Article Text

Abstract
Objective: To determine prospectively gait-related intrinsic risk factors for patellofemoral pain (PFP) in a population of novice recreational runners.
Design: Prospective cohort study.
Participants: 102 novice recreational runners (89 women) with no history of knee or lower leg complaints.
Interventions: The standing foot posture of the subjects was examined and plantar pressure measurements during running were collected. The subjects then participated in a 10-week “start to run” programme. During this period all sports injuries were registered by a sports medicine physician.
Main outcome measurements: The relationship between the standing foot posture and PFP was investigated and gait-related intrinsic risk factors for PFP were determined.
Results: The 17 runners who developed PFP exerted a significantly higher vertical peak force underneath the lateral heel and metatarsals 2 and 3. Logistic regression analysis showed that a significantly higher vertical peak force underneath the second metatarsal and shorter time to the vertical peak force underneath the lateral heel were predictors for PFP. No significant evidence was found for an association between an excessively pronated or supinated foot posture and the development of PFP.
Conclusions: The findings suggest that an excessive impact shock during heel strike and at the propulsion phase of running may contribute to an increased risk of developing PFP. The hypothesis that persons at risk for PFP show an altered static foot posture in comparison with non-afflicted persons is not supported by the results of this study.
Statistics from Altmetric.com
The growing interest in disease prevention has led to increased participation by the public in sports during recent decades.1 2 Owing to its easy accessibility, distance running is practised by many people and has increased in popularity.2 The increased participation in sports leads to an increase in sports-related injuries. Runners continue to be among the most commonly injured athletes.3 Studies estimate the yearly incidence of running injuries to be 37–56%.4 5
Epidemiological studies have found that most of the injuries in runners are located in the knee, with patellofemoral pain (PFP) syndrome being the most prevalent injury.2 4 6–9 Owing to the growing interest of the public in running, novice recreational runners are becoming a considerable population at risk for the development of anterior knee pain.
Despite the high incidence of PFP in competitive and recreational athletes,10–12 there is still a lack of consensus concerning the aetiological mechanisms of this disorder. Focusing on the structures around the knee joint, factors such as malalignment of the patellofemoral joint, soft periarticular tissue imbalances, weakness of the quadriceps muscle, vasti muscle imbalance and bony abnormalities have been identified as potential risk factors for the development of PFP.12–14 However, it has been recognised that the mechanics of the patellofemoral joint is also influenced by segmental interactions of the lower extremity.15 Abnormal kinematics of the ankle and foot have therefore been proposed as one of the possible risk factors for PFP.13
A number of studies have investigated foot motion as a risk factor for PFP, with a focus on abnormal pronation of the foot and subsequent lower extremity rotation.13–22 However, a review of the literature has shown that there is no consensus as to whether abnormal pronation of the foot is an aetiological factor for anterior knee pain. One of the most important reasons for this lack of consensus is probably the absence of prospective studies designed to determine risk factors for PFP. Most studies which have investigated the relationship between foot movement and PFP have been retrospective or theoretically-based.13–22 Because of their retrospective design, it is unclear if the deficits found in these studies are a cause or a consequence of the injury.
With the current emphasis on injury prevention, studies designed to examine potential intrinsic risk factors for PFP before the occurrence of injury are imperative. The purpose of this investigation was therefore to perform a comprehensive prospective study on gait-related intrinsic risk factors for PFP in a population of novice recreational runners. It was hypothesised that subjects who develop PFP show an altered rollover pattern and posture of the foot in clinical measurements.
METHODS
Subjects
One hundred and forty-three novice recreational runners enrolled in a 10-week “start to run” programme organised by a Belgian track and field club in April 2007 agreed to participate in the study. Fourteen were excluded because they had had a surgical procedure involving the knee, lower leg, ankle or foot or a history of an injury to the knee, lower leg, ankle or foot that caused them to seek medical attention during the 6 months before the start of the study, so 129 runners (107 women) were prospectively examined. Twenty-seven of the 129 tested subjects quit the “start to run” programme for reasons other than the development of an injury (social or work-related reasons) and consequently dropped out of the study.
