Article Text

Abstract
Objectives: To culture collagen-producing cells derived from skin fibroblasts and o evaluate prospectively the safety and potential use of this cell preparation for treatment of refractory lateral epicondylitis in a pilot study.
Design: Prospective clinical pilot study.
Setting: Institution-based clinical research.
Patients: A total of 12 patients (5 men and 7 women; mean age 39.1 years) with clinical diagnosis of refractory lateral epicondylitis.
Interventions: Laboratory-prepared collagen-producing cells derived from dermal fibroblasts were injected into the sites of intrasubstance tears and fibrillar discontinuity of the common extensor origin under ultrasonography guidance.
Main outcome measures: The outcome assessment was performed over 6 months. The Patient-Rated Tennis Elbow Evaluation (PRTEE) scale was used to assess pain severity and functional disability. Tendon healing response was measured using four criteria on ultrasonography: tendon thickness, hypoechogenicity, intrasubstance tears and neovascularity.
Results: Cell cultures rich in collagen-producing cells was successfully prepared. After injection, the median PRTEE score decreased from 78 before the procedure to 47 at 6 weeks, 35 at 3 months and 12 at 6 months after the procedure (p<0.05). The healing response on ultrasonography showed median decrease in: (1) number of tears, from 5 to 2; (2) number of new vessels, from 3 to 1; and (3) tendon thickness, from 4.35 to 4.2 (p<0.05). Of the 12 patients, 11 had a satisfactory outcome, and only one patient proceeded to surgery after failure of treatment at the end of 3 months.
Conclusions: Skin-derived tenocyte-like cells can be cultured in the laboratory to yield a rich preparation of collagen-producing cells. Our pilot study suggests that these collagen-producing cells can be injected safely into patients and may have therapeutic value in patients with refractory lateral epicondylitis.
Statistics from Altmetric.com
First described as a clinical condition by Runge in 1873, “tennis elbow” (TE), clinically known as lateral epicondylitis or common extensor origin (CEO) tendinosis, describes a group of symptoms occurring around the lateral elbow.1 It is a painful pathological condition with its origin in the common wrist extensor muscles at the lateral epicondyle and is the most commonly diagnosed elbow condition, affecting 1–3% of the general population each year.2 3 A wide variety of aetiological factors may be involved including overuse, repetitive forceful movements, misalignments, training errors, poor circulation, strength deficits or muscle imbalances.4–6
Although the exact cause of this disorder has not yet been elucidated, it is thought to be a degenerative process resulting in vascular proliferation and hyaline degeneration of the extensor carpi radialis brevis (ECRB) and extensor digitorum communis (common extensor origin) at the lateral epicondyle.2 Overuse leads to microscopic tears in the origin of the ECRB with subsequent lack of repair in the tendons and replacement with immature reparative tissue.7 Histopathological examination shows a degenerative, non-inflammatory process with tissue characterised by the presence of disorganised collagen with immature fibroblasts and neovascularisation, a process described as angiofibroblastic tendinosis.2 7 8
There is a clear lack of consensus about the optimum management despite the advances in understanding of the causes of CEO tendinosis. Numerous options have been advocated, including rest, non-steroidal anti-inflammatory medication, bracing, physical therapy, iontophoresis, botulinum toxin, extracorporeal shock-wave therapy, buffered platelet-rich plasma, dry needling and autologous blood injection.9–12 In most patients (>90%), CEO tendinosis is successfully treated non-operatively, with only a few patients requiring surgical management. Attention has been directed primarily on pain management (analgesics); use of anti-inflammatory medications for this degenerative, non-inflammatory process (corticosteroids); or the stimulation of reparative scar tissue (dry needling and autologous blood injection). The resultant scar tissue formation these treatment options cause lacks the structural properties and mechanical strength of a normal tendon, and none of these treatment strategies has attempted to regenerate tendon tissue for reinforcement of tensile strength.
