Article Text

Abstract
Background: The increase in popularity of soccer and expectations from players make significant numbers of soccer injuries conceivable. Concerns have been expressed about the demand placed on the modern-day footballer and translation of these physical and mental demands into injuries. Despite the popularity and importance of the game of soccer in Benin, no detailed study on the occurrence of soccer injury has been carried out.
Objective: The study sets out to describe and assess the determinants and effects of soccer injuries.
Methodology: Seven clubs (196 players) from the premiership, professional, national and state amateur clubs were studied using a descriptive cross-sectional study design. A pre-designed semi-structured questionnaire and key informants interview guide were used for data collection. Descriptive and inferential statistics were used in the analysis, with significant levels generally taken at 5% level of significance.
Results: A total of 196 players sustained 204 injuries with a prevalence rate of 81.6%. More injuries were recorded during matches (46.1%) than during training (36.8%). Injuries occurring by body contact constituted 62.3% of the total injuries. The ankle (25%) was the most affected site, followed by the knee (20.1%), while sprain injury (33.3%) and strain (13.2%) were the commonest injury types. Moderate injury (28.9%) was the highest form of severity recorded. Recurrent injury accounted for 38.8% of injuries, occurring more in training (44.9%) than in matches (36.7%). A greater percentage (86.8%) of the injuries were traumatic in nature, with tackling (44.6%) being the commonest mechanism. Defenders (34.3%) and strikers (31.4%) had higher injury occurrence. The association between the player’s role and the mechanism of injury was significant (p = 0.02), while that between weather condition and injury type was very significant (p = 0.004). Moreover, the association between experience and mechanism of injury was extremely significant (p<0.001). The study also shows that injury has economic, physical and psychological impacts on players.
Conclusion: A prevalence rate of 81.6% was recorded. Sprain was the leading injury type, while the ankle was the most affected anatomical site. Factors such as weather, previous injury, experience, role, and activity tend to influence injury occurrence. Soccer injury also has economic, physical and psychological implications. It is therefore recommended that preventive measures such as adequate treatment of injuries, full rehabilitation after injuries, use of protective equipment, appropriate exercises and warm-ups, continual team education on injury managements and skill improvement, etc., be utilised and enforced to protect this group of sport workers.
Statistics from Altmetric.com
Football (soccer) is the most popular sporting event in the world, attracting the highest number of spectators; it is also big business.1–3 In recent times, governmental, private and even religious bodies have invested in soccer in Benin City and Nigeria. The Federation of International Football Association (FIFA) has expressed its concern about the demands placed on the modern-day footballer and translation of these physical and mental demands into injuries.4 The overall level of injury to professional footballers is around 1000 times higher than in industrial occupations generally regarded as high-risk.5 6
To enable prevention programmes to be implemented requires quantification of the extent of the problem. Therefore, we studied the distribution of football injuries, their associated factors, and prevalence and potential effects.
METHODOLOGY
The study was conducted in Benin City, the capital of Edo State in the Nigerian Oil-rich South-South Geopolitical Zone. Benin City has a population of 3 218 332. There were about 27 registered male football clubs in Benin in 2006, with over 945 registered players. We adopted the methodology recommendations of the Injury Consensus Group of the Federation Internationale de Football Association Medical Assessment and Research Centre (FMARC), and “UEFA model on practical guideline for epidemiological studies of football injuries”.4 7
A cross-sectional study design was used for the study, which involved amateur and professional soccer players in Benin City who participated in the 2006 national soccer season (generally between February and December).
A sample size of 195 was calculated using the formula for descriptive study and a prevalence of 85% of injury from an earlier study.8 One hundred and ninety-six players were drawn from seven registered football clubs in Benin city as follows: one club from the State amateur division, four from the National amateur divisions, one from the National professional division and one from the National premiership division. The selection was purposive, based on the recommendation of Edo State Football Association that national league teams were more organised, reliable, and consistent, and moreover were reachable during the period of the study. All registered members of the selected clubs who played in the 2006 football season were selected based on the fact that they had equal chances of participation according to the coaches. Written informed consent was obtained from clubs and management; verbal assent was provided by players.
