Article Text

Abstract
Internal impingement is a commonly described cause of shoulder pain in the overhead athlete, particularly in tennis players. Three shoulder dysfunctions, often correlated with internal impingement symptoms, require attention in the rehabilitation strategy of internal impingement in the tennis player: (1) acquired glenohumeral anterior instability, (2) loss of internal rotation range of motion, and (3) lack of retraction strength.
Based on recent literature, the following guidelines are proposed in the rehabilitation of the tennis player with internal impingement symptoms: (1) shoulder rehabilitation should be integrated into kinetic chain training, not only in the advanced phases of the athlete’s rehabilitation, but from the initial phases; (2) both angular and translational mobilisations can be used in the treatment of acquired loss of glenohumeral internal rotation range of motion to stretch the posterior structures of the glenohumeral joint; and 3) in the rehabilitation of scapular dyskinesis, the therapist should focus on restoration of intramuscular trapezius muscle balance in the scapular exercises, with special attention to strength training of the retractors.
Statistics from Altmetric.com
Chronic shoulder pain is probably the most common arm problem in recreational and competitive overhead athletes.1–4 Throwing athletes, athletes involved in racquet sports such as tennis, volleyball players and swimmers need full, unrestricted arm function to optimally perform in their sport.5
Non-traumatic shoulder pain in the overhead athlete is a diagnostic challenge. The causes of chronic shoulder pain are numerous, but often difficult to identify and diagnose.6–10 Research indicates that shoulder impingement is the most common cause of shoulder pain in overhead athletes.11 12 In recent literature, impingement has been described as a group of symptoms rather than a specific diagnosis. In this current opinion, it is thought that numerous underlying pathologies may cause impingement symptoms. Glenohumeral instability,5 13–15 rotator cuff or biceps pathology,13 16 scapular dyskinesis,14 17 18 and glenohumeral internal rotation deficit19–21 have been associated with impingement symptoms in clinical literature. Various anatomical structures can be impinged internally or externally, probably depending on the motion and loading put on the shoulder during the pain-provoking activity.7 22 However, a possible instability in the shoulder is often “silent” and difficult to show by ordinary tests, and has therefore by some been termed “functional instability”. It is now thought that functional instability in the shoulder may lead to a vicious circle involving microtrauma and secondary impingement, and may eventually lead to chronic shoulder pain.22
Since the first paper, published by Walch23 et al, describing a new site of impingement between the humeral head and the posterosuperior rim of the glenoid, internal impingement has been suggested to be a common cause of chronic shoulder disorder in overhead athletes.24–26 This type of impingement occurs in the cocking position of throwing, with the glenohumeral joint in maximal external rotation, maximum horizontal abduction, and, depending on the sport, in abduction or forward flexion. Walch23 et al showed, by performing shoulder arthroscopy with the shoulder placed in 90° of abduction and 90° of external rotation (90/90 position), that the supraspinatus and infraspinatus tendons tend to rotate posteriorly. This more posterior orientation of the tendons aligns them so that they become compressed between the humeral head and the posterosuperior rim of the glenoid. In general, overhead athletes with internal impingement have posterior shoulder pain and tenderness of the infraspinatus tendon on palpation, and are typically athletes intensively active in overhead sports such as tennis.27 Internal impingement particularly occurs when the humeral shaft goes beyond the plane of the body of the scapula during the cocking position of throwing. Under normal circumstances, the scapula goes into retraction simultaneously with the horizontal abduction movement of the humerus. When the body of the scapula and the humeral shaft fail to remain in the same plane of movement during the cocking phase of throwing, encroachment of the rotator-cuff tendons between the humeral head and the glenoid rim may cause internal impingement symptoms. This phenomenon is called “hyperangulation”.19 However, in spite of the documented structural pathology and cuff lesions, shown by several groups to be related to internal impingement symptoms,13 19 23 it is suggested that functional disturbances, such as subtle glenohumeral instability, glenohumeral range of motion (ROM) restrictions, scapular dysfunction and muscle stiffness, are often associated with internal impingement symptoms, rather than structural deficits and pathologies.17 28–30 These dysfunctions are often the base for conservative treatment, in particular rehabilitation exercises, and need to be considered in the prevention and rehabilitation of shoulder pain in the tennis player.