By definition, stem cells are able to self-renew, exist in an undifferentiated or unspecialised state, and are capable of differentiation or specialisation along multiple lineages. Recent studies indicate that nascent stem cells exist within various adult tissues, including bone marrow, brain, dermis, periosteum, skeletal muscle, synovium, trabecular bone and vasculature.13–16 Recently, de Mos et al showed that human tendon cells possess an intrinsic differentiation potential and also suggested a possible role for altered tendon-cell differentiation in the pathophysiology of tendinosis.17 Previous studies in animal models have shown that regeneration of tendon tissue can be achieved by implantation of tendon or tendon-like (tenocyte) cells that have the ability to lay down collagen matrix.18 19 Similarly, bone marrow-derived mesenchymal stem cells have also been used for tendon-tissue engineering and tendon regeneration in horses.20 21
In this study, we evaluated the use of collagen-producing tenocyte-like cells derived from skin fibroblasts as a potential treatment option for refractory and chronic CEO tendinosis. Our hypothesis was that cells derived from dermal fibroblasts can be cultured under standard laboratory conditions to yield a cell preparation rich in collagen-producing tenocyte-like cells. The second goal of our investigation was to evaluate the safety and potential of this tenocyte-like cell culture preparation as an alternative treatement for CEO tendinosis. To our knowledge, this pilot study is the first report in the literature on the treatment of CEO tendinosis using the implantation of collagen-producing cells derived from skin fibroblasts in humans.
METHODS
Institutional review board and ethics committee approval were obtained for the study and all participants gave informed written consent before taking part.
Participants
We performed a prospective pilot clinical trial in the outpatient and radiology departments at a tertiary referral orthopaedic hospital. During the period January 2007 to March 2007, patients were referred by a surgeon specialising in the treatment of the upper limb to received therapy for refractory CEO tendinosis using tenocyte-like cell injection. In total, 12 consecutive patients (five men, seven women; mean age 39.1 years (range 29–48) with refractory CEO tendinosis were included into the study. The mean duration of symptoms was 18.1 months (range 6–24 months).
Clinical assessment
The clinical diagnosis of the TE was based on pain with point tenderness at the lateral epicondyle, with resistant wrist dorsiflexion and with passive wrist flexion. Criteria for inclusion were symptomatic patients with a clinical diagnosis of TE for at least 6 months, failure of conservative treatment including rest, physiotherapy and analgesics, and confirmation of the diagnosis on MRI.
Magnetic resonance imaging
The clinical diagnosis of CEO tendinosis was confirmed with MRI using a standard imaging protocol. The radiological interpretation was performed by consensus of two consultant musculoskeletal radiologists (FA and DC) experienced in sport-trauma MRI. The diagnosis of CEO tendinosis was based on the presence of high-signal intensity focus on T2-weighted fat-suppressed images in the extensor carpi radialis brevis tendon at the lateral epicondyle. Additional findings including marrow oedema at the lateral epicondyle, a mild increase in joint fluid (which may have been physiological) and increased signal intensity at the brachioradialis tendon and radial collateral ligament were also identified.22–24
Exclusion criteria are outlined in the box.
Exclusion criteria
Trauma to the affected elbow in the preceding 6 weeks
History of elbow instability
Previous elbow surgery
Any other pathology involving the affected upper limb or cervical spine pathology
Use of oral/systemic steroids
MRI showing:
Full-thickness tear of the common extensor origin
Any intra-articular pathology or chondral defects
Lateral collateral ligament tears
Patients with contraindication to injection therapy
Patients with bleeding diathesis or on anti-coagulant
Local or systemic infection
Prosthetic elbow joint
Outcome measures
We used the Patient-Rated Tennis Elbow Evaluation (PRTEE) scale and ultrasonography (US) imaging as the outcome measures at 6 week, 3 month and 6 months after treatment.
PRTEE Scale
Patients were asked to rate their pain severity and functional disability on PRTEE scale before the procedure and after the injection at 6 weeks, 3 months and 6 months time intervals. PRTEE scale (formerly known as the Patient-Rated forearm Evaluation Questionnaire) is a validated TE disability questionnaire developed by Overend et al.25 It consists of two subscales (including pain and function) and are scored with a range from 0 to 10 (0, no pain or difficulty to perform various activities of daily living; 10, meaning worst possible pain or inability to perform).
