Article Text

Abstract
The built environment and physical activity agenda provides a unique opportunity for public health, physical activity and planning researchers to be front and centre of a movement aimed at creating healthier and more sustainable environments. However, in order to optimise environments that encourage physical activity across the life course, researchers in this field need to think beyond their “square” —that is, the target group, setting and physical activity behaviour with which they work. We suggest that researchers working in this field need a better understanding of systems theory to appreciate that a change to one part of a complex system can positively and negatively influence other parts of the system. An understanding of systems theory would help minimise unintended negative consequences to other population subgroups or to other types of physical activity from the implementation of our research findings. In this way, a more comprehensive set of research, practice and programme-related activities may emerge, which will advance physical activity research and practice, and improve population health across the life course.
Statistics from Altmetric.com
There is growing recognition that the way cities are built can profoundly affect health and health-behaviour outcomes,1 as well as transportation patterns.2 Sprawling patterns of uniform, low-density, car-orientated land development typical of metropolitan housing developments in Australia, the USA and other industrialised countries discourage walking, cycling and public transit use and increase motor vehicle dependency.3 4 This design not only produces poor environmental outcomes (eg, increased greenhouse gas emissions and poor air quality), but also detrimentally affects human health by reducing transport-related physical activity and increasing sedentary behaviour, excess weight and obesity, respiratory problems due to poor air quality,4 5 the likelihood of vehicular crashes with increasing vehicle miles travelled, and stress associated with longer commuting times.1
The idea that planning and public health are linked is hardly new.6 7 Public-health concerns were the driving force behind 19th-century urban reform in the UK and the USA.1 The provision of public open spaces,8 the construction of urban water supply and sewerage systems, and the introduction of tenement housing reforms7 all aimed to improve the health and quality of life of the working classes living in squalid, crowded and polluted inner cities. A major goal of the separation of land uses and later, the introduction of zoning, was to reduce human exposure to noxious industrial pollution.7 In some areas, the introduction of minimum lot sizes aimed to reduce the potential for spread of communicable diseases and avoid ground-water contamination.9 The introduction of public-transport systems revolutionised cities, allowing workers to live in suburban areas and commute to work and other essential services.1 Mass production and distribution of motor vehicles offered residents mobility and independence, allowing people to live even further away from employment centres and this further encouraged suburbanisation. Who could have envisaged that, together, these early planning decisions, combined with post-World War II private-sector imperatives to achieve the primacy of car travel, would have contributed to 21st-century problems associated with suburban sprawl? If we reflect upon the decision making of policy-makers at the time, the reasons were both important and valid. Many decisions were made with a genuine concern to protect the public’s health, to improve living conditions, and to maximise the population’s mobility. However, the unintended consequence of trying to reduce infectious diseases in the 20th century and maximise population mobility has spawned environmental and chronic health problems in the 21st century, the full effect of which we are yet to see in an energy-deficient global economy.
As solutions are sought, the fields of public health, clinical care, planning and transportation are uniquely placed to work together to reshape the way cities and neighbourhoods are built and rebuilt in the future. However, a key question in tackling present-day built environment challenges is how to avoid unintended consequences that detrimentally affect the health of the community. In an ever-changing world, it may not be possible to anticipate every negative effect. However, the goal of this paper is to discuss systems theory with the aim of encouraging interdisciplinary teams working together to think through built form policy reforms with the aim of avoiding unintended consequences to health and other aspects of daily life.
INCREASING PHYSICAL ACTIVITY BY CREATING MORE WALKABLE NEIGHBOURHOODS: IS THIS THE SOLUTION?
There is now growing and consistent cross-sectional evidence that among general adult populations, walking for transport is facilitated by living in higher-density areas with more mixed use and connected street networks.10 11 Thus, it is tempting to simply recommend returning to higher-density developments with mixed use planning and access to transit. However, perhaps before doing so, we should be mindful of the Latin precautionary dictum primum non nocere – first, do no harm – by exploring more fully the consequences of such a recommendation and thinking through the avoidance of any negative consequences.
For example, research on the relationship between the built environment and physical activity to date has predominantly been undertaken with working-age adults, rather than with children and older adults. As we proceed towards recommending policy reform, are we confident that the evidence gathered to date holds true for all people or population segments, or will there be subtleties that need to be considered? As shown in figure 1, there are many population segments that will be affected by changes to the built form and their needs must be accommodated.