The remaining 102 runners had a mean (SD) age of 37 (9.5) years, a mean (SD) height of 165 (25) cm, a mean (SD) weight of 69 (15) kg and a mean (SD) body mass index (BMI) of 25 (3) kg/m2.
Evaluation
Before the initiation of the “start to run” programme, the static standing foot posture of the subjects was evaluated using the foot posture index (FPI). The rollover pattern of the subjects’ feet was examined during running using a footscan pressure plate.
Evaluation of standing foot posture
The FPI is a validated clinical tool for quantifying the degree to which a foot can be considered to be in a pronated, supinated or neutral position.23 It is intended to be a simple method of scoring various features of foot posture into a quantifiable result, which gives an indication of the overall foot posture.
According to the guidelines of Redmond et al,23 the subjects were asked to stand on a platform in a relaxed stance position with double limb support, their arms by the side and looking straight ahead. By palpation and a series of observations, the weight-bearing foot posture was rated according to a series of predefined criteria. The six clinical criteria employed in the FPI were: (1) palpation of the talar head; (2) observation of the supralateral and infralateral malleolar curvature; (3) observation of the calcaneal frontal plane position; (4) observation of prominence in the region of the talonavicular joint; (5) observation of the congruence of the medial longitudinal arch; and (6) observation of abduction/adduction of the forefoot on the rearfoot. Each of the component tests was graded 0 for neutral, −1 for moderate signs of supination, −2 for clear signs of supination, +1 for moderate signs of pronation and +2 for clear signs of pronation. When the scores of each test were combined, the aggregate value gave an estimate of the overall foot posture. High positive aggregate values indicated a pronated posture (pronated, +6 to +9; highly pronated, 10+), high negative aggregate values indicated a supinated overall foot posture (supinated, −1 to −4; highly supinated, −5 to −12) and an aggregate score from 0 to +5 indicated a neutral foot. Each foot was scored independently. All of the subjects were evaluated by the same examiner.
Plantar pressure measurements
Before the start of the training period all subjects underwent plantar pressure measurements during barefoot running. By running barefoot, discrepancies due to unusual footwear were controlled. Clarke et al24 have stated that barefoot is an acceptable baseline state in running analysis, and it has been shown that gait-related risk factors for exercise-related lower leg pain are more distinct in the barefoot condition than when wearing shoes.25 A footscan pressure plate (RsScan International, Olen, Belgium; 2×0.4 m, 480 Hz) was mounted in the middle of a walkway 15 m in length. The walkway was covered by a thin rubber mat so that the pressure plate would not be visible to the subjects.
The subjects were asked to run at a comfortable moderate velocity along the walkway. All subjects were allowed to familiarise themselves with the procedures before data collection. Three valid left and right stance phases were measured. A trial was considered to be valid when there was a heel strike pattern and no adjustment in step length or frequency to aim on the pressure plate. De Cock et al26 found that temporal plantar pressure variables measured with a footscan pressure plate are reliable (ICC >0.75).
Data analysis
For each trial of the plantar pressure measurements, the footprint was divided into eight anatomical areas (fig 1). These eight zones were defined as the medial heel (H1), lateral heel (H2), metatarsals I–V (M1, M, M3, M4, M5) and the hallux (T1).