Ultrasonography
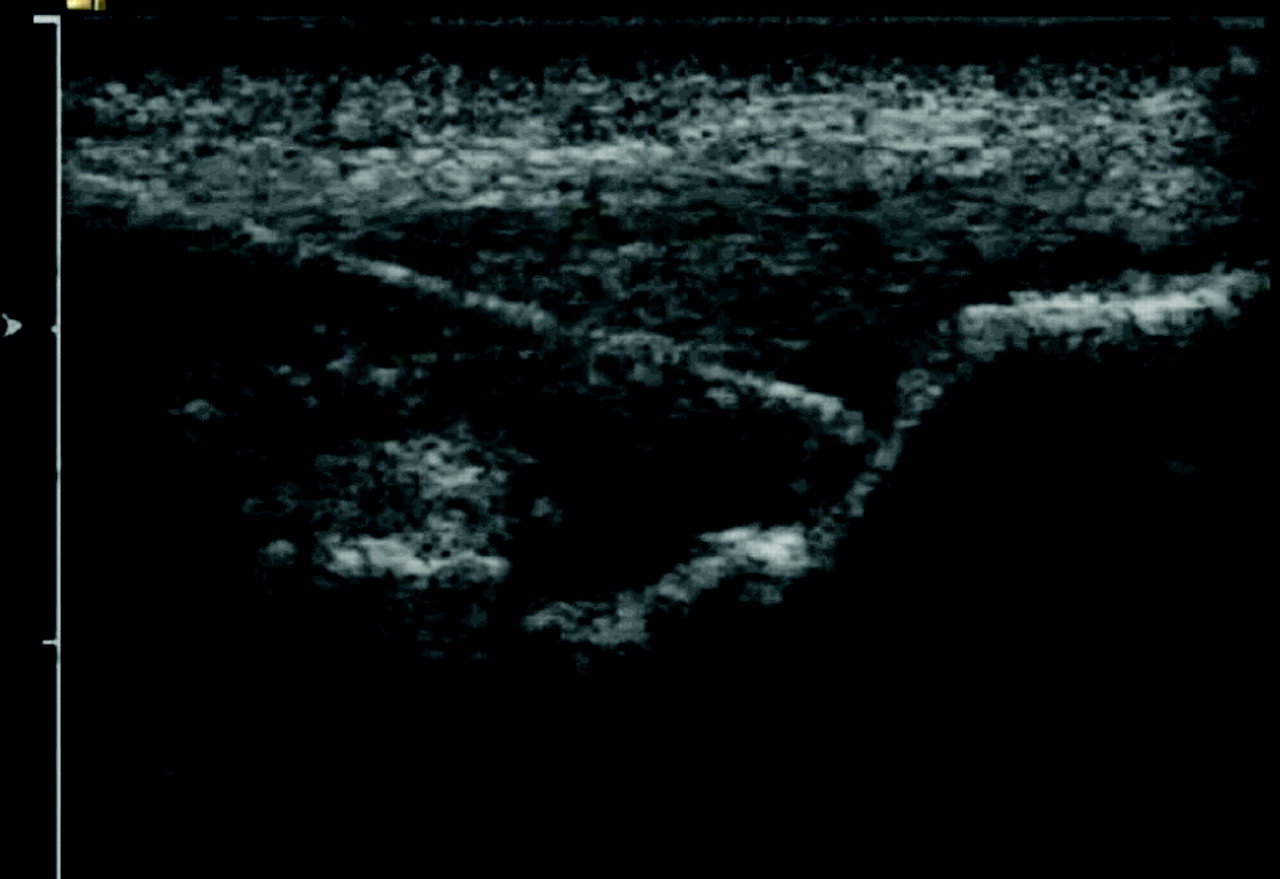
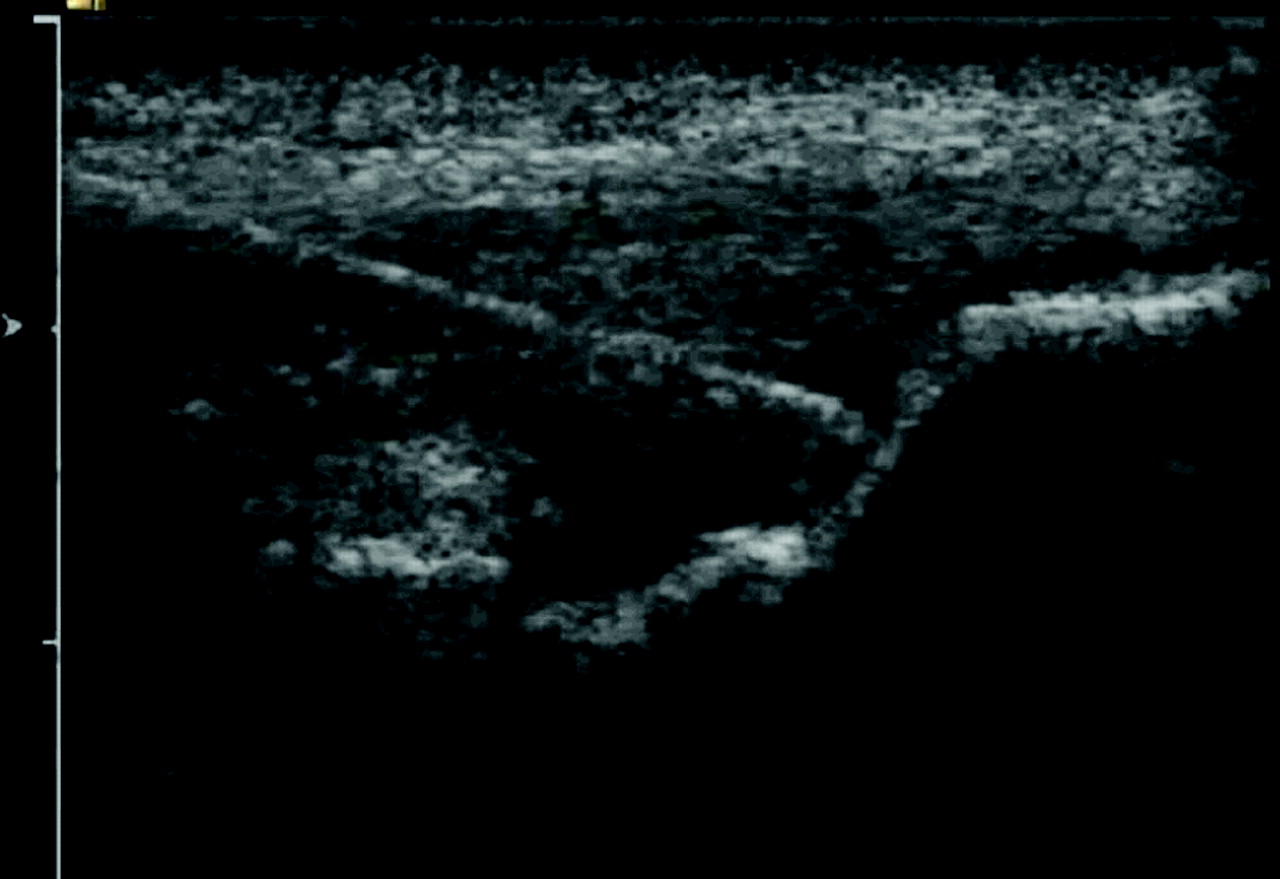
All patients were examined by US (Philips, Eindhoven, The Netherlands) before the injection and thereafter at 3 and 6 months. Sonographic evaluation of the extensor tendon origin was performed and the diagnosis of tendinosis was confirmed according to four US criteria (fig 1): (1) tendon thickness or size, (2) echo texture, (3) fibrillar discontinuity (tears) and (4) neovascularity.26 Tendon size was measured by placing one marker on the tendon surface and another marker on the cortical bony interface of the lateral epicondyle at the tendon mid-portion. For the purpose of reproducibility, this was performed 5 mm from the joint margin. Echo texture was evaluated by identifying areas of hypoechoic change within the tendon, which had otherwise preserved its fibrillar pattern. A semi-quantitative score of 1–10 was awarded (0, normal echogenic tendon; 10, diffuse hypoechoic change seen throughout the entire common tendon origin). Discrete tears within the tendon were identified as focal areas of anechoic change with no intact fibres or as distinct hypoechoic planes of fibril discontinuity. The number and size of these tears was recorded. In addition, neovascularity was assessed by the maximum number of colour pixels occupying the tendon origin and scored between 1 to 10 (0, no vessels (normal tendon); 10 (⩾10 blood vessels)).

Ultrasonography image showing a hypoechoic area of fibrillary discontinuity (tear) with increased vascularity on colour Doppler at the common extensor origin.
