Article Text

Abstract
Background: The protection of athletes’ health by preventing injuries is an important task for international sports federations. Standardised injury surveillance provides not only important epidemiological information, but also directions for injury prevention, and the opportunity for monitoring long-term changes in the frequency and circumstances of injury. Numerous studies have evaluated sports injuries during the season, but few have focused on injuries during major sport events such as World Championships, World Cups or the Olympic Games.
Objectives: To provide an injury surveillance system for multi-sports tournaments, using the 2008 Olympic Games in Beijing as an example.
Methods: A group of experienced researchers reviewed existing injury report systems and developed a scientific sound and concise injury surveillance system for large multi-sport events.
Results: The injury report system for multi-sport events is based on an established system for team sports tournaments and has proved feasible for individual sports during the International Association of Athletics Federations World Championships in Athletics 2007. The most important principles and advantages of the system are comprehensive definition of injury, injury report by the physician responsible for the athlete, a single-page report of all injuries, and daily report irrespective of whether or not an injury occurred. Implementation of the injury surveillance system, all definitions, the report form, and the analysis of data are described in detail to enable other researchers to implement the injury surveillance system in any sports tournament.
Conclusion: The injury surveillance system has been accepted by experienced team physicians and shown to be feasible for single-sport and multi-sport events. It can be modified depending on the specific objectives of a certain sport or research question; however, a standardised use of injury definition, report forms and methodology will ensure the comparability of results.
Statistics from Altmetric.com
The protection of athletes’ health by preventing injuries is an important task for international sports federations and for the International Olympic Committee (IOC). Standardised assessment of sports injuries provides not only important epidemiological information, but also directions for injury prevention and the opportunity for monitoring long-term changes in the frequency and circumstances of injury.1–6 Finch et al4 stated that injury surveillance during sporting events should be a part of the duty of care to the participants to help make future events safer. Therefore, the IOC has decided to conduct an injury surveillance study during the Olympic Games 2008 in Beijing.
Injury surveillance studies have been reported for various sport events, but the results of these studies cannot be compared with one another, due to the heterogeneous injury definitions, methods of data collection, observation periods, study designs and sample characteristics used.7–10 The need for agreement on the definition and standards to be used in sports injury epidemiology has been expressed,2 9 11 12 and consensus statements for certain sports, such as football,13 rugby14 and cricket15 have been published. These consensus statements provide detailed approaches for injury surveillance studies within specific sports, but they may not be appropriate where several diverse sports are being compared. Although some variations in methodology may be necessary to address the specific objectives of a particular sport, a broad consensus agreement on the methodology of sports injury surveillance would not only improve the scientific value of studies on sports injuries substantially, but also help to generalise conclusions and recommendations, and to combine the effort in injury prevention across different sports.
Injury surveillance systems for major sports events have been published by Harrison and Price,16 Finch et al4 and Junge et al,5 17 but only the latter has proved its feasibility in different types of sports tournaments.5 17–23 It should be noted that several organisations have developed and implemented injury report systems to register injuries of specific groups of athletes during the season such as the Canadian Intercollegiate Sport Injury Registry24 and the National Collegiate Athletic Association Injury Surveillance System.25 These systems include injuries during tournaments of the athletes surveyed but are not tailor-made to monitor injuries during major sports events. In major tournaments, such as World Championships, World Cups or the Olympic Games, large numbers of teams from different backgrounds and with diverse medical support participate and it is more difficult to obtain reliable information about the incidence, occurrence and characteristics of injury.
Few injury-surveillance studies have been performed during single-sports tournaments, except for football5 18–22 26 27 and rugby,28–31 and even fewer for multi-sport events.17 32–35
The aims of the present project were to present standards for injury surveillance during major single- and multi-sports tournaments, and specifically to provide the methodology that will be applied during the 2008 Olympic Games in Beijing.
METHODS
The feasibility and quality of an injury-report system is dependent on the definition of injury, the source of information, the characteristics of the injury documentation form and the availability of exposure data.7 9 10 In accordance with the guidelines of the Centers for Disease Control, it should also be simple, flexible, acceptable, sensitive, representative and immediate/timely.2
The IOC injury surveillance system for multi-sports events is based on an injury-reporting system well-established for top-level international football5 18–22 and handball23 tournaments, and which was used for all team sports tournaments during the Olympic Games in 2004.17 The acceptability of and compliance with the procedure was excellent, with a response rate >90% in almost all tournaments at the Athens Olympic Games. The consistent findings in different studies confirmed the high quality of the data obtained.17 This injury-reporting system developed for team sports tournaments was modified to be applicable for both individual and team sports. The key modifications are presented in table 1.
