Article Text

Abstract
Background and aim: Eccentric training has become a popular treatment for patellar tendinopathy. Our purpose was to review the evolution of eccentric strength training programmes for patellar tendinopathy with a focus on the exercise prescriptions used, to help clinicians make appropriate choices and identify areas needing further research.
Methods: A computerised search of the entire MEDLINE database was performed on 1 September 2006 to identify prospective and randomised clinical trials with a focus on clinical outcome of eccentric training for patellar tendinopathy.
Results: 7 articles with a total of 162 patients and in which eccentric training was one of the interventions, all published after 2000, were included. The results were positive, but study quality was variable, with small numbers or short follow-up periods. The content of the different training programmes varied, but most were home-based programmes with twice daily training for 12 weeks. A number of potentially significant differences were identified in the eccentric programmes used: drop squats or slow eccentric movement, squatting on a decline board or level ground, exercising into tendon pain or short of pain, loading the eccentric phase only or both phases, and progressing with speed then loading or simply loading.
Conclusion: Most studies suggest that eccentric training may have a positive effect, but our ability to recommend a specific protocol is limited. The studies available indicate that the treatment programme should include a decline board and should be performed with some level of discomfort, and that athletes should be removed from sports activity. However, these aspects need further study.
Statistics from Altmetric.com
Chronic tendinopathies are common in both recreational and elite athletes. The prevalence of jumper’s knee is high in sports characterised by high demands on leg extensor speed and power, such as volleyball, basketball, soccer and athletics, where as many as 40–50% of participants are affected.1–3 Moreover, the symptoms are often serious, resulting in chronic impairment of athletic performance, and the condition can severely limit or even end an athletic career.1,4
The aetiology and pathogenesis of chronic tendon pain is not fully understood, although histopathological and biochemical evidence indicates that it is not an inflammatory condition.5,6 The incomplete understanding of the underlying pathology limits our ability to establish effective treatment options. Surgery is advocated by some authors in recalcitrant cases,1,7,8 although the benefits of open tenotomy can be questioned on the basis of the result of a recent randomised, controlled study.9 Conservative treatment for patellar tendinopathy may include rest, use of anti-inflammatory drugs, taping, massage, electrotherapy, ultrasound, laser therapy, extra-corporeal shock wave therapy and other modalities.10,11 However, non-surgical treatment methods also need to be evaluated in well-controlled clinical studies.
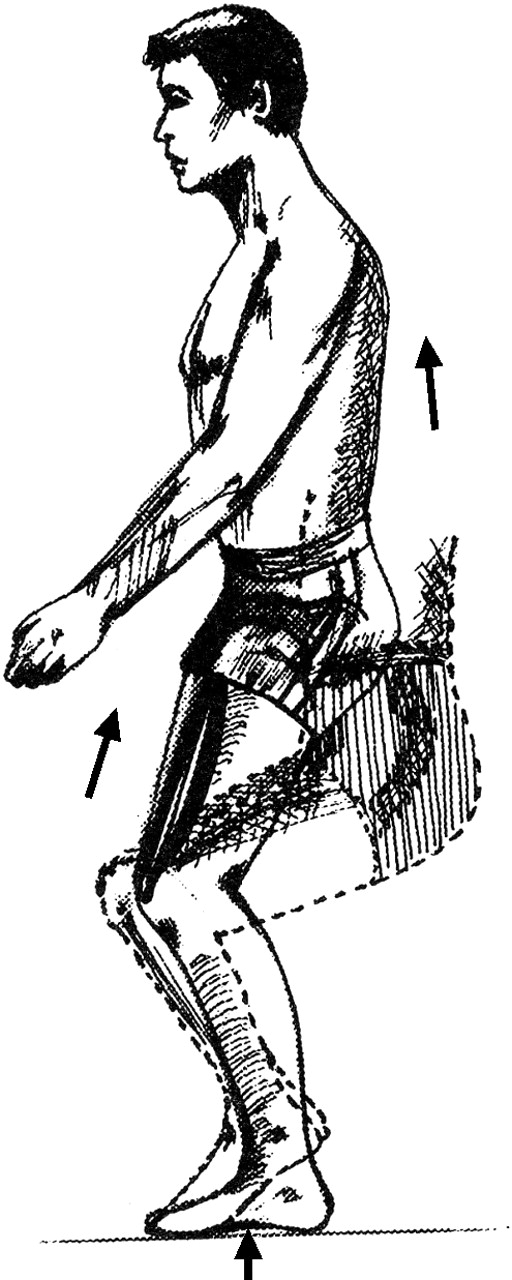
Eccentric training as a treatment option for tendinopathy was first presented by Curwin and Stanish12 in 1984, with encouraging results. Their book presents a treatment programme that includes warm-up and stretching before the eccentric exercise, and stretching and ice afterwards. The programme was based on eccentric drop squats (fig 1 and box 1). When the training became pain-free, load was increased by first increasing the speed of the eccentric phase, and then adding weight.