Cell preparation
A 4-mm skin sample was obtained from lateral side of the hip using a 4-mm punch biopsy needle, after infiltration of the skin with local anaesthetic (lidocaine 1%) under aseptic technique. Once obtained, the skin sample was placed in cell transport medium (DMEM/F12 plus gentamicin) and sent to a Good Manufacturing Practice (GMP)-compliant cell-culture facility with manufacturing authorisation for human fibroblasts under standard conditions of 4–10° refrigeration. According to the regulations for cell therapy in humans, 10 ml of whole blood was also collected from the antecubital fossa and sent for exclusion of syphilis, hepatitis B and C virus, and HIV as per regulatory guidelines. A bar-coded computer tracking system was used to ensure that there was no mix-up of patient-derived material.
Within the GMP clean room, the sample container was opened within a biosafety laminar flow hood (class A) chamber and a sterility test was performed. The skin sample was washed in phosphate-buffered saline (PBS), underwent mechanical disintegration, after which the connective tissue was digested by adding a 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES)-containing medium with collagenase type 1 and fetal calf serum. PBS was added during the next day (14–24 hours from the time of sampling) and the connective tissue was pelleted by centrifugation. The pellet was resuspended by adding fibroblast medium to each 50 ml tube. The medium with the connective tissue pieces was transferred to tissue-culture flasks, which were incubated in an incubator (5% CO2, 37°C). FCS 15% served as a medium additive for the propagation of connective tissue cells. The serum originates from a country free of bovine spongiform encephalopathy and is covered by a European Drug Quality Directorate certificate.
Injection technique under ultrasonography guidance
All US assessment and injections were performed by a single musculoskeletal radiologist with >12 years’ experience (DC). US was used to identify intrasubstance tears and clefts within the injured tendon. At the start of the procedure, 2 ml bupivacaine 0.25% were infiltrated along the surface of the tendon using a 23G needle. Following this, the dose of cell preparation was slowly introduced into the site of tendinosis and fibril discontinuity (fig 2), using a double-chambered delivery system containing an equal amount (2 ml) of cell preparation injectate in one arm and centrifuged plasma concentrate in the other arm. The total procedure time was kept to minimum ranging from 2–4 minutes. We introduced approximately 10×106 collagen-producing cells (approximately 2 ml) into the intrasubstance tears within each tendon. Immediately after injection, the patient was kept in a supine position without moving the arm for 5 minutes. Patients were sent home with instructions to limit their use of the arm for next 24 hours and then to perform normal activities but avoiding lifting heavy weights. The use of non-steroidal medication and any pain-provoking activities were prohibited.
Ultrasonography-guided needle insertion into the area of fibril discontinuity (tear) in the common extensor origin at lateral epicondyle.
Statistical analysis
The analyses compared the results before treatment with those at each of the subsequent time periods. The same subjects were measured on >1 occasion, giving rise to paired data. Comparison was made between the PRTEE scores before and after the procedure and the US findings at 6 weeks, 3 months and 6 months. The Kolmogorov–Smirnov test was used to assess the normality of all the data including the PRTEE scores and the ultrasonography findings. Both the PRTEE scores and ultrasonography findings did not follow a normal distribution and were therefore analysed using the Wilcoxon matched pairs test. The figures reported are median and interquartile range to summarise the measurements, and p values significance. All statistical analysis was performed using SPSS for Windows, V.12.0 (Chicago, Illinois, USA) and p <0.05 was considered significant.
RESULTS
There was no loss to follow-up during the study and all patients maintained compliance for the study protocol. None of the patients were positive for syphilis, hepatitis B and C or HIV.
