Article Text

Abstract
The mechanism of the overhead action in throwing sports has been studied extensively. This motion is unnatural and highly dynamic, often exceeding the physiological limits of the joint. Owing to overload of various anatomical structures, the shoulder is susceptible to injury. Optimal shoulder function requires good kinetic chain function, optimal stability, and coordination of the scapula in the overhead action. A well balanced action of the rotator cuff muscles and capsular structures is necessary to obtain a stable centre of rotation during the overhead action. This review concerns shoulder injuries, related to the overhead motion in tennis players, which can be explained by the same mechanism as thrower’s shoulder.
- GIRD, glenohumeral internal rotation deficit
- IGHL, inferior glenohumeral ligament
- SLAP, superior labrum anterior to posterior
- shoulder
- tennis
- kinetic chain
- glenohumeral internal rotation deficit
- SICK scapula
Statistics from Altmetric.com
- GIRD, glenohumeral internal rotation deficit
- IGHL, inferior glenohumeral ligament
- SLAP, superior labrum anterior to posterior
The shoulder is the most mobile joint in the human body. Its anatomical design provides stability allowing a wide range of motion in all directions. This leads to a fragile equilibrium between stability and mobility, particularly in the tennis player, who is trying to generate as much energy as possible for the serving motion. In sports science literature, this is referred to as the “thrower’s dilemma”. The repetition of the abduction-external rotation movement of the arm during the overhead action—for example, in a tennis serve, baseball throw, and javelin throw—carries an increased risk of overloading various structures around the shoulder. As the large majority of shoulder injuries in tennis players have multiple anatomical, physiological, and biomechanical alterations that combine in various ways to produce specific injury patterns and patterns of dysfunction, knowledge of the alterations that may occur is essential for understanding the clinical symptoms and treatment options of shoulder injuries.
BIOMECHANICAL ASPECTS
To understand the function of the shoulder in the tennis serve, it is important to examine all aspects that contribute to this action, including the kinetic chain, scapular function, and the role of the static and dynamic shoulder stabilisers.
Kinetic chain theory
The tennis serve has five different phases: (a) wind up (knee flexion, trunk rotation); (b) early cocking; (c) late cocking (position of maximal abduction-external rotation); (d) acceleration phase (including long axis rotation); (e) follow through (fig 1).
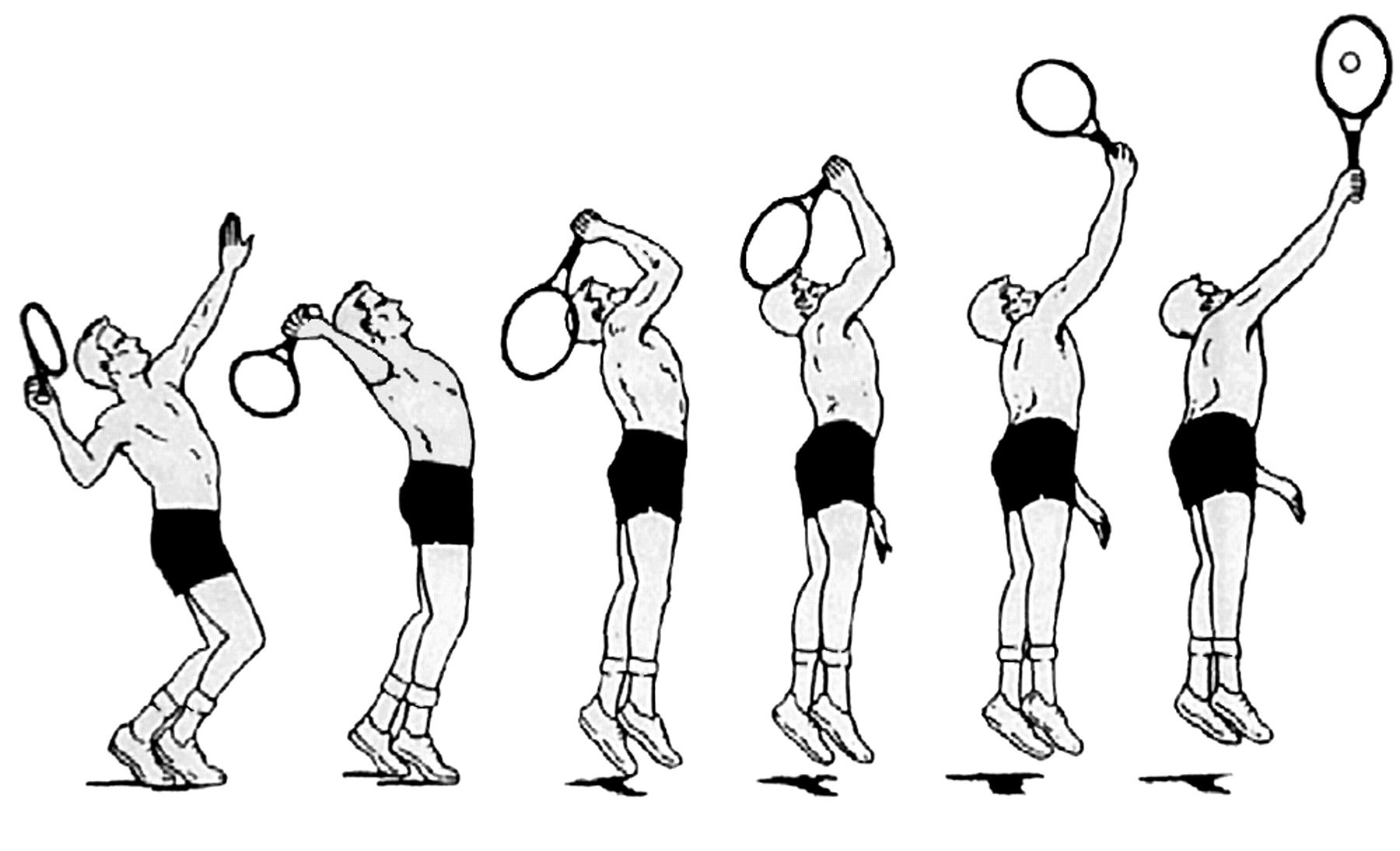
Different phases of the tennis service motion.