Patient drops (or lowers) to a semi-squatting position.12
Box 1 The Stanish and Curwin programme12
The eccentric exercise programme for jumper’s knee starts with a general, whole-body warm-up exercise not involving knee extension. The stretching is a static stretch of quadriceps and hamstrings. The patients should hold these at least for 30 s and repeat the exercise three times. The main programme starts with the squatting movements. Patients were instructed to focus primarily on the rapid deceleration phase between the downward and upward movement phases. The progression was defined as no added resistance on days 1 and 2 (slow) and increased speed on days 3–7. In week 2, resistance was added (10% of body weight). In weeks 3–6, 4.5–13.5 kg was added progressively. Subjects were instructed to do three sets of 10 repetitions once daily, which was reduced to three sets of 10 after 6 weeks, three times weekly. Every session ended with the same static stretch exercise as in the warming-up phase. The patients were also instructed to use ice on patellar tendon for 5 min after programme.
Although eccentric training has been used by some to treat patients with various forms of tendinopathy since the mid-80s, research interest in this treatment form was limited until Alfredson et al13 published their paper on Achilles tendinopathy in 1998. Their training model had some potentially important differences from the Curwin and Stanish12 model, mainly that the eccentric movement was defined as a slow movement, that treatment progressed by adding not speed but load, and that the patients were instructed to exercise despite pain during the eccentric movement (fig 2 and box 2).

The Alfredson Achilles tendon programme:13 from an upright position and standing with all weight on the forefoot and the ankle joint in plantar flexion (A), the calf muscles are loaded eccentrically by having the patient lower the heel with the knee straight (B) or slightly flexed (C).
Box 2 The Alfredson eccentric Achilles tendon programme13)
The patients were instructed to do their eccentric exercises two times daily, 7 days/week, for 12 weeks. Running activity was allowed if it could be performed with only mild discomfort and no pain. Two types of eccentric exercises were used. The calf muscle was eccentrically loaded both with the knee straight and, to maximise the activation of the soleus muscle, also with the knee bent. Each of the two exercises included 15 repetitions done in three sets. The patients were told that muscle soreness during the first 1–2 weeks of training was to be expected. In the beginning, the loading consisted of the body weight, and the patients were standing with all their body weight on the injured leg. From an upright body position, the calf muscle was loaded by having the patient lower the heel beneath the forefoot. They were only loading the calf muscle eccentrically; no concentric loading was used. Instead, the non-injured leg was used to return to the start position. The patients were told to go ahead with the exercise even if they experienced pain. However, they were told to stop the exercise if the pain became disabling. If they could perform the eccentric loading exercise without experiencing any minor pain or discomfort, they were instructed to increase the load by adding weight. This was done by using a backpack that was successively loaded with weight. If very high weights were needed, the patients were told to use a weight machine.
