Article Text

Abstract
Objective: The aim of this study was to investigate the kinetics, kinematics and muscle activity in runners with Achilles tendinopathy.
Design: Case–control study.
Setting: Biomechanics laboratory.
Participants: 21 runners free from injury and 21 runners with Achilles tendinopathy performed 10 running trials with standardised running shoes. Injured runners were diagnosed clinically according to established diagnostic criteria. Uninjured runners had been injury-free for at least 2 years.
Main outcome measurements: During each trial, kinetic and lower limb kinematic data were measured using a strain gauge force plate and six infrared cameras respectively. Electromyographic (EMG) data from six muscles (tibialis anterior (TA), peroneus longus (PE), lateral gastrocnemius (LG), rectus femoris (RF), biceps femoris (BF) and gluteus medius (GM)) were measured with a telemetric EMG system.
Results: Knee range of motion (heel strike to midstance) was significantly lower in injured runners than in uninjured runners. Similarly, preactivation (integrated EMG (IEMG) in 100 ms before heel strike) of TA was lower for injured runners than uninjured runners. RF and GM IEMG activity 100 ms after heel strike was also lower in the injured group. However, impact forces were not different between the two groups.
Conclusion: Altered knee kinematics and reduced muscle activity are associated with Achilles tendinopathy in runners. Rehabilitation exercises or other mechanisms (e.g. footwear) that affect kinematics and muscle activity may therefore be beneficial in the treatment of runners with Achilles tendinopathy.
Statistics from Altmetric.com
Achilles tendinopathy is one of the most common injuries of the Achilles tendon and is particularly prevalent in distance runners, representing 5 to 18% of the total injuries in runners.1 Intrinsic and extrinsic factors have been associated with the aetiology of the Achilles injury.2 Extrinsic factors associated with Achilles tendon injury include training errors, running technique, previous injury, footwear and running surfaces. Intrinsic factors related to the injury include tendon vascularity, gastrocnemius–soleus dysfunction, age, gender, body weight, genetic factors, muscle weakness and lower limb misalignment (cavus feet and increased pronation).1–5 It is important to note that the scientific evidence for the majority of these extrinsic and intrinsic risk factors is based on clinical evidence rather than experimental studies.2 6–8
In a single case–control study, training history, muscle strength, lower limb kinetics and ankle kinematics were studied in 31 runners with Achilles tendinopathy and 58 non-injured controls. The findings of this study showed that Achilles tendinopathy was associated with more years of training, greater plantar and dorsiflexion torque and an earlier and increased peak pronation.1 However, this study did not investigate hip and knee kinematics and used two-dimensional instead of three-dimensional kinematic analysis.
In recent years the importance of neuromuscular control during running has been suggested as an important variable to investigate in the aetiology of running injuries.9 In one study, muscle activity during walking and running was compared between patients with anterior cruciate ligament (ACL) deficiency and non-injured controls. In this study, a reduction in muscle activity during running and after 10 minutes of walking was documented in the ACL-deficient group.10 However, there are no similar studies of muscle activity in runners with Achilles tendinopathy.
Based on the muscle activity and kinematic differences seen in other studies with injured populations, we hypothesised that runners with Achilles tendinopathy may have reduced muscle activity and altered lower limb kinematics. Therefore, the aim of this study was to compare the three-dimensional kinematics, kinetics and muscle activity in runners with Achilles tendinopathy with matched uninjured runners.
METHODS
Subjects
Twenty-one uninjured runners (UN) (16 men and five women) and 21 runners with Achilles tendinopathy (IN) (16 men and five women) participated in this study. Participants’ characteristics are described in table 1.