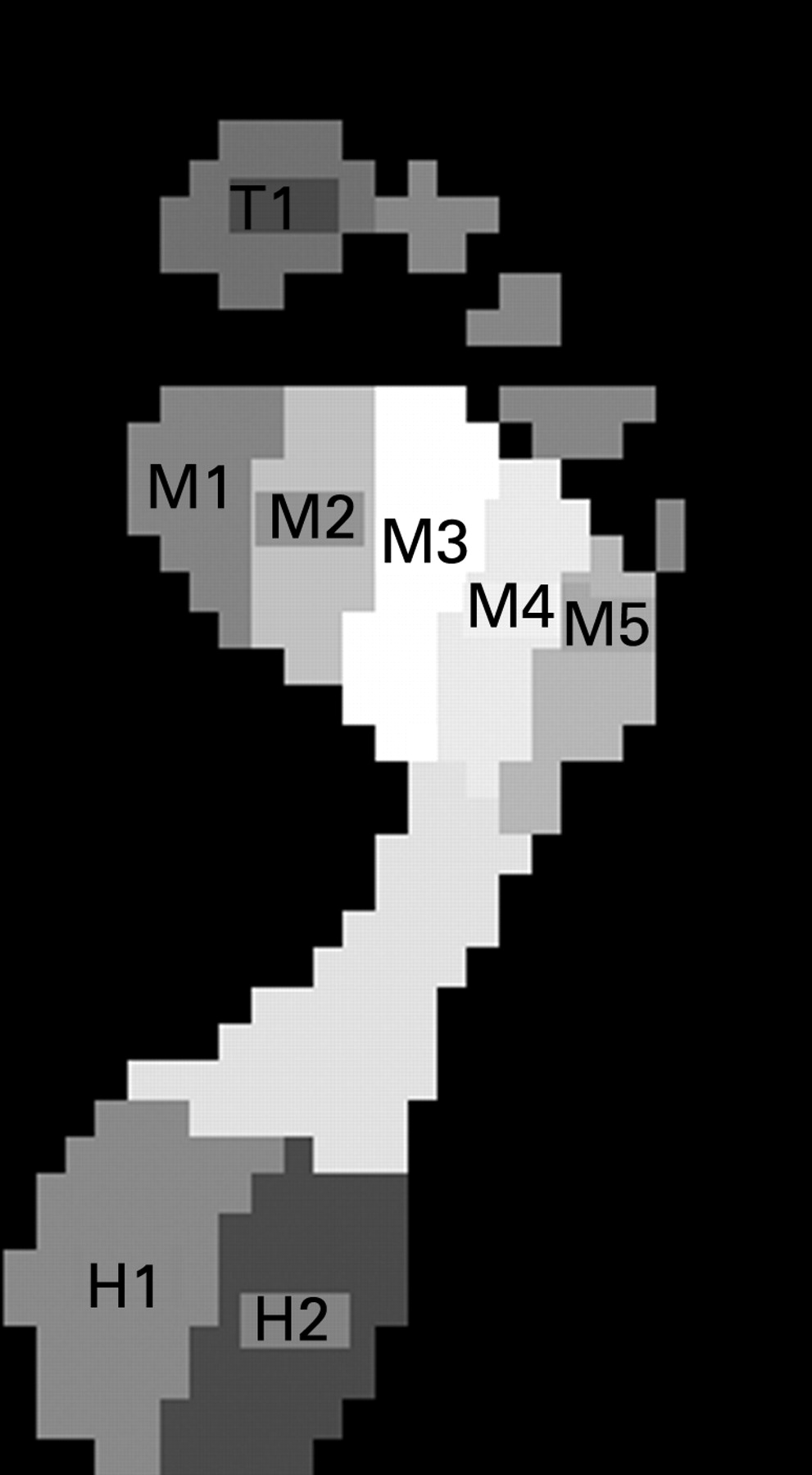
Temporal data (time to peak force, time at which the regions made contact and time at which they ended contact), peak force data and absolute impulses (mean force × loaded contact time) and relative impulses (absolute impulse ×100/sum of all impulses) were calculated for all eight regions. The total foot contact time and five distinct times of foot rollover were determined for each trial. These five instants of foot rollover were: first foot contact (FFC), first metatarsal contact (FMC), forefoot flat (FFF), heel off (HO) and last foot contact (LFC). FFC was defined as the time point at which the foot made first contact with the pressure plate; FMC was defined as the time point when one of the metatarsal heads contacted the pressure plate; FFF was defined as the first time point when all metatarsal heads made contact with the plate; HO was defined as the time point at which the heel region ended contact with the plate; and LFC was defined as the last contact of the foot on the plate. Based on these time points, total foot contact could be divided into four phases: initial contact phase (ICP = FFC to FMC), forefoot contact phase (FFCP = FMC to FFF), foot flat phase (FFP = FFF to HO) and forefoot push-off phase (FFPOP = HO to LFC).