Numerous studies examining the possible causes and biomechanical backgrounds of internal impingement have been perfromed. In general, two pathological mechanisms in the possible aetiology of internal impingement have been described: (1) excessive humeral translations, compromising glenohumeral congruence,31 and (2) scapular dyskinesis, decreasing the quality of functional scapular stability, and hence jeopardising overhead shoulder function.30
The most commonly described cause of excessive humeral translations is anterior shoulder instability.10 Overhead athletes very often exhibit acquired glenohumeral instability, characterised by laxity of the anterior capsule, as a result of the extreme use of their shoulder during overhead throwing or smashing activities. This type of acquired instability is often referred to as acquired instability overuse syndrome (AIOS).10 Several authors have suggested that this type of instability is present in recreational and professional tennis players.10 12 32
A second mechanism related to increased humeral translations is tightness of the posterior structures.10 19 30 33 A consistent finding present during examination of overhead athletes is reduced internal rotation ROM of the dominant arm.5 19 21 30 Several possible mechanisms have been described to explain the glenohumeral internal rotation deficit (GIRD).19 34 The tightness of the posterior capsule and the muscle tendon unit of the posterior rotator cuff is believed to limit internal joint rotation. Burkhart19 et al. defined GIRD as a loss of internal rotation of ⩾20° compared with the contralateral side. When the posterior structures of the glenohumeral joint are shortened, this may compromise the hammock function of the inferior glenohumeral ligament (IGHL), and increase the risk for impingement symptoms during throwing. Under normal circumstances, the IGHL functions as a hammock in the stability of the glenohumeral joint. However, where there is tightness of the posterior band of the IGHL, the humeral head will translate anteriorly, as a result of imbalances between the anterior and posterior band of the IGHL. There is some disagreement about the humeral head movement during the cocking position of throwing or overhead serving in tennis. According to some authors, the posterior band of the IGHL moves inferiorly and slightly anteriorly of the humeral head, thus inducing a posterosuperior translation of the humeral head. This mechanism possibly explains the findings of internal impingement symptoms in the cocking position.19 During the follow-through phase of throwing, the posterior band of the IGHL is at the posteroinferior side of the humeral head. Tightness in this part of the capsule will induce anterosuperior translations of the humeral head, thus increasing the risk for subacromial impingement. However, other studies35 suggest an anterior and inferior translation of the humeral head during cocking with a tight posterior capsule. As a result, posterior capsule shortness possibly increases internal and subacromial impingement in the overhead athlete.19 33 35 Loss of internal rotation ROM in tennis players has been shown by several authors.36–38
The treatment goals during the intermediate phase are improvement of functional dynamic stability under circumstances of increasing complexity and specificity, introduction of eccentric exercises and open kinetic chain exercises in preparation for a throwing programme, and strength enhancement of all glenohumeral muscles.27 Informed consent was obtained for publication of this figure.
Besides the glenohumeral component as a possible cause of internal impingement, scapular dyskinesis may play an important role in functional shoulder pain in the overhead athlete.17 29 The role of the scapula in normal athletic shoulder function and in shoulder pain in the overhead athlete has been extensively described in the literature.18 39 Both clinical experience and scientific data show that athletes with shoulder pathology consistently have abnormalities in scapular rotator activity.3 5 28 40 41 42 43 Numerous studies have been published examining muscle activity in the scapular muscles during a variety of movements in athletes involved in overhead activities. Most authors suggest, based on their data, that there are alterations in muscle activity in the upper trapezius (UT), lower trapezius (LT) and serratus anterior (SA) muscles in patients with symptoms of impingement.28 40 41 42 43 44
During overhead throwing, it is imperative that the scapula can move towards retraction as well as protraction. In the cocking phase, sufficient retraction is necessary to avoid hyperangulation and impingement symptoms.18 Several studies have shown that overhead athletes have a scapular muscle balance between protractors and retractors slightly <1, meaning that protractors are stronger than retractors.10 40 41 Normal non-athletic subjects have equal strength in their protractors and retractors.45 This shift in scapular muscle balance may be the result of sport-specific adaptations; however, a lack of retraction strength may increase the risk for hyperangulation and hence internal impingement.
Therefore, three diagnoses, correlated with internal impingement symptoms, need consideration in the rehabilitation strategy of internal impingement in the tennis player: (1) acquired glenohumeral anterior instability, (2) loss of internal rotation ROM, and (3) lack of retraction strength. These diagnoses are functional disorders rather than structural pathologies, and are probably interrelated to each other. Although cause–effect relationship between these symptoms is not clear, they deserve attention in the prevention and rehabilitation of shoulder pain in the tennis player.
REHABILITATION OF ACQUIRED INSTABILITY
The following description of rehabilitation guidelines for shoulder instability in the overhead athlete is based on clinical literature 10 14 15 18 27 39 46 47 rather than scientific rationale. It should therefore be taken into account that although numerous authors have described a rehabilitation protocol for shoulder pathology in the overhead athlete, scientific evidence to support the effect of these rehabilitation protocols is scarce. Future investigations should focus on examining the efficacy of these exercise protocols.