The injured runners were diagnosed by a sports physician at the Sports Science Institute of South Africa. All the participants in the injured group fulfilled the following clinical diagnostic criteria of non-insertional Achilles tendinopathy:2 11 (1) gradual progressive pain over the posterior lower leg (Achilles tendon area), (2) early morning pain and stiffness, (3) history of swelling over the Achilles tendon area, (4) tenderness to palpation over the Achilles tendon, (5) palpable nodular thickening over the affected Achilles tendon, and (6) a positive “shift” test (movement of the nodular area with plantar-dorsiflexion). All the injured runners suffered from either grade I (pain after running) or grade II (pain during running but not restricting running) injury.12 The participants in the uninjured group were runners who had been injury-free for at least 2 years. In both groups the runners had to have run more than 15 km per week for at least 3 years and have no current or past history of physical deformities, neurological disorders, diabetes mellitus or previous lower limb surgeries.
The study was approved by the Research Ethics committee of the Faculty of Health Sciences at the University of Cape Town in South Africa and a written informed consent was obtained from all subjects before the study.
Experimental procedure
Each subject was required to report to the laboratory on one occasion. All the testing took place at the Gait Analysis Laboratory in the Sports Science Institute of South Africa.
The trials were conducted with a standard neutral running shoe (Rainha Athens, Alpargatas Inc; shore A 40). Fifteen retroreflective markers from the modified Helen Hayes marker set13 were placed on subjects (fig 1) and a six-camera motion analysis system (Oxford Metrics Vicon System 370 Version 2.5, Oxford Metrics Ltd, Oxford, United Kingdom) was used to collect kinematic data at 120 Hz.
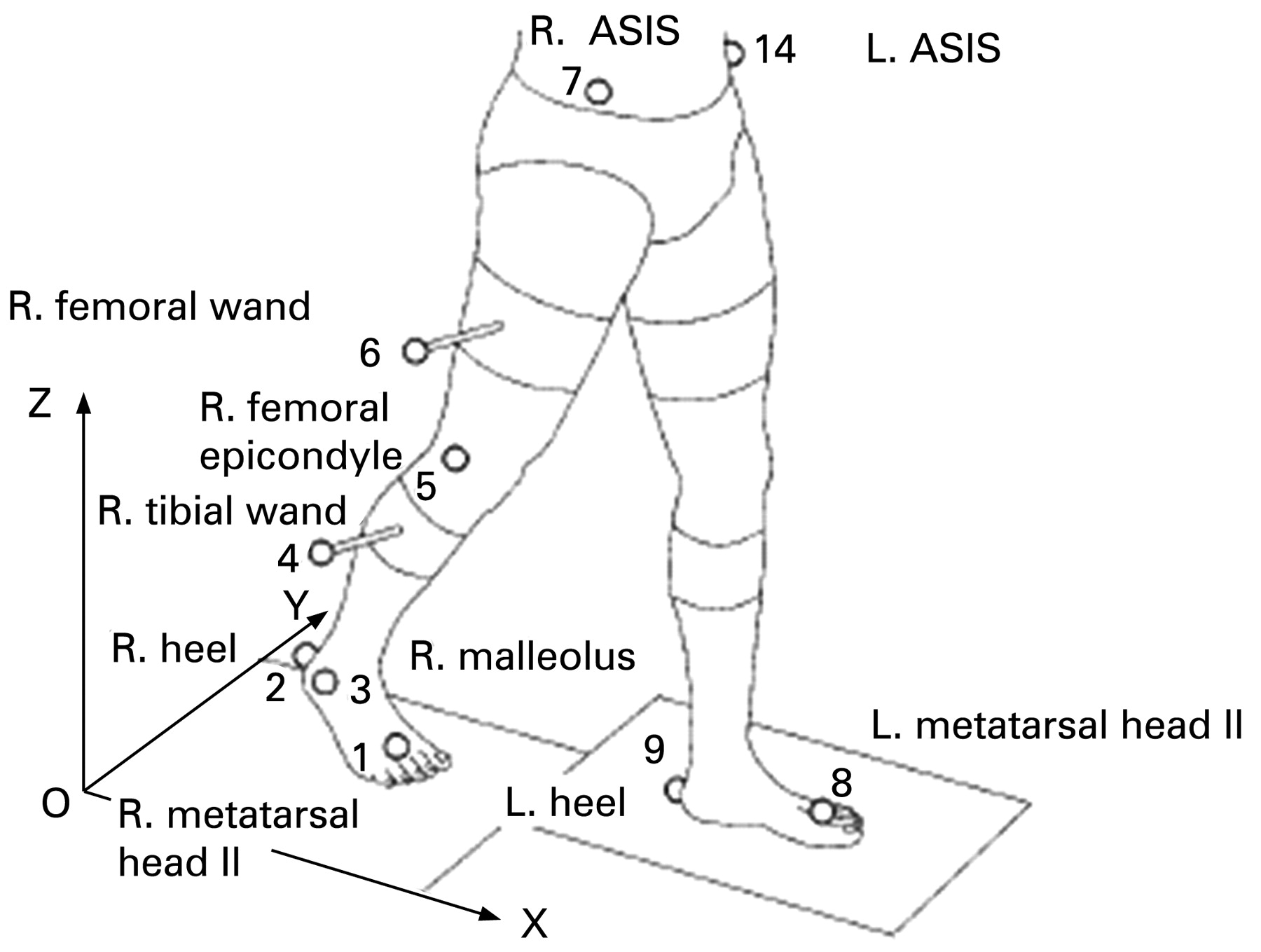
{kind=link}
Helen Hayes marker set.13
Ground reaction force data were collected with an Advanced Mechanical Technology, Inc. (AMTI Newton, MA, USA) force plate (1000 Hz), which was situated underneath the surface walkway. Vertical and horizontal forces were normalised by body weight (BW). Bipolar surface electrodes were placed over the visual midpoint of the contracted belly of tibialis anterior (TA), lateral gastrocnemius (LG), peroneus longus (PE), rectus femoris (RF), biceps femoris (BF) and gluteus medius (GM) muscles.14 The electrodes were placed on the right limb for the uninjured runners and on the affected limb for the injured runners. A single electrode (ground electrode) was placed over the patella. The cables and amplifiers were taped to the skin to minimise movement artefacts. Surface