A mediolateral force ratio ((M1 + M2 + H1)/(M4 + M5 + H2)) was calculated at the five time points of foot contact. This ratio describes the force distribution in the foot at the five time points of foot contact. Excursion ranges of this ratio were calculated over the four phases (ICP, FFCP, FFP, FFPOP).
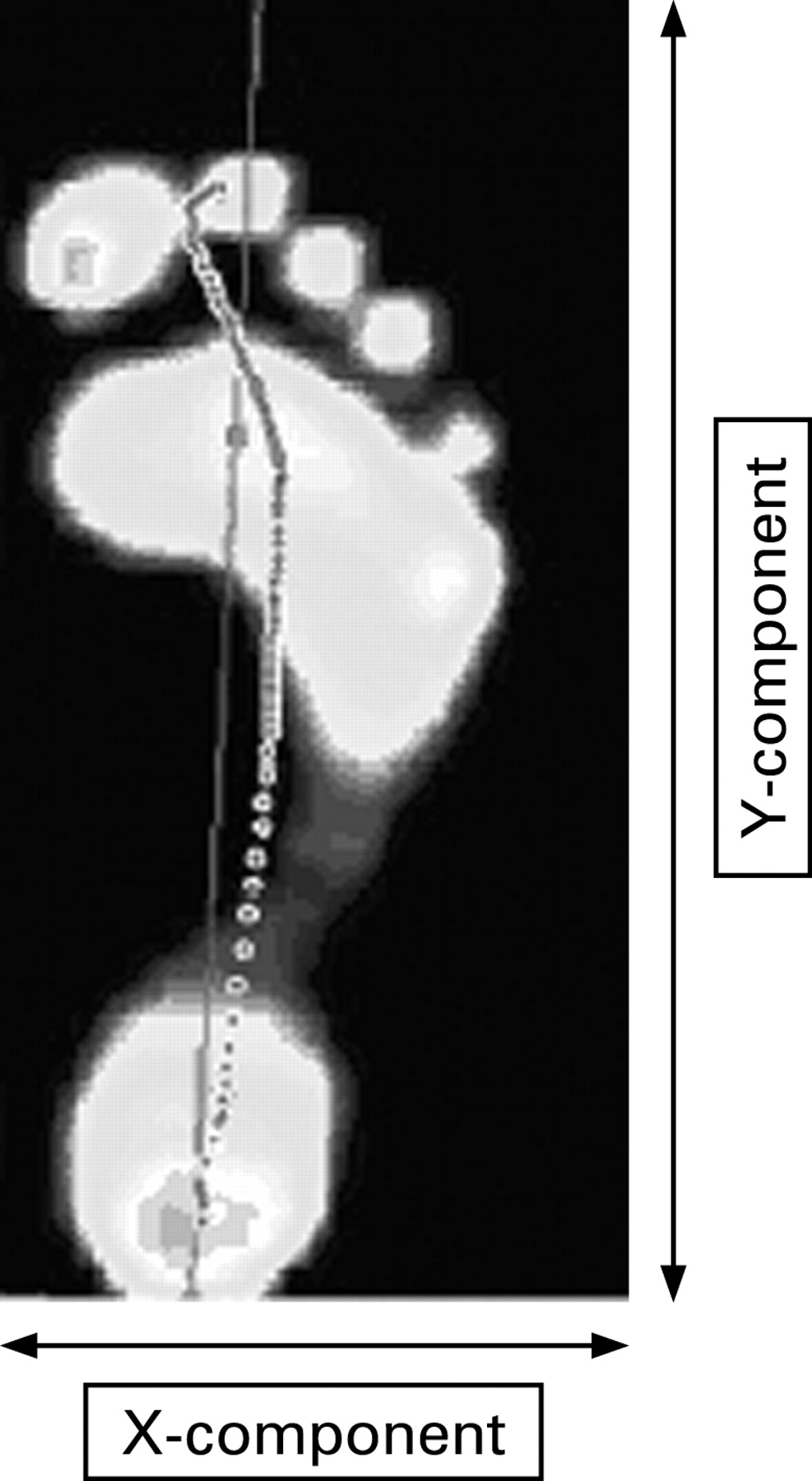
The X-component (mediolateral) and Y-component (anterior–posterior) of the centre of force (COF) scaled to the foot width and foot length, respectively, were analysed (fig 2). The positions and displacements of the components at the five time points and in the four phases were calculated.