A pre-designed questionnaire was used in collecting information from players, while a key informant’s interview guide was used for the key informants, namely club officials and the team physicians. Information collected from players included personal data, exposure types, game situation, field and weather conditions, injury types, injury locations, injury mechanism, severity, treatment, psychological state, effect and expenditure, while that of key informants included their designation and experience, injury management and annual injury expenditure of the clubs etc. Generally, the questionnaires were self-administered after relevant explanations. However, where this would not have been effective, coaches or other club officials administered the questionnaire to players after instruction. Supplementary injury reports for two of the teams — Bendel Insurance and D.C. International football clubs — were obtained from injury records of the teams. Injuries occurring during leisure time or other sports were not recorded.
Statistical packages were used, including SPSS (version 10). Descriptive statistics were calculated as appropriate. The level of significance was set at p<0.05.
RESULTS
A total of 206 players were enlisted in the study. However, only 196 (95.15%) responded, with an attrition rate of 4.85%.Though about 233 injuries were indicated, only 204 (87.6%) were valid. The invalid injuries were discarded due to poorly completed questionnaires that lacked other essential information necessary for data processing and analysis. Hence the study was based on 204 injuries recorded during the 2006 football season. The total number of injuries sustained exceeded the number of players involved due to the tendency to sustain multiple injuries. The general results are presented as follows.
The table showed that prevalence tends to increase as level of participation increases, with 78.6% in the state amateur league and 100% in the professional and the premiership leagues. However, the slight departure from the above statement in the National amateur division 3 side may be due to an early exit of the latter from competition.
Sprain was the commonest injury (33.3%), followed by strain (13.2.%). Bruises (9.8%) were the third commonest injury, followed by laceration (6.9%), while injuries classified as others (2%) and lumbago (0.5%) were the least common. Supplementary hospital data collected from Bendel Insurance also had sprain (48%), strain (21%) and bruises (6%) as the commonest injuries, consistent with the findings in table 2. Body contact injuries gave rise to 62.3% of injuries, traumatic injury led to 86.8% of injuries and overuse injury accounted for 13.2%. Traumatic mechanisms of injury involved include tackling/being tackled (44.6%), jumping and landing (11.8%), turning and twisting (10.8%), running (7.4%), shooting (8.8%) and collision (2%).
The ankle was the most affected region (25%), followed by the knee (20.1%) then the thigh (13.2%). The elbow was the least injured site (2%), followed by the wrist and the abdomen (2.5%). However, there was no significant difference in the frequency of these injuries between match and training.
Injury severity was measured on a time-loss basis (number of absences from participation). Moderate injuries (8–28 days) have the highest percentage (28.9%) of occurrence followed by mild injuries (4–7 days) with 21.6% and then minimal injuries (1–3 days) with 18.6%.Severe injuries (>28 days) accounted for 12.3%.
