Article Text

Abstract
Tennis elbow or lateral epicondylalgia is a diagnosis familiar to many within the general community and presents with an uncomplicated clinical picture in most cases. However, the underlying pathophysiology presents a more complex state and its management has not been conclusively determined. Research on this topic extends across anatomical, biomechanical and clinical literature; however, integration of findings is lacking. We propose that the current understanding of the underlying pathophysiology of lateral epicondylalgia can be conceptualised as encompassing three interrelated components: (i) the local tendon pathology, (ii) changes in the pain system, and (iii) motor system impairments. This paper presents a model that integrates these components on the basis of a literature review with the express aim of assisting in the targeting of specific treatments or combinations thereof to individual patients.
Statistics from Altmetric.com
Pain over the lateral epicondyle associated with gripping and manipulation of the hand is generally linked with a diagnosis of tennis elbow or lateral epicondylalgia (LE). With an annual incidence of four to seven cases per 1000 patients in general practice1 2 and 1–3% within the general population,3–7 LE is a common condition that significantly impacts on the individual and society. It occurs primarily between the ages of 35 and 54 years, and typically affects the dominant arm in men and women alike.1 2 7 Tennis players8 and those working in industries requiring manual tasks with a combination of force, repetition and poor posture are at greater risk.7 9 10
LE is commonly recognised as being challenging to treat and prone to recurrent episodes. The average duration of a typical episode ranges from 6 to 24 months, with most patients (89%) reporting recovery by 1 year.1 High recurrence rates have been reported with corticosteroid injection, a common conservative treatment of LE. In a recent randomised controlled trial, 72% of patients reported a recurrence in their condition within 12 months of receiving a corticosteroid injection in comparison to 9% with a “wait and see” policy.11 It has been estimated that between 5% and 10% of patients develop chronic symptoms and eventually undergo surgical intervention.12–15
The clinical presentation of LE is reasonably straightforward and easy to recognise, which contrasts with a more complex underlying pathophysiology. Whilst our knowledge of clinically effective treatments is increasingly evidence-based, the challenge for the healthcare practitioner, whether in the clinic or the laboratory, is to reconcile this with emerging findings of the condition’s pathophysiology. This paper provides a synopsis of the current evidence of the pathology of LE and proposes a model that seeks to reconcile this evidence with emerging best practice strategies in the management of the condition.
A PROPOSED PATHOPHYSIOLOGICAL MODEL OF LATERAL EPICONDYLALGIA
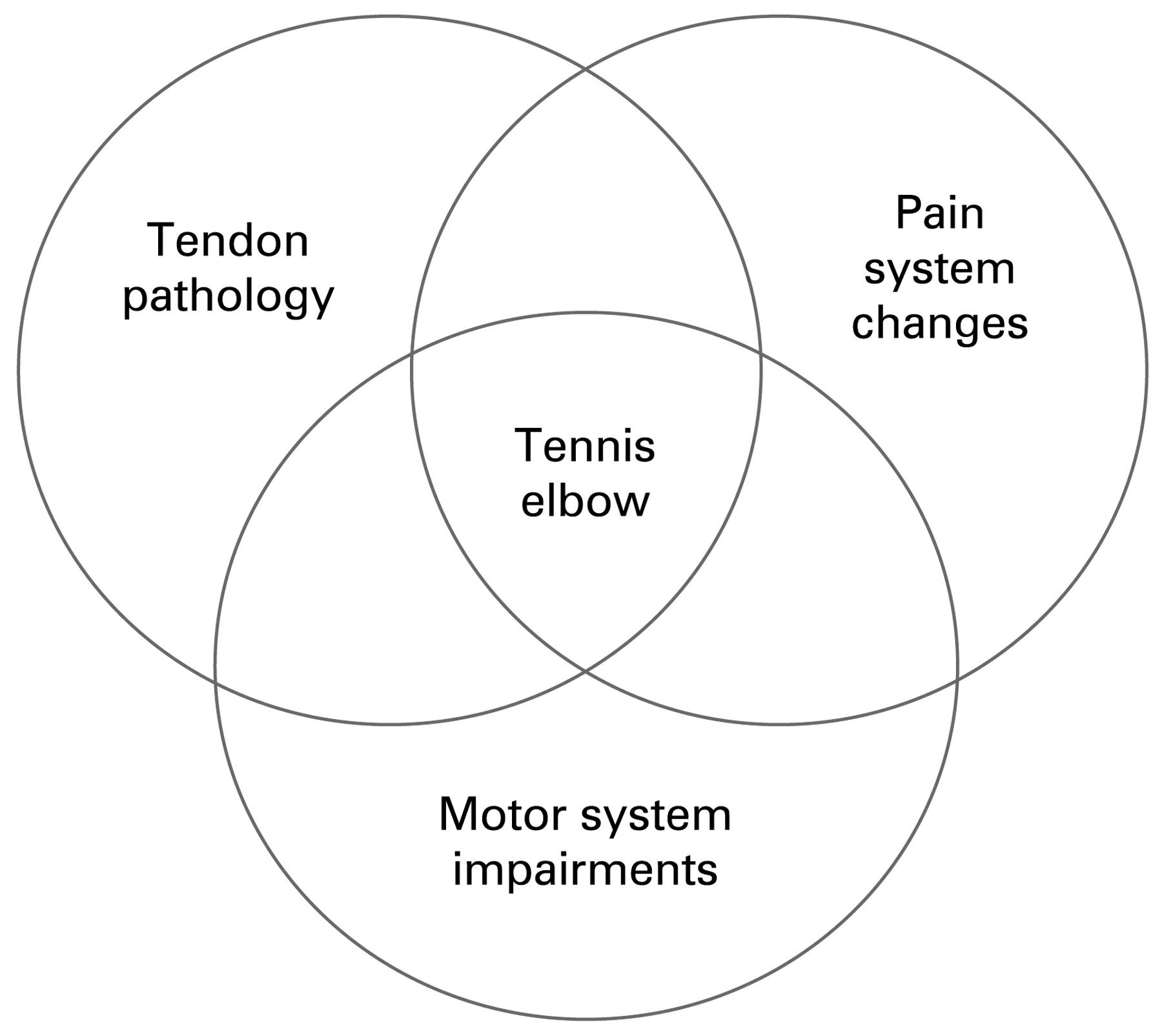
A new model is proposed to assist integration of current evidence of LE’s pathophysiology with the purpose of providing a better rationale for emerging management strategies. We propose that LE can be conceptualised as comprising three interrelated components: (i) the local tendon pathology, (ii) changes in the pain system, and (iii) impairment in the motor system (fig 1). In this model it is recognised that not all LE patients have the same clinical presentation. It is proposed that, through comprehensive evaluation, different proportions of tendon pathology, pain system dysfunction and motor system impairments can be used to define subgroups of LE in the clinic and research laboratory. This will assist in the matching of individual patient presentations to effective treatment approaches.
{kind=link}
A new model of lateral epicondylalgia emphasising its multifactorial pathology.
EVIDENCE OF LOCAL TENDON PATHOLOGY