During the serve, the shoulder is part of a kinetic energy chain, in which the body is considered as a linked system of articulated segments, each part contributing to the final energy needed for hitting the ball (fig 2). All segments (leg, hip, trunk, shoulder, elbow, and wrist) of the kinetic chain have to be in perfect shape to be able to create a sufficient level of energy to produce an effective serve. To create an optimal service motion with maximum power release, the following prerequisites are necessary: an intact kinetic chain function, normal scapular function, and intact dynamic and static stabilisers of the shoulder.
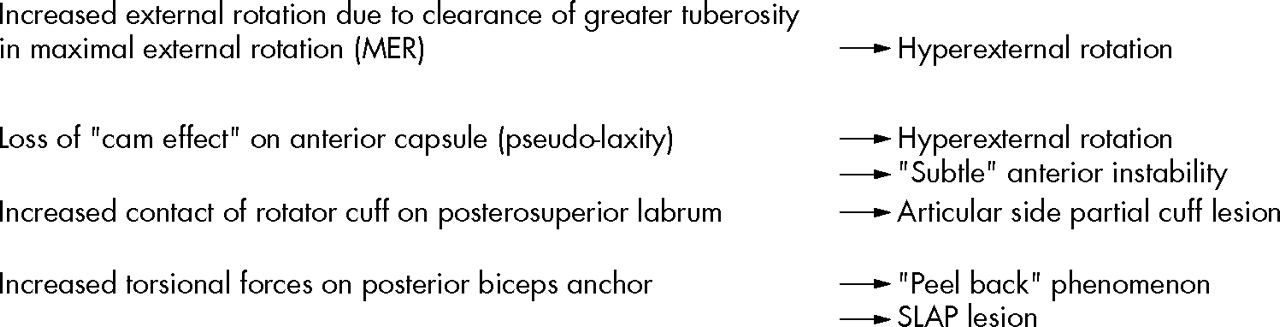
Posterosuperior shift of centre of rotation. SLAP, Superior labrum anterior to posterior.
The kinetic chain allows generation, summation, and transfer of forces from the legs to the hand. Sequential involvement of the links of the chain allows the force generated by ground reaction forces, and activity of the large, powerful leg and trunk muscles to be transferred to the shoulder and upper arm. Kibler1 calculated that 51% of total kinetic energy and 54% of total force are developed in the leg/hip/trunk link and can be defined as the force generators of the kinetic chain. In the same way the shoulder can be seen as a funnel and force regulator. Finally the arm, elbow, and wrist act as a force delivery mechanism. Breakage of a link in the proximal part of the chain will lead to a higher demand on the more distally located segments. Only enhancement of the functional ability of these distal segments will result in the same level of energy at the end of the kinetic chain. This is called the “catch up” phenomenon (fig 3). From this mechanism, it is clear that the more distal parts of the kinetic chain (shoulder, elbow, and wrist) are more susceptible to overuse and injury than the proximal parts.
