Article Text

Abstract
Objective: To compare the effect of a whole body vibration training (WBVT) programme with a conventional training (CT) programme on knee proprioception and postural stability after anterior cruciate ligament (ACL) reconstruction.
Methods: Twenty athletes with unilateral ACL reconstruction were randomly assigned to the WBVT or CT group; all participants received 12 sessions of WBVT or conventional training. Absolute error in joint repositioning for two target angles (30° and 60°) was measured with the Biodex dynamometer; bilateral dynamic postural stability (anteroposterior, mediolateral and overall stability indices) was measured with the Biodex Stability System pre-intervention and post-intervention.
Results: The improvement in postural stability in the WBVT group was significantly greater than that in the CT group (p⩽0.05). The p values of the changing scores of open overall, open anteroposterior, open mediolateral, closed overall, closed anteroposterior and closed mediolateral stability indices were 0.002, 0.010, 0.0001, 0.001, 0.0001 and 0.046, respectively. In addition, there were significant differences in all averages of absolute angular error at 60° and 30° between the WBVT and CT groups in both knees (p = 0.001 in healthy knees and p = 0.001 and p = 0.0001 in reconstructed knees), apart from the healthy knees at the 30° target position, which was not significant (p = 0.131).
Conclusions: Whole body vibration training improved proprioception and balance in athletes with reconstructed ACL.
Statistics from Altmetric.com
Proprioception is conscious perception of limb position in space. Many proprioceptors such as Ruffini and Paccini endings have been found in the anterior cruciate ligament (ACL).1 2 ACL has a major function as a significant sensory organ that provides proprioceptive information initiating protective and stabilising muscular reflex as well as mechanical function.2–4 ACL injuries cause instability and disability in a high percentage of ACL-deficient athletes and reduce proprioceptive ability and postural stability. Owing to proprioception loss in ACL injuries, postural sway may increase. It also seems that any degenerative joint diseases following ACL injuries are not purely due to joint instability but also to disruption of proprioception feedback.5 ACL injuries are a common occurrence in young athletes. Without normal joint stability and proprioception, athletes often find it difficult to return to normal activity after ACL injuries and reconstructive surgeries; therefore, rehabilitation programmes are frequently indicated to return the ACL-deficient athlete to the highest level of activity. This means a full range of motion, normal muscle strength, normal agility and coordination, maximum proprioception and stability in the knee.6
Whole body vibration training (WBVT) is a neuromuscular training method that has been recently developed and introduced as a rehabilitative protocol.7 8 The transmission of mechanical oscillations (30–50 Hz) to the body stimulates many biological systems. This in turn may lead to physiological changes at numerous levels including stimulation of skin receptors, muscle spindles, joint mechanoreceptors, vestibular system, changes in cerebral activity and changes in neurotransmitter and hormone concentrations.9 It has also been suggested that WBVT can affect muscle strength and power, soft tissue flexibility, body balance, neuromuscular conditions, gait parameters and mechanical properties of bones.7 10–14
Because WBVT has a strong sensory stimulatory effect on muscle receptors, it might also be a stimulus for other proprioceptors.15 Some studies have analysed the effect of WBVT on muscle performance and balance in normal subjects. Torvinen et al12 reported that after 4 min of WBVT in young adults there was a 15.7% improvement in body balance; however, in another study no effect was found after 4 months of training.16
Verschueren et al17 reported a reduction in postural sway in postmenopausal women after a brief voluntary abduction of the arm following 6 months of WBVT. Schuhfried et al9 found a positive effect of WBVT in postural control of moderately disabled multiple sclerosis patients. Bogarets et al15 reported that WBVT was associated with a reduction in fall frequency from a moving platform and an improvement in some aspects of postural control in older individuals. Van Nes et al18 in a study on a unilateral chronic stroke patient concluded that WBVT may be a candidate to improve proprioceptive control of posture in stroke patients. Fontana et al19 studying the effect of WBVT on lumbosacral proprioception showed how a single 5 min period of WBVT combined with a static closed chain exercise improved lumbosacral proprioception. Melnyk et al20 indicated a single WBVT had a beneficial effect on functional knee stability in normal subjects.