Similar tendon changes have been identified in LE and in Achilles and patellar tendinopathies, suggestive of a consistent underlying process.16 Microscopic and histological analyses of affected tendons have identified four key changes, collectively termed angiofibroblastic hyperplasia: (1) increased cell numbers and ground substance; (2) vascular hyperplasia or neovascularisation; (3) increased concentration of neurochemicals and (4) disorganised and immature collagen.17–19 Consistent absence of inflammatory cells has resulted in the general consensus that the process is non-inflammatory in nature, although neurogenic inflammation may play a role.19 20 Instead, the pathological process has been described as “degenerative”, or one of “dysfunctional, immature healing”.17 18 21 A continuum of tendon cellular and structural changes has been recently proposed to occur in tendinopathy, accounting for heterogeneity of presentation.22 Neovessel ingrowth has recently received increased attention as a source of pain in LE, owing to the close association between neural structures, microvasculature and neurochemicals at the proximal tendinous insertion of extensor carpi radialis brevis (ECRB).23–25
Tendons are a living tissue and respond to mechanical forces by altering their structure, composition and mechanical properties, a process referred to as mechanotransduction.22 26–29 Physical training promotes both synthesis and degradation of collagen with a dominance of the former process, resulting in increased Type I collagen.29 30 Stress-deprivation adversely affects tendons, resulting in increased fibroblasts, decreased longitudinally aligned collagen, decreased tendon stiffness and tensile strength.29 31 Altered gene expression, imbalance of matrix metalloproteinases, a group of enzymes involved in remodelling of the extracellular matrix, and growth factors are currently being studied to better understand the dynamic response of tendon to mechanical loading.32
LE is traditionally described as an overuse injury, where the ability of the tendon to repair itself becomes overwhelmed, leading to microscopic and macroscopic changes.17 19 33 However, recent studies of patellar and Achilles tendons have identified lower strain levels in the deeper regions of the tendon associated with tendinopathic change.34 35 It was suggested that stress-shielding, a term used to describe the tissue experiencing lower strain levels, may predispose specific regions of the tendon to structural weakening, making it more susceptible to overload.22 27 36 37 It has also been argued that insertional tendinopathies may not be purely tensile injuries, but that compressive and shear forces may be involved.21 38 39 The fibrocartilaginous composition of the ECRB enthesis may reflect a functional adaptation to these forces.40
Pathological changes have been reported in the deep and anterior fibres of the proximal insertion of the ECRB tendon, defining LE as an “insertional tendinopathy” or “enthesopathy”.15 18 41 42 An understanding of the unique structure and function of the extensor region of the elbow is useful for appreciation of pathology. The ECRB enthesis comprises a superficial, narrow attachment to the lateral epicondyle and a broad attachment to an intermuscular septum.40 43 The deeper aspect merges directly with the lateral collateral ligament and indirectly with the annular ligament. The extensive connections of this enthesis are believed to be involved in the natural dissipation of stress across a broad area.33 40 43 High levels of stress within the ECRB musculotendinous unit have been suggested as contributing to the overuse changes seen in LE.44 45 In summary, local tendon pathology may be the result of overuse, underuse, or tensile, compressive or shear forces, which leave the tendon in a debilitated state.
Diagnostic imaging of local pathology
