Article Text

Abstract
Background: Atrial function is an integral part of cardiac function that is often neglected. The presence of left ventricule hypertrophy (LVH) due to arterial hypertension may impair atrial function. However, it has also been suggested that physical training attenuates the age-associated impairment of diastolic filling. This study investigated whether mechanical dysfunction in the left atrium (LA) is present in patients with either physiological or pathological LVH, using two-dimensional strain rate imaging (2D strain echocardiography; 2DSE).
Methods: Standard echocardiography, exercise stress echo and 2DSE of the left atrium were performed in 40 patients with arterial hypertension, 45 age-matched elite athletes (>40 years) and 25 healthy sedentary controls. Atrial longitudinal strain was performed from the apical views for the basal segments of the LA septum, lateral wall and roof.
Results: LV mass index and ejection fraction were comparable between patients with either physiological or pathological LVH. Elite athletes showed increased LV end-diastolic diameter, end-diastolic volume and stroke volume, whereas circumferential end-systolic stress was higher in patients with hypertension. LA diameter and maximum volume were increased but similar between the two groups of patients with LVH. LA active emptying volume and fraction were both higher in patients with hypertension. Conversely, peak systolic myocardial atrial strain was significantly reduced in patients with pathological LVH compared with controls and athletes for all the analysed atrial segments (p<0.0001). Using multivariate analysis, LV end-diastolic volume/body surface area (BSA) (β coefficient 0.52; p<0.0001) and LV mass (β = 0.48; p<0.001) in athletes emerged as the only independent determinants of LA lateral wall peak systolic strain. In contrast, in patients with hypertension, an independent negative association of LA lateral wall peak systolic strain with both LV mass (β = −0.42; p<0.001) and circumferential end-systolic stress (β = −0.43; p<0.001) was found. In addition, in the overall population of patients with LVH, LA lateral wall systolic strain (β = 0.49; p<0.0001) was a powerful independent predictor of maximum workload during exercise testing.
Conclusions: 2DSE represents a promising, non-invasive, simple and reproducible technique to assess LA myocardial function in patients with either physiological or pathological LVH. LA myocardial deformation is impaired in patients with hypertension compared with age-matched sedentary controls and elite athletes, and is closely associated with functional capacity during effort.
Statistics from Altmetric.com
Haemodynamic overload due to long-term training usually involves both left and right ventricles, inducing changes in cardiac structure as increase of internal cavity diameters, wall thickness and mass.1–4 In competitive athletes, left ventricular hypertrophy (LVH) often mimics pathological conditions (arterial hypertension or hypertrophic cardiomyopathy).5 6 In particular, athletes who engage in rigorous strength training may exhibit a concentric cardiac hypertrophy pattern similar to that of hypertensive hypertrophy.4 7 However, athletic hypertrophy is thought to be a benign, physiological response without the prognostic significance of hypertensive hypertrophy. Although standard Doppler echocardiography has been widely used to distinguish athlete’s heart syndrome from pathological LVH, conflicting data have been reported about the nature (physiological versus pathological) of LVH in elite athletes and veterans.8 9
Atrial function is an integral part of cardiac function that is often neglected. The presence of LVH due to arterial hypertension may impair atrial function.10 Recognition of the upper limits of atrial size and function in competitive athletes may be of clinical relevance by assisting in distinguishing cardiac remodelling in athletes from structural heart disease.11
Of the various echocardiographic techniques currently available, Doppler myocardial imaging (DMI) and Doppler strain rate imaging have gained acceptance because of their ability to define myocardial timing, contractility and deformation in patients with LVH, and are easy to perform and repeat.12–14 Previous studies have reported the usefulness of DMI to identify the influence of training on LV myocardial function, the relationship between DMI parameters at rest and cardiac performance during effort,15–20 and the differences in LV myocardial function in various types of LVH.21–25 However, both DMI and Doppler strain imaging are limited by the Doppler angle of incidence. A novel approach to quantify regional LV function from routine grey-scale two-dimensional echocardiographic images, known as speckle-tracking two-dimensional strain echocardiography (2DSE), calculates myocardial strain independent of angle of incidence, and has been recently validated against sonomicrometry and tagged magnetic resonance imaging.26–28 To date, no previous report has analysed myocardial function in the left atrium (LA) in elite competitive athletes with this technique.
