Article Text

Abstract
In 1992 van Mechelen et al published a “sequence of prevention model” based on a four-step process. This model has been widely used to implement preventive measures in response to sports injuries. However, the execution of this model has been shown to lack validity in determining the success of a preventive measure. A modified model has therefore been proposed which incorporates additional steps that enable the inclusion of external factors with a significant effect on the outcome of a prevention intervention. This expansion of van Mechelen’s model leads to a more global model in which the compliance level and risk-taking behaviour of the individual and the assessment of efficiency of the stakeholders have a key influence on the preventive measure. This model gives a better insight into the different processes in injury prevention that can be used by clinicians, coaches and managers to decide whether to implement a preventive measure programme.
Statistics from Altmetric.com
Managers and trainers are responsible for coaching athletes to meet the requirements of the sport in terms of their physical capacity as well as their mental aptitude. An athlete’s job is physically and mentally demanding, and when the physical stress exceeds the loading capacity, injury occurs. Overuse injuries in both professional and recreational athletes are costly owing to working days lost and the cost of medical care.1 The introduction of successful injury prevention programmes has reduced morbidity in athletes as well as providing economic benefits. Injuries are of great concern for the athletes, their families, trainers, managers, sponsors, team mates and for the society in general.2 3 Injuries reduce the level of readiness of the athlete, cause harm, reduce morale and cost time and money.4 Injuries of the musculoskeletal system may be of acute or traumatic origin (eg, rupture of the anterior cruciate ligament, ankle sprain) or due to chronic or overuse (eg patellofemoral pain, Achilles tendinopathy). These pathologies have also been divided into “single event” (traumatic) or “repeated event” (series of minor stresses) conditions.5–7