While LE is usually diagnosed clinically, recent research using imaging suggests that certain modalities may be helpful in diagnosing local tissue pathology. Ultrasound imaging has been used to identify grey-scale or structural changes in affected tendons in LE, including tendon thickening or thinning, focal areas of hypoechogenicity, tendon tears, calcification or bony irregularity.42 46–48 Tendon neovascularisation in LE has been detected with Doppler ultrasound and correlated with degenerative tissue on biopsy.41 47 Comparison of these two imaging modalities by du Toit et al (2008) found neovascularity detected by power-Doppler to be diagnostically superior in identifying chronic LE compared with grey-scale changes.47 The absence of both tendon neovascularity and grey-scale changes was shown to conclusively rule out LE as a diagnosis and should prompt further investigation.47 However, the amount of neovascularity was not correlated with clinical measures of pain severity or function.47 In summary, current evidence suggests that imaging is useful for confirmation of the diagnosis of LE and that neovascularity, but not structure, might be related to clinical findings. There is currently no evidence to suggest that findings on imaging should dictate management of the condition or be used as an outcome measure.39 49
EVIDENCE OF PAIN SYSTEM CHANGES
In chronic musculoskeletal pain states such as LE, the patient’s pain experience may culminate from changes in both the peripheral and central nervous systems, possibly involving both nociceptive and non-nociceptive processes as well as neuronal and non-neuronal tissues. We use the term “pain system changes” to define this complex phenomenon. It is increasingly recognised that a disordered pain system itself may contribute to the pathophysiology of the condition.24 25 50 51 Microdialysis of LE-affected tendons has demonstrated increased concentrations of glutamate.20 Substance P and calcitonin gene-related peptide reactive nerve fibres have been located in the proximal ECRB tendon in conjunction with small blood vessels.23–25 These neurochemicals are known to be potent modulators of pain in the human nervous system, with additional roles in regulating the local tendon circulation and neurogenic inflammation.19 23–25 50
Quantitative sensory testing has been used to better understand the pain-processing mechanisms underlying LE symptoms. In brief, LE is typically characterised by hyperalgesia, defined as an exaggerated or increased response to a noxious stimulus.52 Reduction in pressure pain thresholds by an average of 45–54% has been demonstrated over the lateral epicondyle of affected elbows compared with unaffected elbows of LE sufferers.53–56 In comparison with a healthy control group, Slater et al (2005) demonstrated significant bilateral hyperalgesia in LE.57 It was suggested that transition from a unilateral localised pain to chronic LE with bilateral manifestations may be a time-dependent process.57 Whilst thermal pain threshold is not affected in the majority of LE,54 58 cold hyperalgesia was found in a subgroup of patients with chronic LE who responded to a regional block with guanethidine, that is, those with a component of sympathetically maintained chronic pain.59
Secondary hyperalgesia in lateral epicondylalgia
A number of interacting neurophysiological mechanisms may explain the hyperalgesia observed in LE. The presence of bilateral deficits in pain thresholds,57 along with bias towards mechanical rather than thermal hyperalgesia,51 is characteristic of secondary hyperalgesia. This implicates some form of altered processing within the neuraxis (spinal or supraspinal centres), often referred to as central sensitisation.52 Extrapolation from other neurophysiological studies suggests that this process is initiated by activity in peripheral nociceptors, but may be sustained in the absence of peripheral nociceptor input.52 Release of excitatory amino acids and neuropeptides, such as glutamate and Substance P, from presynaptic nociceptive afferents may be involved in initiation of a cascade of changes that enhance the neuron’s responsiveness, which include increased excitability of wide-dynamic range neurons and increased receptive field size.52 Further supporting the involvement of this process in LE is evidence of myelinated group A fibres mediating the reduced mechanical pain thresholds in LE.51