Thus, the aims of this were to detect, using 2DSE, LA myocardial function in patients with either physiological or pathological LVH, and to investigate a possible correlation between LA myocardial function and exercise capacity during an exercise stress test.
METHODS
The study was approved by the institutional ethics committe, and informed consent was obtained from the participants.
Study population
In total, 110 participants (all male) were enrolled into the study: 40 patients with LVH secondary to newly diagnosed arterial hypertension, 45 strength-training elite athletes with concentric LVH, and 25 healthy sedentary control subjects.
Hypertensive patients
This group comprised 40 male patients with newly diagnosed essential hypertension. A SpaceLabs monitor (model 90207; SpaceLabs Inc., Redmond, Washington, USA) weighing 340 g (including batteries) was used for 24-hour ambulatory blood pressure (ABP) monitoring to diagnose hypertension. To ensure a new diagnosis, patients were excluded if they had had any diagnosis of hypertension or had used any drugs to treat hypertension before the ABP. The upper limits of “normality” for average ABP values in our study were <135/85 mmHg during the day, <120/75 mmHg during the night and <130/80 mmHg over 24 hours. Other inclusion criteria were: (1) age 40–55 years; (2) exercise stress echocardiography results negative for ischaemia; and (3) LV mass index (LVMI) >50 g/m2.7 according to the Cornell criteria.29 Exclusion criteria were coronary artery disease, valvular and congenital heart disease, congestive heart failure, cardiomyopathies, diabetes mellitus, ejection fraction >55% by echocardiography, and echocardiograms of inadequate quality.
Elite power athletes
The athletes group comprised 45 strength-trained elite competitive athletes (ATS) (short-distance swimmers), all having evidence of LVH by echocardiography. We defined a competitive elite athlete as one aged >40 years who participates in an organised team or individual sport in which regular competition is a component. All the subjects had been training intensively for 15–20 hours/week for >7 years. ATS underwent anaerobic isometric static exercise at incremental workloads at 40–60% of maximum heart rate. In particular, their training protocol included both 3 hours/day of short-distance swimming (3000 metres/day divided into series of 25–50–100 metres) and 1 hour/day of weight-lifting at high workload.
Exclusion criteria for athletes were as for the hypertensive group with the addition of past clinical diagnosis of hypertension.
Sedentary healthy controls
We also studied 25 age-matched sedentary subjects without detectable cardiovascular risk factors. These were all recruited in Naples, were selected from our cardiology department from subjects investigated for work eligibility, and were examined in a single centre (Monaldi Hospital, Naples).
Standard echocardiography
Standard Doppler echocardiography and 2DSE were performed with the subjects partially recumbent on their left side. All the measurements were analysed by two experienced readers, taking an average of ⩾3 cardiac cycles. LV mass was calculated by the Penn convention, and indexed for height2.7 (Cornell adjustment).29 Heart rate (HR) was measured from ECG tracings. Stroke volume was calculated by the LV outflow Doppler method as the product between outflow tract area and LV output time–velocity integral.30 Tricuspid annular plane systolic excursion (TAPSE) was calculated as the index of right ventricular global systolic function multiplied by the difference between end-diastolic and end-systolic measurement (mm).31 Circumferential end-systolic stress (ESSc) was calculated as a measurement of LV afterload using a cylindrical model according to the following formula:
ESSc (g/cm2) = SBP x ½ Ds2 {1+[(½ Ds+Ps)2/(½ Ds+½ Ps)2]}/(½ Ds+Ps )2−½ Ds2,
where SBP is systolic BP, Ds is end-systolic diameter and Ps is posterior wall thickness in systole.32
LA volumes were calculated using the biplane area-length method as follows: LA volume = 8× (LA area in four-chamber view)×(LA area in two-chamber view)/3Π (LA length). Left atrial length was defined as the longest line that could be drawn between the posterior LA wall and the midportion of the mitral valve, and was similar in the four-chamber and two-chamber views, which are perpendicular to each other. LA maximum volume was measured at the point of mitral valve opening, and LA minimal volume was measured at the point of mitral valve closure. LA volume at onset of atrial systole was considered the volume corresponding to the onset of the P wave in the simultaneously recorded ECG. All LA volume values were corrected for BSA. Left atrial systolic (active emptying) function was assessed using (1) LA active emptying volume = LA volume at onset of atrial systole − LA minimal volume and (2) LA active emptying fraction = LA active emptying volume/LA volume at onset of atrial systole.33 34