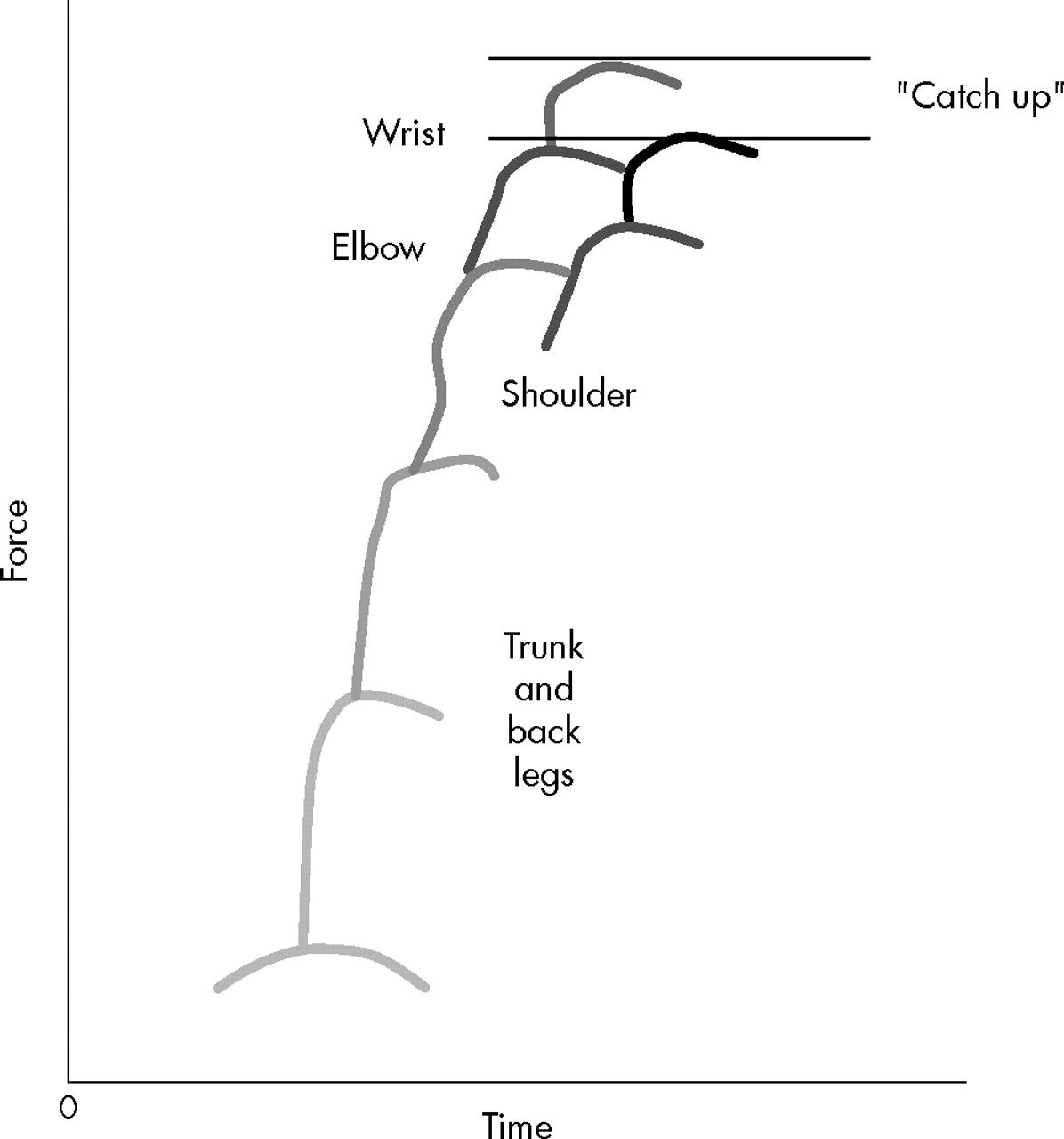
Schematic illustration of the kinetic chain theory.
Scapular function
The scapula plays a pivotal role in the function of the shoulder. Firstly, it acts as a stable base for the humeral head during the overhead motion to guarantee a congruent socket during the tennis serve. Secondly, it has to move around the thoracic wall, while the arm moves from early cocking to late cocking and follow through (retraction/protraction). In the same way the scapula has to move in an upward direction (rotation) in order to clear the acromion from the moving humeral head. Finally, it forms a stable base for the intrinsic and extrinsic muscles that control arm motion and the position of the scapular against the thorax. Fine tuning of scapular motion is provided by coupling of muscle action. The serratus anterior and trapezius muscle act together to stabilise the scapula against the thoracic wall. Similarly, elevation of the scapula is regulated by coupling of the upper and lower trapezius muscle, as well as the serratus anterior and the rhomboideus. Dysfunction of these muscles leads to scapular dyskinesis, caused by inflexibility, weakness, and imbalance of the muscles. This dysfunction can be either primary through direct injury of the muscles or secondary as a result of pain induced muscular inhibition.2
In the clinical situation, three types of scapular dyskinesis can be distinguished, although overlap between the three types can be present. The first of these, type I, is inferomedial scapular border prominence, which becomes more evident in the cocking position. It is often associated with tightness at the anterior side of the shoulder (inflexibility of the pectoralis major/minor muscles) and weakness of the lower trapezius and serratus anterior muscles. Posterior tipping of the scapula is responsible for functional narrowing of the subacromial space during the overhead motion, leading to pain in the abduction/externally rotated position. This is often noticed in the early stages of shoulder disorders.
The type II pattern is winging of the entire medial border at rest. It becomes more prominent in the cocking position and after repetitive elevation of the upper extremity, and is caused by fatigue of the stabilising muscles (trapezius, rhomboideus) (fig 4).

Type II scapular dyskinesis of the right shoulder in a man with anterior instability. The patient has given permission for publication of this figure.
Both types of scapular dyskinesis create an abnormal position of protraction at rest, as well as an abnormal pattern of motion during the overhead action. A lack of retraction and elevation of the scapula in the cocking and acceleration phase is present and subsequently leads to an abnormal relation between the humeral head and the glenoid, referred to as “hyperangulation”. In this position, distraction forces occur at the front of the shoulder, which can possibly cause capsular stretching and instability. At the posterior side of the shoulder, compressive forces are generated, which may contribute to posterior impingement of the shoulder (fig 5).