While modifying the injury-reporting system, the most important principles and advantages of the established system were preserved, such as the consensus definition of injury, injury report by the physician responsible for the athlete, report related to a time period independent of whether or not an injury occurred, and one report form per team (not per injury). The modified injury surveillance system was implemented and proven feasible during the World Championships of the International Association of Athletics Federations (IAAF) 2007 in Osaka.
Definition of injury
Based on a recent international consensus on the definition and data collection procedures in studies of football injuries,13 an injury was defined as “any musculoskeletal complaint newly incurred due to competition and/or training during the tournament that received medical attention regardless of the consequences with respect to absence from competition or training”. This injury definition includes five aspects that can be modified in future studies: (1) all injuries that received medical attention (not only time loss or reduced performance), (2) newly incurred (exclusion of pre-existing and not fully rehabilitated injuries), (3) injuries occurring in competition or training, (4) injuries occurring during the period of the tournament and (5) exclusion of illnesses and diseases.
All injuries that received medical attention
The advantage of this broad definition of injury is that it becomes possible to assess the effect of the full spectrum of injuries from mild contusions to fractures.5 36 This might be of importance in assessing the long-term consequences of injuries, as an analysis of injury sequences shows that minor injuries are often followed by moderate or major ones,37 and acute complaints are a predictor of subsequent injuries.38 In addition, athletes sometimes compete despite an injury.39 Finally, an “all-encompassing” injury definition36 does not leave it to the physician to judge which injuries should or should not be included. The availability of additional information regarding time loss (estimated duration of subsequent absence from sport) allows expression of the incidence of time-loss injury and the possibility of comparing the results with studies that use that definition.
Newly incurred injuries
In agreement with the consensus statements for football13 and rugby,14 pre-existing, not fully rehabilitated injury should not be reported. Recurrent injuries (injuries of the same location and type) should only be reported if the athlete has returned to full participation after the previous injury.
Report by the responsible physician
Injuries should be diagnosed and reported by qualified medical personnel (team physician, physiotherapist) to ensure valid information on the characteristics of the injury and a comparable standard of data. It is advantageous if each team designates one contact person who will take part in the instructional meeting and will be accessible for questions. In general, the chief physician of the national team should be responsible for reporting the injuries of their athletes. The team physicians should report all newly incurred injuries (or the non-occurrence of injuries) daily on the provided injury report form and should return it daily to the study centre in the stadium or the study headquarters via fax. In situations when the diagnosis (or the duration of absence) is revised later as more information about the injury becomes available, the team physician should report the injury again (with the previous data and location of injury to indicate that this is a revised report) and state the corrected information.
In order that information about injured athletes of teams that do not have a physician or physiotherapist should also be received, injuries should also be reported using the same injury report form, by the medical centres (in the stadium/venues) and/or the polyclinic physicians of the local organisers.