The rehabilitation process for overhead athletes with acquired instability must restore muscular balance and muscular endurance, and gradually restore proprioception, dynamic stability and neuromuscular control.10 11 24 27. In the initial phase, the major treatment goals are restoration of rotator cuff muscle balance, baseline proprioception and local muscle control.
In view of the observation that very often the external rotation to internal rotation ratio is reduced in overhead athletes,48 special attention should be paid to restoration of muscle control and muscle strength of the external rotators. Closed kinetic exercises are also performed in this phase (fig 1). Axial compression exercises stress the joint in a weight-bearing position, resulting in joint approximation and improving co-contraction of the rotator cuff muscles.46

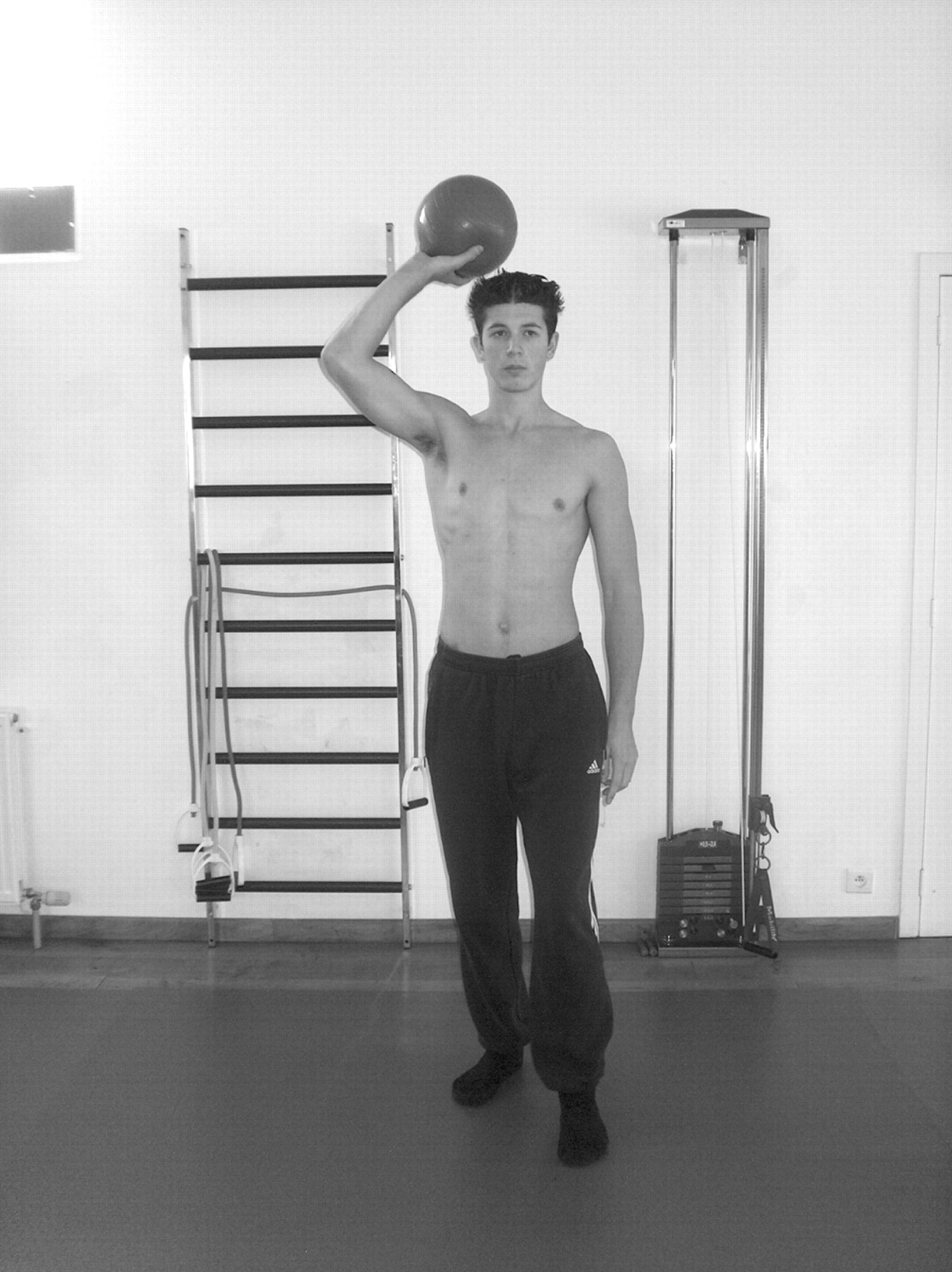
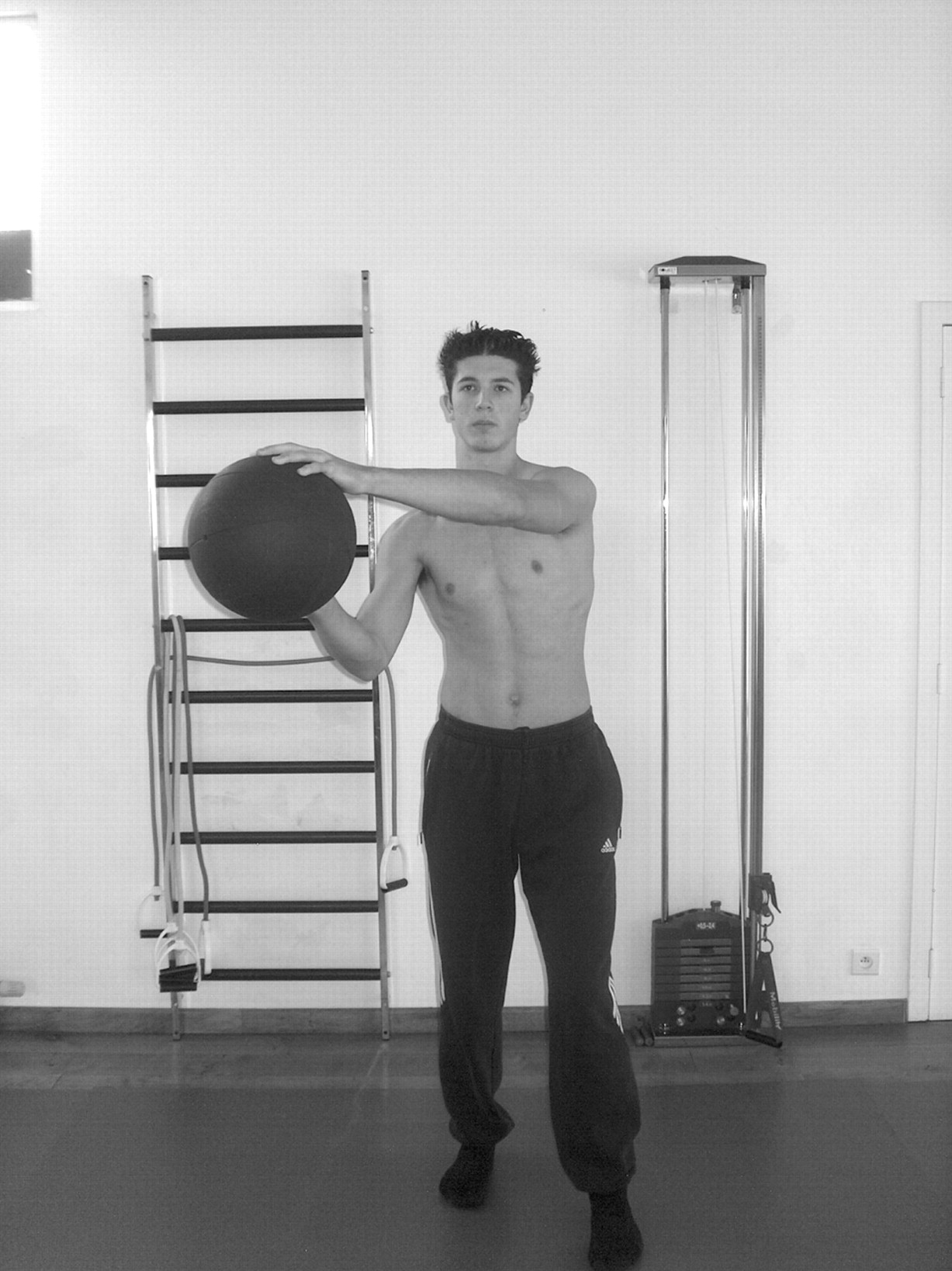
The third phase of a functional rehabilitation programme, the advanced phase, is designed to prepare the athlete to return to full athletic activity. Strengthening exercises are continued, and plyometric drills are introduced.49 Plyometric exercises consist of quick powerful movements, activating the stretch–shortening cycle of the muscle. Initially the athlete performs the plyometrics using both hands and with the shoulder in a moderate external position (fig 2). Two-hand drills progress to one-hand drills, with increasing velocity and resistance (fig 3).