The general utility of walking for transport notwithstanding, it is likely that engaging regularly in more than one type of physical activity behaviour is necessary for many people to achieve and maintain the optimum levels of physical activity recommended for health.12 Undoubtedly, the best available evidence on the effect of the built form on physical activity concerns walking for transport. However, this is only one – albeit important - physical activity behaviour. There are many other physical activity behaviours that provide a range of alternative benefits, such as walking for recreation, team sport participation, active play, and cycling (fig 1). The full range of behaviours may or may not be facilitated by simply providing highly pedestrianised urban neighbourhoods.11 13 14 In fact, unless sufficient attention is given to creating supportive built environments, many other physical activity behaviours (eg, active play and team sport) may be actively discouraged. Insufficient attention to planning for these behaviours may produce unintended negative consequences. For example, what might be the effect on the development and social behaviours of children and young people or on the level of anti-social behaviour if highly urbanised environments are built without providing interesting, convenient, safe and varied opportunities to meet the recreational needs of the population?
Other unintended consequences also may be produced. For example, there is considerable evidence that noise increases stress, and detrimentally influences mental health,15 while nature deprivation may increase aggression, mental fatigue and stress.16 How could these potential negative effects be ameliorated? Even if we do not know the answer, we need to be cognizant of potential negative effects, and place greater attention on how densely populated cities are built (eg, such as building construction that reduces noise transfer and exposure to traffic) and the need for access to high-quality public open space.15
Encouraging the community to be active in as many ways as possible across the life course17 will require consideration of multiple settings (eg, home, school, community, clinical care, recreational) supportive of multiple domains of physical activity. For example, schools can be supportive of organised physical activity through formal physical education, sports and/or fitness programmes during and after school, active play during lunch-time and break, active transport to and from school, and additional physical activity throughout the day through classroom activities. In addition, by having a concept of schools from a broader community perspective, it is possible that with appropriate planning, design, and policy reform, the school grounds and facilities could be used to encourage other members of the community to be physically active during out-of-school hours and in the summer months. For example, school sports grounds can (and often are) used by community sporting groups for team sport after school and on weekends or for independent active play by children. Similarly, with the addition of landscaping, perimeter walking paths and seating, the school grounds could become a safe environment for walks by older adults. The school is also a workplace for teaching and administrative staff, and thus the potential for encouraging their physical activity may prove beneficial for both the workers and the students whom they teach.
Accumulating evidence suggests that the built environment alone may be “necessary but not sufficient” to promote physical activity, given that many factors influence behaviour. The built environment is now consistently being shown to contribute important, but modest amounts of the variance in physical activity behaviour.18 19 Thus to optimise levels of physical activity across the life-course, it is likely that in addition to creating supportive environments, there will be a continuing need for target-group and setting-specific programmes and policies (fig 1). The health sector can advocate for, facilitate, support and enhance these activities by forming partnerships with sectors outside of health (eg, school, transport, recreational) that are responsible for their adoption and implementation.
USING A SYSTEMS THEORY APPROACH TO OPTIMISE PHYSICAL ACTIVITY ACROSS THE LIFE COURSE
Making advances toward active lifestyles across the life course will probably require extending the use of ecological models. Currently these models have been used largely to conceptualise and study correlates of behaviour.20 However, as the evidence mounts and recommendations are formed, a broader application of systems theory will help the field to think through the consequences of their recommendations. Systems theory provides a framework for considering people, places, physical activities, programmes and policies in combination rather than in isolation.
SYSTEMS THEORY AND ITS APPLICATION
Ecological models used in physical activity research20 are based on general systems theory, which is used by a wide range of disciplines (social sciences, natural sciences and engineering) to study “the interaction of individual components within a complex whole”.21 Like all other organisms, human beings are part of a “system of dynamic interdependencies” and are constantly adjusting to changes in the external environment.22
By definition, a system, whether biological or social, is composed of two or more inter-related parts that are ever-changing and interacting in a complex manner.23 Viewed broadly, numerous social systems (eg, government, education, health, industry, law and welfare) and built environments (eg, community, school, workplace, home) effect human existence at the local, regional and macroenvironmental levels.24 25 A change to one part of the system can positively or negatively influence other parts of the system. Human survival depends on our ability to adapt to the complex interactions with and between the social and built environments.22
Newell et al26 recommend taking a systems approach to think through the consequences of decision-making or policies.26 At the simplest level, this involves interdisciplinary teams working together to identify variables that may be relevant to a problem, and grouping these into three categories: systems variables, external “drivers” of the system and those irrelevant to the problem. These are then used to construct “influence diagrams” that consider the likely influence and links between variables and possible feedback loops.