Although great attention is paid to the selection, training and individual equipment of the athlete, overuse injuries occur frequently in sport and in the military environment where individual soldiers may be considered as professional athletes performing for a longer duration (full career) but at a lower level than the professional sports athlete.8 9 Overuse injuries in the military environment last five times longer than traumatic injuries of the musculoskeletal system.10
The adage of Erasmus (1466–1536) that “prevention is better than cure” has been translated or has an equivalent expression in all languages of the world—for example, “an ounce of prevention is worth a pound of cure” or “a stitch in time saves nine”—and the application of this philosophy in injury prevention reduces the likelihood of long-term morbidity by proactively addressing causative factors.
MODEL
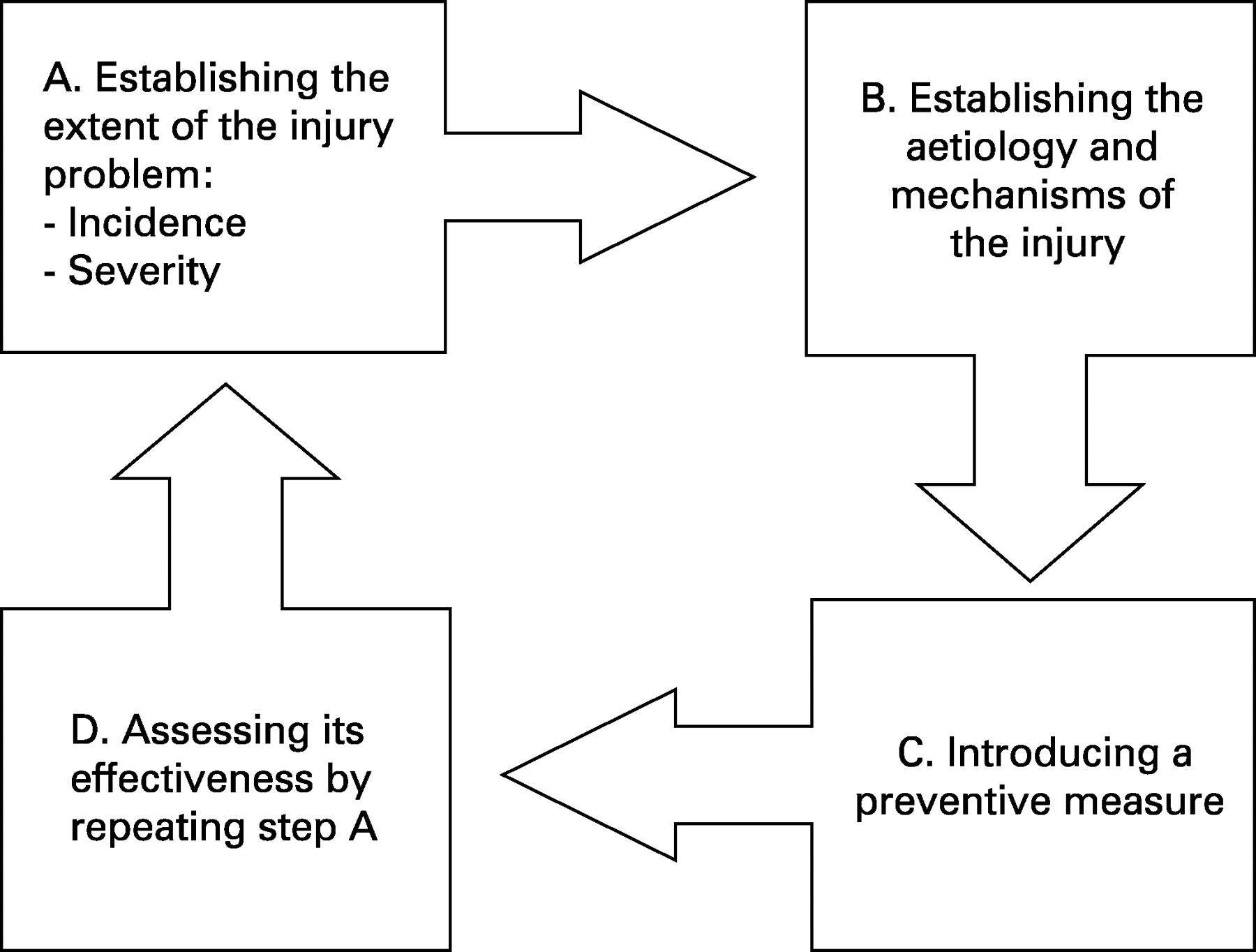
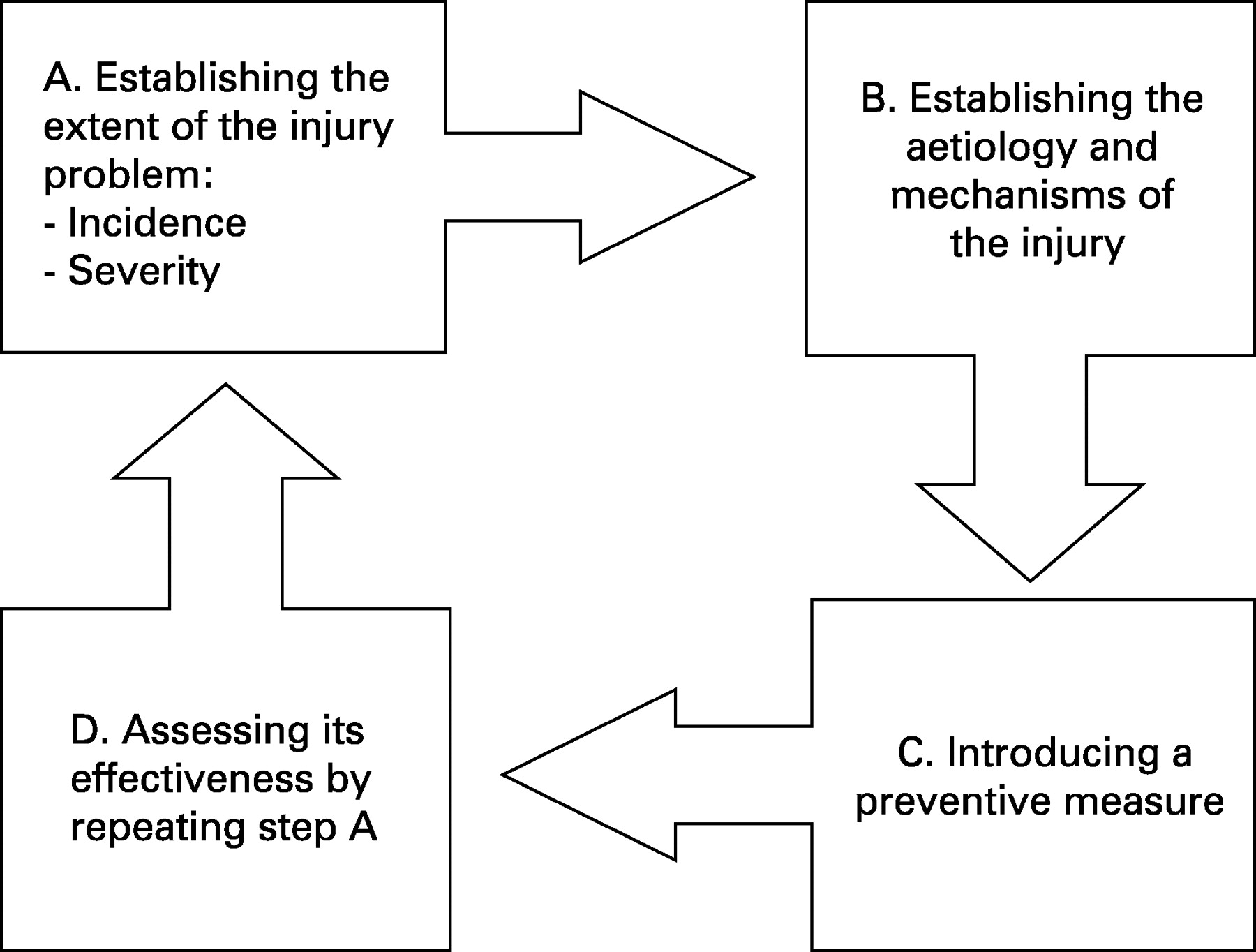
van Mechelen et al11 presented a four-step model to implement injury prevention programmes efficiently (fig 1). In step A, data are collected to establish the extent of the injury in the predetermined population. The localisation and extent of overuse injuries in athletes is largely sport-specific12–21—and even position-specific in team sports22–24—and therefore the boundaries of the population need to be clearly defined. During step B the aetiology and mechanisms of the injury are identified before introducing preventive measures in step C. These preventive measures must be based on the data collected on the aetiology and injury mechanisms in the previous step. However, the majority of (sports) overuse injuries have a multifactorial origin which complicates identification of the mechanisms and risk factors. Finally, the effectiveness of the preventive measure is assessed by repeating the first step (step D). A review of the literature has shown that few prospective studies of the risk factors (step B) and subsequent prevention of injuries (step C) have been published.25 26