A defining feature of secondary hyperalgesia is the spread of the reduced mechanical pain threshold beyond that of the original site of tissue injury.52 This may explain how symptoms of LE can arise from tissues, such as the cervical spine and neural tissues, that are neurologically related to, but not at, the injured tissue site.53 60–64 Positive findings on manual examination of the cervical spine have been documented in 56% of LE sufferers.61 Comparison with an age-matched control population found a significantly higher prevalence of self-reported neck pain in LE participants, suggesting that degenerative and age-related changes do not sufficiently account for neck pain in people with LE.60 Several studies have also reported positive radial nerve neurodynamic testing in LE participants.54 61 62 The presence of concomitant neck pain has been associated with higher pain scores at 1 year follow-up,1 while female patients with nerve symptoms (pins and needles or numbness) were more likely to experience a poorer short-term outcome after 8 weeks of physical therapy.61
EVIDENCE OF MOTOR IMPAIRMENTS
Evidence of dysfunction of the motor system has been demonstrated in LE, including diminished strength,56 57 65 morphological changes66 and altered motor control.67–70 Consistent with the pattern of impairments in the pain system, some of the motor system changes are apparent bilaterally67 71 and at both local and remote sites.72
Deficits of gripping capacity
The wrist extensors are strongly activated in a stabilising role to prevent wrist flexion during gripping activities.33 Interestingly, pain-free grip is more sensitive to change than maximum grip strength, and is the recommended clinical outcome measure in LE.73 Pain-free grip force is reduced in LE by an average of 43–64% in comparison with the unaffected side.54 55 67 74 75 By definition, this measure reflects the amount of force required to first reproduce pain and as such it is an indirect measure of the pain system, rather than a measure of strength. Testing of maximal grip strength in LE participants has revealed differing results between studies, with unilateral weakness,57 bilateral weakness72 and no weakness67 reported. Unpublished data from the latter study showed that maximal grip strength testing reproduced an average pain intensity on visual analogue scale of 53 mm, indicating that this test in this population is strongly pain-provocative (Bisset, L. and Vicenzino, B. unpublished data, 2006), further emphasising pain-free grip testing rather than maximum grip strength as an outcome measure.73
Specific muscle strength deficits
Flexor and extensor strength deficits have been observed at the wrist and hand in LE participants compared with healthy controls,57 72 with the exception of extension of the metacarpophalangeal joint.72 It was suggested that LE sufferers may maintain or increase strength of the finger extensors to compensate for weakness in the wrist extensors.72 Assessment of shoulder rotation strength identified weakness in LE participants, indicating the local and remote impact of the condition.72 In a subsequent study, Alizadehkhaiyat (2007) assessed muscle function in participants with a history of LE who had been asymptomatic for at least 6 months.70 Remaining weakness was demonstrated on all upper limb strength measures except for strength of muscles of the metacarpophalangeal joint, compared with control participants, indicating incomplete functional recovery despite attenuation of pain.70
Morphological changes of muscle
Morphological abnormalities have been identified in the ECRB muscle of patients with long-standing LE.66 These include moth-eaten fibres, fibre necrosis and signs of muscle fibre regeneration as well as higher percentages of the fast twitch oxidative muscle fibre type.66 These changes are consistent with the identified strength deficits and would likely contribute to ongoing motor system impairment.