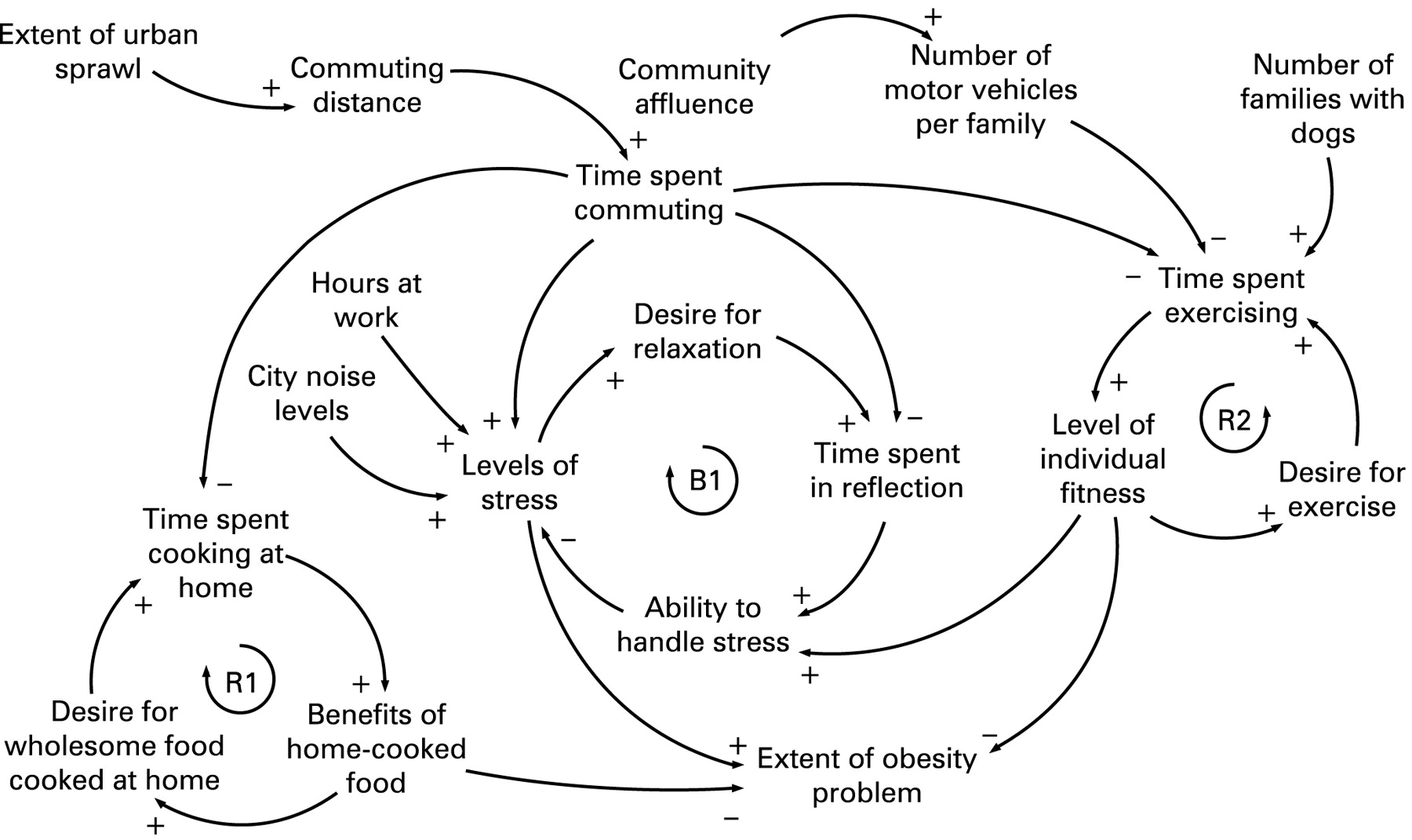
For example, figure 2 shows a simplified diagram of the human–urban system that produces obesity developed by Newell et al.26 As shown, complex systems have a large number of “parts” that interact with, influence and constrain one another via a network of feedback loops,26 and each part of the system can produce positive and negative effects. In this simplified example, three driving variables are considered: urban sprawl, community, and the number of families with dogs. These driving variables affect each other and also affect other variables in the system, which in turn produces positive and negative outcomes. Unintended negative consequences of a changing system often go undetected as the overall system continues to fulfil its various functions. It is only over time that it is recognised that the system has irreversibly changed. Although it may seem implausible that unworkable or suboptimal parts of the system may at first go undetected, this is because complex systems rely on a sharing of parts,24 and other parts of the system continue to operate. For example, although local streets are used for walking, as a conduit for social interaction and, when landscaped, to create restorative space that can beautify neighbourhoods, their primary function in contemporary society is for motor-vehicle transport.27 Thus, in neighbourhoods designed with disconnected street networks without sidewalks, the potential effect on the community of children not being able to walk to school or a reduction in some forms of social interaction may be delayed or may go undetected for some time because the roads still function as conveyors of motor vehicles. Individuals adapt by using their motor vehicles for transport rather than walking. It is often only much later that society recognises the negative health and social consequences of creating disconnected, car-dependent local communities with child-free streets.