Despite the availability of biomechanical models to assess injury causation and prevention, they do not take into account important psychosocial factors such as the behaviour, attitude or motivation of the individual athlete. Some authors6 27 28 warn against modifications in the “risk homeostasis” by implementing preventive measures.29 This means, for instance, that cycling with a special helmet or driving a “safe” car might result in more risk-taking behaviour by cycling or driving faster or more aggressively. In a sports context, wearing knee and elbow pads could change the risk-taking behaviour of the athlete during training, which does not necessarily lead to a reduction in the incidence of injury and may even lead to other injuries.30
In 2006 Finch31 redesigned van Mechelen’s model by reviewing the efficacy step. She brought to notice the possible gap between the proposed interventions suggested by scientific research and their actual implementation due to “real-life” situations. The model presented in this paper complements the modifications proposed by Finch by incorporating risk-taking behaviour and compliance of the individual as limiting factors in sports injury prevention. It is constructed as a flow chart for clinical use, but is also applicable for policy makers and managers who are not directly involved in scientific research.
The proposed modification to van Mechelen’s model1 involves the insertion of an additional process between steps C and D which appraises the effectiveness of a preventive measure. Before implementing any preventive measure, the respective processes in relation to two dichotomous but related sides should be assessed. On one side are the stakeholders (eg, government agencies, sports federations, team manager, advertisers) for whom the efficiency of the prevention programme is of major concern, and on the other side is the employee (the athlete) whose compliance is of major importance. The modified model is shown in the flow chart in fig 2.

{kind=link}
{kind=link}
A method of prevention has to be efficacious (scientifically proven) before being evaluated by stakeholders in terms of its efficiency. The compliance of the individual and the control of a potentially modified behaviour are of equal importance. The effectiveness of prevention therefore depends on the efficacy, efficiency and compliance. The integration of all these processes provides a better insight into the effectiveness of a preventive programme before implementation, and will lead to a more successful outcome when implemented.