Motor control deficits
Electromyographic activity of the forearm muscles has been studied during the backhand tennis stroke.68 Activity within ECRB muscle in LE-affected players was significantly lower during the early acceleration phase, while greater at ball impact compared with uninjured players. Recently, reduced activity of extensor carpi radialis (ECR) muscles was demonstrated in participants with LE, during isometric wrist extension69 and gripping tasks,72 implicating an endurance deficit. Follow-up testing of participants with symptomatic recovery from LE revealed improved ECR activity, suggestive of a link between neuromuscular activity and symptoms.70 Pain-related inhibition or fear of pain and further injury were suggested as underlying mechanisms, but no comment was made about the pain responses during testing.72
Bilateral deficits in wrist position during gripping (11° less extension)67 and bilateral impediments in reaction time and speed of movement with reaching tasks67 71 have been identified in unilateral LE, possibly reflecting a motor correlate to alterations in central processing found in the pain system. Consistent with this is greater error in detection of movement found in affected elbows of participants with LE when compared with a healthy control group, and suggests that poorer proprioception may contribute to impairments in motor function.76 The optimal wrist posture for maximal grip force in healthy adults is reported to be slight wrist extension,77–79 with wrist flexion reducing maximal force development according to proposed models of length–tension relationships at the wrist.44 This may account for grip strength deficits found in some LE patients.
HETEROGENEITY OF CLINICAL PRESENTATION
The clinical presentation of LE varies between individuals and possibly over the time course of the disorder. We propose that the three model components discussed above do not occur in isolation and do not independently provide a complete explanation for a patient’s clinical presentation. Some patients with acute LE may exhibit increased involvement of the pain system, while others, with more recalcitrant conditions, may present with marked local tendon pathology. It is our contention that healthcare practitioners should seek to identify the relative expression of local pathology, pain and motor system dysfunction in individual patients, so that treatment strategies may be better matched to the clinical presentation.
CONSERVATIVE MANAGEMENT OF LE
Ideally, management should involve the integration of the patient’s clinical presentation with the evidence base of treatment efficacy and the condition’s underlying pathophysiology. We propose that our model be used to aid in interpreting the evidence base in order to customise the management approach for each individual patient. The following section will present a synopsis of the current evidence for conservative management of LE and highlight potential links to pathophysiological bases. Pharmacotherapy, electrophysical therapy, exercise and multi-modal therapy tend to be the main conservative management strategies for LE.
Pharmacotherapy
Pharmacotherapy may be prescribed to facilitate early symptomatic relief and indirectly, through reduced nociceptive input, may limit potential sensitisation processes and motor impairment.
Corticosteroid injection is considered effective in terms of short-term relief of symptoms in LE, supported by level 1 evidence from multiple randomised controlled trials.11 80–82 However, poor long-term outcomes have been consistently reported following this treatment,82–84 including evidence of greater use of pain-relieving medication and significantly higher recurrence rates than physiotherapy.11 The physiological basis for these positive and negative effects has been attributed to alterations in release of noxious chemicals19 23 85 and inhibition of collagen and granulation tissue23 86 respectively.
Polidocanol, an aliphatic non-ionised nitrogen-free surface anaesthetic that is used as a sclerosing agent,87 has been used in LE to predominantly target neovessels under ultrasound guidance.88–90 Injection of polidocanol has been shown to be comparable to an injection of lidocaine and epinephrine in effecting an approximate 34 mm improvement in pain on visual analogue score (VAS) at 12 months.88 Considering that this improvement is of similar magnitude to that of corticosteroid injection,11 91 92 further consideration should be given to evaluating their relative clinical efficacy, including recurrence rates.
