Article Text

Abstract
Background: The placement of automated external defibrillators (AEDs) in schools and public sporting venues is a growing national trend.
Objective: To determine the prevalence and use of AEDs in Washington State high schools and to examine the existing emergency preparedness for sudden cardiac arrest (SCA).
Design: Cross-sectional survey.
Setting: High schools in Washington State.
Participants: The principal at each high school in the Washington Interscholastic Activities Association (n = 407) was invited to complete a web-based questionnaire using the National Registry for AED Use in Sports (http://www.AEDSPORTS.com).
Main outcome measurements: The primary outcome measures studied included AED prevalence and location, funding for AEDs, AED training of school personnel, coordination of AED placement with local emergency response agencies, and prior AED use.
Results: 118 schools completed the survey (29% response rate). 64 (54%) of the schools have at least one AED on school grounds (mean 1.6, range 1–4). The likelihood of AED placement increased with larger school size (p = 0.044). 60% of AEDs were funded by donations, 27% by the school district and 11% by the school or athletic department itself. Coaches (78%) were the most likely to receive AED training, followed by administrators (72%), school nurses (70%) and teachers (48%). Only 25% of schools coordinated the implementation of AEDs with an outside medical agency and only 6% of schools coordinated with the local emergency medical system. One school reported having used an AED previously to treat SCA in a basketball official who survived after a single shock. The estimated probability of AED use to treat SCA was 1 in 154 schools per year.
Conclusions: Over half of Washington State high schools have an AED on school grounds. AED use occurred in <1% of schools annually and was effective in the treatment of SCA. Funding of AED programmes was mostly through private donations, with little coordination with local emergency response teams. Significant improvement is needed in structuring emergency response plans and training targeted rescuers for an SCA in the high-school setting.
- AED, automated external defibrillator
- AHA, American Heart Association
- CPR, cardiopulmonary resuscitation
- EAP, emergency action plan
- EMS, emergency medical system
- SCA, sudden cardiac arrest
- SCD, sudden cardiac death
Statistics from Altmetric.com
- AED, automated external defibrillator
- AHA, American Heart Association
- CPR, cardiopulmonary resuscitation
- EAP, emergency action plan
- EMS, emergency medical system
- SCA, sudden cardiac arrest
- SCD, sudden cardiac death
The placement of automated external defibrillators (AEDs) in high-risk public locations for cardiac arrest and use by trained or untrained responders has shown a clear survival benefit in the treatment of out-of-hospital cardiac arrest.1–5 The favourable results shown in public access defibrillation trials combined with the desire to prevent sudden cardiac death (SCD) in young athletes have accelerated the implementation of AEDs in schools and public sporting venues. In the National Collegiate Athletic Association Division I universities, over 90% of schools have already placed AEDs at selected athletic venues.5 Few studies have assessed the presence and impact of AEDs in the high school setting.6–8 The purpose of this study was to determine the prevalence and utilisation of AEDs in Washington State high schools and to examine existing emergency preparedness for sudden cardiac arrest (SCA).
METHODS
The principal at each high school in the Washington Interscholastic Activities Association (n = 407) was invited to complete a web-based questionnaire using the National Registry for AED Use in Sports (http://www.AEDSPORTS.com) in November 2005, with a follow-up invitation sent in December 2005. The survey consisted of questions regarding the prevalence, location and past utilisation of AEDs. Schools reporting a prior AED utilisation were contacted directly to clarify the circumstances and outcomes of the AED use. Schools without AEDs were asked to identify the obstacles to acquiring an AED. The survey also investigated emergency preparedness for SCA in high schools, AED training of school personnel, and coordination of existing emergency action plans with outside emergency medical agencies. Selected information on the prevalence of AED was requested from 53 non-responding schools via email in June 2006. Non-responding schools contacted in follow-up were chosen through random sampling.
