Article Text

Abstract
Exercise Associated Muscle Cramps (EAMC) is one of the most common conditions that require medical attention during or immediately after sports events. Despite the high prevalence of this condition the aetiology of EAMC in athletes is still not well understood. The purpose of this review is to examine current scientific evidence in support of (1) the “electrolyte depletion” and “dehydration” hypotheses and (2) the “altered neuromuscular control” hypothesis in the aetiology of EAMC. In this review, scientific evidence will, as far as possible, be presented using evidence-based medicine criteria. This is particularly relevant in this field, as the quality of experimental methodology varies considerably among studies that are commonly cited in support of hypotheses to explain the aetiology of EAMC. Scientific evidence in support of the “electrolyte depletion” and “dehydration” hypotheses for the aetiology of EAMC comes mainly from anecdotal clinical observations, case series totalling 18 cases, and one small (n = 10) case–control study. Results from four prospective cohort studies do not support these hypotheses. In addition, the “electrolyte depletion” and “dehydration” hypotheses do not offer plausible pathophysiological mechanisms with supporting scientific evidence that could adequately explain the clinical presentation and management of EAMC. Scientific evidence for the “altered neuromuscular control” hypothesis is based on evidence from research studies in human models of muscle cramping, epidemiological studies in cramping athletes, and animal experimental data. Whilst it is clear that further evidence to support the “altered neuromuscular control” hypothesis is also required, research data are accumulating that support this as the principal pathophysiological mechanism for the aetiology of EAMC.
Statistics from Altmetric.com
Exercise Associated Muscle Cramps (EAMC) is one of the most common conditions that require medical attention during or immediately after sports events. EAMC is particularly common in endurance events such as ultra-marathon running and triathlon.1–4 Despite the high prevalence of this condition the aetiology of EAMC in athletes is still not well understood.
Muscle cramping in athletes may occur as a result of many underlying medical conditions,5 and therefore not all athletes with muscle cramping suffer from EAMC. However, in the sports medicine literature, cramping during or immediately after exercise is more commonly referred to as Exercise Associated Muscle Cramping (EAMC),6–9 which has been defined as a “painful, spasmodic and involuntary contraction of skeletal muscle that occurs during or immediately after exercise”.10 This term will be used in this review.
The first reports of muscle cramping related to physical activity were from labourers working on steamships and in mines in hot, humid conditions more than 100 years ago.11 12 In these early reports it was noted not only that muscle cramping occurred in the heat but also that cramps were accompanied by profuse sweating.12 These early anecdotal observations led to the development of the traditional “electrolyte depletion” and “dehydration” hypotheses for the aetiology of EAMC. These case reports often related the development of cramping to physical activity performed in hot and humid environmental conditions, and this has led to the terminology “heat cramps” or “exertional heat cramps”. This terminology is still used today,5 6 13 14 often synonymously with EAMC. This is despite the fact that EAMC is known to occur in individuals exercising in moderate to cool temperatures,6 15 and exposure to extreme cold has also been associated with EAMC in swimmers.2 It has also been reported that the development of EAMC is not directly related to an increased core temperature.16 Furthermore, passive heating alone (at rest) does not result in EAMC and cooling does not relieve muscle cramps.10 It would therefore appear that heat alone is not a direct cause of muscle cramping during exercise, and therefore the term “heat cramps” is a misnomer, and its use should be discouraged.
A novel hypothesis for the aetiology of EAMC was first proposed about 10 years ago.10 This hypothesis explored evidence that altered neuromuscular control as a result of the development of muscle fatigue may be the primary factor that is associated with the development of EAMC.10 This “altered neuromuscular control” hypothesis has only recently gained some acceptance and “muscle fatigue” has, in a recent review, been acknowledged as a predisposing factor in the development of EAMC.6
The purpose of this review is to examine current scientific evidence in support of (1) the “electrolyte depletion” and “dehydration” hypotheses” and (2) the “altered neuromuscular control” hypothesis in the aetiology of EAMC. In this review, scientific evidence will, as far as possible, be presented using evidence-based medicine (EBM) criteria.17 This is particularly relevant in this field, as the quality of experimental methodology varies considerably among studies that are commonly cited in support of hypotheses to explain the aetiology of EAMC.