Pharmacology research has also focused on the role of various agents in stimulating tendon healing. The efficacy of topical application of nitric oxide patches in LE has been investigated in LE and other tendinopathies due to a hypothesised effect on collagen and matrix synthesis.93 A clinical trial with placebo comparison in LE demonstrated a 21% greater effect than with exercise alone.94 The major complications of this medication were headache, weakness, dizziness and skin irritation, with 12% discontinuing treatment due to side-effects. Notably, the positive clinical effects of nitric oxide patches were not supported in a recent dosing study95 in which these patches were combined with stretching only (not the concentric and eccentric exercises of the previous study).94 This appears to infer that the beneficial clinical effects of nitric oxide patches in treating LE may be dependent upon the physical stimulus of specific concentric–eccentric exercise. Preliminary case series studies of injection of autologous blood or platelet-rich plasma have reported positive effects on pain and patient satisfaction in LE; however, no randomised clinical trials have been reported.96–98
While the above pharmacological agents are promising, selectively treating those patients who present with a predominance of pain system involvement or with identifiable structural tendon pathology may enhance their effectiveness. We suggest that implementation of the model may be used by clinicians and researchers to match patient presentations with appropriate pharmacological agents.
Electrophysical agents
The efficacy of electrophysical agents in treatment of LE has been evaluated in a number of systematic reviews.99–102 The rationale for their clinical use is generally attributed to either stimulation of soft tissue healing and/or inhibition of pain receptors.99 102 Bjordal et al (2008) recommend that low level laser therapy (LLLT) may be considered as an alternative therapy to pharmacological agents in management of tennis elbow.99 Meta-analysis of data from 10 trials found a significantly greater improvement in pain (VAS of 10.2 mm) with LLLT over controls at the end of the treatment period. The narrowly defined regime of 908 nm wavelength directly at the tendon site provided greater pain relief (17.2 mm (95% CI: 8.5 to 25.9) and RR of 1.53 (95% CI: 1.28 to 1.83)) in the short term, which highlights the importance of considering specificity of dosing parameters. Currently there is no consensus on the use of shock wave therapy for this condition, owing to a lack of high-quality trials and contradictory evidence between trials and between systematic reviews.100 102 Weak evidence was reported for the effectiveness of ultrasound in comparison with placebo on the basis of two small trials,103 while a recent study found no significant effects of this modality.99 104
In lieu of evidence from the literature, it is difficult to recommend or dissuade the clinical use of electrophysical agents as the sole intervention in LE. We contend that these treatments should be considered adjunctive treatments, largely to target the pain system to allow optimal, pain-free tendon loading. Further research regarding the effects of electrotherapy on accelerated and long-term healing of tendon is necessary.
Manual therapy
There is some evidence, albeit low-level, of positive initial effects of several manipulative therapy techniques for pain relief and restoration of function when compared with control interventions.55 74 105–107 It is hypothesised that the manipulation-induced analgesia is primarily mediated via non-opioid, descending pain inhibitory mechanisms.55 75 107 108 Soft tissue manipulations in the form of transverse frictions and Mill’s manipulations have been advocated for targeting the local tendon pathology, but results of clinical trials have not supported their use when compared with exercise109 or corticosteroid injection.110 No firm conclusions were made regarding use of orthotic devices for LE by two systematic reviews,111 112 while a third reported an early positive, but inconclusive, effect.113
Exercise
The effect of exercise training on stimulating tendon remodelling and producing muscular adaptive responses has been clearly documented.26 29 30 Thus, there exists a rationale for use of exercise to address two characteristic impairments in LE, as outlined in fig 1. In addition, exercise may have local analgesic effects, as observed following specific therapeutic exercise in chronic neck pain patients.114
Surprisingly, few studies have investigated the effect of therapeutic exercise as the sole treatment of LE compared with a control or no intervention.111 Positive benefits after concluding an 8 week exercise programme were demonstrated in a chronic LE population, who had high baseline pain (73/100 mm on VAS) and had failed other conservative treatments, including corticosteroid injection.115 On following a similar group of patients (exercise n = 12, ultrasound n = 11) for an average 36 months, these researchers showed that, compared with an ultrasound treatment, exercise resulted in fewer medical consultations, less surgery (relative risk (RR): 0.18 (95% CI: 0.03 to 1.33); number needed to treat (NNT): 3) and 586 fewer sick days.116 In another randomised controlled trial, the supervised exercise programme produced the largest reduction of pain and improvement in function at all time points in the 6 month follow-up period, compared with Biopton light and soft tissue frictions with elbow manipulation.109