Two-dimensional echocardiographic atrial strain
The 2DSE method uses grey scale (B-mode) sector image and is based on frame-by-frame tracking of small rectangular image blocks with a stable speckle pattern. A minimum frame rate of 30 Hz was required for reliable operation of this program, and frame rates of 30 to 90 Hz were used for routine grey-scale imaging.26 Apical four-chamber views were obtained using the same ultrasound system and probe used for standard echocardiography; end systole was chosen as the single frame for the endocardial to epicardial region of interest to include maximumwall thickness for strain calculation. The “Zoom/RES” feature on the echocardiographic machine was used to improve the accuracy of atrial measurements. A circular region of interest was traced on the endocardial cavity interface of the apical four-chamber view at LA systole (minimum cavity area) using a point-and-click approach. A second larger concentric circle was then automatically generated, which was near the epicardium, with a default width of 15 mm. The region of interest thus included the entire LA myocardial wall, and a click feature increased or decreased the width of the two circles for thicker or thinner walls respectively. The tracking algorithm followed the endocardium from this single frame throughout the cardiac cycle. The image-processing algorithm automatically subdivided the region of interest into blocks of approximately 20–40 pixels containing stable patterns of speckles. Subsequent frames were then analysed automatically by searching for the new location of each of the blocks with correlation criteria and the sum of the absolute differences. The location shift of these acoustic markers from frame to frame, which represents tissue movement, provides the spatial and temporal data used to calculate velocity vectors. Temporal alterations in this stable speckle patterns are identified as moving further apart or closer together, and a series of regional strain vectors are calculated as change in length/initial length. The tracking process and conversion to Lagrangian strains was performed offline using dedicated software (EchoPAQ PC 2D strain, GE Healthcare, Milwaukee, USA).26
The software then automatically divided the image into six standard segments and provided an automated tracking score, similar to standard deviation, as feedback of the stability of the regional speckle tracking, ranging from 1.0 to 3.0 in arbitrary units. A tracking score value of <2.5 was considered acceptable as previously described, and slight adjustments were made to the placement of the region of interest in regions with greater SDs in an attempt to improve tracking stability.
Analysis was performed for atrial longitudinal strain from the apical views for the basal segments of the LA septum, lateral wall, and roof. Atrial radial strain was not calculated from the parasternal short and long axis views because the atrial wall is too thin to be properly analysed in these views, as we had found in our previous pilot studies. Continuous care was taken to keep the sample volume out of the pulmonary veins and the oval fossa.
Exercise stress echocardiography
All patients enrolled in the study underwent a supine bicycle exercise stress echocardiography test after the resting echocardiogram. The test was analysed by cardiologists blinded to the study. Participants were enrolled into the study if they had negative results for myocardial ischaemia. The following functional indexes were assessed at peak effort: maximum HR, maximum systolic blood pressure (SBP), maximum workload (number of watts generated in a supine bicycle test) and rate–pressure product (maximum HR×maximum SBP).35
Statistical methods
All analyses were performed using a commercially available software package (SPSS V.11.0 2002, SPSS Inc., Chicago, Illinois, USA). Analysis of variance (ANOVA) using Newman–Keuls post hoc test for multiple comparisons, and Student t test for unpaired data were performed to estimate differences between groups. Variables are presented as mean (SD). Linear regression analyses and partial correlation test by either the Spearman or Pearson method were performed to assess univariate relations.