SCIENTIFIC EVIDENCE SUPPORTING THE “ELECTROLYTE DEPLETION” AND “DEHYDRATION” HYPOTHESES FOR THE AETIOLOGY OF EAMC
Scientific evidence in support of the electrolyte depletion hypothesis for the aetiology of EAMC
More than a century ago, it was first reported that individuals who were exposed to physical exercise in hot and humid environments could develop muscle cramps that were apparently associated with disturbances in serum electrolyte concentrations, notably hypochloraemia.11 18 Following these early reports, it has been suggested that other serum electrolyte abnormalities, including hyperkalaemia, hypomagnesaemia and hypocalcaemia, can also be associated with EAMC.12 19–21 The scientific methodology in all these studies was in the form of case reports or case series, with no control groups. There is not a single published study that has shown that serum electrolyte concentrations are abnormal in athletes at the time of acute EAMC, when compared with non-cramping control athletes.
In contrast, there are now four prospective cohort studies, from two laboratories, in two different endurance sports that have shown no relationship between serum electrolyte abnormalities and EAMC in marathon runners or triathletes8 9 16 (Drew N, MPhil Sports Medicine dissertation, University of Cape Town, 2006). In all these studies a cohort of endurance athletes (runners or triathletes) with normal pre-exercise serum electrolyte concentrations was followed and those with EAMC that occurred during the race (cramp group) were compared with a control group of athletes who did not develop EAMC. In a very consistent fashion, the results of these four prospective cohort studies have shown that in the cramp group serum electrolyte concentrations were not significantly different from those in the control (non-cramping) group at the time