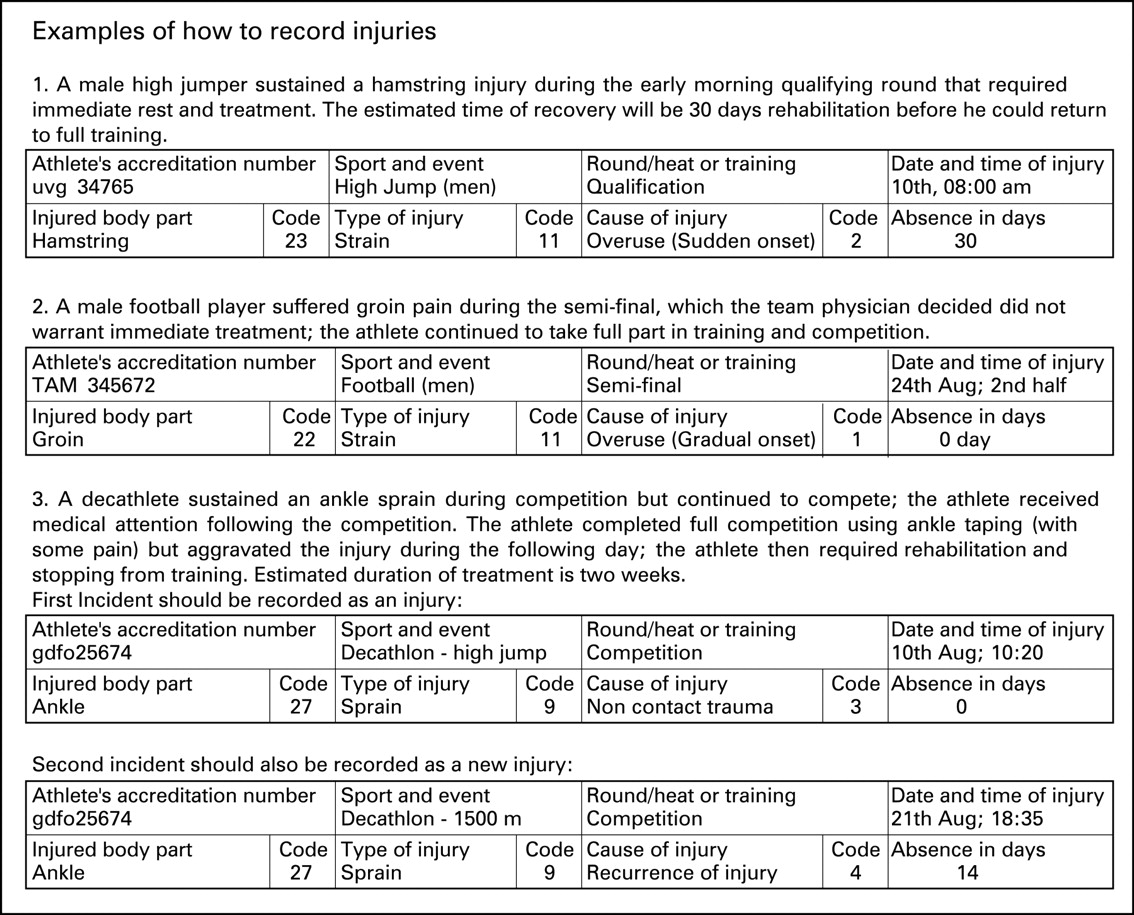
The injury report form
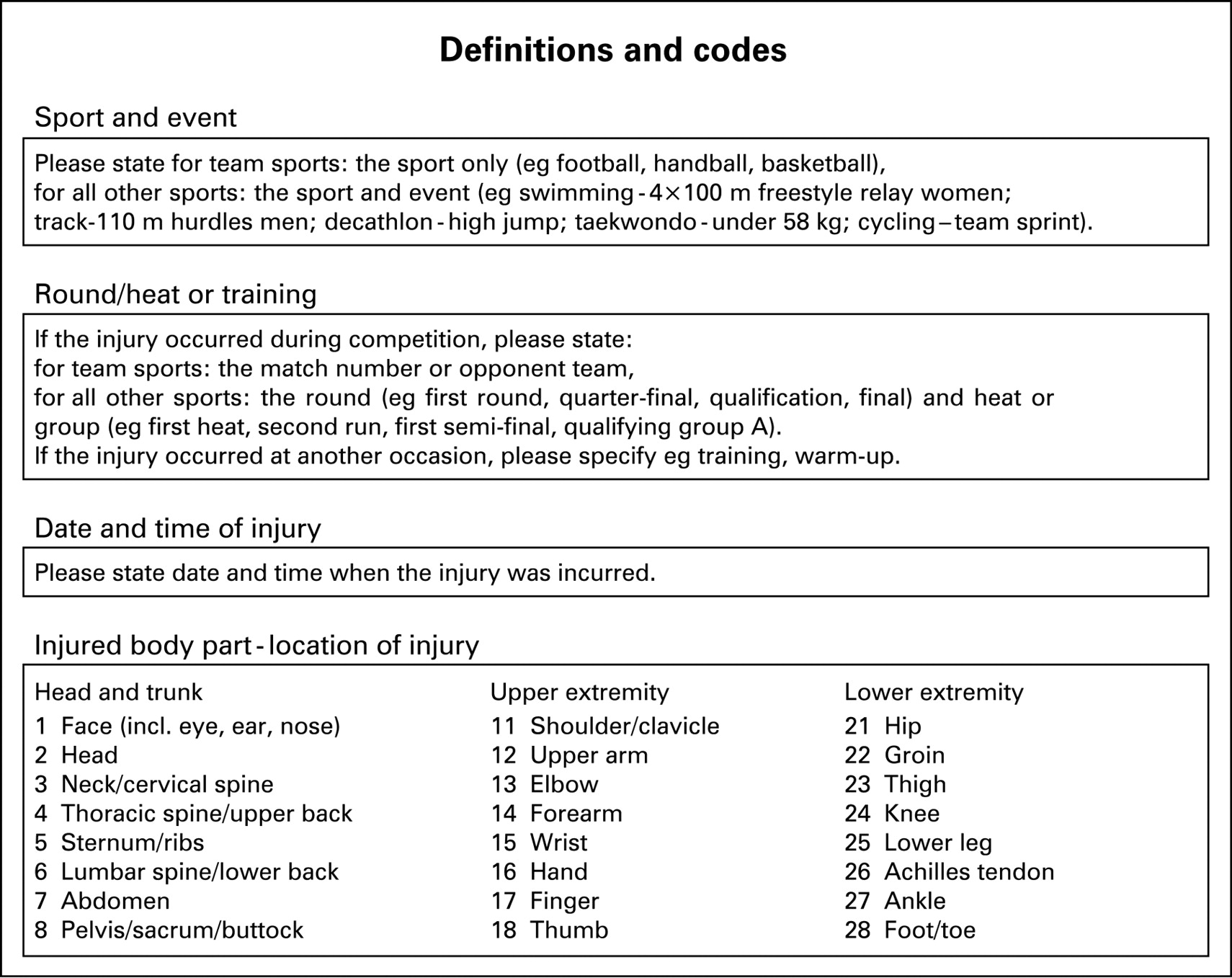
A simple and concise injury report form including the most important variables was developed and tested according to the recommendations of Finch et al.4 This standardised form comprises a single page on which all sports injuries that receive medical attention from the team physician during the day or, if no athlete is injured, the non-occurrence of injury, should be described in tabular form (see appendix 1). The injury report form requires documentation of the following information: accreditation number of the athlete, sport and event, round/heat/training, date and time of injury, injured body part, type of injury, cause of injury and an estimate of the expected duration of subsequent absence from competition and/or training. For “sports and event” and “round/heat or training” the requested information slightly differs between team and individual sports (see appendix 2 for details). Team sports are defined as sports where two teams of athletes who can be substituted during a match play against each other (football, handball, basketball, field hockey, baseball, softball, water polo, volleyball). All other sports (which do not allow the substitution of athletes during a match, heat or race) are considered as individual sports, even if some include team competitions. Definitions of all parameters to be documented are given on the back page of the injury report form (see appendix 2). The injury report form should be provided in all relevant languages.
Accreditation number of the athlete
The accreditation number of the athletes should only be used (1) to avoid double reporting of an injury by the team physician and the medical centre/policlinics, (2) to recognise reports that provide revised information about an already reported injury and (3) to receive additional information about the