Loss of retraction of the scapula causes an abnormal angle between the humeral head and scapula (thick arrow).
Type III scapular dyskinesis displays prominence of the superior medial border of the scapula and is often associated with impingement and rotator cuff injury. It is clear that scapular dyskinesis plays an important role, but further validation of this clinical finding is needed.
The term “SICK scapula” was introduced to describe a pathological state of the scapula, characterised by scapular malposition, inferior medial border prominence, coracoid pain and malposition, and kinesis abnormalities of the scapula.3 This syndrome, characterised by a drooping shoulder, is often seen in overhead athletes and is thought to contribute to the development of shoulder injuries. In most tennis players such an abnormal position of the scapula can be detected. Although it seems that the affected shoulder has a lower position compared with the healthy side, actually there is scapular malposition consisting of forward tilting and protraction. According to Kibler,3 this clinical picture is associated with anterior coracoid based pain, posterosuperior localised pain, and pain at the superolateral side of the shoulder (subacromial space, acromioclavicular joint). The anterior localised pain in particular can be confused with other causes of anterior shoulder pain, such as instability or a SLAP (superior labrum anterior to posterior) lesion. The pain at the posterior side is caused by insertional pain of the levator scapulae and is due to chronic overtension by the abducted and protracted scapula.
Capsulolabral complex
The role of the capsulolabral complex in the development of a shoulder injury remains a topic of debate. The most important function of the ligaments is to limit the range of motion of the shoulder joint. At the beginning of abduction/external rotation, it is mainly the dynamic stabilisers that keep the shoulder in a central position in the glenoid socket. At the end of the range of motion, the ligamentous structures become more important. At maximal abduction and external rotation, the inferior glenohumeral ligament (IGHL) is taut and limits further movement.4 In the IGHL, a distinctive reinforcement is present, called the anterior band, which moves in front of the humeral head, providing a restraint to anterior and inferior displacement. Behind this, the posterior part of the IGHL shifts in front of the posterior side of the humeral head in abduction and internal rotation, protecting the head against posterior displacement. This dynamic interplay of the ligaments means that, in the overhead athlete, the shoulder area is often susceptible to injury. Several explanations have been developed to clarify the pathogenesis of shoulder injuries in overhead athletes.
As mentioned above, one explanation is that the repetitive nature of the serve causes microtrauma of the anterior capsule. Elongation of the ligaments may be responsible for (subtle) instability. The anterior displacement of the humeral head shifts the centre of rotation to a more anterior position. This probably brings the tuberculum majus and rotator cuff tendon close to the posterior glenoid, causing internal impingement. Although posterior impingement occurs in healthy shoulders, it can become pathological in the tennis player.
Halbrecht et al,5 however, showed that an anterior subluxated shoulder will have less contact at the posterosuperior edge of the glenoid.
When we look at the clinical picture of the shoulder in the overhead athlete, the combination of signs and symptoms cannot be explained by anterior capsular insufficiency alone.
Glenohumeral internal rotation deficit (GIRD)
A common finding in tennis players is a change in the rotational arc of the shoulder. Usually, there is an increase in external rotation and a decrease in internal rotation. Burkhart et al6 proposed that this loss of internal rotation caused by posteroinferior capsular contracture is the essential lesion in thrower’s shoulder. GIRD can be defined as the loss in degrees of glenohumeral internal rotation of the throwing shoulder compared with the non-throwing shoulder. It has been suggested there is an association of GIRD with the development of shoulder injuries.7 If the limitation of internal rotation exceeds the gain in external rotation, resulting in a decrease in rotational arc (>10% of the contralateral side), the shoulder is susceptible to injury.3
According to the theory of Burkhart et al,2 the posterior capsule is subjected to distractive forces in the follow through stage of the overhead motion. These forces (750 N) have to be resisted by the posteroinferior capsule and the compressive forces of the rotator cuff muscles, especially the infraspinatus muscle. These authors believe that these distractive forces cannot fully be compensated for by activity of the infraspinatus muscle. One of the factors contributing to this phenomenon is the eccentric activity of the infraspinatus muscle. Because of the eccentric contraction, adaptive changes occur in the muscle belly. This results in a decrease in active tension, an increase in passive muscle tension, and disturbed proprioceptive mechanisms.8 This thixotropic mechanism of the infraspinatus muscle will contribute to higher loads on the posterior capsule. The posterior capsule reacts with hypertrophy and reduced capsular pliability. The stiffness and shortening of the posterior structures have consequences for stabilisation of the shoulder during abduction and external rotation.