To identify significant independent determinants of LA myocardial strain in patients with LVH, their individual association with clinical relevant and echocardiographic variables was assessed by multivariable Cox regression analysis.36 The following variables were included into the analysis: clinical data (age, blood pressure, BSA, aetiology of LVH), standard echocardiographical indexes (LV volumes, LA volumes, LV mass, Doppler transmitral inflow measurements and circumferential end-systolic stress (ESSc)). These variables were selected according to their clinical relevance and potential effect on LA function, as shown by previous studies.10 Variable selection was performed using multivariable Cox regression as an interactive stepwise backward elimination method, each time excluding the variable with the highest p value according to Wald statistics. The assumption of linearity was checked graphically by studying the smoothened martingale residuals from the null model plotted against the covariate variables. The linearity assumptions were satisfied. The Hosmer–Lemeshow goodness of fit test was used to check that the model adequately fitted the data. To reduce the inflation of the type 1 error rate due to multiple testing, tsignificance was defined as p<0.01 (two-sided).
Reproducibility of 2DSE measurements was determined in all the subjects. Interobserver and intra-observer variability was examined using both the Pearson bivariate two-tailed correlations and Bland–Altman analysis. Relationship coefficients, 95% CI and percentage errors were calculated.
RESULTS
Clinical characteristics of the study population
The characteristics of the study population are shown in table 1. The three groups were matched for age. In accordance with the effects of training, heart rate in athletes was lower than in controls. Conversely, both systolic and diastolic blood pressure were higher in patients with hypertension.
Supine bicycle stress test
During physical effort (supine bicycle stress test; table 2), ATS showed a better functional capacity, as expected, with greater maximum workload achieved with lower maximum HR and maximum systolic blood pressure.
Ventricular standard Doppler echocardiographic analysis