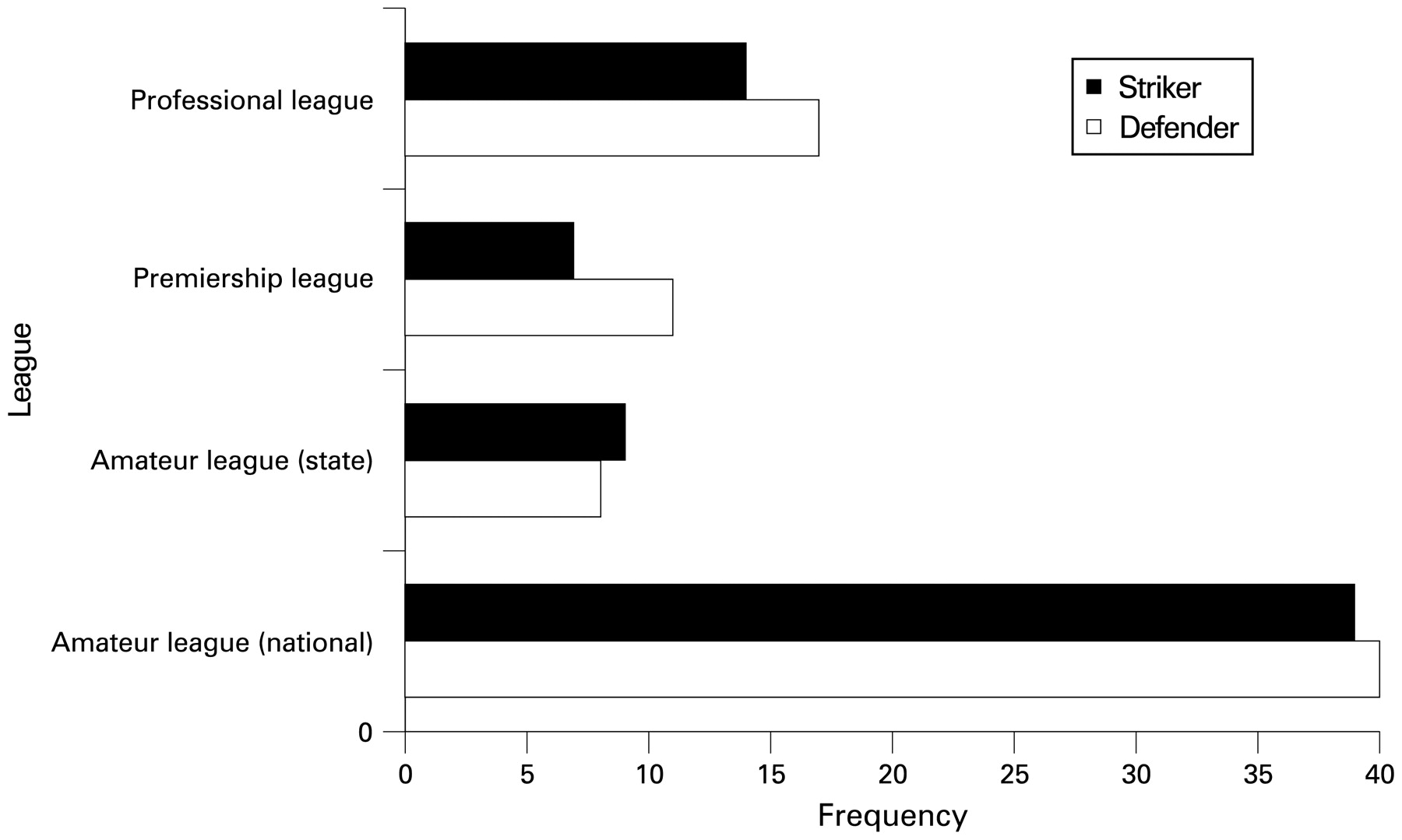
That defenders sustained higher number of injuries than other positions (roles) was consistent within the national league. However, while defenders tended to sustain more injuries in the premiership league (47.6%), the professional league (47.1%) and the national amateur league (30.9%), strikers (34.7%) ranked higher than defenders (30.4%) in the state league side that participated in this study.
Most of the injuries (78.9%) occurred under weather conditions described as hot or sunny, while about 20.1% occurred in rainy or cold weather. Association between weather conditions and injury type was very significant (χ2 = 13.37, p = 0.004). Field conditions described as either hard or dry gave rise to 81.4% of injuries, but there was no association between field conditions and injury type (χ2 = 2.64, p = 0.24). Matches (52.9%) more than training (46.6%) accounted for more injuries, but association between exposure and injury type (χ2 = 5.39, p = 0.15), exposure and recurrent injury (χ2 = 1.19, p = 0.27) and exposure and traumatic injury(χ2 = 2.71, p = 0.1) were not significant. Defenders recorded a higher occurrence of injuries (34.3%, role-specific injury of 1.3), while goalkeepers had a lower injury occurrence (9.8%, but with higher role-specific injury of 1.4). However, while there were no associations between role and injury type (χ2 = 3.17, p = 0.53) or role and injury severity (χ2 = 10.43, p = 0.53), an association was found between role and mechanism of injury (p = 0.02). Players with 6–10 years of experience have more injuries (58.8%) than others, but associations between experience (skill) and injury location (χ2 = 5.64, p = 0.46) and between experience (skill) and injury type (χ2 = 7.68, p = 0.26) were not significant. However, association between experience (skill) and injury mechanism was extremely significant (p<0.001). About 34.8% of injuries (recurrent) were as a result of previous injury experience. About 28.3% of injuries occurred in players with a negative mind state (anxiety and fear). However, while there was no association between players’ mind state and injury types (χ2 = 1.46, p = 0.48) or between players’ mind state and traumatic injury (χ2 = 1.02, p = 0.31), an association was found between mind state and type of exposure (χ2 = 4.72, p = 0.03). Players aged 16–19 years sustained a higher number of injuries (48.5%), but there was no association between age and injury type (p = 0.17), age and injury severity (p = 0.25) or age and injury mechanism (p = 0.12).