The first studies evaluating eccentric training as treatment of Achilles tendinopathy concluded that eccentric training is an appropriate treatment for mid-portion Achilles tendinopathy.13–15 The results of these prospective studies were good, and many chronic patients became pain-free. Since then, further studies on the Achilles tendon have focused less on clinical outcome and more on changes in tendon structure as evaluated by MRI or ultrasonography.6,16,17
The advent of the Alfredson13 protocol for Achilles tendinopathy has spurred recent research interest in eccentric training as treatment for patellar tendinopathy. The purpose of this review is to describe the evolution of eccentric strength training programmes for patellar tendinopathy with a focus on the exercise prescriptions used, to help clinicians make appropriate choices, and to identify areas needing further research.
METHODS
A computerised search of the entire MEDLINE database was performed on 1 September 2006. Table 1 lists the keywords used in the search. The search was limited to literature in English. All articles relevant to the subject were retrieved. In order to be included in this review, the design had to be a prospective study or a randomised clinical trial. The paper had to focus on clinical outcome and had to document how this was defined. The references selected were reviewed by the authors and judged on their contribution to the body of knowledge. Review articles and editorial comments were not included. In addition, reference lists of articles selected from this search, and previous review papers were searched for relevant articles.
Results from MEDLINE search (1966–September 2006)
RESULTS
We identified seven articles on the clinical effects of eccentric training on patellar tendinopathy,9,18–23 all published after 2000, and including a total of 162 patients. Of these, 112 patients were included in the groups assigned to various forms of eccentric training. Table 2 presents the main study characteristics.
Studies on the effect of eccentric training on patellar tendinopathy
The first paper describes a small pilot study by Cannell et al,18 comparing eccentric drop squat with concentric leg extension/curl exercise. Their eccentric model was based on the Curwin and Stanish12 programme, using eccentric drop squats with a rapid deceleration phase, performed by starting from a standing position and unlocking the knees rapidly. Subjects were advised to use the quadriceps muscles of both legs to stop their fall just short of the thighs being parallel to the ground. Subjects were encouraged to ice their patellar tendons after performing the drop squat programme, and were treated with anti-inflammatory drugs and relative rest in the first 2 weeks. When they could do three sets of 20 drops easily, they progressed to the next level. The programme prescribed a detailed progression through four different levels, which included adding gradually increasing weights and an alternate daily running programme beginning with 1 km and increasing by 1 km every third run, with intensity increasing from one level to the next. One notable feature of this exercise programme is that both legs were trained at the same time. The control group performed a similar programme of leg extension and curl exercises, which were performed slowly to provide concentric loading. After 12 weeks, both groups had a significant reduction of pain, but there was no difference between the groups. Nine of 10 subjects who performed the drop squat programme returned to sporting activity by 12 weeks, as did six of the nine subjects who performed the leg extension/curl programme (no significant difference). It should be noted that there was no extended follow-up after the end of the treatment period.
The most notable difference between this and the subsequent studies is that these employed training programmes based on the Alfredson13 model, with painful, slow eccentric exercise. In the first of these, a small, non-randomised study by Purdam et al,19 single-leg eccentric training on a decline board was compared with performing the same exercise with the foot on a flat surface. The training programme was the same for both groups; the only difference was the use of a decline board. The exercise was completed with the trunk in an upright position, and subjects were instructed to perform the exercise by slowly bending the knee to 90° of flexion. They were told to perform the eccentric loading on the quadriceps muscles only and to return to the starting position using the non-injured side. If they had bilateral tendinopathy, the arms and both legs were used to return to starting position. Subjects were asked to increase the load with weights in a backpack once the exercise could be completed without pain. As prescribed in the Alfredson programme,13 load was increased so that exercises were always performed with some pain or discomfort. Subjects were not allowed to continue their competitive sporting activity during the first 8 weeks of the treatment period. After 4 weeks of the eccentric training regimen, they were allowed to complement it with slow jogging on flat ground, and cycling and water activities, if these could be performed without sharp pain in the patellar tendon. After 8 weeks, the patients were allowed to return gradually to previous activity. The results showed that after 12 weeks, there was a significant decrease in the amount of pain during activity in the nine patients in the decline squat group, and no change in the flat floor group. Only one of nine returned to sport in the standard flat floor group, compared with six of eight patients in the decline board group. However, of these six, only four were still active at pre-injury levels when they were followed up after 15 months.