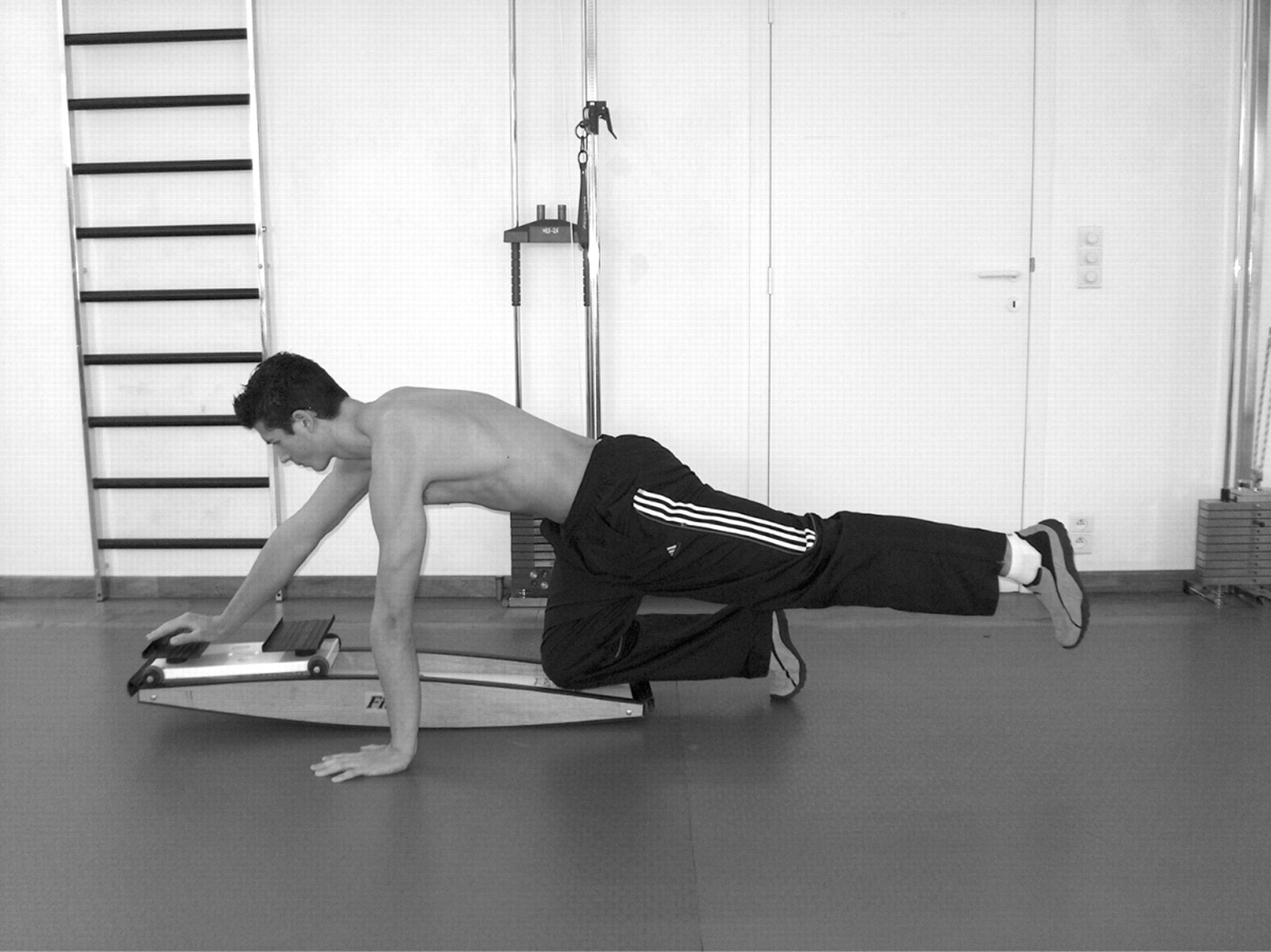
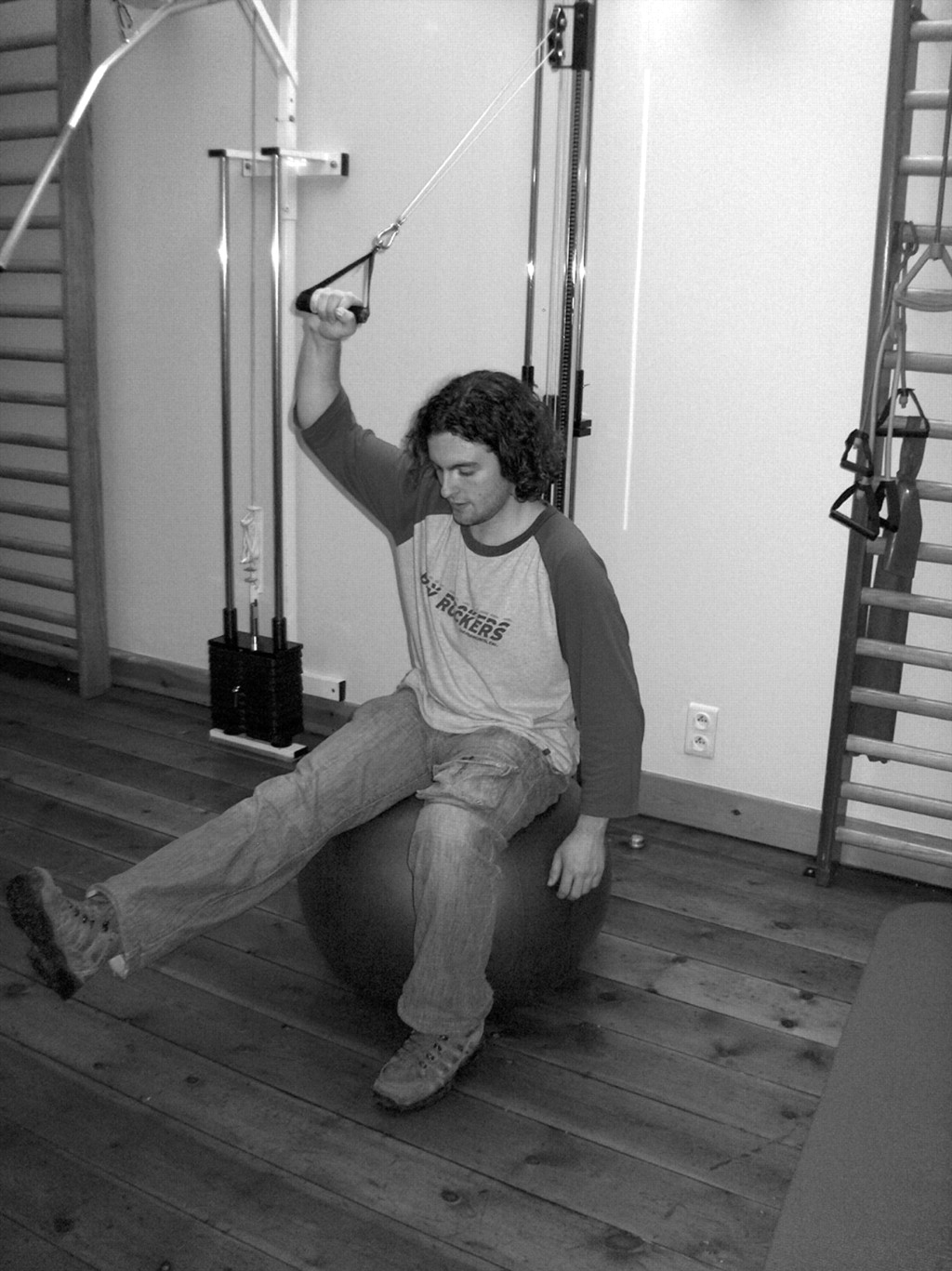
In recent literature, the role of the kinetic chain has been emphasised in the rehabilitation of the tennis player with shoulder pain.17 18 47 The rationale behind the kinetic chain principle is that other body parts, such as the legs or trunk, should be integrated in the shoulder rehabilitation programme, in order to prepare the athlete’s whole body, not only the shoulder, for the return to athletic activity.18 27 Core stability, leg balance, and diagonal movement patterns are examples of facilitation of the kinetic chain into the rehabilitation of the shoulder (figs 4–8). In recent rehabilitation programmes, kinetic chain exercises are prescribed not only in the sport-specific phase of the rehabilitation process, but from the initial phase.27 The specific use of kinetic chain exercises also depends upon the sport the athlete performs: diagonals in prone position may be important for swimming athletes, whereas core stability with minimal leg support may be relevant for the volleyball player. In general, unilateral stance exercises on the non-dominant leg, core stability, and diagonal patterns from the non-dominant leg to the dominant arm can be used in tennis players.15 17 18 39 46 47




REHABILITATION OF GIRD
In general, two types of stretching exercises are described in literature to reduce GIRD27 50 51 Angular stretches as well as translational mobilisations are used to increase glenohumeral internal rotation ROM.
In the angular stretching techniques, internal rotation or horizontal adduction movements are passively performed by the therapist or by the patient.39 51 52 A popular stretch is the “sleeper’s stretch” (figs 9, 10).17 19 The patient’s lies on the injured side with the shoulder in 90° forward flexion. While the scapula is manually fixed into retraction, glenohumeral internal rotation is performed passively, thus stretching the posterior structures of the shoulder. Attention should be paid to the patient’s reaction: a stretching feeling at the back of the shoulder is allowed; however, if the patient feels pain anteriorly, the intensity of the stretching should be reduced by limiting the amount of forward flexion or turning the trunk slightly backwards, thus decreasing the strain on the posterior structures.