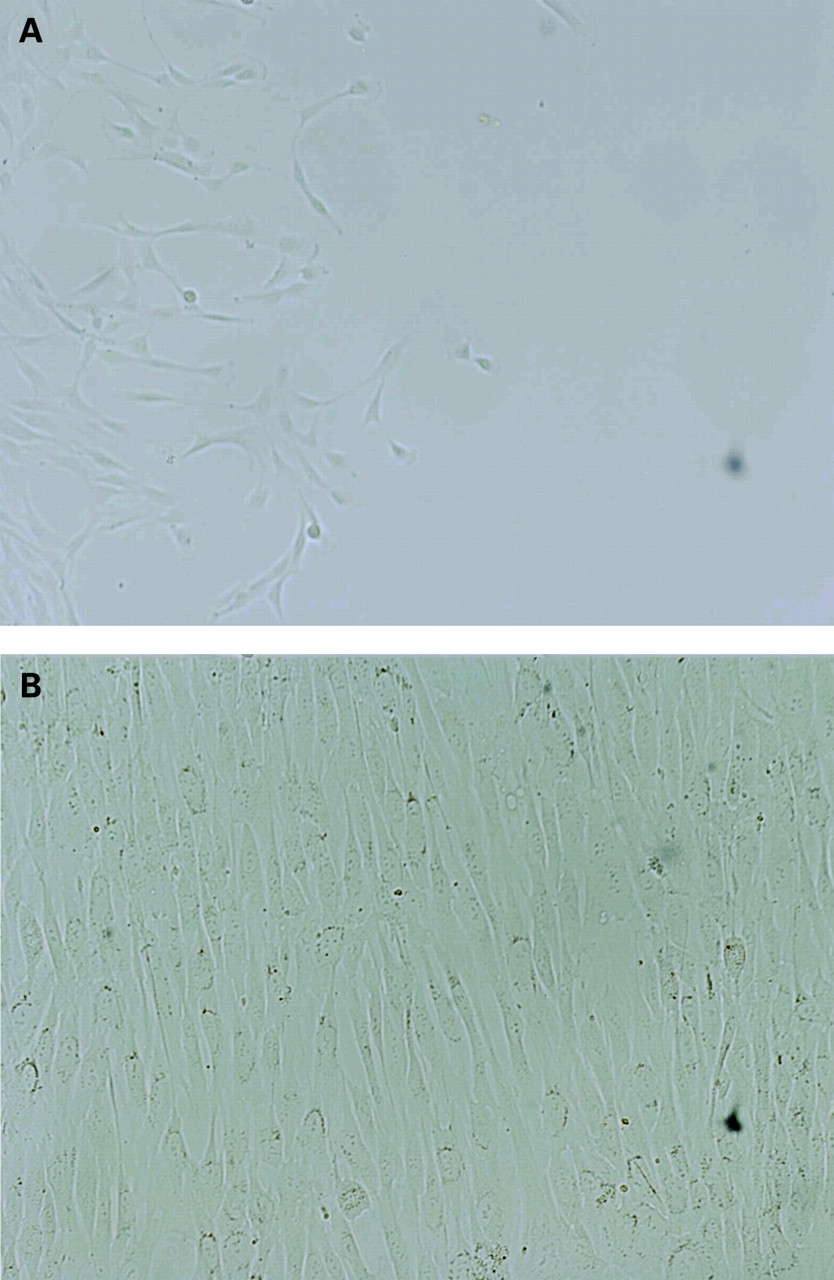
In the GMP facility, tenocyte-like cells were successfully grown in culture (fig 3). These cells showed exponential growth in cell medium culture and approximately 10×106 cells were grown over a 4-week period. These cells exhibited elongated nuclei and spindle-shaped cytoplasm, characteristic of a fibroblast-like morphology. After expansion, the cells were characterised by flow cytometry and the releasing criteria for tenocyte-like cells included positive CD90 marker and mean viability (by 7-amino-actinomycin D (7AAD) staining) of 90 (SD 10)%. In an ex vivo model, where linear periodic stretch was transferred to these cells over a plasma scaffold, increased collagen type I and type III expression was seen. Similar results occurred in other fibroblast-like cells.