Size classification of high schools was based on the Washington Interscholastic Activities Association taxonomy derived from total student enrolment in grades 10–12. Schools with ⩾1201 students were classified as 4A, those with 601–1200 enrolment as 3A, those with 301–600 enrolment as 2A, those with 151–300 enrolment as 1A, and those with 1–150 enrolment as B. The location of the school was subdivided into urban/inner city, suburban and rural settings. Categorical data were analysed by χ2 analysis or Fisher exact test if the expected cell frequency was <5 (SPSS V.11.5). Two-sided p values are reported. The study was approved by the Human Subjects Division of the University of Washington, Seattle, Washington, USA.
RESULTS
AED prevalence and location
In all, 118 schools completed the survey (29% response rate). Of these, 64 (54%) schools have at least one AED on school grounds (mean 1.6, range 1–4). Larger schools were more likely to have AEDs than smaller schools, χ2 test for trend = 4.07 (1 degree of freedom (df), p = 0.044; table 1). AED prevalence was no different based on the location of the school (urban, suburban and rural, χ2 = 3.28, 2 df, p = 0.19), or between public and private schools (Fisher exact test, p = 0.59). The most common locations for an AED were the training room (23%), basketball facility (17%), classroom building (17%) and nurse’s office (14%). Schools had had AEDs in place for an average of 2.4 (range 1–11) years.
Automated external defibrillator prevalence at Washington State high schools
AED funding
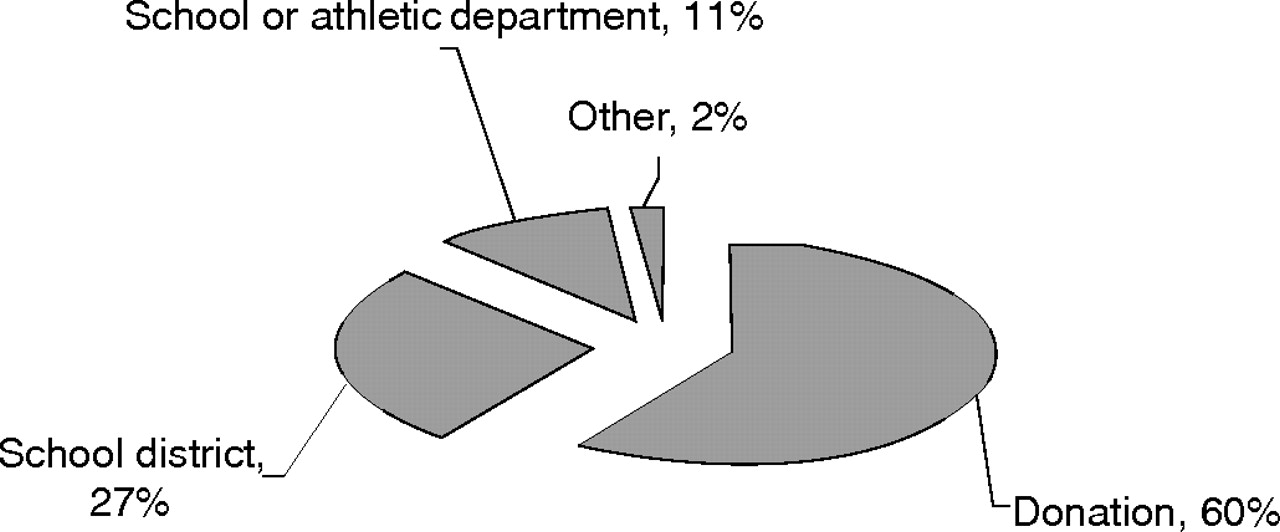
Washington State high schools with an AED had received funding to purchase the AED predominantly through outside donations. In all, 60% of AEDs were funded by donations, 27% by the school district, and only 11% by the school or athletic department itself (fig 1).

Funding for automated external defibrillators in Washington State high schools.
AED training and emergency coordination
In schools with AEDs, coaches (78%) were the most likely to receive AED training, followed by administrators (72%), school nurses (70%) and teachers (48%). Only 16 (25%) of 64 schools coordinated the implementation of AEDs with an outside medical agency, with only 4 (6%) schools coordinating with the local emergency medical system (EMS), 2 (3%) schools coordinating with a local medical centre, and 1 (2%) school coordinating with the local police (fig 2).