In a paper from the same group, Young et al21 compared eccentric training performed on a decline board with eccentric drop squat training performed with the foot placed flat on a 10 cm box. The decline training group used the same programme as Purdam et al,19 the only changes being that the squats were completed to about 60° of knee flexion instead of 90°, and that they specified that load was increased by adding weight to a backpack in 5 kg increments. In contrast, the flat step group was instructed to exercise with minimal tendon pain only and progress their speed from slow to fast, as outlined in the Curwin and Stanish protocol,12 completing both components of the squat on the symptomatic leg. When subjects could complete their squats at a fast speed, they increased load in the same manner as the decline board group. Both groups used single (affected) leg training. The results showed that both groups had significantly improved scores on the Victorian Institute of Sport Assessment (VISA) and a visual analogue scale (VAS) during the 12-week training period, and that this improvement was maintained after 12 months, but that there was no difference between groups for either outcome measure at any time.
Stasinopoulos and Stasinopoulos20 compared eccentric training with two other treatment methods: pulsed ultrasound and transverse friction. The eccentric training programme also included static stretching exercises before and after the training session, as described by Jensen and Di Fabio.24 The eccentric programme was built on the principles of the Alfredson programme,13, although it was performed only three times a week. Subjects used unilateral, slow eccentric squats, and the leg was unloaded in the concentric phase as the non-injured leg was used to get back to the starting position. Subjects were told to go ahead with the exercise even if they experienced mild pain, but to stop if the pain was disabling. The authors claimed a 100% success rate in the eccentric group, but no validated outcome measures were used and the patients were followed for only 3 months after the 4-week treatment period.
In a randomised trial on competitive volleyball players, Visnes et al22 used a similar treatment programme to the decline groups in the studies by Purdam et al19 and Young et al.21 The main difference was that the athletes were allowed to train and compete as usual during the treatment period. Otherwise, the same principles with slow, painful decline squats were applied by the eccentric training group (fig 3 and box 3). The control group continued to train as normal. The results showed that there was no change in VISA score during the intervention period in the training or control group, nor was there any change during the follow-up period at 6 weeks or 6 months. This indicates that it may not be possible to combine sports participation and eccentric exercises twice daily, and that the total load on the tendon was too high, resulting in increasing tendon soreness.

{kind=link}
{kind=link}
{kind=link}
The patellar training programme. (A) Starting position for eccentric training on a 25° decline board with the entire weight on the injured leg. From this position, the knee was slowly flexed to 90°. (B) End position for eccentric training.
Box 3 The eccentric training programme on the patellar tendon22
The players performed the eccentric training programme on a 25° decline board. Each training session was to be completed two times daily with three sets of 15 repetitions in each session. The exercises could be performed without warming up. The downward component (eccentric component) was on the affected leg, and the upward component on the asymptomatic leg. If both legs were injured, the subjects were instructed to use their arms to assist during the concentric phase and train only one leg at a time. They were instructed to take 2 s for each eccentric component of each exercise, and to avoid bending forward but keep the back as vertical as possible throughout the squat. The squat went to 90° of knee flexion, which ensured that the subjects went past 60° of knee flexion, the joint angle thought to place maximal load on the patellar tendon. The subjects were instructed to exercise despite pain during exercise, but to stop if the pain became disabling. They were recommended to have a pain value of 4–5 on a visual analogue scale during the eccentric training sessions (0, no pain and 10, the worst pain ever). Load was increased as pain decreased, and they added load in a backpack in 5 kg increments. Those with pain <3–4 on the VAS were recommended to increase the weight. Players with pain >6–7 on the VAS during the exercises were recommended to do the exercise with less weight.