EFFICACY
The scientific efficacy of a preventive measure has to be proved before it can be considered for implementation by the stakeholders. Systematic reviews of interventions to prevent soft tissues injuries or stress fractures and stress reactions of the bones in the lower limb reveal the first limitation in the sequence, since there is no indisputable evidence of prevention efficacy.26 32–34 Hence, before the efficacy of a proposed intervention can be assessed, additional evidence must be obtained to enable a greater understanding of prevention of these conditions. However, the efficacy35 or inefficacy of protective equipment36 in specific sports has been shown more clearly, and it is by using studies of this nature that the efficacy of an intervention can be assessed.
EFFICIENCY
Once an efficacious technique has been identified for the prevention of an injury that exceeds the target level of risk, stakeholders can analyse the method with respect to the financial, practical and administrative implications and its potential impact on the improvement of the well-being of the athletes (eg, health, motivation). Introduction of preventive measures by stakeholders produces a number of benefits including fewer injuries leading to less distress of the athlete, fewer training hours lost, a higher level of readiness, lower medical costs and improved morale. However, investments have to be made for these to be achieved, including the production of guidelines or regulations for the application of the measure.37 It is reasonable to assume that, in some cases, the preventive measure could outweigh the problem or shift the limiting factor of injury to a different area (eg, the need to carry additional equipment which limits movement or reduces speed of movement).38 A target level of risk should therefore be determined above which a potential preventive measure should be assessed. The determined target level of risk will also be influenced by external factors such as internal regulations and national laws on safety and well-being, and priority levels in material and financial resources.39 The implementation of health and safety policy conforms to the maxim of intervention to achieve a target level “as low as reasonably practicable” which enables a balance between economic principles and reduction of injury risks to be determined. Injury risk must be reduced until a level is reached above which the costs and difficulties to take further action overcome the benefits. If muscle stretching or warming up was found to be efficacious in preventing lower limb injuries, the stakeholders would not be opposed to the implementation of this method during training routines.40–42 However, alternative techniques such as reducing training load,33 43 modifying equipment,44 45 adding braces46 47 and insoles39 48–50 require decisions to be carefully thought out owing to the financial and performance impact of their introduction.
COMPLIANCE AND RISK-TAKING BEHAVIOUR
The efficiency of a preventive measure will be assessed by the athlete’s counsellors and coaches, but its implementation will have consequences for the individual athlete so its success will depend on the compliance of the athlete with the preventive measure. He/she will internalise specific learning processes and experience with the introduction of a measure, and this learning process and experience will affect its adoption and success. Lund and Aarø51 identified four factors that are influenced by the modification of attitude, behaviour and structural conditions to prevent injuries. Those four factors can be divided into two categories of risk factors (behaviour and physical/organisational environment) and two process factors (attitude/beliefs and social norms/culture).
In effect, the growing awareness of injury risk and the beneficial effects of prevention should lead to a modified attitude. The “KAP” path (Knowledge → Attitude → Practice) appears to be weak:51 having the knowledge is not a guarantee to modification of the attitude and subsequent behaviour of the individual. Smoking is known to have a detrimental effect on health, yet individuals continue to smoke and it is not chastised by society as a whole.52 53 However, if knowledge about certain hazards was supplemented by information sources from appropriate media such as advertisements, safety centres or experience of colleagues and relatives, this could have a positive influence on the risk perception of the individual athlete. As a consequence of their personal evaluation, prescribed guidelines for prevention are followed (or not) and injuries avoided (or not).51 54 For example, if an individual has personally experienced the effects of a previous injury, he/she will be more likely to comply with and adopt the preventive measure, particularly if it is understood that the previous injury significantly predisposes to a repeat occurrence.55 Preventive measures for injury have the potential to be successful in a professional sport or in a military environment owing to the disciplined physical and organisational environment and the specific social norms and culture which will influence the behaviour of the sportsman/soldier. However, even studies in the military environment have shown that the presumed good compliance resulting from the strict organisational environment is not always correct.56 57 The most appropriate means of achieving behavioural modification is to integrate it into the athlete’s skills training rather than in a dictatorial fashion. This will implement the behaviour at an early stage in their career and reinforce the good behaviour by associating it with the skills learnt so that it becomes an accepted part of their routine.
What is already known on this topic
van Mechelen’s model has been widely used to conduct scientific research on sports injury prevention. This model takes only the efficacy of a method into account.
Finch extended this model by adding an important “real life” component to conduct research in this area.
Risk-taking behaviour is modified in individuals using “safe” equipment.