injured athlete. Usually the organisers of the tournament (eg national/international sports federation or IOC) have a database with information on accreditation number, sex, date of birth, sport, event and country (sometimes also height and weight) of all registered athletes. Based on the accreditation number, this information can be added to the injury database. The advantage of using the accreditation number is that the team physician does not need to document these data, and the injured athletes can be described in more detail and compared with uninjured ones. Furthermore, it facilitates identification of the injury on video coverage for additional analysis.
The accreditation number of the athletes should not be entered into the injury database, and all data must be subsequently made anonymous. If it is not possible to document the accreditation number of the athletes for legal reasons in some countries, the injury report form has to be modified, and the team physicians and medical centre/policlinics need to report the age, sex and nationality of the injured athletes also.
Injured body part
The physician should describe the location of injury in words and give the respective code(s) of the 24 injury locations (each eight of head and trunk, upper limb and lower limb) specified on the back of the form. The selection of injury locations is based on the review of other injury reporting systems (eg Junge et al17, Dick et al25, Lindenfeld et al40), and the consensus statements for football13 and rugby.14 It allows comparison with other established coding systems such as the Orchard Sports Injury Classification System41 and the Sports Medicine Diagnostic Coding System.42 The locations can be summarised under a main heading (head, trunk, upper and lower limb), or in future studies, be subdivided in more detailed categories (eg quadriceps muscle, adductor muscle, abductor muscle, and hamstrings).