Jonsson and Alfredson23 compared an eccentric training programme using a decline board with a concentric programme on a decline board. The starting position for the eccentric quadriceps training was standing on the 25° decline board with the entire body weight on the injured leg. From that position, the knee was slowly flexed to 70°. The starting position for the concentric quadriceps training was standing on the 25° decline board with the entire body weight on the injured leg and with the knee in 70° flexion. From that position, the knee was slowly straightened to full extension. All patients were instructed to cease sporting activities for the first 6 weeks. At the 12-week follow-up, pain scores were significantly lower and VISA scores significantly higher in the eccentric training group compared with the concentric training group, and the patients were satisfied with treatment for 9 of 10 tendons. In the concentric group, pain levels remained high and no patient was satisfied with the result of the treatment. At follow up >2 years later, patients in the eccentric group were still satisfied and active in sports, whereas all patients in the concentric group had been treated surgically or by sclerosing injections. The study had aimed to include 20 patients in each group, but was stopped at the half-time control because of poor results in the control group.
In the most recent study on eccentric training, Bahr et al9 compared the effect of eccentric training with that of surgical treatment with open tenotomy. Subjects in the surgical treatment group also performed the same eccentric training programme as part of their rehabilitation after surgery. The eccentric programme was the same programme as that used by Visnes et al22 (fig 3 and box 3). During the first 8 weeks of treatment, the patients were not allowed to take part in sports-specific training. After 4 weeks, they were allowed to cycle, to jog on a flat surface or to exercise in water, if these activities could be done without pain. After 8 weeks, the patients were allowed to gradually return to their sport if there was no or minimal pain. The results showed that, although both treatment options resulted in a definite improvement in knee function, there was no measurable difference between the groups. Only half of all patients were able to return to sport within 1 year after treatment with either option, and even fewer had relief of all symptoms.
DISCUSSION
All seven studies included concluded that eccentric training has an important role in the conservative treatment of patellar tendinopathy. Even if the results should be interpreted with caution, the effect of the treatment could be estimated to give the patients a 50–70% chance of improvement of knee function and pain, so that they could return to pre-injury level of sports activity. However, the quality of the studies is variable; some are non-randomised, some are pilot studies with small numbers and some have not followed the patients for a sufficient post-treatment period.
Moreover, this review shows that there are a number of potentially significant differences in the different eccentric programmes used: drop squats or slow eccentric movement, squatting on a decline board or level ground, exercising into tendon pain or short of pain, loading the eccentric phase only or both phases, and progressing with speed, then loading or simply loading. On the basis of these differences in the exercise prescription, it would be inappropriate to attempt a quantitative meta-analysis of the clinical outcome after eccentric training for patellar tendinopathy. Thus, in the current review, we have chosen to focus on the training protocols, to examine whether there is sufficient evidence to provide guidance for clinicians, and possibly also inspire research directed at defining the most appropriate treatment protocol.
To date, no study has made a direct comparison of the effect of slow eccentric training based on the Alfredson programme13 with that of drop squat exercise based on the Curwin and Stanish model12; further studies are needed to investigate this issue. Young et al21 compared slow eccentric training with drop squats, but the groups also differed in other respects. The slow eccentric training group was trained with pain or discomfort and on a decline board, whereas the drop squat group was trained with no pain and on a 10 cm flat surface step.