EFFECTIVENESS
The sum of the efficacy and the efficiency of a preventive measure, together with good compliance and controlled risk-taking behaviour of the individual athlete, results in the effectiveness of prevention of sports injuries. Looking at other methods of prevention rather than overuse and sports injuries, the compliance of the individual seems the most difficult factor to overcome.57 Preventive measures would become more effective if an efficient and encompassing method of gaining compliance by individuals across the required population was achieved. In addition, if a method of prevention could be introduced that does not rely on an individual’s behaviour modification, the effectiveness of the measure would be unaffected by their compliance. For example, modification of the standard military sock to one that reduces the incidence of foot blisters58 would be a more effective solution than requiring the individuals regularly to undertake their own foot care because the former does not require behavioural modifications and good compliance. Lund and Aarø51 found that injury prevention programmes implementing structural modifications such as regulations, enforcement methods, environmental and product modifications were more effective than behavioural modifications.
What this paper adds
We present a model that integrates the different aspects and processes that interfere with the effectiveness of a potential preventive measure in sports medicine.
Before implementing a preventive measure in sports medicine, all steps of this model should be considered.
APPLICATION OF THE MODEL
Patellofemoral pain syndrome (PFPS) is one of the most frequently encountered knee conditions in sports medicine practice.59 60 The establishment of the extent of this pathology has largely been undertaken in sports medicine and the military.61 Researchers agree on its multifactorial origin, with intrinsic and extrinsic risk factors being inherently linked to the onset of pain.61 Intrinsic factors such as shortened quadriceps muscle, altered onset of the vastus medialis obliquus muscle compared with the vastus lateralis, decreased explosive strength and a hypermobile patella have been shown to affect the onset of pain.62 Furthermore, measures of plantar pressure have been shown to be reliable in detecting risk factors.63 Alignment and anthropometric risk factors such as Q-angles, genua vara/valga body length and weight are controversial issues and their overall contribution to the onset of PFPS has yet to be fully determined, despite an apparent difference in the rates of PFPS between men and women.51 62 In understanding the risk factors of PFPS, it is important also to consider the extrinsic risk factors that contribute to its onset. Training errors, poor equipment, training surfaces and psychosocial variables have all been shown to be extrinsic risk factors for PFPS. Caution should be taken in extrapolating these studies across a general population. All prospective studies have been performed on physical education students or military recruits and are likely to be subject to the healthy worker effect.
The quadriceps muscle plays a key role in the pathology of PFPS. If a preventive measure for PFPS is suggested (step 3), it should be acting on as many modifiable risk factors as possible. Stretching has not been proved to be an efficacious method for preventing running injuries33 and would therefore not progress past step 4 in the model. In contrast, patellofemoral bracing has been shown to be an efficacious method for preventing PFPS in recruits.47 64 In van Mechelen’s model it would be categorised as effective in preventing PFPS. However, in applying our modified model to the proposed implementation of this preventive measure, it is evident that the efficacy and compliance of its introduction would be assessed poorly and would therefore not progress past steps 5 and 6. A thorough identification of the individual at risk is therefore needed (efficiency), demonstrating the importance of a clearly defined population when assessing and implementing preventive measures. For example, a young female recruit with poor quadriceps muscle function, hypermobile patellae and supinated feet would have a profile for this method to be efficient. In order to be categorised as an effective preventive method for this individual, we have to assume that the young female recruit will be compliant with the method and that she would not modify her behaviour by unnecessary training. This step is crucial and could be considered as the weakest link in the prevention strategy.
CONCLUSION
An extension of van Mechelen’s model of “the sequence of prevention”11 is presented which examines the efficacy of sports injury prevention programmes. To implement an effective measure for the prevention of overuse injuries, the model has been modified to consider also the efficiency, compliance level and risk-taking behaviour of the individual. By using the modified model, the outcome and bottlenecks of an intervention to prevent overuse injuries can be better predicted. As a result, the financial implications of any preventive measure can be better modelled to determine the likelihood that it will produce a successful outcome and therefore provide a more balanced assessment of the cost benefit of its introduction. van Mechelen’s model assumes that a proposed preventive measure will be endorsed by stakeholders and athletes alike. In reality, external pressures and individual interpretations have a significant impact on the uptake of a measure, and it is by understanding these that an accurate evaluation of the implementation of a preventive measure can be assessed.
REFERENCES
Footnotes
Competing interests: None.