electromyographic (EMG) signals were recorded with a telemetric EMG system (Telemyo, Noraxon USA, Inc.) at a sampling rate of 2000 Hz. The EMG, kinetic and kinematic data were collected simultaneously during the recording process through Oxford Metrics Vicon System and thus synchronised. The synchronisation was processed through Workstation (Oxford Metrics, England), which auto-adjusts the setting to agree with the cameras (120 Hz). Therefore, the force plate was processed at 960 Hz and the EMG at 1920 Hz.
After a familiarisation trial, the runners were instructed to run 10 trials at a self-selected speed on the 10 m pathway of the gait laboratory. The running velocity (m/s) was determined by the sacrum retroreflective marker that was attached to each runner. The horizontal velocity was calculated through the movement of the marker on the x-axis of the global reference system of the laboratory for each trial. To promote a more natural running style during the short 10 m run, the runner was motivated not to stop running during the 10 trials. Furthermore, the force plate was hidden on the floor so the participant would not target the force plate while running. A trial was considered valid when (1) the runner’s foot made contact with the force plate and (2) there was no alteration in the running style as judged subjectively by the investigator. The injured runner touched the force plate with the affected foot and the uninjured runner contacted the force plate with the right foot.
Data analysis
Five valid trials were selected based on the quality of the data (e.g. no missing markers or interference) for each subject for further analysis. The data were processed for one stride length (one step before and one step after the force plate). For the runners who reached the force plate with the right foot (uninjured runners and runners injured on their right limb), the data was processed from left heel strike to left heel strike. For runners who reached the force plate with the left limb (runners injured on their left limb), the data was processed from right heel strike to right heel strike.
Kinetic and kinematic data were processed to determine the timing of gait events, segment the data and calculate kinematic, kinetic and temporal distance parameters using Workstation and Body Builder (Oxford Metrics, England) and the Gait Model. Kinematic data was filtered with the weighted average filter, and a low pass digital filter was applied for the kinetic data. The processed data for each stride were also normalised in time to 51 data points (0 to 100% gait cycle, intervals of 2%) (MATLAB). This allowed the averaging of the five trials for each subject (Excel). The kinetic and kinematic variables presented in table 2 were included in the analyses.