However, there is little scientific evidence with regard to the effects of WBVT on proprioception and postural stability in ACL-reconstructed athletes. Accordingly, the aim of this study was to compare the effects of a WBVT programme with conventional therapy on knee proprioception and postural stability in ACL-reconstructed subjects.
METHODS
The study was a single, blind, randomized clinical trial that was approved by the Ethical Committee of Medical Sciences of Tehran University and each subject provided informed written consent. Subjects were introduced to the Sport Physical Therapy Clinic between May and October 2006.
Participants
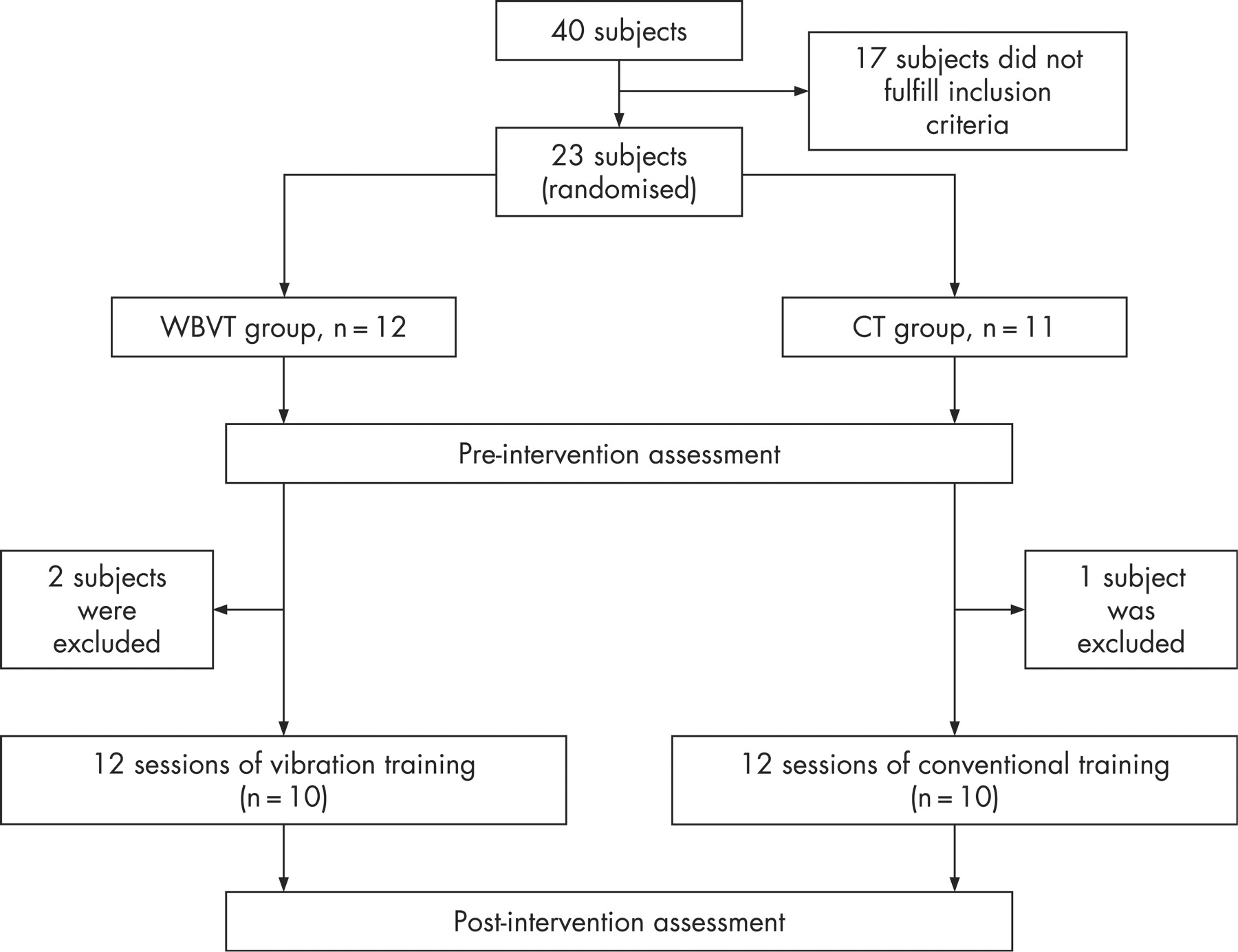
Forty subjects participated in the study; the majority were referred by their orthopaedic surgeon. Seventeen subjects did not fulfil the inclusion criteria and three subjects were excluded at the next stage (fig 1). Twenty of the participants were male athletes who had undergone arthroscopy for ACL reconstruction with a central bone−patellar tendon approach. All participants fulfilled the following inclusion criteria: ACL reconstructive surgery 3 months before, competitive athletes of national or international level, no previous or concomitant injury or surgery on the relevant knee and other joints, no history of surgery or traumatic injuries to the contralateral limb, full range of motion in the reconstructed knee, no history of medical problems such as heart disease that limited activities and no history of WBVT contraindications for participants of the WBVT group. In addition, all subjects were released from a formal rehabilitation programme, which was the same for both groups before participation. Participants were randomly allocated to the WBVT and conventional training (CT) groups (12 and 11, respectively). Before participation, all subjects gave their informed written consent.