LV ejection fraction and TAPSE were comparable among the three groups (table 3). The elite athletes showed increased LV end-diastolic diameter, LV end-diastolic volume/BSA and LV stroke volume, whereas relative wall thickness and circumferential end-systolic stress were higher in patients with hypertension. Transmitral Doppler indexes were all better in athletes.
Left atrial morphology and function
LA diameter and maximum volume were increased but similar between the two groups of patients with LVH (table 4). Conversely, LA active emptying volume and fraction were both higher in patients with hypertension compared with both controls and athletes.
Overall, speckle tracking was possible in 95.5% of 330 attempted segments from the 110 subjects with technically adequate images, with only 3.5% of segments with tracking variation scores >2.5 eliminated. Overall tracking variation scores were <2.0 in 77%. of segments.
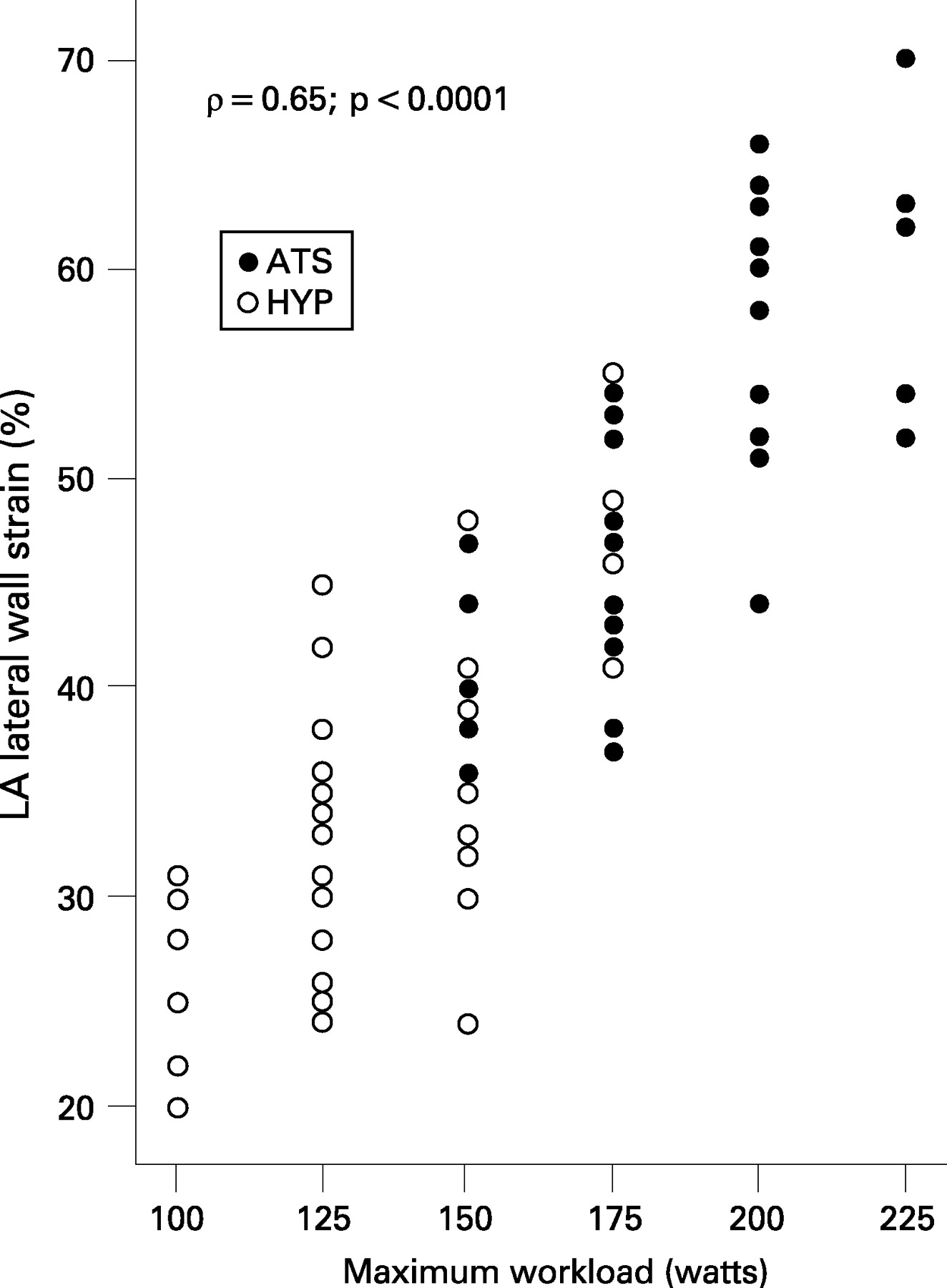
Peak systolic myocardial atrial strain was significantly reduced in patients with pathological LVH compared with controls and athletes for all the analysed atrial segments (fig 1). In addition, a close association was observed between LA strain in the lateral wall and maximum workload during exercise testing (ρ = 0.65; p<0.0001) (fig 2).


By multivariable analysis, after adjusting for potential determinants such as age, HR, BSA, LV and LA volumes, LV end-diastolic volume/BSA (β coefficient in the final model 0.52; p<0.0001; β coefficient estimate averaged across bootstrap samples 0.51; p<0.0001) and LV mass (β coefficient in the final model 0.48; p<0.001; β coefficient estimate averaged across bootstrap samples 0.47; p<0.001) emerged as the only independent determinants of LA lateral wall peak systolic strain in athletes. In contrast, in patients with hypertension, independent negative associations of LA lateral wall peak systolic strain with both LV mass (β coefficient in the final model −0.42; p<0.001; β coefficient estimate averaged across bootstrap samples −0.41; p<0.001) and circumferential end-systolic stress (β coefficient in the final model −0.43; p<0.001; β coefficient estimate averaged across bootstrap samples −0.44; p<0.001) were found.
In addition, in the overall population of patients with LVH, LA lateral wall systolic strain (β coefficient in the final model 0.49; p<0.0001; β coefficient estimate averaged across bootstrap samples 0.47; p<0.0001) was a powerful independent predictor of maximum workload during exercise testing (fig 3).