In the “cross-body stretch”, the arm is moved into horizontal adduction (figs 11, 12). Recently, Mc Clure52 et al showed significantly better results for this stretching technique in increasing the internal rotation ROM compared with the sleeper’s stretch in subjects with restricted internal rotation ROM. However, further research is needed on larger patient populations to confirm these results and to correlate the findings to other clinical features such as pain and symptoms in these patients.


In addition to the angular stretching techniques, translational mobilisation techniques that increase internal rotation ROM have been reported .27 53 In order to influence the posterior ligaments, high-grade end-range dorsal-glide mobilisations can be performed. The patient’s shoulder is placed in the end range of internal rotation (fig 13) or horizontal adduction (fig 14), and the therapist performs manual translational glides in the dorsal direction. Research indicates that particularly high-grade end-range mobilisations result in a permanent increase in ROM, greater than that achieved with low-grade mid-range mobilisation techniques.53 54 However, it should be noted that these investigations were performed on patients with adhesive capsulitis or in cadavers. Moreover, as mentioned earlier, internal impingement may be associated with subtle glenohumeral instability, and GIRD in the tennis player may be present in a potentially unstable shoulder. Therefore, the recommendation of high-grade mobilisations should be interpreted with caution, and its use limited in cases of GIRD without glenohumeral instability.


Little scientific evidence about the effectiveness of these techniques and the possible decrease in internal impingement symptoms is available. Moreover, the literature discusses the causes of GIRD as being stiffness of the posterior capsule or the IGHL, or muscle or bony abnormalities such as retroversion of the humeral head.55 Future research should focus on the possible causes of the loss of internal rotation ROM in overhead athletes, as well as on the efficiency of physical therapy techniques.
REHABILITATION OF SCAPULAR DYSKINESIS
In view of the new insights and research findings on the role of the scapula in shoulder pathology, current exercise protocols emphasise the importance of scapular muscle training as an essential component of shoulder rehabilitation.6 14 15 17 24 27 39 in particular, restoration of muscle control and balanced coactivation is a challenge to the clinician. For patients with an imbalance in the scapular muscles, selective activation of the weaker muscle parts with minimal activity in the hyperactive muscles is an important component in the reduction of the imbalance. Because a lack of activity in the LT, UT and SA muscles is often combined with excessive use of the UT, the balance ratios UT:LT, UT:MT, and UT:SA are of particular importance.28 40–43 In addition, integration of shoulder girdle exercises into a global functional kinetic-chain pattern has become a treatment goal in shoulder rehabilitation, especially in overhead athletes.17 18 47