Type of injury
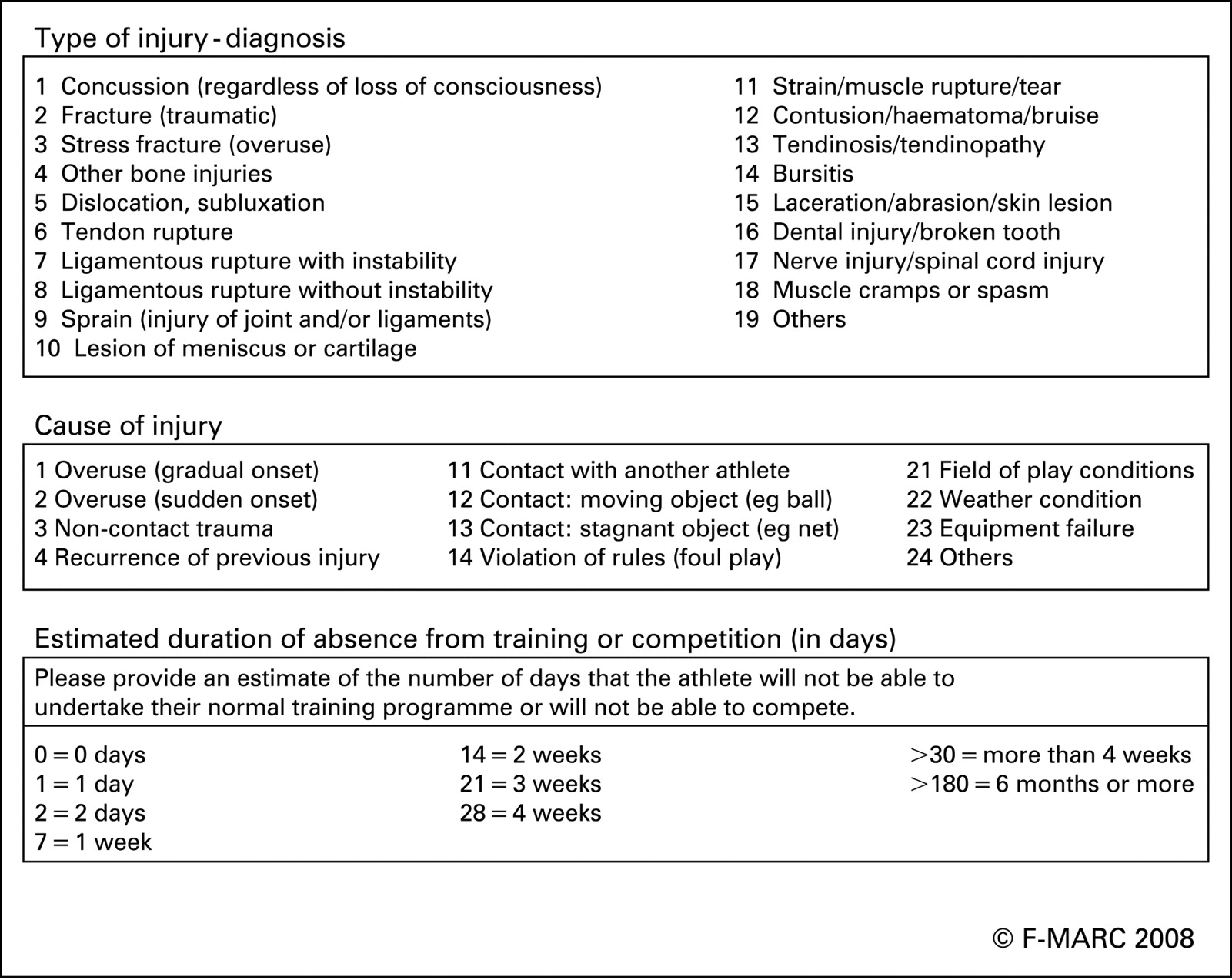
The physician should describe the type of injury in words and give the respective code(s) of the 19 injury types stated on the back of the form. The selection of injury types is based on the review of other injury reporting systems16 17 25 40 and the related consensus statements for football13 and rugby,14 which allows comparison with other established coding systems such as the Orchard Sports Injury Classification System41 and the Sports Medicine Diagnostic Coding System.42 The types of injury can be summarised under a main heading (muscle and tendon, joint and ligament, bone, skin, brain/spinal cord/peripheral nervous system and others), or in future studies, be subdivided in more detailed categories (eg concussion with and without loss of consciousness). In future studies, other medical problems such as illnesses, diseases, or psychological complaints can be included as separate categories.