{kind=link}
{kind=link}
{kind=link}
Reproducibility of left atrium strain as measured by two-dimensional strain echocardiography
Intra-observer variability
For intra-observer variation, Pearson correlations were r = 0.86 (p<0.00001); r = 0.87 (p<0.00001); and r = 0.84 (p<0.00001) for lateral wall, atrial septum and atrial roof, respectively. Bland–Altman analysis gave 95% CI (percentage error) of ±1.7 (3.3%); ±1.1 (3.1%); and ±1.5 (3.2%), respectively.
Inter-observer variability
For intra-observer variation, Pearson correlations were r = 0.84 (p<0.00001); r = 0.85 (p<0.00001); and r = 0.83 (p<0.00001) for lateral wall, atrial septum and atrial roof, respectively. Bland–Altman analysis gave 95% CI (percentage error) of ± 1.6 (3.4%); ±1.4 (3.5%); and ±1.6 (3.2%), respectively.
DISCUSSION
The results of the present study demonstrate the usefulness of 2DSE in analysing LA myocardial function in patients with either physiological or pathological LVH.
The advantages and perspectives of two-dimensional strain echocardiography in the study of la function in left ventricular hypertrophy
Previous reports by our group and others have already noted that echocardiography, with its newer applications such as DMI and strain imaging, may be a useful technique to evaluate LV myocardial function in patients with LVH.12 13 15–25 In particular, the strain rate analysis of athletes’ LV myocardial function has recently confirmed that, despite the signs of combined concentric and eccentric LVH, both systolic and diastolic functions remains normal or even “supernormal” in endurance athletes. In the paper by Claessens et al, the significant differences between athletes and controls for the Doppler strain values of both basal and middle septum in the longitudinal axis, and the end-diastolic strain at the end of the A-wave were particularly striking.24 In contrast, in a very recent study by Saghir et al, patients with hypertensive LVH showed significant longitudinal Doppler strain and strain rate reductions in the interventricular septum compared with both controls and power athletes.25
To our knowledge, the current study is the first to analyse LA function in patients with both physiological and pathological LVH, using speckle–tracking 2DSE.
In our previous articles we reported for the first time the feasibility of Doppler strain in analysing myocardial deformation properties of both atria.37 38 However, in patients with LVH and dilated atria, Doppler strain estimation, because of its angle dependency, presents an important limitation due to poor alignment between the Doppler beam and the LA myocardial walls.14 Thus, in the current study we used 2DSE, a novel approach to quantify regional myocardial deformation within a scan plane that is inherently two-dimensional and independent of interrogation angle as it tracks speckle patterns (acoustic markers) within serial B-mode sector scans.26
Left atrium function in pathological left ventricular hypertrophy
Normal LA function consists of three components. The LA is: (1) a contractile chamber (booster pump) that actively empties immediately before the end of LV diastole and establishes final LV end-diastolic volume; (2) a reservoir that stores pulmonary venous return during LV systole and isovolumic relaxation after the closure and before the opening of the mitral valve; and (3) a conduit that empties its contents into the LV down a pressure gradient after the mitral valve opens and during LV diastole.10
In subjects with normal diastolic function, the relative contribution of the reservoir, conduit and contractile functions of the LA to the filling of the LV are approximately 40%, 35% and 25%, respectively. However, the LA is exposed during ventricular diastole to the pressures of the LV. In patients with hypertension, with increased stiffness or noncompliance of the LV, LA pressure rises to maintain adequate LV filling, and the increased atrial wall tension leads to chamber dilatation and stretch of the atrial myocardium. As a result, early in hypertensive heart disease, LA pump function is augmented but LA stiffness increases and work mismatch occurs.