of the acute EAMC. Furthermore, as cramping subsided, and athletes became asymptomatic, no changes were observed in serum electrolyte concentrations (immediately post-race to recovery), indicating that recovery from EAMC was not associated with any normalisation of serum electrolyte concentration. Therefore, there is a dissociation between EAMC and serum electrolyte concentrations.8 9 Small decreases in pre–post serum sodium concentrations in the cramp group reported in these studies were within the normal range and were not of any clinical significance.8 9 These reductions in serum sodium concentrations in the cramp group were likely as a result of increased fluid intake, because the pre–post percentage change in body weight was consistently less in the cramp group.8 9 The findings in these studies are consistent and do not support any association between EAMC and abnormalities in serum electrolyte concentrations.
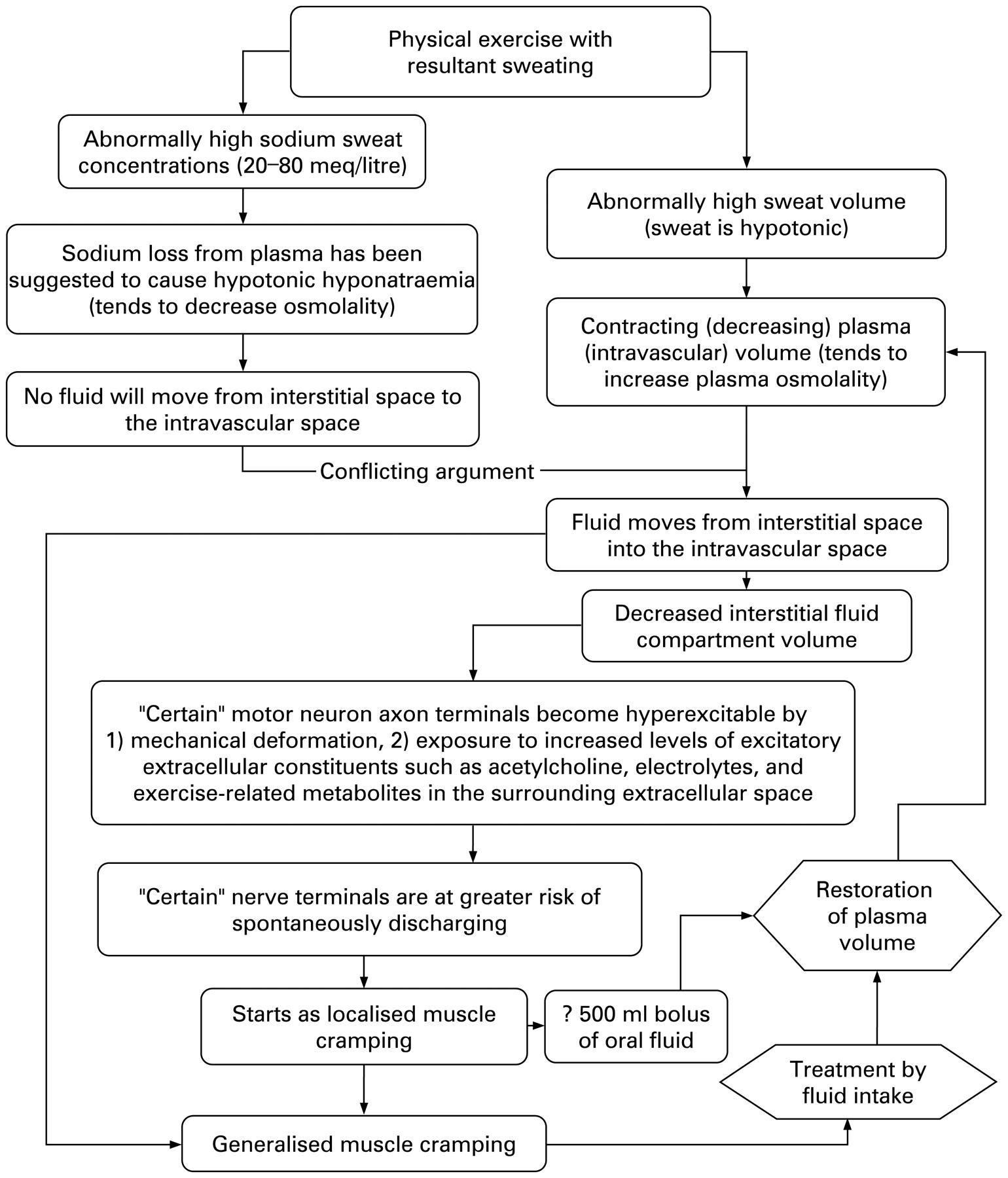
This finding of a dissociation between EAMC and serum electrolyte concentrations has more recently prompted the proponents of the “electrolyte depletion” hypothesis to suggest that, rather than changes in serum electrolyte concentrations, the mechanism for EAMC is increased sweat sodium concentration or “salty sweating”, resulting in sodium depletion, which then causes EAMC.22 23 However, the pathophysiological basis for this hypothesis is not clear, and has never been formally outlined. In this review, an attempt was made, using the explanation offered by Bergeron,23 to formulate the possible progression of physiological events that may take place and how, through “salty sweating” as a result of exercise, this can lead to the development of EAMC (fig 1).

The “electrolyte depletion” hypothesis for the development of Exercise Associated Muscle Cramping (EAMC).