A total of 68.7% of injuries had an adverse psychological impact on players, while 2.9% of injuries led to physical deformity. Injury also has a negative impact on availability of players for team activities. An average of 13 (SD 8.6) days, i.e. approximately 14 days, was lost for every injury sustained by a player.
DISCUSSION
The prevalence of 81.6% for injuries was high compared with other previous studies,8 9 and prevalence increased with increasing level of participation, depicting the competitive nature of events as play level increased. Sprain and strain were the commonest injuries recorded in the study. Though some studies have recorded higher frequencies of contusion10 11 and concussion,12 in most of the available literatures, sprain and strain injuries have the highest occurrence.
Traumatic injuries tend to predominate in matches (91.5%) rather than in training (84%), when compared with non-traumatic injuries. This tends to suggest the competitive nature of matches, which increases the injury-proneness of various actions in the field of play. Previous studies have also confirmed that “overuse” (non-traumatic) injury was associated more with training than with matches.13
The traumatic mechanism — tackling — which appeared in this study as the most common mechanism of traumatic injury has also been recorded in other previous studies.9 16 The findings, therefore, underscore the need for appropriate exercises, adequate warm-up and improved skills, to reduce injuries.
All body regions were subject to injury. Though knee injury ranked higher than ankle injury in the professional league side, this study generally tends to give support to several studies9 10 14 15 that have described the ankle as the most affected site. This study, with 77.5% lower extremity injuries, supported previous studies that attributed over 60% of soccer injuries to the lower extremity.5 10 12 16 17 The high rate of lower-extremity injuries may suggest a need for increased use of protective equipment.
Generally, injury severity tends to increase with movement from lower to higher leagues. This may be due to an increase in the competitive nature of the game as level of participation increases. Though some works have recorded higher occurrences of mild injury8 and slight injury,10 the findings in this study corroborate a Rwandan study which recorded moderate injury as the commonest.9 Association between injury severity and the number of substitutions because of injuries was extremely significant (p<0.001). Therefore the substitution of players following an injury may be an indication that the injury is severe.
Certain extrinsic factors are generally believed to influence injury occurrence. These include weather type, field conditions, exposure type, experience, player’s role etc. Most of the injuries recorded (81.4%) occurred on a dry or hard ground, while about 78.9% occurred in sunny or hot weather. This suggests that injury occurrence could be influenced by weather and field conditions. Previous studies have also reported a higher frequency of injuries on hard and dry ground,3 13 19 as well as when the weather was hot.19 There was a significant association between weather conditions and injury type. This may further suggest a relationship between high temperature and vulnerability of the body to injuries, since most of the injuries occurred in hot or sunny weather. Also, the highly significant association found between experience and mechanism of injury in this study is supported by many reports that the less skilled the player, the higher the injury occurrence.20 Probably more experienced players tend to acquire skills relevant to avoiding injury-prone actions. The higher injury experience of defenders followed by strikers lends credence to several past works.21 22 Defenders usually defend the goal area, which is the area of the pitch that is highly prone to injury.11 A very significant association was found between players’ position and mechanism of injury (p<0.05).Certain role-associated actions may suggest that certain positions may be more associated with some mechanisms of injuries. Defenders are usually known for their hard tackling, strikers glory in their “hot” shots, while the “wingers” are marked by their overlapping running.