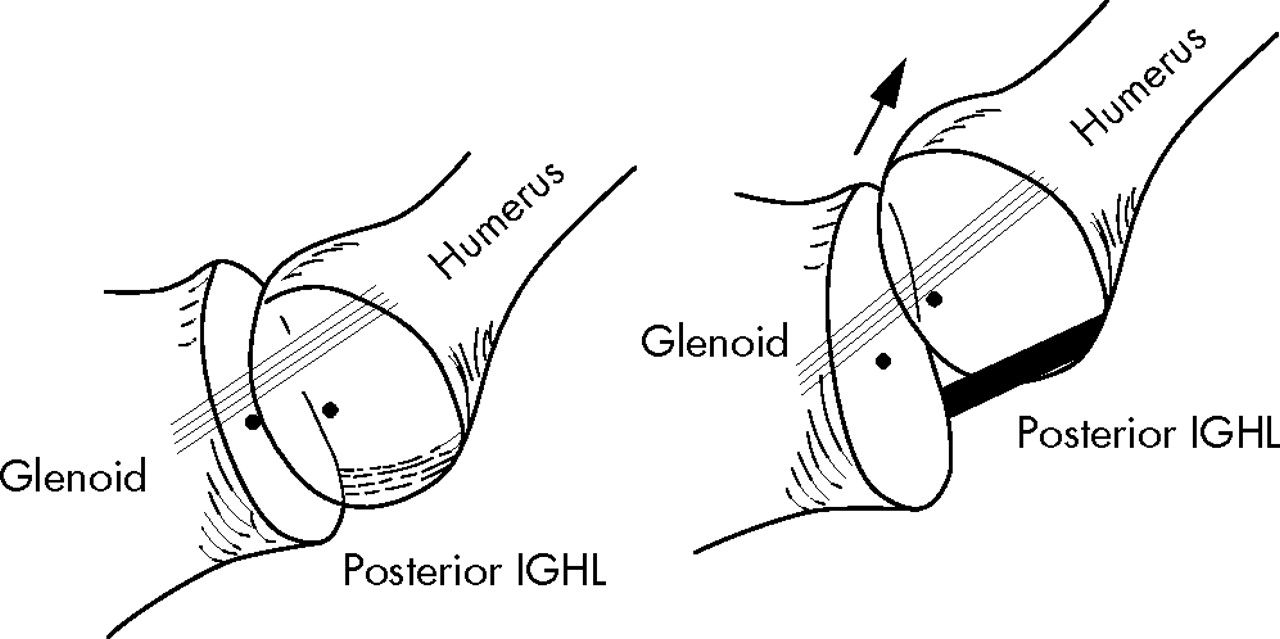
According to the theory of O’Brien et al,9 the IGHL is the most important stabilising capsular component in the shoulder (anterior band in abduction/external rotation; posterior band in internal rotation). In the position of abduction and external rotation of the shoulder, the posterior IGHL is positioned under the humeral head. In the case of a functionally shortened posterior IGHL, a posterosuperior directed force exists, shifting the centre of rotation of the shoulder to a more posterosuperior location (fig 6). The consequences of this posterosuperior shift have been depicted by Burkhart et al6 (fig 2).
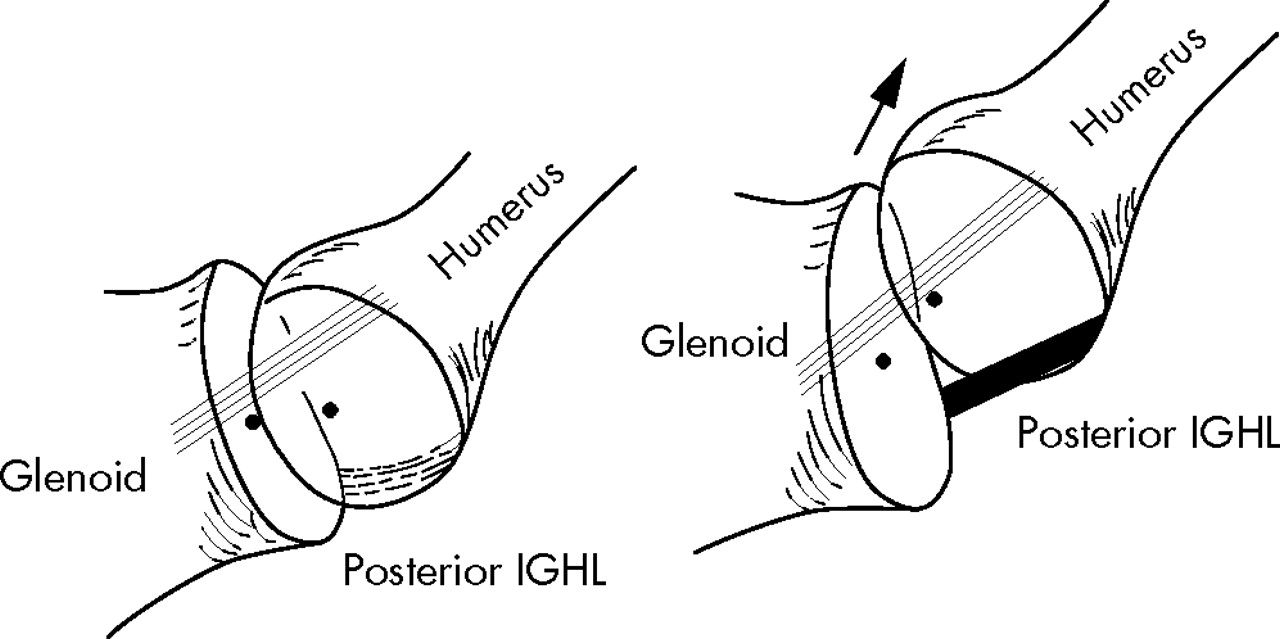
In abduction/external rotation, the posterior inferior glenohumeral ligament (IGHL) shifts under the humeral head. Shortening exerts an upwards directed force, shifting the centre of rotation to a more posterosuperior position.