{kind=link}
Testing procedures
Participants were familiarized with testing procedures 2 days before the testing session. In all sessions, each subject was dressed in shorts, without shoes and socks. Our evaluating systems were calibrated before the sessions in accordance with the manufacturer’s instructions. The testing session started with a 10 min jogging warm-up programme on a treadmill (Technogym, Italy) and lower body stretching exercises.
Postural stability test
Postural stability was evaluated by the Biodex Stability System (BSS; Biodex Medical Systems, Shirley, NY, USA). The BSS's specialized software (Version 3.1) measures the deviation of the centre of pressure (COP) during static conditions, and measures the degree of tilt during dynamic conditions. The COP can be used to evaluate the amount of sway from the centre of gravity over the foot during stance. Postural stability was measured by overall, anterior–posterior and medial–lateral stability indices (OSI, APSI and MLSI, respectively). A high score indicated poor balance.22 23
The BSS was shown to be reliable in previous studies. Schmitz and Arnold23 reported intraclass correlation coefficient (ICC) values for dominant single limb stance ranging from 0.8 to 0.43, using a decreasing stability level from 8 to 2 over 30 s. Pincivero et al24 reported ICC values of 0.6 (level 8) to 0.95 (level 2) in healthy subjects. We also confirmed the reliability of BSS during our pilot study (table 3).
Subjects were requested to step on the platform and assume a comfortable position while maintaining slight flexion in the knees (15°). When subjects felt comfortable, the platform was released. At this stage, the subjects were asked to change their position so that they felt balanced standing on the platform, then the platform was locked and the position of their feet recorded. The testing procedure consisted of progressively decreasing the stability of the platform from level 8 to 4 in 25 s.
Bilateral stance position was evaluated with opened and closed eyes. Three trails of tests in either condition were performed and participants had a 3 min rest between each condition. In the open-eye condition, subjects were requested to look ahead at a spot marked directly in front of them.
Knee joint reposition test
Evaluation of proprioception was performed with the joint reposition test. The position sense of the knee was tested by examining the ability of subjects to reproduce actively an angle at which the joint had been placed before in a non-weight-bearing position. Knee position sense was performed on the Biodex Dynamometer (Biodex Medical Systems, Shirley, NY, USA with software Version 3.27) using this system’s electrogoniometer (sensitive to 1° increments ) to record the angles of knee movement during testing. The Biodex isokinetic dynamometer has been found to be a valid and reliable device for torque and position measurements.25 26 The reliability of the Biodex dynamometer in the knee reposition test was measured during our pilot study (table 3).
The subjects were seated up straight in the Biodex chair with the seat adjusted approximately 5 cm from the popliteal fossa. To eliminate visual input during testing, subjects were blindfolded and an air splint was positioned around the leg to reduce cutaneous sensory input. The knee of the tested leg was aligned with the axis of the dynamometer and the thigh was secured to the seat with a strap. The tibial pad was secured to the shank 3 cm superior to the lateral malleolus. Then the subjects were asked to extend actively the knee from starting position (90° knee flexion) to target angle (60° knee flexion).When the target angle was reached, the Biodex held the position for 5 s, then returned to the starting position. After a short interval, the subject was requested to reproduce actively the target angle, and then press the hold button. The same procedure was used to evaluate the active reposition test at 30° of knee flexion. Both knees were tested and each test trail was conducted five times for each target angle. The absolute angular error, the absolute difference between the target angle and the subject’s estimated test angle, of the five trails was measured in both knees and the average of absolute angular error was recorded in reconstructed (ReAE) and uninjured (UnAE) knees.