The selection of appropriate exercises in the rehabilitation of scapular muscle performance depends not only on the actual strength of the muscles, but also on the relative strength of one muscle in relation to another. In a study by Ludewig56 et al, a selection of exercises was introduced with a low UT:SA ratio, meaning high activity in the SA with simultaneous minimal activation of the UT. However, only UT:SA ratios were examined, and only variations of the push-up exercise were performed.
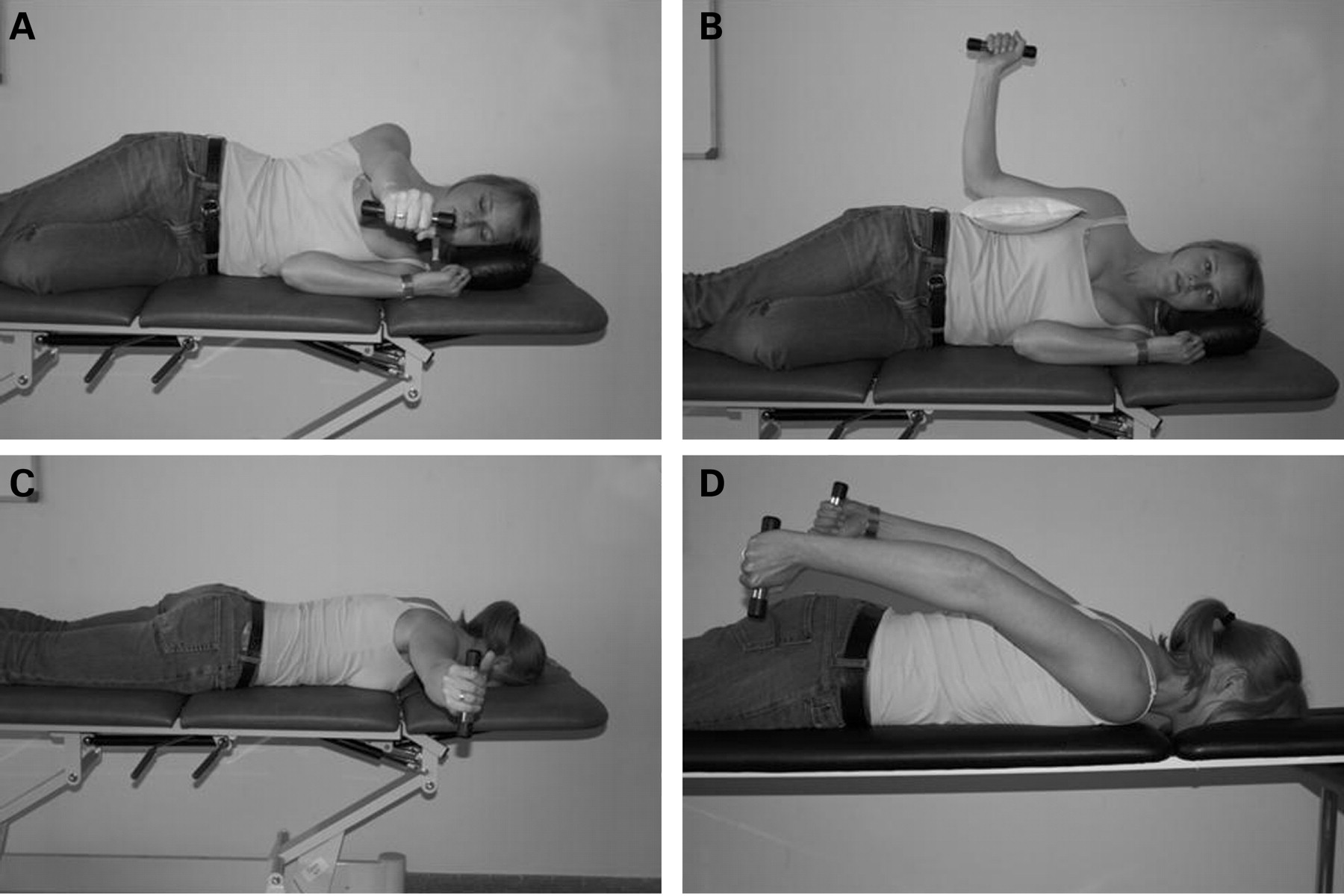
In a recent investigation,57 we identified scapular muscle strengthening exercises in which the LT and middle trapezius (MT) were optimally activated with minimal participation of the UT. Activity of the UT, MT and LT was analysed using surface electromyography during 12 commonly used scapular exercises, and UT:LT and UT:MT muscle balance ratios were calculated. Four exercises were selected as exercises with a low UT:LT or MT:LT ratio (fig 15): (A) side-lying forward flexion, (B) side-lying external rotation, (C) prone horizontal abduction with external rotation and (D) prone extension in neutral position. As several studies have shown that overhead athletes with impingement symptoms show decreased activity in both LT and MT, with excessive activation of the UT,28 40 41 42 these exercises may be used for restoration of both muscle imbalances.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
From a clinical viewpoint, the major limitation of these exercises can be found in the outcome itself. Indeed, all the exercises selected based on a low UT:LT or UT:MT ratio are performed in a lying position, prone or side-lying. However, recent literature emphasises the importance of functional exercises, resembling daily or sport specific arm function, and integration of the shoulder rehabilitation into a functional kinetic chain.17 18 47 These treatment goals are very difficult to accomplish with the patient lying down. Diagonal patterns, combined with trunk and lower limb stabilisation, as promoted by a number of authors, are not possible in these exercise techniques. Therefore, we propose that our exercises should be performed in the early stages of rehabilitation, and before more functional kinetic chain exercises, in which functional recruitment patterns can be trained with normalised intermuscular and intramuscular balance ratios.
CONCLUSION
Internal impingement is possibly the result of acquired anterior instability, acquired loss of internal rotation ROM due to posterior shoulder stiffness, and scapular dyskinesis. Before a rehabilitation programme, a thorough physical examination should be performed to define the specific dysfunctions and determine the treatment goals. Physical therapy of acquired instability should focus on integration of the functional kinetic chain in the rehabilitation exercises. Angular stretches and dorsal glide mobilisations may be performed to improve internal rotation ROM; however, the therapist should be cautious in cases with instability. In cases with scapular dyskinesis, restoration of intermuscular and intramuscular muscle balance is the main treatment goal.
REFERENCES
Footnotes
Competing interests: None.
Patient consent: Informed consent was obtained for publication of figures 1–12.