The hypothesis of Burkhart et al has recently been supported by Grossman et al,10 who found that, by creating a posterior capsular contracture in a cadaveric model, a posterosuperior shift of the centre of rotation occurred in abduction and external rotation.
The relation between SLAP lesion and instability, proposed by this theory, is supported by several studies,11,12 in which an increase in anterior translation was found after creation of a SLAP lesion in cadaveric shoulders. Repairing the lesion led to a return to normal total range of motion and translation.12 This is in accordance with the “circle concept theory” proposed by Burkhart et al6—that is, breakage of the labral ring causes apparent laxity to the opposite side of the ring.
The model described by Burkhart et al seems to be the most appropriate at this time to explain the pathological findings in thrower’s shoulder. In clinical practice, the biomechanical findings correlate well with the clinical signs and symptoms occurring in tennis players with shoulder problems.
HISTORY
Clinical findings show that players initially experience shoulder pain in the late cocking position and acceleration phase of the tennis service, although usually a long history of non-specific pain and a variety of (non)-surgical treatments has preceded this. Most of the time, pain is located deep in the shoulder, often at the posterior side, although anterior localised pain can also be present, because of contracted structures (coracoid based tightness) at the front of the shoulder. Pain is often experienced at the medial side of the scapula, resulting from insertional pain of the scapula stabilising muscles. During the course of the injury, pain is aggravating and the ability to serve at a maximal level is impossible (dead arm syndrome). At a later stage, forehand and backhand strokes may also be impaired. Many patients complain of soreness and stiffness in the shoulder, especially before and after loading of the shoulder. They can also have feelings of instability or clicking sensations.
PHYSICAL EXAMINATION
A shoulder examination starts by inspecting, from behind, the scapula in a resting position. The position of the scapula is defined (see scapular function). Dynamic scapular dyskinesis is detected by asking the patient to raise and/or abduct both arms repeatedly in a rhythmic motion, until fatigue of the scapular stabilisers results in failure to keep the scapula well positioned in relation to the thoracic wall. Active scapular retraction and elevation are checked.
The next step is to look for muscle atrophy. Palpation of areas of tenderness is important, but one should be aware of secondary causes of the pain (insertional pain, secondary impingement, etc). Active and passive range of motion should be examined and compared with the non-injured shoulder. Passive range of motion is best tested with the patient lying on his/her side. In this position, the scapula is fixed and the true passive range of external and internal rotation can be measured (fig 7).

On the left side, passive internal rotation is normal. On the right side, the dominant throwing arm clearly shows limited passive internal rotation. Testing the arc of rotation in this position is the most reliable way to detect differences between the two shoulders. The patient has given permission for publication of this figure.
The next step is to perform tests for impingement (Neer test, empty can test, Hawkins test, external rotation resistance test, etc) and instability (sulcus sign, apprehension test, relocation test, hyper-abduction test, posterior apprehension test). It is wise to perform several tests, because none of them are sufficiently sensitive and specific on their own.13 Therefore the diagnosis can be readily reached with a standard examination.14
In addition, more specific tests can be very useful in examining the shoulder of the overhead athlete. As mentioned above, the position of the scapula is of great importance in the normal functioning of the shoulder. A protracted scapula will cause functional narrowing of the subacromial space, mimicking symptoms of impingement. Kibler3 introduced the scapular assistance test, which can be very useful for detecting a secondary impingement in the shoulder of an overhead athlete. This test involves assisting scapular upwards rotation by manually stabilising the upper medial border and rotating the inferior medial border while the arm is abducted. The test is positive when relief of the impingement symptoms, clicking or rotator cuff weakness, is found. Another helpful test in assessing the role of the scapula is the scapula resistance test, also described by Kibler.3 In this test the entire medial border of the scapula is stabilised in a normal retracted position. The test is considered positive if there is increased muscle strength of the rotator cuff in the stabilised position. Another finding is that pain occurring in the relocation test disappears by repositioning the scapula.
A further striking feature in the throwing shoulder is that posterior localised pain experienced deep in the shoulder in the apprehensive position that disappears during the relocation test may be associated with posterosuperior labral pathology. Several tests have been developed to detect superior labral pathology (active compression test, biceps load test, etc). However, none of these are sufficiently reliable to prove the presence of a SLAP lesion.15,16
It can be hard to establish a provocative test at an early stage of the disease. Sometimes it is possible to provoke specific pain experienced by the athlete in the cocking phase by placing the arm in the cocking position and manually resisting active internal rotation by the athlete from that position, simulating acceleration of the upper arm (the thrower’s test).
The flexibility and strength of the hip and trunk also need to be investigated. A weakness in the hip abductors can be detected by the one leg stance and one leg squat. A loss of control in these positions has been correlated with back and shoulder injury.