The EMG signals were analysed as follows (MyoResearch): signals were band-pass filtered, 15–500 Hz, and the root mean square amplitude (RMS) was calculated for consecutive periods of 50 ms. The mean dynamic method was applied to normalise the EMG.15 Values were expressed as a percentage of the mean RMS EMG. The integrated EMG (IEMG) was then calculated for each trial for two periods: 100 ms before heel strike (pre) and 100 ms after heel strike (post). After this initial analysis the EMG data were normalised in time using the same method as for the kinematic and kinetic variables and the five trials averaged for each subject.
Statistical analysis
All data are expressed as mean (standard deviation) (X (s)). Differences between the two groups were compared using the t test for independent variables. The false discovery procedure was used to account for multiple comparisons.16 This practical method overcomes some of the pitfalls associated with other common techniques (Bonferroni, Newman–Keuls and least square difference). Statistical significance was accepted as p⩽0.05 before the adjustments were made.
RESULTS
The temporal distance parameters (table 3) and kinetic variables (table 4) were similar in uninjured and injured runners.
The kinematic variables of the two groups are presented in table 5. There was a decreased range of knee flexion between heel strike and midstance (KROM) in the injured runners compared with the uninjured runners (p = 0.011). It can also be noticed that both groups of runners were rearfoot strikers, indicated by the negative values of ankle angle at initial contact (Aic).
The IEMG activity 100 ms before heel strike (pre) and 100 ms after heel strike (post) of the lower limb muscles is depicted in table 6. There was a significant decrease in the pre-heel strike IEMG activity of TA in the injured runners compared with the uninjured runners. Likewise, post-heel strike IEMG activity of RF and GM were significantly lower in the injured runners than in the uninjured runners.
DISCUSSION
The main findings of this study were that runners with Achilles tendinopathy had a lower KROM and decreased IEMG of the TA, RF and GM during the critical pre- or post-heel strike periods of the running cycle. These findings, therefore, identify that there are neuromuscular and kinematic differences between runners suffering from Achilles tendinopathy and uninjured runners, supporting the initial hypothesis. To our knowledge, this is the first study to report reduced muscle activity of the lower extremity in runners who present with a lower limb overuse running injury.
In the past, lower limb biomechanical analysis of injured runners was limited to the assessment of kinematic and kinetic variables.1 3 17 However, in recent years, there has been a shift in focus, and the possible role of altered muscle activity either in the development or as a result of running-related injuries has been identified.18 There has been speculation that the increase in muscle activity before and after heel strike is important to reduce muscle vibration during impact forces.18 In our study vertical impact force peak and loading rate were similar in the two groups (table 4), and this is in agreement with the findings from a previous study on runners who had Achilles injuries.1 However, in our study the relative muscle activity was significantly lower for TA pre-heel strike, and RF and GM post-heel strike in the injured group (table 6). This shows differing muscle activation strategies at this crucial time in the gait cycle.
Studies of running shoes with different hardnesses have shown that, although impact forces were not altered by hardness, loading rate and muscle activity were affected.19 20 Some authors speculate that changes in internal load (e.g. muscle activity) do not correspond to changes in external load (e.g. impact forces) and suggest that internal load should be considered when shoe materials are studied as this could have implications for potential injury.19 Comparing these results with the findings of our study, we can suggest that the injured runners experienced a similar external load (similar impact forces) but different internal load (lower muscle activity) when running with standardised running shoes. We suggest that further studies should investigate a range of running shoes in order to identify whether footwear modification could attenuate the differences in muscle recruitment between injured and uninjured populations.