{kind=link}
{kind=link}
The mean value of all the kinetic data was taken from the three trials. De Cock et al have shown that the mean of three trials is sufficient for analysis.26 27
“Start to run” programme
The subjects included in this study were all untrained novice runners at the start of a 10-week “start to run” programme. During this “start to run” programme the subjects trained three times a week following a fixed schedule with the aim of being able to run a distance of 5 km at the end of the 10th week of the training programme. The training sessions were all group sessions under supervision of an experienced track and field trainer. The subjects who participated in this study did not practise any other kind of sports activities during the course of the “start to run” programme.
Registration of injuries
During the 10-week “start to run” programme, patellofemoral complaints were diagnosed and registered by the same sports medicine physician. The subjects were able to freely consult this sports medicine physician, who was present at each training session. For a diagnosis of PFP, subjects had to have a characteristic history and symptoms of PFP syndrome and exhibit two of the following clinical criteria on assessment: pain on direct compression of the patella against the femoral condyles with the knee in full extension; tenderness of the posterior surface of the lateral or medial rim of the patella on palpation; pain on resisted knee extension; or pain with isometric quadriceps muscle contraction against suprapatellar resistance with the knee in 15° of flexion. In addition, subjects had to have negative findings in the examination of knee ligaments, menisci, bursae, synovial plicae, Hoffa’s fat pad, iliotibial band, the hamstrings, quadriceps and patellar tendons and their insertions. Previous studies indicate that these criteria are sensitive and specific for diagnosing PFP.12 28 29
Statistical analysis
Statistical analysis was performed with SPSS for Windows Version 12.0. A binary logistic regression analysis30 was performed to identify gait-related intrinsic risk factors for PFP. In order to reduce the number of variables, Student t tests (if the distribution of the data was normal) or Mann-Whitney U tests (if no normal data distribution was obtained) were undertaken to examine possible differences between the group who developed PFP and those with no symptoms for each of the test variables. All variables with a p value <0.1 in the univariate analysis were entered separately into the logistic regression analysis.
A Pearson χ2 test was conducted to examine the relationship between the static standing foot posture and the development of PFP. Statistical significance was accepted at the level of α⩽0.05.
RESULTS
Seventeen of the 102 runners (16 women) developed PFP during the 10-week “start to run” programme. The anthropometric characteristics of the 17 subjects who developed PFP were compared with those without PFP (table 1). There were no significant differences between these two groups with respect to their mean age, height, weight and BMI.
Analysis using Student t tests showed that the vertical peak force underneath the second and third metatarsals (p = 0.016 and p = 0.026, respectively) and underneath the lateral heel (p = 0.034) was significantly higher in the PFP group than in the non-PFP group. Logistic regression analysis revealed a significantly higher vertical peak force underneath the second metatarsal as a predisposing factor for PFP (p = 0.037, table 2).
For the temporal data, t tests indicated that the time to the vertical peak force underneath the lateral heel and the medial heel (p = 0.037 and p = 0.016, respectively) relative to the total time of foot contact was significantly shorter in the PFP group than in the non-PFP group. Logistic regression showed a significantly shorter time to the vertical peak force underneath the lateral heel as a predisposing factor for PFP (p = 0.048, table 3). Logistic regression did not identify significant differences for any other temporal parameters.
There were no significant differences between the runners who developed PFP and the non-PFP group in the mediolateral force distribution at the five time points and four phases of foot contact during foot roll-over.