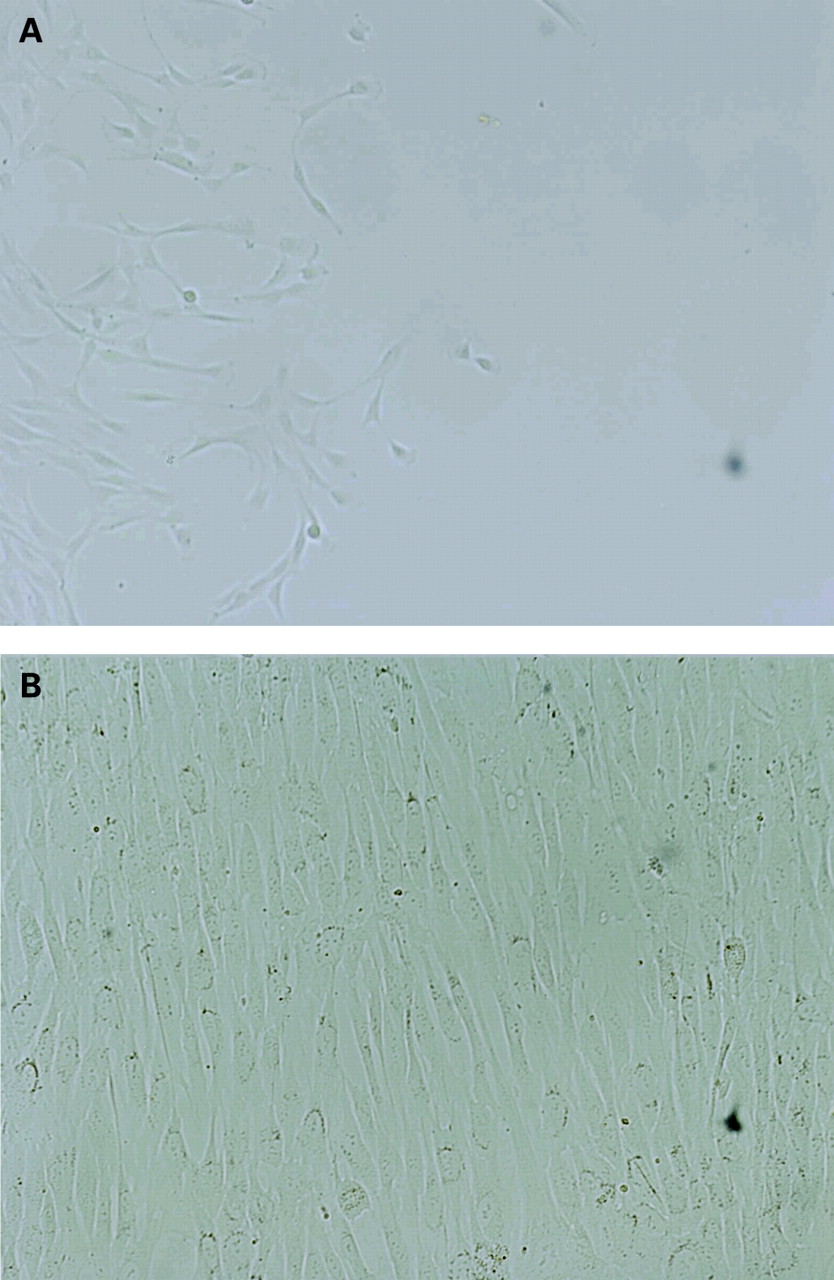
Cells in the laboratory at (A) 5 and (B) 14 days.
Each subject had only one injection of cells. Of the 12 patients, 11 (91.6%) patients expressed satisfaction with both the procedure and the outcome and 10 (83.3%) were ready to undergo the procedure again if needed. No infection, reflex sympathetic dystrophy, elbow flexion contracture or other untoward effects occurred. One patient failed to improve satisfactorily at the end of 3 months and eventually underwent surgery for CEO tendinosis.
The median PRTEE score before injection was 78 (interquartile range 71–88), at 6 weeks had decreased to 47 (17.5–80) and further reduced to 35 (0–42) at 3 months. At the end of 6 months, the median PRTEE score was 12 (0–25). There was a significant difference between the PRTEE scores at 6 weeks and 3 months (p = 0.01), and at 3 months and 6 months (p = 0.003) (table 1).
There was a significant difference between the pre-treatment values and the values at each of the other subsequent times (p<0.05 for all). On the PRTEE scale, the values at the 3 months and 6 months interval were significantly lower than the pre-treatment values in all cases. At the end of 6 months, the scores in 11 patients were still lower compared with the scores at 6 weeks and 3 months.
US examination at 3 and 6 months (fig 4) showed a tendency for tendon appearance to change towards normality with a decrease in tendon size, restoration of the fibrillar pattern, and near-total resolution of the intrasubstance tears. Neovascularisation was reduced, but still identifiable at the end of 6 months. The results of the US assessment (before and at the end of 6 months) are summarised in table 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ultrasonography before and after treatment in a 53-year = old patient with a 22 = month history of refractory CEO tendinosis: (A) before treatment, showing a thickened tendon with diffuse hypoechoic change, interstitial tearing and neovascularity; (B) at 6 months after treatment, showing tendon remodelling with restoration of the normal echogenic fibrillar pattern and resolution of the interstitial tear.
Histopathological correlation of the repaired tendon was available only for the single patient who underwent open surgery. This surgical specimen showed evidence of cellular necrotic debris and inflammation with minimal healing response in the tendon tissue.