Cause of injury
The physician should describe the mechanism or cause of injury in words and give 1 or more of the respective codes of the 12 causes stated on the back of the form. The selection of injury mechanism and causes is based on the review of the literature (eg Finch et al4, Fuller et al16, Dick et al25, Lindenfeld et al40) and focuses mainly on extrinsic risk factors. As cause of injury is important information for injury prevention, the selected causes cover a wide spectrum, of which some (eg rule violation, foul play) might only apply to team sports. The main injury mechanisms are defined as follows.
An overuse injury refers to an injury resulting from repeated micro-trauma without a single, identifiable event responsible for the injury and a traumatic injury refers to one caused by a specific, identifiable event. Overuse injuries are divided into two groups based on the onset of symptoms.
A non-contact trauma is defined as a traumatic event without contact with another athlete or object, such as a fall.
The definition and recording of recurrent injury in injury surveillance studies has been outlined in detail by Fuller et al.43 In agreement with recent consensus statements,13 14 a recurrent injury (re-injury) is defined as an injury of the same location and type, which occurs after an athlete’s return to full participation from the previous injury.
Contact events are categorised as contact with another athlete, a moving object (eg ball, puck, racket) or a static object (eg hurdles, net, goalpost). If applicable, it should be indicated whether or not the injury was caused by a violation of the rules of the respective sport.
Playing field conditions (eg uneven ground) include alterations of the playing field by the weather (eg slippery ground.). In such cases, both codes should be provided.
Absence in days
The team physician is asked to provide an estimate of the number of days that the athlete will not be able to undertake their normal training programme or will not be able to compete. A follow-up of the injured athletes could improve the validity of the data, but might be impractical because some athletes participating in the Olympic Games have no associated physician or physiotherapist. In future studies, a follow-up of athletes estimated to be out of competition for >7 days should be arranged with the responsible physician. Duration of absence from sport is regarded as an indicator of injury severity.1 13
IMPLEMENTATION
Beside the methodological issues outlined above, sufficient funding and ethics approval are pre-requisites for implementation of an injury surveillance project. The sports federations and medical representatives of all participating countries/teams should be informed before the championships and be requested to participate in the study. The athlete’s informed consent to participate in the injury surveillance project should be included in their registration for the tournament. The team physicians should receive a booklet with detailed information about the study approximately 1 month before the tournament and should be invited to an instructional meeting 1–2 days before the start of the tournament. They should be motivated to comply with the study and should be instructed by the leader of the project on the correct procedures for completing the injury report forms. During the tournament the returned injury report forms should be checked on a daily basis (for details see below) and the leader of the study should be available to answer questions and to provide motivation to the team physicians. Personal contact and good relationships between the staff conducting the injury surveillance and the physicians providing the injury data is of invaluable importance for the success of the project. It is recommended to pay special attention to team physicians with the most participating athletes. After some days, all team physicians should receive feedback on the completeness of their reports and the first results to increase their compliance with the study. The team physicians, the medical centre physicians, all participating sports federations and the involved organising committees (eg National Olympic Committee) should receive a formal report of the study in adequate time after the end of the tournament.
Confidentiality
It is of utmost importance that the confidentiality of all information is ensured. Regardless of whether the accreditation number or the date of birth and sex of the athlete is documented, this information enables the identification of the injured athlete and must therefore be treated with strict confidentiality. All injury report forms should be stored in a locked filing cabinet and be made anonymous (or destroyed) after the tournament. The accreditation number of the athletes should not be entered into the injury database, and all data files should be anonymous. All analysis and the reports should be either for groups of athletes, or in a way that no individual athlete or team can be identified.