Pearson’s χ2 test showed no relationship between the presence of a neutral, pronated, highly pronated, supinated or highly supinated static foot posture and the development of patellofemoral problems in the investigated population (p = 0.788). The distribution of the subjects in the PFP and non-PFP groups into the five FPI categories is shown in table 4.
No differences were seen when the foot roll-over patterns and the relationship between the standing foot posture and the development of PFP were analysed in women only, which formed the majority of the investigated population.
DISCUSSION
Motions of pronation and supination occur during the roll-over pattern of the foot and assist in normal locomotion during walking and running. It has been suggested that aberrations in these motions may contribute to the pathomechanics of PFP.1 14 15 20 21 31 Excessive pronation of the subtalar joint is an abnormality which has been considered a possible risk factor for the development of PFP. However, there is no consensus on this issue in the current literature.1 13–15 20 21 31 32
The purpose of this investigation was to determine prospectively if a certain roll-over pattern and static posture of the foot predisposes recreational runners to the development of anterior knee pain.
In the recreational runners who participated in this study, anterior knee pain was the most common sustained injury (17%) followed by shin splints (11%) and injury due to Achilles tendon overuse (10%). The other injuries sustained were overuse of the ankle joint (6%), iliotibial band friction syndrome (4%), adductor injuries (3%), ankle inversion injuries (3%), patellar tendinitis (1%) and meniscal injury (1%). The incidence of patellofemoral problems in this population of novice runners is in accordance with previous studies which have reported the knee as the most common site of overuse injury in runners, with patellofemoral problems predominating.2 4–9 15 33
The results of this study show that the runners who developed patellofemoral problems exerted a significantly higher vertical peak force underneath the lateral heel and underneath the second and third metatarsal during running. The results indicate that an excessive vertical peak force at the lateral side of the heel during heel impact and an excessive vertical peak force underneath the second and third metatarsal during the propulsion phase of running may be discriminating factors between runners who develop PFP and those who do not. Our results are similar to the findings of Callaghan and Baltzopoulos14 who also found that runners with PFP exerted a significantly higher maximum vertical force at heel impact and a significantly higher maximum vertical propulsive force than those without PFP. Logistic regression analysis of our results showed that a significantly higher vertical peak force underneath the second metatarsal was a predicting factor for the development of PFP in the investigated population. During the roll-over pattern of the foot the peak pressures for the metatarsal areas occur during the forefoot push-off phase of foot roll-over.26 According to a study by De Cock et al,26 the rise to peak pressure starts laterally at the fifth metatarsal, followed by a synchronous push-off pattern of the fourth, third and first metatarsal. Finally, the second metatarsal reaches its maximal pressure at approximately 62% of total foot contact and is the last metatarsal to reach its peak pressure and leave the ground.26 Our finding is in accordance with the findings of Messier et al18 who also demonstrated a significantly higher maximum vertical propulsive force in runners with PFP. Although in our study the difference in vertical peak force between the PFP and non-PFP groups was only significant underneath the lateral heel and second and third metatarsals, it is remarkable that, in the PFP group, the vertical peak force values where higher underneath all eight anatomical areas (table 2).
In the runners who developed PFP, the significantly higher vertical force at the lateral heel during the heel strike and at the second metatarsal near the end of the propulsion phase could cause higher vertical forces to be transferred to the more proximal joints such as the knee. This higher impact shock could cause an excessive load on the patellofemoral joint which eventually may lead to an overload of this joint, resulting in the development of PFP.
The vertical peak force at the medial and lateral heel at heel strike was reached sooner in the runners who developed PFP than in the non-PFP group. Logistic regression identified a significantly shortened time to the vertical peak force at the lateral heel as the second gait-related risk factor for the development of PFP. These results are in contrast with the findings of Messier et al18 who did not find a significant difference in the time to maximum vertical force at heel impact between runners who developed PFP and those who did not. However, in our study, logistic regression identified a relatively shorter time to the vertical peak force at the lateral heel as an intrinsic risk factor for PFP, with an odds ratio (which depicts the ratio of the odds of an event occurring in one group to the odds of it occurring in the other group) of 3.45×10−14. Because the odds ratio of this parameter approached zero, the odds that PFP developed as a result of a shortened time to the vertical peak force at the lateral heel is very small. We therefore believe it would be wise to consider the significance of this parameter as a trend that requires further verification.