DISCUSSION
Chronic overuse injuries such as CEO tendinosis are the result of multiple microtrauma events that cause disruption of the internal structure of the tendon and degeneration of the cells and matrix, which fail to mature into normal tendon.2 Although the tensile strength of the healing tendon improves over time, it does not reach the levels of uninjured, normal tissue. The process of tendon repair is a complex orchestrated series of physiological events and a number of factors may interfere with this healing process.
A variety of scaffolds and cell therapies has been proposed in tendon tissue engineering. The two cell types most commonly identified are cells derived from normal tendon and stem cells of mesenchymal origin. The latter have been used with some success to treat acute tendon ruptures in horses.27–29 Our reasoning for using collagen-producing cells derived from dermal fibroblasts was based on a number of factors: they are available in quantities of hundreds of million cells per individual, can be accessed through a relatively non-invasive method, have the potential to express the same scaffold proteins as tenocytes, can be transplanted in an autologous manner, and can be manufactured in a controlled, large-scale procedure in accordance with regulatory guidelines. Laboratory studies in animal models have suggested that fibroblasts have the potential to heal tendon defects.30 31 From a 4 mm skin biopsy, we have been able to grow approximately 10×106 collagen-producing cells with similar appearance and behaviour to tenocytes. We chose to deliver these cells embedded in a plasma concentrate, so that this mixture could fill and set like a gel within the intrasubstance defects and tears within the injured tendon. Furthermore, this would make use of growth factors (platelet-derived, eye-derived, fibroblast-derived) within the plasma concentrate to encourage collagen deposition and tendon regeneration.11
In our study, we have tried to simulate the normal healing process by injecting collagen-producing cells from skin fibroblasts into the site of tendon injury. Our pilot study shows that this can be performed safely, with no significant adverse events reported other than by one patient who had continued intense pain at 3 weeks and eventually required surgery. Furthermore, 11/12 patients reported at least modest improvements in their symptoms, and ultrasonography confirmed features of healing with a tendency for the interstitial tears to heal and the tendon architecture to return towards normality. US performed at regular intervals showed a decrease in tendon size, restoration of the fibrillar pattern and resolution of the intrasubstance tears. There was some decrease in the amount of neovascularisation, although this remained present to varying degrees.
In the laboratory, we have observed the phenomenon in which collagen-producing cells derived from patient skin have a tendency to orient along the lines of applied tension. In rehabilitation practice, there is a strong argument for beginning to load the implanted tendon soon after treatment to aid in the longitudinal orientation of collagen fibres seen in a normal tendon. Indeed, previous studies have shown that physiotherapy can be an effective option for the conservative management of CEO tendinosis.32 33 To avoid a potential bias in results, physiotherapy was not included in our study protocol.
We injected our cells using a dual-syringe technique so that the cell preparation would be mixed and set within a plasma concentrate. The plasma concentrate alone has been shown to stimulate tendon healing, so we do not know how much of the improved PRTEE scores and changes in US appearance were due to the cell therapy alone. Furthermore, the follow-up US was performed by a solitary sonographer, hence we have no measure of interobserver variability and the introduction of possible bias.
There are other limitations to our study. Our pilot study was limited to only 12 patients to demonstrate the safety and possible potential of this novel procedure, before undertaking extensive efficacy trials. In addition, we are uncertain about the exact nature of the collagen-producing cells derived from the skin (there are no tenocyte markers) and we do not completely understand the cellular and biological processes taking place within the tendon tissue. Our discussed assumptions were based on in vivo studies performed on animal models. Furthermore, we have little histopathological correlation as only one patient failed the treatment process and underwent surgery. The results of our pilot study are encouraging and we believe that further research to explain the exact cellular and molecular level mechanisms of tendon healing using collagen-producing cells derived from dermal fibroblasts would be interesting. In addition, the potential application of this technique in other tendonopathies should be explored.
CONCLUSION
Our pilot study suggests that collagen-producing cells derived from skin can be isolated and cultured into tenocyte-like cells in the laboratory under standard conditions. These cell preparations can be implanted safely into the tendons of a group of patients with refractory CEO tendinosis. Further research using a control group, a larger patient population and histopathological correlation is recommended.
REFERENCES
Footnotes
Funding: We thank the British Society of Skeletal Radiologists for their funding for the study design.
Competing interests: None.