendon.48 The athlete complains of postero-medial or postero-lateral elbow pain during and shortly after sports activities. Standard radiography can be normal; additional imaging such as MRI, CT, or bone scan may be necessary to confirm the diagnosis (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Magnetic resonance imaging of an olecranon stress fracture (arrowed).
Treatment starts with cessation of sports activities and active rest. The role of bone growth stimulation remains unclear. Stress fractures of the olecranon have to be distinguished from avulsion fractures of the tip of the olecranon and from persistent olecranon apophysis.49
In the high demand overhead athlete, stress fractures of the olecranon often require internal fixation—for example, with cannulated screws or plate osteosyntheses—while persistent olecranon apophyses may additionally require bone grafting.16,50
CONCLUSIONS
The ligamentous, osseous, musculotendinous, and neural structures at the postero-medial side of the elbow are at risk for various injuries in overhead athletes. These injuries can be the result of a single traumatic event or repetitive microtrauma. The combination of valgus and extension overload during overhead activities results in tensile forces along the medial stabilising structures with compression on the lateral compartment and shear stress posteriorly. The combination of tensile forces medially and shear forces posteriorly can result in ulnar collateral ligament tears, flexor-pronator mass injuries, neuritis of the ulnar nerve, posterior impingement, and olecranon stress fractures.
It is important to recognise that these injuries may occur in combination and that every entity must me treated accordingly.
In general, most symptomatic conditions of the overhead athlete can be treated conservatively initially. In cases where conservative treatment is unsuccessful, surgical intervention is indicated. Recent advances in arthroscopic surgical techniques and ligamentous reconstruction ensure that the prognosis for return to preinjury performance level is generally good.
REFERENCES
Commentary
Here is a good review and presentation of the most common problems around the athlete’s elbow, with a nice overview of the anatomy and the pathological changes resulting from chronic overuse of the elbow. The different injuries are well described and there is a satisfactory explanation of the pathophysiology. The paper serves as an eye opener for the possibilities of treatment. We liked the milking manoeuvre—new for many orthopaedic surgeons and easy to learn and perform.
Footnotes
-
Competing interests: none declared