Previous retrospective or theoretically-based studies have speculated on the relationship between excessive foot pronation and PFP.1 11 19 20 22 34 In the present study the mediolateral force distribution underneath the sole of the foot during foot roll-over was not seen as an intrinsic risk factor for PFP. Thus, in this study population the results did not show signs of the presence of abnormal dynamic foot pronation in those with PFP. It has been suggested that excessive pronation can lead to excessive tibial and femoral internal rotation and patellar displacement resulting in pain. However, Powers et al[13 did not find significant differences in the magnitude and timing of peak foot pronation between individuals with PFP and those without PFP. Also, in a prospective study, Hetsroni et al32 found no consistent association between static or dynamic parameters of foot pronation and the risk of anterior knee pain.
What is already known on this topic
An abnormal foot posture and aberrations of foot motion during walking and running have been suggested to contribute to the pathomechanics of PFP, with a focus on abnormal foot pronation.
In the investigated population there was no significant evidence of an association between individuals with neutral, pronated, highly pronated, supinated or highly supinated static foot posture and the development of PFP. In the literature there is controversy regarding the static posture of the foot and its contribution to PFP.12 17 18 35 Powers et al35 reported that subjects with PFP had a greater degree of rearfoot varus than those without PFP. Similarly, Levinger and Gilleard17 found that individuals with PFP had a significantly more inverted position in subtalar joint neutral measurements and more rearfoot valgus in relaxed standing posture than asymptomatic controls. In contrast, a prospective study by Witvrouw et al12 found no significant differences in foot types between persons with and without PFP. Messier et al18 found that individuals with PFP had normally arched feet. However, Powers et al35 and Levinger and Gilleard17 reported that subjects with PFP had a more inverted position in subtalar joint neutral measurements, but caution must be made in generalising this finding to the entire population of subjects with PFP. Both authors indicated that the differences between the group means (approximately 1° and 2°, respectively) were only slight and are debatable, despite the statistical significance. In addition, other factors that may contribute to PFP were not controlled for in their studies. The results of our study are in agreement with the findings of Witvrouw et al12 which suggest that static foot posture is not a predictive factor for the development of PFP. The more inverted position of the subtalar joint in individuals with PFP reported by Powers et al35 and Levinger and Gilleard17 was measured with the subtalar joint in a neutral position during non-weight-bearing, while in our study the foot posture was evaluated in a weight-bearing position. The differences in the methods may also partly account for the differences found between these studies.
What this study adds
A significantly higher impact shock during the heel strike and propulsion phase of running may contribute to the development of PFP.
No evidence was found for an association between the static standing foot posture or mediolateral force distribution during foot roll-over and the development of PFP.
In addition, the studies of Powers et al and Levinger and Gilleard were retrospective studies. A frequent question in retrospective studies is whether the findings are the result or the cause of the injury. The findings of these authors are not, however, supported by the results of the earlier prospective study of Witvrouw et al12 or our prospective study.
CONCLUSION
A significantly higher vertical propulsive peak force underneath the second metatarsal and a shortened time to the vertical peak force at the lateral heel were identified as predisposing factors for PFP. Runners who developed PFP also had a significantly higher vertical peak force at the lateral heel and the third metatarsal. Further verification is needed to determine the association between this predisposing factor and the development of PFP. The results indicate that a significantly higher impact shock during running may contribute to the development of this disorder.
No significant evidence was found of an association between an excessively pronated or supinated foot posture or mediolateral force distribution during foot roll-over and the development of PFP in the investigated population.
More prospective studies are required to determine whether the examination of foot posture and roll-over pattern of the foot is an important addition to other clinical measurements to explore the underlying aetiology of PFP.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: The aim of the study was explained to each subject, all of whom gave written informed consent. The study was approved by the ethics committee of the Ghent University Hospital.