Moreover, some intrinsic factors, such as age, players’ state of mind and previous injury, have also been found to be capable of influencing injuries. The mean age of approximately 20 years (late adolescent period) was low compared with 22.9 years reported for first and second division players in Rwanda.9 This may be due to the discrepancy between actual age and the so-called “football age” in Nigeria. Literature has reported an increasing risk of injury above 25 years of age, and injury types as differing by age.12 However, this study could not identify any significant association between age and injury occurrence. Some other researchers did not find any association between age and injury prevalence23 or between age and severity of injury.23
The effects of injuries could be quantified in terms of the number of days lost to injuries, physical and psychological impacts as well as the associated cost of treatment. The mean time lost per injury was roughly 2 weeks. This was, however, lower than the 22.3 days and 34.3 days reported in some studies.13 21 Absence of players could demoralise a team as well as reduce its chances of winning a competition, especially when key players are involved. Furthermore, that soccer injuries could lead to disability is confirmed by the 2.9% rate of deformity reported in this study. About 68.8% of the injuries sustained resulted in players either being demoralised or feeling dejected. Another serious effect of injury was its financial implication. The enormous sum involved has been a source of concern in previous studies. For instance, in 1999, about 6.89 billion dollars (medical, legal, liabilities, work lost, pain and suffering) was estimated in the United States.24 An estimate of treatment cost in this study showed that a total estimate of N1 002 350.00, with an average of N6903 per injury, was spent annually in Benin City. The average cost for Benin was actually lower than the global estimate of $150 (N19 050) per injury, according to a study published in 2000.2 This is understandable in consideration of the fact that most research into soccer injuries is carried out in developed countries where good economy and sophisticated medical treatment may contribute to the high cost. Generally, however, it should be expected that the cost of treatment could be higher than that calculated, if proper insurance, adequate treatment and proper documentation were to be made.
In conclusion, the present study described the extent of soccer injuries in Benin, as well as reporting factors that play a part in the occurrence of injury.16 We recommend that evidence-based preventive measures such as adequate treatment of injuries, full rehabilitation after injuries, use of protective equipment, appropriate exercises and warm-ups, continual team education on injury management and skill improvement, etc. be utilised and enforced to protect this group of sports workers.
{kind=link}
Distribution of two commonest affected positions by levels of participation.
Acknowledgments
The corresponding author hereby expresses his sincere appreciation and gratitude:
to the co-author, Prof. OH Okojie, whose encouragement, academic exposure and research experience contributed immensely to the success of this work;
to my beloved and indefatigable parents Rev. and Mrs GI Azubuike for their solid, resilient and unequalled moral and financial support;
to Dr (Mrs) Wagbatsoma (Community Health Department, University of Benin) for all her encouragement and supportive guidance;
to Dr Joseph Esemokhae and Dr Yah C, who provided assistance in the analyses of the data;
to my elder sister Gloria, and other siblings Eunice, Chiagozie, Chizoro, Chinemerem and Echezona, for the support and understanding they showed in the course of this research;
to my Christian brothers and sisters, especially the family of Dr and Mrs Emma Iwuozo, for their numerous supports and prayers for the success of this work;
to the secretary of Edo Football Association, Mr Victor, and the team physician of Bendel Insurance football club, Dr Owen, for their cooperation and extensive assistance;
to the football coaches and officials of the various football clubs, especially Coach Rapu and Ziggy (DC international), Steve and Tony (Igbino), Stanley and Patrick (St Pauls), Emeka and Idehen (Hausa), Henry and Jeff (Paulson), Ndubuisi and Izinne (Royal Domingo), Ogbede and Chico (technical adviser and secretary of Bendel Insurance) for their varied cooperation and assistance;
to the Captains of the various football clubs who made special contributions toward the project, especially Osasu (Hausa), Kamar (Bendel Insurance), Solomon (Igbino), Ibrahim (Paulson);
to the honourable team players of the various clubs who willingly participated in the research.
REFERENCES
Footnotes
Competing interests: None.