IMAGING
A radiographic evaluation may be necessary to establish the diagnosis or to rule out intra-articular pathology. Concomitant pathology can also be detected.14 Magnetic resonance imaging arthrography is considered to be the state of the art technique. Meister17 confirmed high sensitivity and specificity with respect to under surface rotator cuff pathology (>90%), as well as for labral pathology.
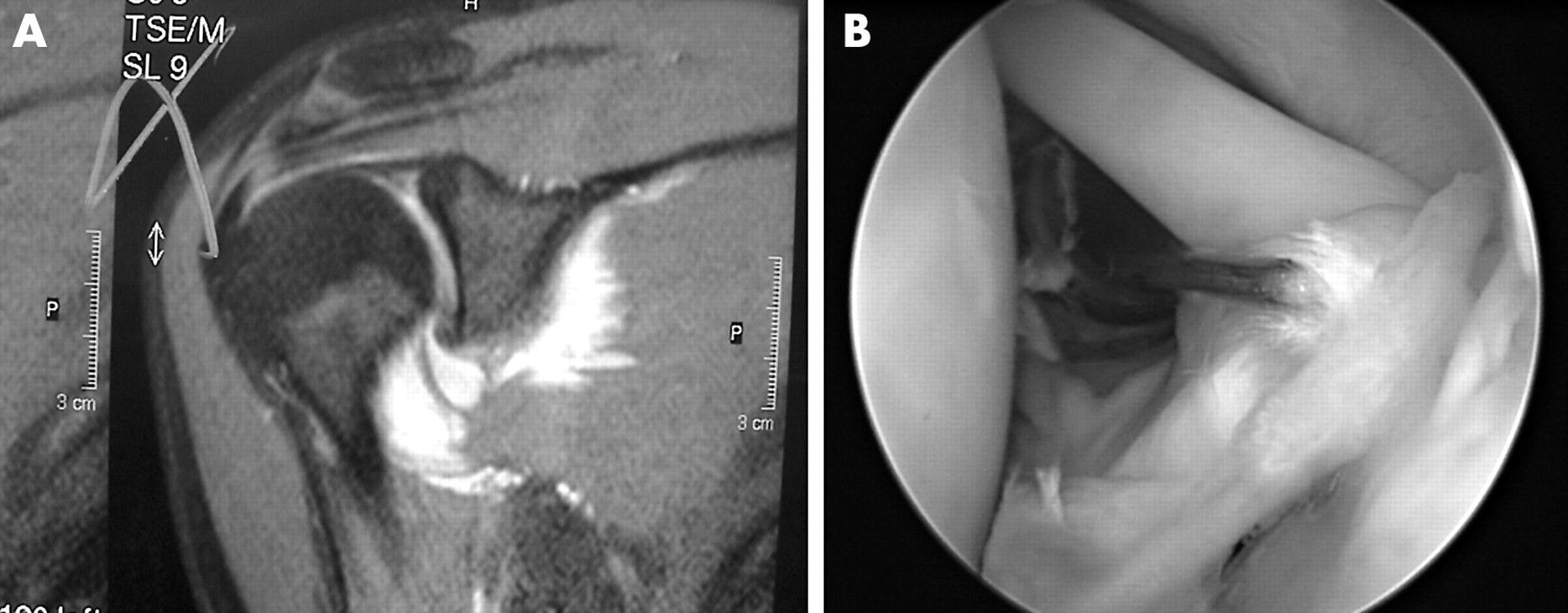
Findings at magnetic resonance imaging can be very difficult to detect. There are many variations in the appearance of the labral attachment to the glenoid. In particular, the superior labrum can be difficult to interpret. A blurring of contrast in the biceps anchor may be the only radiological sign of a SLAP lesion (fig 8).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Blurring of contrast is seen in the superior labrum; (B) an arthroscopic view of the same patient showing extensive damage to the biceps anchor. The patient has given permission for publication of this figure.
IMPLICATIONS FOR TREATMENT
Treatment of these kinds of injury in the tennis player requires a thorough knowledge of the aetiological factors. If only the local damage in the shoulder is treated, treatment is doomed to fail. In evaluating patients, a standard examination should be conducted, and appropriate treatment to improve the function of the kinetic chain prescribed. This is followed by a well founded interpretation of scapular function. Correction of abnormal scapular motion patterns is necessary to improve maintenance of the centre of rotation of the humeral head in every position of the arm. Improvement of retraction of the scapula in the cocking position and stabilisation against the thoracic wall are necessary to guarantee a “full tank of energy” in the late cocking and acceleration phase. Perfect couple forces of the trapezius ascendens/descendens and serratus anterior/rhomboideus are needed for proper elevation of the scapula in order to clear the subacromial space for abduction and external rotation of the shoulder. Concomitantly, a normal active and passive range of motion has to be established. A normal arc of rotation is necessary to allow normal shoulder kinematics. The occurrence of GIRD particularly predisposes these athletes to shoulder injury. Daily stretching of the shortened structures at the posterior side of the shoulder is important. At an early stage of the disease, it may be possible to restore normal range of motion in two weeks, but it will generally take much longer in long standing cases and older athletes.