Quality control and response check
During the championship, the returned injury report forms should be checked on a daily basis. First, it should be ascertained that all participating team physicians have returned at least one daily form. Second, the forms should be scanned for missing information. In cases of double reporting by the team physician and the medical centre, the data should be compared and the discrepancies should be clarified. It might be important to analyse the number of injuries reported from different countries in relation to the number of registered athletes of the respective country to check if the injury rates are as expected. It is of great advantage to control the completeness and quality of the injury documentation during the championships, as the team physicians can immediately be contacted, open questions clarified and missing information added. Furthermore, the involved physicians learn during the process, the injury documentation becomes a routine procedure, and prompt feedback increases the compliance with the system.
ANALYSIS OF DATA
Preparation of data
Before analysing the data, it is important to control for double reporting of injuries by the team physician and medical centre/polyclinic. If discrepancies between the reports cannot be clarified, the medical centre report should be excluded. Only injuries incurred in competition or training during the period of the championships should be included in the analysis. If an athlete injures two body parts (eg ankle sprain and abrasion of the knee) or incurs two types of injury in one body part (contusion and laceration of the calf) in one incident, this is counted as one injury with two diagnoses. If the same injury of an athlete is again reported with the same date of injury but a different diagnosis and/or duration of absence, this should be regarded as a corrected update of the injury report. If an athlete incurs the same type of injury at the same body part more than once during a championship this should be regarded as a recurrence and should not be counted as a new injury. Fuller et al13 defined a recurrent injury as: “an injury of the same type and at the same site as an index injury and which occurs after a player’s return to full participation from the index injury”. If an injury was reported for the first time during a championships but the physician reports the cause as “recurrence of previous injury”, this injury is counted as an injury, as no details about recovery from the previous injury are available, and it is assumed that the athlete was able to compete at the beginning of the tournament. Because of the complexity of judging the injuries, it is recommended that the input of the data is prepared and supervised by a person experienced in sports medicine.
What is already known on this topic
Numerous studies have evaluated sports injuries during the season, but few have focused on injuries during major sport events such as World Championships, World Cups or the Olympic Games.
What this study adds
A concise injury surveillance system for multi-sports events has been developed and proved feasible for both team and individual sports.
It will be used during the 2008 Olympic Games in Beijing and should serve as a role model for future studies in single and multi-sport events.
Standardised use of injury definition, report forms and methodology will ensure the comparability of results.
Response rate and coverage
First, the total number of teams or countries and athletes participating in the championships should be ascertained. As not all teams may have a team physician, the response rate can be determined by dividing the number of team physicians participating in the injury surveillance project by the number of teams with a team physician. Subsequently, the number of received injury report forms and its percentage of number of expected forms should be calculated. As the number of athletes varies between teams, the coverage of athletes by the team physician’s reports can be best estimated by multiplying the number of athletes and the number of returned report forms for each team, and relating the sum to the total number of athletes multiplied with the days of the championships. In addition, the number of injury reports from the medical centres should be determined and related to the number of athletes without a team physician. Finally, a comparison of the proportion of injuries reported by the team physicians and the medical centres in relation to the number of athletes in teams with and without team physicians might indicate the completeness of the injury reports.
Frequency and characteristics of injury
It is important to distinguish between number of injuries and number of injured athletes, as an athlete can incur more than one injury during a tournament. It should be reported how many athletes incurred no injury, one injury and >1 injury. If an athlete has an unexpectedly high number of injuries, the data should be carefully inspected. Injuries in competition and training should be analysed and reported separately. It is recommended to present the frequency of different diagnoses (best in tabular form), instead of reporting the number of injuries for body part and type of injury unconnectedly. Concerning the cause of injury, the rate of overuse and traumatic injuries at least should be reported. However, for the development of preventive interventions, it is of interest to know how many athletes suffered a recurrent injury and how many injuries were caused by contact with another athlete or an object, by violation of rules, by equipment, by playing field properties or by weather conditions.
All injuries that result in the athlete being unable to undertake their normal training programme or being unable to compete for at least the day after injury are classified as time-loss injuries. In accordance with Fuller et al13 the severity of an injury is defined as the number of days the athletes are unable to undertake their normal training programme or to compete. Injury severity is usually classified as minor (1–7 days, some studies further subdivided into 1–3 and 4–7 days), moderate (8–28 days), severe (>28 days), and career-ending injuries. The characteristics, circumstances and causes of severe and career-ending injuries should be described in detail, together with information about the athlete (age, gender, type of sport).