Interventions
All subjects in both groups followed a physiotherapy programme immediately after surgery for 12 weeks. At the beginning of the 12 weeks, subjects were randomly assigned to two groups (WBVT and CT groups) and began a three times a week training programme for 1 month. The WBVT group exercised on a vibration platform (Powerplate, USA) while barefoot. Table 1 shows the details of WBVT programme. The CT group continued the conventional strengthening exercises programme (table 2), flexibility training for both lower limbs and proprioceptive training on a tilt board progressing from two-legged to one-legged positions and also from open to closed eyes. The subjects had a 10 min warm-up prior to their exercises.
Statistical analysis
The Statistical Package for the Social Sciences (SPSS, Version 11.5, SPSS Inc., Chicago, IL, USA) was used to conduct the analysis. Normal distribution of data was determined by the one-sample Kolmogorov−Smirnov test and parametric tests were used to analyse the data. A paired-sample t test was applied to determine the differences between each group. An independent sample t test was used to compare the baseline measurements between the groups at the beginning and at the end of training. Between group differences were analysed using an independent t test on change scores of both groups after the test .The change scores of a group was defined as the increase or decrease of each variable from pre-test to post-test. The level of significance was set at p⩽0.05. To assess the intratester reliability of the above-mentioned tests, 11 subjects with the same type of ACL reconstructive surgery had repeated measurements taken 1 week apart.
Test−retest reliability of all measurements was assessed using interclass correlation coefficients (ICC) with a 95% level of confidence. Absolute reliability (standard error of measurement) was also measured (table 3).
RESULTS
There were no significant differences between WBVT and CT groups for the demographic variables listed in table 4, indicating that the groups were well matched.
In both groups, subjects became acquainted very rapidly with the training protocols. There were no reports of adverse reactions and discomfort in either group. All subjects in the WBVT group found the vibration training to be an effective, enjoyable and fatiguing modality for exercise therapy. During the second and third weeks of training, three subjects withdrew (two in the WBVT group and one in the CT group) due to a death in the family, travel and an accident. All remaining subjects completed 1 month of training and the evaluation sessions.
Pre-test results
An independent-sample t test revealed no significant differences between the two groups at the beginning of the study.
Post-test results
WBVT group
In the WBVT group, there were significant differences in overall stability, anteroposterior and mediolateral indexes in open and closed eye conditions between pre-test and post-test (p⩽0.05). The mean absolute error for a target of 60° was 6.00° then changed to 2.53° after vibration training, which was significantly more than the values for the CT group. The same results were obtained for 30° in the WBVT group. In the WBVT group, there were significant differences in the averages of absolute angular error between pre-test and post-test in reconstructed knees at both 30° and 60° (p⩽0.05), but in the healthy knees, at 30° there was no significant difference in the average of absolute error (table 5).
CT group
In the CT group, there were significant differences between open and closed eyes in overall stability indexes and also a significant difference in closed eyes mediolateral index between pre-test and post-test (p⩽0.05). There were no significant differences in the averages of absolute angular error between pre-test and post-test in both knees and at both target positions (table 6).
Comparison between training groups
The improvement of postural stability in the WBVT group was significantly greater than that in the CT group. In the WBVT group, the changing scores of all stability indices between pre-test and post-test were much greater than those in the CT group (table 7). Moreover, there were significant differences in all averages of absolute angular error between the WBVT group and CT group in both knees, except in the healthy knees at the 30° target position, which was not significant.
DISCUSSION
Whole body vibration is a new kind of somatosensory stimulus for proprioception with a long-lasting postural effect on healthy subjects.27 There are several reports about the effect of WBVT on postural balance; some results have supported a positive effect9 12 15 18 while others have not.16 21 However, there is a lack of scientific evidence to support a positive effect of WBVT on proprioception, especially on knee proprioceptors after ACL reconstruction. In this study, a WBVT protocol was used for postoperative rehabilitation of athletes who had undergone ACL reconstruction in comparison with conventional training. The principal finding in this investigation was the positive effect of WBVT in improvement of knee proprioception and postural balance. The results showed that WBVT increased postural stability and proprioceptive function in ACL-reconstructed athletes.