Several authors have recently shown that LA peak systolic myocardial atrial strain, which is LA passive stretching during LV systole, could be used as an index of LA reservoir function.39–42 In our study protocol, in patients with pathological LVH, indexes of LA booster pump function (LA active emptying fraction) were increased, whereas LA passive deformation (peak systolic myocardial atrial strain) was significantly impaired compared with both controls and elite athletes in all the analysed atrial segments. In addition, the results indicated in patients with hypertension a close negative relationship of LA function with both LV mass and LV ESSc, the latter representing a reliable marker of LV increased afterload. This association emphasises the effect of chronic pressure overload on LA myocardial function in pathological LVH.43 Such LA myocardial dysfunction, known as “stiff LA syndrome”, may cause a reduction in LA compliance, a marked increase in LA and pulmonary pressures, and a progressive impairment in exercise capacity, as clearly seen in our study population by the direct correlation between LA systolic strain and maximum effort workload during exercise echocardiography.
Left atrial function in physiological left ventricular hypertrophy
LA enlargement in trained athletes has been regarded as a physiological and benign adaptation to exercise conditioning and another component of the “athlete’s heart.” In particular, Pelliccia et al showed that enlarged LA size (⩾40 mm) is relatively common and was present in 20% of a large cohort of competitive athletes (1.777 subjects); marked dilatation (⩾45 mm) was found in 2% of athletes. In addition, multivariate regression analysis showed that LA enlargement occurred in close association with LV cavity enlargement, and that this morphological change was minimally related to body size and largely dependent on the type of sport participated in by the athlete.11
In our population of elite athletes undergoing long-term power training, the chronic increase of LV afterload during isometric activity determined development of physiological concentric LV hypertrophy, with normal global systolic and diastolic LV function, and parallel increase in both LA volume and myocardial deformation. These findings are in accordance with the reported effects of static anaerobic exercise, which is characterised by prolonged isometric contraction of single muscle fibres, with rapid increase of local metabolic requests without proportional increase of blood perfusion.1–4 In addition, in our athletes, enhanced LA myocardial deformation was closely associated with LV end-diastolic volume and LV mass, and was an independent determinant of maximum exercise capacity during stress test. Our observations confirm, therefore, that both LA and LV cavity remodelling observed in elite athletes represent the physiological consequence of a global cardiac adaptation to the increased workload associated with intensive and chronic exercise training.
Study limitations
Our study has several limitations. In our protocol we selected a population of elite power athletes and relatively young patients, all men, with a first diagnosis of arterial hypertension, to avoid potential effects of pharmacological therapy and significant differences in ages of the athletic, control and hypertensive groups. Consequently, it had insufficient numbers to discern the LA strain profile of the young athlete or of the older patient with hypertension. In nonhypertrophied hearts, a previous study found a linear decay in LV strain rate with a positive movement of 0.004/second/per year of age.44 Further research is therefore needed to determine whether LA strain rate decays in a linear fashion in the hypertrophied heart.
A technical limitation is that speckle-tracking echocardiography is dependent on frame rate as well as image resolution.26 A low frame rate results in the speckle pattern changing too much from frame to frame, which prevents the precise characterisation of regional myocardial motion and affects the overall temporal resolution of the regional strain map. In contrast, increasing the frame rate reduces scan line density, which in turn reduces image resolution. The frame rate in our study ranged from 35 to 90 frames/second. This value is lower than frame rate available with Doppler strain imaging; however indexes of LA function used in this study did not rely on difference in the timing of contraction. In our study, radial atrial strain was not calculated from the parasternal short-axis and long-axis views because the atrial wall is too thin to be properly analysed in these views, as found in our previous studies.37 38
Conclusions
This study showss for the first time that a novel speckle-tracking algorithm applied to routine grey-scale two-dimensional images represents a promising, non-invasive, simple and reproducible technique to assess LA atrial myocardial function in patients with either physiological or pathological LVH. Left atrial myocardial deformation is impaired in patients with hypertension compared with age-matched sedentary controls and elite athletes, and is closely associated with functional capacity during effort. As LA enlargement has been proposed as a proxy of diastolic burden and a predictor of common cardiovascular outcomes,10 future longitudinal studies are warranted to further our understanding of the natural history of LA myocardial function in LVH, the extent of reversibility of LA dysfunction with medical treatment, and the potential effects of various types of exercise training on LA deformation.
REFERENCES
Footnotes
Competing interests: None declared.