A decline board has been used in five studies,9,19,21–23 and all the more recent studies in this review use the same principle. The introduction of the decline board was based on a biomechanical study by Purdam et al,25 which suggested that the load on the patellar tendon could be maximised by performing the squats on a 25° decline board. In the same way, the rationale for keeping the trunk in the upright position was to minimise involvement of the hip extensors. This theory has recently been supported by Kongsgaard et al,7 who showed that patellar tendon strain is significantly greater, stop angles of the ankle and hip joints are significantly smaller, and electromyographic (EMG) amplitudes of the knee extensor muscles are significantly greater during the decline compared with standard squats. Purdam et al19 made a direct comparison, using the same eccentric training programme, between using a decline board and exercising on a flat floor. In this pilot study, decline board training resulted in improved pain scores, whereas there was no short-term change in the regular squat group. Thus, although the evidence is limited, based on these results and the biomechanical rationale, the decline board now seems to have become a standard component of most eccentric training programmes.
A major change was Alfredson’s principle of exercising into tendon pain. In contrast, the original Curwin and Stanish programme12 prescribes that “the intensity of the exercise should be such that pain, or discomfort, is experienced in the last set of 10 repetitions”. However, there are no studies comparing slow eccentric training with pain versus training with minimal or no pain, and therefore there is no documentation on how much pain and discomfort should be recommended. Further research is clearly needed to deal with this issue.
Most programmes load only during the eccentric phase, and patients were instructed to use their non-affected leg and/or arms in the concentric phase of the movement. Jonsson and Alfredson23 showed that eccentric training alone was effective, while concentric training only produced no effect. However, whether the affected leg can be trained in both phases has not been studied in patients with patellar tendinopathy.
Progressing was done by adding weight or by increasing speed and then adding weight. However, these contrasting prescriptions have not been compared directly in studies. In addition, there are large variations on when and how other training (running, sports-specific training) is introduced. Most studies do not allow other training during the first 6 weeks of eccentric training. Visnes et al,22 in contrast, tried to combine treatment with eccentric training with regular volleyball competition and training at the same time. In this study, the treatment group did not show any improvement. The authors’ interpretation was that the combined load of the treatment programme and volleyball training exposed the tendon to too much stress.
Most recent studies have used a home-based exercise programme with three sets of 15 repetitions twice a day for 12 weeks, although the total number of sessions varied between studies from 168 to 12 (3 times a week for 4 weeks). There is no documentation on the ideal frequency and volume of training or on the length of the treatment period. Most studies have simply copied the prescription from the Achilles programme. However, it should be noted that, even if the number of sessions was the same, the Achilles programme involves three sets of 15 repetitions with the knee straight and three sets of 15 repetitions with the knee bent. Hence, it should be noted that the total training volume of the Achilles programme is twice as high as that used in the patellar tendon programmes. Further research is needed to study the influence of differences in training loads on treatment outcome.
Curwin and Stanish presented a total rehabilitation programme that included warm-up, stretching, drop squat exercises, stretching and cool down with ice.12 In all but one of the seven studies included in this review, the treatment programme consisted of eccentric training only.9,18,19,21–23 A clinical approach will often be more complex than eccentric training alone. However, the effect of factors such as stretching, use of ice and warming up has not been studied properly.
What is already known on this topic
-
Eccentric training has become a popular conservative treatment model for patellar tendinopathy.
What this study adds
-
Even if most studies suggest that eccentric training may have a positive effect, our ability to specify which protocol component is responsible for the observed effects is limited.
-
The studies available indicate that the treatment programme should include a decline board, should be performed with some level of discomfort, and that athletes should be removed from sports activity.
In conclusion, even if most studies suggest that eccentric training may have a positive effect, our ability to specify which protocol component is responsible for the observed effects is limited. The studies available, which are small and of variable quality, indicate that the treatment programme should include a decline board, should be performed with some level of discomfort, and that athletes should be removed from sports activity. However, these aspects need further study.
Acknowledgments
The Oslo Sports Trauma Research Center has been established at the Norwegian School Sport Sciences through generous grants from the Norwegian Eastern Health Corporate, the Royal Norwegian Ministry of Culture, the Norwegian Olympic Committee and Confederation of Sport, and Norsk Tipping AS.
REFERENCES
Footnotes
-
Published Online First 26 January 2007
-
Competing interests: None declared.