Based on the results of the current study, it might be suggested that several types of receptors are sensitive to these mechanical stimuli. The most important effects of vibration are stimulation of extroceptive receptors on the sole of the foot (Merkel, Meissner, Ruffini receptors). Furthermore, stimulation of proprioceptive receptors could initiate stretch and cutaneous reflexes and hence increase muscle strength.
The nature of this repetitive stimulation might be a rearrangement of balance control strategies, which results in improvement of postural stability.9 In this investigation, the indices of postural stability in the WBVT group was significantly improved. This finding is in agreement with the results of authors who studied the positive effects of vibration in patients’ balance.9 15 18 This might be due to positive effects of WBVT on muscle strength, improved synchronization of firing of the motor units and improved co-contraction of synergist muscles, which could bring about better balance control strategies in patients.18 28 In our study it was noted that WBVT was a very pleasant experience for all subjects, and the acceptance of the programme by all participants of the WBVT group was encouraging. In addition to OSI, APSI and MLSI were also measured to evaluate the postural control. We found a significant difference in all postural stability indices between the WBVT group and CT group, and more improvement in the stability of WBVT subjects. In the WBVT group, all stability indices demonstrated a significant difference between pre-test and post-test. In the CT group, there were significant differences in OSI in both open and closed eyes and also in closed eye MLSI. It seems that WBVT had a greater somatosensory effect on balance control than conventional training.
Some improvement in lumbosacral proprioception has been reported after WBVT.19
Our results revealed a significant difference in absolute angular error results in the reconstructed knees in both WBVT and CT groups. The WBVT group showed significant differences in the results of the joint repositions test, but within the CT group there were no significant differences. In the WBVT group, there was a significant difference in healthy knees between pre-test and post-test at 60°. WBVT increased the difference between the absolute angular errors of reconstructed knees. The beneficial effect of WBVT on functional knee stability has been reported in normal subjects.20
The results of pervious studies suggested that the patients who had undergone ACL reconstructive surgery had bilateral deficits in neuromuscular control of the knee.29–31 Thus, re-establishing the mechanical function of ACL by reconstruction and restoring normal joint function with proper rehabilitation programmes, especially after surgery, for 6 months may improve knee kinematics and enhance proprioception.2 WBVT may be a new candidate for rehabilitation after ACL reconstruction. However, further research into the effects of WBVT on knee proprioception is recommended, and investigations should be directed to find out the most efficient WBVT protocols. Furthermore, more clinical studies are required to establish the long-term effects of vibration in ACL-deficient athletes.
This study had several limitations. The sample size of the current study was small and there was no follow-up period due to loss of calibration in the Biodex system. In addition, there has been no previous investigation on this topic and therefore the current exercise protocol for WBVT might not be optimal.
CONCLUSION
It seems that WBVT and CT methods are effective in the rehabilitation of patients with ACL reconstruction. The results of this study showed that WBVT was associated with a greater improvement of joint stability and balance. The positive effect of WBVT, the short period of training required and participant satisfaction in the present study support the need for future research into this new method of training for rehabilitation of ACL injuries.
What is already known on this topic
ACL injuries cause instability and disability in a high percentage of ACL-deficient athletes and reduce proprioceptive ability and postural stability.
Whole body vibration is a new kind of somatosensory stimulus for proprioception with a long-lasting postural effect on healthy subjects.
What this study adds
It appears that WBVT had a greater somatosensory effect on balance control than conventional training.
The principal finding in this study was the positive effect of WBVT in improvement of knee proprioception and postural balance.
WBVT may be a new candidate for the rehabilitation of patients after ACL reconstruction.
Acknowledgments
This project was supported by a grant from the Postgraduate Studies and Research Programme, Medical Sciences/Tehran University. The authors would like to acknowledge the generous assistance of the staff of the Sport Physical Therapy Clinic of IR Sports Medicine Federation and Faculty of Rehabilitation, Tehran University. The authors thank the participants for their excellent cooperation. We would also like to thank Dr. Hossein Karimi, PhD PT, for his review of an earlier draft of the manuscript.
REFERENCES
Footnotes
Competing interests: None.