In this study muscle activity was investigated in a window period of 100 ms before and after heel strike (table 6). Studies which measured muscle activity in a similar window period (100 to 150 ms) found that muscle preactivation is affected by running speed,21 shoe material22 and level of running proficiency.23 It has been speculated that preactivation increases the stiffness of the tendon–muscular system to tolerate and absorb impact forces.24 Therefore, the reduced relative activation of TA in the injured group (table 6) could indicate an increase in tendon loading during initial contact. It is estimated that the peak load of the Achilles tendon during running is around six to eight times the body weight.2 Therefore, the increase in the loading of the Achilles tendon due to a decrease in the activity of the muscles recruited for shock absorption could be interpreted as a negative adaptation for the Achilles-injured runners. However, further prospective studies are needed to investigate whether this result is an adaptive response to injury or an aetiological causative factor. It is plausible to suggest that, during the rehabilitation period, training methods should be explored as possible mechanisms to stimulate muscle activity and reduce internal load.
During the contact phase the main role of muscle activity is to alter skeletal position and velocity.18 This study has shown that relative RF activity during the first 100 ms and KROM were reduced in the injured group (tables 5, 6). RF acts eccentrically during the early stance phase to restrain the movement of the tibia as the knee flexes and it is an important muscle for absorbing impact during the stance phase.25 The reduction of KROM in the injured group during the stance phase could reflect a weakness of the quadriceps during eccentric actions,26 and this is supported by the observation of lower IEMG activity of the RF during the stance phase observed in this group.
Another muscle affected during contact phase was the GM. The GM is an important muscle which stabilises the hip with respect to the thigh during early stance phase. Weak hip abductors have been associated with the iliotibial band friction syndrome.27 The relationship between weak GM muscles and Achilles tendinopathy is not clear, but a weak GM muscle could result in adduction of the femur and internal rotation of the tibia, possibly increasing pronation. Pronation was not measured in this study because it has been reported that there is an average error of 63% of frontal plane and 70% on transverse plane between skin markers and bone markers on three-dimensional running kinematics, compared with 21% on the sagittal plane (plane of movement analysed in this study).28 However, in a study using two-dimensional kinematics, higher peak pronation was found in runners with Achilles tendinopathy.1
In this study we also found a trend (significant before correction) of reduced PE muscle activity during the first 100 ms after contact phase in the injured group (table 6). This result may be related to a reduction in joint stiffness and ankle joint lateral stability in this group. Similar results were found in participants with functional ankle instability where post-heel strike IEMG activity of PE during walking was significantly lower than in a control group.29
Eight of the 21 participants in the injured group presented with an injury on the left limb. Although some studies have found no difference between left and right limb kinetic and kinematic parameters in non-injured runners,30 others found asymmetry between the dominant and non-dominant leg on EMG parameters during walking.31 Therefore, we suggest that further studies should balance left and right side measurements in the control group to match the injured population.
In conclusion, this study shows that muscle activity and kinematic data can distinguish runners with Achilles tendinopathy from uninjured runners. Additionally, considering that impact forces were similar between the two groups and that muscle activity was lower in the injured group before and during stance phase, we can speculate that the injured group were experiencing lower shock absorption than the uninjured group. It may be postulated that rehabilitative exercises or other mechanisms (e.g. footwear) that increase muscle activity may be beneficial for runners with Achilles tendinopathy.
What is already known on this topic
Kinetics and kinematics parameters are commonly associated with running injury. However, only recently has muscle activity been suggested as a variable that may play a role in the aetiology of running injury.
What this study adds
Runners with Achilles tendinopathy present with a lower muscle activity of tibialis anterior, rectus femoris and gluteus medius during the running cycle. This may indicate that rehabilitation exercises that promote an increase of muscle activity during the running cycle may be beneficial for treatment.
Acknowledgments
The authors would like to acknowledge the Medical Research Council of South Africa for financial support throughout the study, São Paulo Alpargatas for the donation of the running shoes and the University of Worcester for offering the first author time to write the article.
REFERENCES
Footnotes
Competing interests: Liane Azevedo works as a consultant for São Paulo Alpargatas.
LA was affiliated to the UCT Exercise Science and Sports Medicine Research Unit, Department of Human Biology, Faculty of Health Sciences, University of Cape Town at the time of the research.