{kind=link}
{kind=link}
Coordination of automated external defibrillator implementation with local emergency response teams for Washington State high schools.
AED utilisation
One school reported having used an AED previously to treat a basketball official with SCA. After collapsing, the official was treated by an athletic trainer who applied the AED and delivered a single shock for presumed ventricular fibrillation. The official was successfully resuscitated at the scene, was alert before transport to the emergency department, and survived to hospital discharge. One additional school brought an AED to the scene of a school accounting employee who had an acute myocardial infarction without cardiac arrest. Although the presence of the AED was valuable and provided an additional measure of safety, the AED was never applied or used in that case. With 64 schools having AEDs for an average of 2.4 years, the estimated likelihood of AED use to treat SCA was 1 in 154 schools per year, or an annual probability of 0.65%. No cases of AED utilisation to treat a student athlete with SCA were reported.
Obstacles to acquiring AEDs
In all, 65% of high schools without AEDs identified monetary resources as the main obstacle, and 17% identified monetary resources as the second most important obstacle for acquiring AEDs. Medical–legal concerns accounted for 20% of primary and secondary obstacles to acquiring AEDs.
Non-responders
Fifty-three initially non-responding schools were randomly selected and asked to respond to selected questions on AED prevalence. Of these only 11 non-responding schools completed the follow-up survey (21% response rate). In all, 5 of 11 (45%) schools currently have at least one AED on school grounds. Two additional schools recently obtained grant funding and were in the process of obtaining an AED for the following school year. The limited response to the follow-up survey of schools that did not respond initially indicates no difference in the prevalence of AEDs by the initial respondents and the non-respondents who answered the follow-up contact (Fisher exact test, p = 0.75).
DISCUSSION
Survival following out-of-hospital cardiac arrest has been greatly improved by lay rescuer and public access defibrillation programmes designed to shorten the time interval from SCA to shock delivery. Studies achieving rapid defibrillation by placing AEDs with non-traditional first responders or in high-risk locations such as casinos, airlines and airports for public access and use by trained or untrained laypersons have demonstrated survival rates as high as 41–74% if bystander cardiopulmonary resuscitation (CPR) is provided and defibrillation occurs within 3–5 min of collapse.1–5,9–12 Key elements to the success of these programmes include training of motivated responders in CPR and AED use, short response times, and a structured and practised response.
The success of public access defibrillation studies has accelerated broad implementation of AED programmes in schools and at public sporting venues. In 2001, 25% of high schools in California and Iowa were found to have an AED on school grounds,8 and in 2004, 35% of high schools in Wisconsin voluntarily implemented AED programmes.6 This study found a 54% prevalence of AEDs in Washington State high schools, and suggests a growing national trend towards school AED programmes.
SCA is a rare but catastrophic event and the leading cause of death in young athletes.13,14 The best available studies estimate the incidence of SCD in high-school athletes to be 1:100 000–1:200 000.14,15 However, with no mandatory national reporting or surveillance system, the true incidence of SCA/SCD in athletes is unknown, and prior reports may have underestimated the actual occurrence of SCA/SCD in young athletes. SCA is more common in the older population, with an estimated frequency of 1 in 1000 people aged ⩾35 years in the US.16 The placement of AEDs in schools and sporting facilities provides a means of early defibrillation for young athletes and also for other individuals on campus with SCA. Jones et al8 found a 2.1% annual probability of SCA on high-school campuses mainly due to SCA among older school employees, spectators and visitors on campus. This study found an annual probability of AED use for SCA of 0.65%. At Division I universities, older non-students such as spectators, coaches and officials also accounted for the majority of AED use, representing 77% of AED use for SCA at collegiate athletic facilities.5 In this study, no cases of AED utilisation to treat a student athlete with SCA were reported. Because of the lower incidence of SCA in the young athletic population, the effect of high-school AED programmes on young athletes with SCA requires further long-term investigation.