The most effective exercise protocols in treating LE are not clearly established.117 118 The successful program utilised by Pienimaki et al (1996) comprised a combination of exercise modes — isometric and isotonic forearm exercises, forearm stretches and, in the final stages, functional exercises including gripping and manipulation tasks.115 Alizedehkhaiyat et al (2007) assert that a comprehensive rehabilitation programme may be necessary to address the widespread upper limb weakness and changes in muscle activity found in LE.72 Retraining of the functional task of gripping using a more efficient, slightly extended wrist posture may need to be factored into the design of rehabilitation programmes.67 Recently, there has been an increased emphasis placed on the role of isolated eccentric strengthening exercises for LE, modelling the apparently successful use of such exercise for lower limb tendinopathies.119 120 However, a recent systematic review concluded that there is currently insufficient evidence to support eccentric over concentric exercise for LE.121 The intensity and frequency of tendon loading are also important variables, and there should be an attempt to match these to the stage and reversibility of tendon pathology.22 The pain system must be acknowledged to avoid peripheral nociceptive input reinforcing the hyperalgesic state. Reduction of load may be necessary in the early phases of rehabilitation through avoidance of aggravating activities.
Given hypotheses concerning stress-shielding27 36 37 and the role of compressive forces in the aetiology of insertional tendinopathies,21 38 39 further research is necessary to determine the most efficient positions and exercises for tendon loading in LE. Greater success has been demonstrated for insertional Achilles tendinopathy with restriction of eccentric exercise to avoid full dorsiflexion.122 As elbow extension has been found to be a more provocative position for gripping in LE,123 likely due to compressive forces at insertion, we recommend that exercise of the wrist extensors be commenced in a flexed elbow position.
Multimodal management
Given the complexity of the pathophysiology of LE and the heterogeneity of clinical presentation, we propose a multimodal approach to management of this condition. Multimodal programmes are recommended in other chronic musculoskeletal conditions124 and have been studied in a number of randomised controlled trials of LE.11 92 The physiotherapy programme utilised by Bisset et al (1996), combining concentric, eccentric and isometric exercise with “Mobilisation with Movement” manipulation techniques to the elbow, has shown positive results. It was superior to “wait and see” at 6 weeks (RR: 2.44 (95% CI: 1.55 to 3.85); NNT: 3) and to corticosteroid injection at 26 weeks (RR: 1.88 (95% CI: 1.41 to 2.5); NNT: 2).11 Other studies utilising exercise, ultrasound and friction massage have not found significant benefits over a wait and see approach.92 In clinical practice, injections are commonly prescribed in conjunction with active exercise. Comparison of corticosteroid injection alone or combined with a progressive exercise programme has been made only in one short-term study,125 but it suffered from a high drop-out rate and was unable to support or refute the combined approach.
CONCLUSION
A new model of the pathophysiology of LE is presented, integrating local tendon pathology, pain system changes and motor impairment. This model encompasses an understanding that individual patients may present with relatively different contributions of local tendon pathology along with pain and motor system impairments. Importantly, it is our contention that to optimally manage each patient the clinician should consider this relativity. It must be appreciated that this model is conceptual in nature and reductionist by definition, but with capacity for development as new knowledge emerges. Furthermore, it may be seen as a precursor stage to the development of clinical prediction rules, classification and subgrouping studies, as has occurred for other musculoskeletal conditions, albeit spinal.126–129
What is already known on this topic
Tendinopathies appear to share similar pathological features.
Lateral epicondylalgia can be challenging to treat with many treatment options available to the clinician.
What this study adds
An appreciation of the heterogeneous clinical presentation of lateral epicondylalgia.
A model that conceptualises lateral epicondylalgia as involving local tendon pathology, abnormal pain processing and motor system impairments.
A rationale for physical interventions to be customised to each individual patient on the basis of proportional representation of local tendon, pain and motor deficits in the patient’s clinical presentation.
Multi modal management approaches may offer practitioners better coverage of the problems facing patients.
REFERENCES
Footnotes
Funding: National Health & Medical Research Council Grant #511238.
Competing interests: None.