These are the starting points for rehabilitating the shoulder in the overhead athlete. At a later stage, more selective strengthening exercises for the rotator cuff muscles are added to the programme to improve the dynamic stabilisation of the shoulder. Introducing these exercises too early into the rehabilitation process will lead to overloading of these muscles and a delay in achieving rehabilitation goals. When treatment goals concerned with kinetic chain and scapular function are fulfilled, more sport specific drills are introduced, which gradually build to the level of the desired sporting performance. Periodical evaluation of kinetic chain function, scapular function, and muscular strength can be very useful in preventing shoulder injuries.
OPERATIVE TREATMENT
In more advanced cases, with intra-articular disruption of structures, such as posterosuperior impingement, SLAP lesion, and/or (subtle) instability, surgical treatment may be inevitable. The treatment is directed to the intra-articular pathology. A SLAP lesion can be treated arthroscopically with good to excellent results. Fixing the loose superior labrum to the upper glenoid will stabilise the biceps anchor and neutralise the rotational forces on the biceps anchor, which had led to injury of the superior labrum and the “peel back” phenomenon. In overhead athletes, the lesion of the biceps anchor is usually localised at the posterior part of the glenoid. Stabilisation of the biceps anchor posteriorly is needed to counteract the peel back forces during the overhead action.
Special attention must be given to the integrity of the anteroinferior capsule. If there is still redundancy of the anterior capsule after repair of the biceps anchor, a capsular plication can be added to the surgical procedure. Sometimes an articular sided partial rupture of the rotator cuff is present, which is due to hyper twisting of the tendon fibres and rubbing of the cuff against the posterior glenoid. Debridement of the cuff lesion (usually posterior supraspinatus tendon) and fraying of the superior labrum are sufficient in most cases. In more extensive defects, repair of the cuff may be necessary, influencing the prognosis and rehabilitation protocol. Owing to the probability of combined intra-articular lesions, it is wise to establish a well defined preoperative diagnosis, using a standard physical and radiological examination. This provides the opportunity to develop a well based treatment programme, conservative or surgical. It requires cooperation from the athletes, and establishes well defined treatment goals and a realistic prediction of returning to sport.
RETURN TO SPORT
The results of SLAP repair show that there is a reasonable chance of the athlete returning to the level of sport reached before injury. According to the literature, return to sport can be achieved in most cases. Burkhart and Parten18 found an 87% return to the pre-injury level. Ide et al19 stated that a return to the pre-injury level of sport was possible in 84% of baseball players, but also stated that the success rate in the literature showed great variability (22–92%), and was mainly dependent on the aetiology of the injury—that is, overhead sports showed a lower rate of return to sport than others. The main reason is that the overhead action is an unnatural, complex motion at the physiological limits of the shoulder. Therefore it is crucial to take preventive measures in this patient group. Preseason screening and regular inspection of overhead athletes with respect to kinetic chain function, scapular function, and shoulder function can prevent the development of serious intra-articular damage.
What is already known on this topic
-
The overhead action in throwing sports is unnatural and highly dynamic, often exceeding the physiological limits of the shoulder, making it susceptible to injury
-
Optimal shoulder function requires good kinetic chain function, optimal stability, and coordination of the scapula in the overhead action, and a well balanced action of rotator cuff muscles and capsular structures is necessary to obtain a stable centre of rotation during the overhead action
What this study adds
-
The theoretical assumptions of the pathophysiology of the thrower’s shoulder can be used for the tennis player, as, during the serve, the same phases can be distinguished
-
To reduce the risk of shoulder injury in tennis, careful evaluation of kinetic chain function, scapular function, rotator cuff muscle balance, and the integrity of the capsular structures should be carried out, and specific training programmes incorporating scapular stabilisation and capsular stretching at an early stage of shoulder injury can prevent intra-articular damage of the shoulder
CONCLUSION
Shoulder injuries in tennis players are both a diagnostic and therapeutic challenge. Knowledge of every aspect of the development of shoulder disorders is necessary to apply proper treatment modalities. This includes understanding of the kinetic chain function in tennis, scapular stability, and the interaction of the capsulolabral complex of the shoulder. It is important to recognise early signs of shoulder dysfunction to be able to treat this complex problem at the earliest opportunity. Intervention at an early stage can alter the natural course of the disorder and may prevent the development of serious intra-articular injury.
REFERENCES
Commentary
This article reviews the theories on the pathophysiology of painful shoulders in tennis players. The hypothesis is based on the research of Kibler in throwing sports, which is transposed to tennis players. The theory of the SICK scapula is very useful in clinical practice; however, some aspects have to still to be proven. Distinguishing scapular dyskinesis into three types looks a bit artificial, and they may be just three phenomena of the same pathology. The theory on the contracture of the posteroinferior capsule has yet to be proven, considering the difference in anatomy, where the posterior capsule is quite thin and less strong than the anterior capsule. It has never been shown by arthroscopy or otherwise that the capsule is actually contracted. My final comment is that this review describes what is known so far about shoulder pathology in throwing sports, but does not explain the biomechanics of tennis action and the differences in the movements between tennis and throwing sports.
Footnotes
-
Informed consent was obtained for publication of figures 4 and 7
-
Competing interests: none declared