Financial resources are the primary obstacle for high schools with budgetary constraints to implement an AED programme. In this study, 60% of high schools funded the acquisition of an AED through donated funds, and 65% of schools without AEDs identified monetary resources as the primary obstacle to acquiring an AED. In the greater Boston area, after a single AED was donated to 35 schools, 25 schools purchased additional AEDs using predominantly donated funds (n = 21) and grants (n = 11), and less commonly through school budget resources (n = 8).7
School nurses, teachers, coaches, administrators and athletic trainers may be called upon to provide emergency care during school hours and extracurricular sporting activities. However, emergency training for many of these potential first responders has been inadequate. A survey of school nurses in New Mexico documented that few school nurses and staff had any emergency training.17 In the Midwest, one-third of teachers surveyed had no first aid training and 40% had never completed a course in CPR.18
AEDs alone are not sufficient for adequate emergency preparedness, but should be part of a more comprehensive emergency action plan (EAP). Essential elements for a comprehensive EAP include
-
establishing an effective communication system;
-
establishing a coordinated and practised response plan;
-
risk reduction to prevent injuries;
-
training of likely first responders in CPR and AED use; and
-
access to early defibrillation and/or implementation of an AED programme.19
Rescuers should be trained and equipped to recognise SCA, activate the EMS system, provide CPR and use an AED.
As demonstrated in this study, significant deficiencies in emergency planning and coordination still exist in high schools. Only 25% of high schools coordinated the implementation of AEDs with any outside medical agency, and only 6% of schools coordinated with their local EMS. The divergence of AED prevalence and appropriate emergency planning in consultation with local emergency resources may be associated with the high reliance on donated funds to purchase the AEDs and also represent a lack of funding or planning of a more comprehensive EAP.
Studies involving AED implementation as part of a comprehensive EAP have demonstrated great success. In the greater Boston area, 35 high schools were donated a single AED and educated in the development of a protocol to train appropriate staff and assess the need for purchasing additional AEDs.7 In this study, 90% of schools trained their faculty, 76% trained their staff and custodial workers, 71% trained their athletic trainers, and 48% trained some or all of their student body in AED use.7 Over a 2-year study period, an AED was used successfully in two cases of SCA (one occurring in a referee and the other in a teacher). Every school participating in the study found participation in an AED programme to be worthwhile.7 Similarly, in the state of Wisconsin, the Automated Defibrillators in Adam’s Memory project has assisted 143 of 400 public high schools implement an AED programme as part of a comprehensive EAP. The goals of the Automated Defibrillators in Adam’s Memory project include education of faculty, staff, parents, students and healthcare professionals about SCA in children and adolescents and advocacy for teaching CPR and AED use to all high-school students before graduation.20
The American Heart Association (AHA) released a scientific statement on response to cardiac arrest and selected life-threatening medical emergencies and the medical emergency response plan for schools in 2004.19 The AHA recommends implementation of an AED programme in schools with one of the following:
-
The frequency of cardiac arrest is such that there is a reasonable probability of AED use within 5 years of rescuer training and AED placement.
-
There are children attending school or adults working at the school who are thought to be at high risk of SCA (eg, children with congenital heart disease).
-
An EMS call-to-shock interval of <5 min cannot be reliably achieved with conventional EMS services, and a collapse-to-shock interval of <5 min can be reliably achieved (in >90% of cases) by training and equipping laypersons to function as first responders by recognising SCA, activating the EMS system, starting CPR and using an AED.19
Schools sponsoring organised athletic programmes must determine whether a time interval of <5 min from collapse to defibrillation can be reliably achieved with the conventional EMS system or whether an AED programme is required to achieve early defibrillation. Studies suggest that for most EMS systems the time interval between activating the EMS and arrival of EMS personnel at the victim’s side is usually >5 min (mean 6.1 min),21 and in some communities the time interval from EMS call to EMS arrival may be 7–8 min or longer.22 The EMS response time to arrive at the scene of an intercollegiate athlete with SCA averaged 7 min.23 Thus, achieving early defibrillation after SCA is largely dependent on the prompt availability of AEDs for responders. In high-school athletic programmes, coaches, officials, athletic trainers and other sports medicine professionals are in a unique position to act as first responders to SCA during organised training and competition. On-site AED programmes are likely to be the only means of achieving early defibrillation.