Population at risk and exposure
The importance of exposure data in injury surveillance has often been stated.10 44 45 Similar to injuries, exposure should be analysed and reported separately for competition and training. Exposure can be expressed in different ways: in relation to the population at risk (total number of athletes), to the number of exposing situations (training session, match or competition) or to exposure time (hours spend in competition or matches). Information about the population at risk and the number of competing athletes is usually available from the schedule and start lists of the championships, but training exposure must be documented for each individual athlete. Exposure time in competition is difficult to determine for most sports (except for team sports with a fixed match duration), and it can be questioned if exposure time is the best basis for a comparison of risk exposure in multi-sport events.17
Registered athletes (population at risk)
All athletes officially registered for the tournament by the governing body (entry list), independent of whether or not they participate in any competition.
Competing athletes (athletes exposed to competition)
For individual sports, the number of competing athletes is defined as all athletes who start at least once in an event, irrespective of whether or not the athlete finishes the event. Athletes who do not finish (DNF), who are disqualified (DQ) or whose result is not measured (NM) are counted as having started. If an individual athlete participated in >1 event, the athlete is counted in each event. Thus, the total number of competing athletes is not identical (but slightly higher) than the sum of the individual athletes. For team sports, the number of competing athletes is the number of players plus the maximum number of substitutes to be used in a match (as defined in the rules of the respective sport).
Participations (athletes’ exposure in competition)
For individual sports, the number of athletes starting in all heats, rounds, qualifications and finals are summed to give the number of participations in a particular event or championship. If an athlete has >1 starts in the same or a different event, each start is counted. For team sports, the maximum number of players allowed on the field of play (as defined in the rules of the respective sport) multiplied by the number of teams and matches determines the number of participations (equivalent to player matches) in a particular event or championship.
Exposure hours
For team sports with a fixed match duration the total exposure hours can be calculated by multiplying the maximum number of players allowed on the field of play and duration of a match in hours by the number of matches.17 For all other sports and for training, the exposure time must be documented individually.
Calculation of injury incidence
In a statistics primer on epidemiological concepts in sports medicine, Kuhn et al46 defined incidence as the “number of new cases that developed over a specific period of time” and distinguished between relationships of this figure with the at-risk population or with the exposure time. In studies on sports injury, the incidence of injury is usually expressed as (1) number of injuries per 100 or 1000 athletes, (2) number of injuries per 100 or 1000 athlete-exposures or (3) number of injuries per 1000 hours training and/or competition. It has been stressed that injury rates should be calculated separately for training and competition.9 13
However, Junge et al17 have previously described a methodological dilemma in comparing the incidence of injury in different sports. The number of injuries per athlete ignores the fact that a tournament is comprised of different numbers of competitions for each sport. An exposure-time related incidence (number of injuries per 1000 hours exposure) seems to be the most accurate methods, but it can be questioned if a comparison of “1 hour of football”, “1 hour of 100 m sprint” and “1 hour of archery” makes any sense in the context of sports injury surveillance. Thus, in agreement with Junge et al,17 we recommend that an athlete’s individual risk of injury in multi-sport events should be best expressed and compared as “injuries in competition per 1000 athlete participations”.
CONCLUSION
An injury surveillance system for multi-sports events was developed, based on established injury-reporting system developed for team sports tournaments. The injury report system proved feasible for team sports during the 2004 Olympics and for individual sports during the IAAF World Championships 2007. It will be used during the 2008 Olympic Games in Beijing and should serve as a role model for future studies in single and multi-sport events. Implementation of the injury surveillance system, all definitions, the injury report form, and analysis and reporting of data are described in detail to enable other researchers to implement the injury surveillance system in any sports tournament. The system can be modified to address the specific objectives of a certain sport or research question; however, a standardised use of injury definition, report forms and methodology will ensure the comparability of results.
Acknowledgments
We gratefully acknowledge the International Olympic Committee (IOC) and the Fédération Internationale de Football Association (FIFA) for their support and the funding of the study. We thank the International Association of Athletics Federations (IAAF), for the conduction of the pilot study during the IAAF World Championship 2007 in Osaka.
Appendix 1

Appendix 2


Appendix 3

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
REFERENCES
Footnotes
Competing interests: None.