Two key principles of the systems approach described by Newell et al26 are that: (1) a human–urban system cannot be optimised by seeking to optimise the behaviour of one part of the system in isolation from another; and (2) the design of effective policies requires an “integrative approach” that crosses existing professional, institutional and disciplinary boundaries. Thus, increasing physical activity across the life course requires us to go beyond thinking of one particular target group and to work in interdisciplinary teams. We describe the application of a systems theory approach to facilitate this process.
THE APPLICATION OF SYSTEMS THEORY
Many years ago, management consultants training people in creative problem-solving used a mental exercise that involved nine dots in a square. The task involved joining all nine dots by only using four straight lines. The task could only be successfully completed by extending one line well beyond the edge of the square made up by the dots. From this exercise, the notion of “thinking outside the square (or box)” was born. For example, typically in physical activity research, we work with one population group, one physical activity and/or one setting. A systems theory approach helps us to think outside “our” square and, in so doing, facilitates identification of both intended and unintended consequences to the system that may result should policy and practice change occur as a consequence of our professional activities.
As supported in systems theory, the concepts presented in fig 1 could be used by scientists and practitioners interested in changing the built environment to increase physical activity to identify at which nexus (ie, “square”) of the different domains (ie, types of physical activities, places, people, etc.) they tend to work. A goal would then be to have a larger effect by exploring ways to going beyond their “square” in broadening their research recommendations or programme-based targets and goals. For instance, healthcare providers and organisations could explore ways to actively partner with physical-activity organisations in the community through formal referral activities and similar ongoing linkages. Healthcare clinics could also continue to evaluate methods for using the clinical care setting in delivering physical activity messages through, for example, providing physical activity skill building and other health promotion information using office-based, state-of-the-art technologies (eg, interactive computerised kiosks stationed in clinic waiting rooms). Finally, through providing print-based physical activity information that also includes potential neighbourhood influences on physical activity patterns, doctors and other healthcare providers can reinforce the concepts of person–environment interactions that can effect regular physical activity participation among their patients.
As another example, there is now consistent evidence that in adults, walking for transport is more likely in neighbourhoods with connected street networks rather than those with disconnected street networks characterised by cul-de-sacs. However, there is conflicting evidence suggesting that this is not the case for younger children,28 and that living in a cul-de-sac may facilitate active play. Thus, all else being equal, the adoption of recommendations by adult or child physical activity by policy-makers or developers to include or exclude cul-de-sacs could produce unintended negative effects on other important subgroups. By working in interdisciplinary teams and thinking outside one’s square, policies and programmes that are developed may be able to accommodate both requirements. For example, fig 3 shows a relatively new medium-density development in California that combines cul-de-sacs with a grid-pattern street network. Another example might involve the creation of cul-de-sacs in a traditional grid-pattern neighbourhood that both prevents vehicular through-traffic but maximises pedestrian (cycling) through-traffic.

{kind=link}
{kind=link}
{kind=link}
 ; Imagery © 2008 Digital Globe, Geo Eye, U.S. Geological Survey; Map Data © 2008 Tele Atlas).
; Imagery © 2008 Digital Globe, Geo Eye, U.S. Geological Survey; Map Data © 2008 Tele Atlas).CONCLUSIONS AND FUTURE DIRECTIONS
The impact of the built environment on physical activity provides a unique opportunity for health professionals, civil engineering and planning academics, practitioners and policy-makers to work collaboratively and reconnect with the roots of their disciplines:7 achieving “social betterment” and improving the health, productivity and quality of life of urban populations.6 Using a systems-theory lens through which to view physical activity and the built environment research draws attention to how critical it is for this reconnection to occur to ensure that multiple forms of physical activity, settings, experts and population groups are considered in tandem.
In summary, the built environment and physical activity agenda provides a unique opportunity for public health, healthcare, physical activity and planning researchers to be front and centre of a movement aimed at creating healthier and more sustainable community environments. In order to optimise environments that encourage physical activity across the life course, we have attempted to build on the general idea of thinking “outside the square” by arguing that to optimise the effect of our research, we may need to think outside our own “square”. In this way, a more comprehensive set of research, practice and programme-related activities may emerge that will advance physical activity research and practice and consequently improve population health.
Acknowledgments
BGC is supported by an NHMRC Senior Research Fellow (grant no 503712). In 2008, the American Fulbright Commission provided her with a Senior Scholar Award to Stanford University and this funding is also gratefully acknowledged.
REFERENCES
Footnotes
Competing interests: None.