Every school sponsoring athletic activities should have a written EAP.24 The school should coordinate the plan with the local EMS agency and integrate it with the local EMS system. The AHA recommends that EMS personnel conduct an on-site “preincident” to identify problems or poorly accessible areas.19 An Inter-Association Task Force developed consensus recommendations for emergency preparedness and management of sudden cardiac arrest in high school and college athletic programmes.25 The key consensus recommendations for emergency preparedness include the following:
-
The EAP should be developed and coordinated in consultation with local EMS personnel, school public safety officials, on-site first responders and school administrators.
-
The EAP should be specific to each individual athletic venue and encompass emergency communication, personnel, equipment and transportation to appropriate emergency facilities.
-
The EAP should be reviewed and practised at least annually with certified athletic trainers, team and attending physicians, athletic training students, school and institutional safety personnel, administrators and coaches.
-
Targeted first responders should receive certified training in CPR and AED use.
-
Access to early defibrillation is essential and a target goal of <3–5 min from the time of collapse to first shock is strongly recommended.25
What is already known on this topic
-
Sudden cardiac arrest (SCA) is a rare but catastrophic event and the leading cause of death in young athletes.
-
Public access to defibrillation and the prompt use of automated external defibrillators (AEDs) by trained and untrained laypersons have improved survival from out-of-hospital SCA.
-
The success of public access defibrillation trials combined with the desire to prevent sudden cardiac death in young athletes have accelerated broad implementation of AEDs in schools and at public sporting venues.
What this study adds
-
Over half of Washington State high schools have placed an AED on school campuses.
-
Financial resources are the main obstacle for high schools to implement an AED programme, with funding for AEDs coming primarily from private donations.
-
High schools with AEDs have considerable deficiencies in emergency planning and coordination with local emergency response teams.
-
Significant improvement is needed in structuring emergency response plans and training targeted rescuers for sudden cardiac arrest in the high-school setting.
Limitations
The primary limitation of this study is the low response rate (29%), raising the potential for selection bias and falsely increasing the AED prevalence. However, a survey of initial non-responders found no significant difference in AED prevalence in the initially responding group. The study was also limited by the survey tool itself, which requests self-reported data and has potential for recall bias.
CONCLUSIONS
Over half of Washington State high schools have placed an AED on school grounds. AED use occurred in <1% of schools annually and was effective in the treatment of SCA. Funding of AED programmes was mostly through private donations with little coordination with local emergency response teams. Significant improvement is needed in structuring emergency response plans and training targeted rescuers for an SCA in the high-school setting.
Acknowledgments
We thank the National Collegiate Athletic Association (NCAA) for their support of this project and the development of the National Registry for AED Use in Sports. Conclusions drawn from the data collected are those of the investigators and do not necessarily represent the views of the officers, staff or membership of the NCAA. We also thank Carol Fahrenbruch, MSPH, for her statistical support and analysis.
REFERENCES
COMMENTARY
As detailed in this paper, the use of automated external defibrillators (AEDs) and implementation of a comprehensive emergency action plan are a critical part of providing medical care to intercollegiate athletic programmes,1 as well as to high schools. Despite the lower incidence of sudden cardiac deaths in this group, there is a significant number of other people entering these arenas (spectators, coaches and referees) who are in an age range where such deaths might be prevented by timely use of an AED by a trained or even an untrained responder.2 Hence, it is reasonable to examine the utilisation of AEDs and emergency action plans in high schools, as well as to identify current sources of funding and potential barriers. The main weakness of this study is the low response rate from the Washington high schools surveyed (compared with similar surveys in collegiate institutions). However, this may also speak to the need to educate this population with regard to the necessity and cost-effectiveness of these initiatives.
Footnotes
-
Published Online First 9 February 2007
-
Competing interests: None declared.