In this hypothesis (fig 1) it has been suggested that excessive sodium loss in sweat results in the development of EAMC22–25 without altering serum sodium or chloride concentrations.23 Because sweat sodium concentration is always hypotonic,26–29 a significant loss of sodium through sweat can therefore only occur if there is an accompanying large loss of fluid. This would mean that dehydration would accompany any significant sodium loss in athletes presenting with EAMC. The proponents of this hypothesis cannot, however, offer a plausible pathophysiological mechanism by which “salty sweating” alone can cause cramping,22 and therefore include dehydration and, more recently, muscle fatigue as additional predisposing factors in the development of EAMC6 — the so-called “triad”.6 22 The only pathophysiological mechanism that has been suggested is that “salty sweating” coupled with significant dehydration causes contraction of the extracellular fluid compartment.23 It is then suggested, with no evidence to support this, that the resultant “loss of interstitial volume causes a mechanical deformation of nerve endings and increasing the surrounding ionic and neurotransmitter concentrations”, which then cause selected motor nerve terminals to become hyperexcitable and spontaneously discharge.23
It is important to point out that scientific evidence for this hypothesis is based on reports in which sweat sodium concentrations were measured (1) during exercise in athletes with a self-reported past history of EAMC, and (2) never at the time of an acute EAMC, or during an exercise bout where EAMC occurred.23–25 There are no published studies in which increased sweat sodium concentrations above those of suitable matched non-cramping controls were measured in athletes presenting with an acute episode of EAMC. It is also important to note that sweat sodium concentrations during exercise, which were measured in athletes with a self-reported past history of EAMC, are only available in 23 subjects from three studies: (1) a single case of one tennis player with EAMC,24 (2) a case series of 17 tennis players with a past history of cramping,23 and (3) a small observational study in 10 American football players (five players with a past history of cramping, and five players with no history of cramping).25 These 23 cases with a past history of EAMC are the only cases where a reportedly “high” sweat sodium concentration is linked to EAMC.
Important methodological considerations in these three studies23–25 are that (i) no suitable control groups were included in the studies on tennis players,23 24 (ii) the sample sizes of cases and control groups in the American football study were very small,25 (iii) sweat sodium concentrations were not measured at the time when athletes experienced EAMC, and (iv) other factors that could determine sweat sodium concentrations, such as dietary intake of sodium, state of acclimatisation, anatomical variability in sweat collection site, variability of sweat electrolyte concentrations within an exercise bout, and seasonal variation were either not documented or not taken into account. Furthermore, in two of these studies, it was suggested that sweat sodium losses could result in “deficits of total exchangeable sodium”, a claim that is not substantiated by any direct measurement.
The definition of what constitutes a “salty sweater” also requires some discussion. At present, there are no data available to define an “abnormally high” sweat sodium concentration during exercise. However, it is important to note that sweat sodium concentrations have been measured during exercise in normal (non-cramping) athletes) of varying ages,26 different genders,27 in varying states of acclimatisation28 or fitness,26 in different body regions,26 26 27 in different exercise durations,27 in different environmental conditions27 and using different techniques to collect sweat and then measure the sweat sodium concentration.28 29 The findings of these studies show that the mean sweat sodium concentration of these normal athletes (with no past history of cramping) is consistently higher than or the same as those mean sweat sodium concentrations reported in the “salty sweaters” listed in the three case series previously mentioned. Therefore, in the 23 cases that form the basis of the “salty sweating” in the “electrolyte depletion” hypothesis, sweat sodium concentrations during exercise were in fact normal to low.
Experimentally induced hyponatraemia, if accompanied by sodium loss, has been associated with generalised skeletal muscle cramping at rest.30 31 In another clinical setting generalised muscle cramping has been reported in 5–20% of patients undergoing haemodialysis.32 Although the mechanisms of cramping during haemodialysis are also not well understood, this form of cramping has been linked to changes in plasma osmolality and altered serum sodium concentrations.33 Recently, it has been shown that this form of cramping can be reduced if serum osmolality and serum sodium concentrations are normalised using a technique known as “sodium profiling”.32 Altered serum electrolyte concentrations caused by systemic abnormalities can therefore result in generalised skeletal muscle cramping at rest.34 However, it is important to note that, in the majority of athletes presenting with EAMC, cramping occurs in the localised muscle groups that are involved in the repetitive contractions associated with exercise,23 25 35 and that these contractions occur in spasms lasting 1–3 minutes.6 This clinical presentation of localised EAMC has been well described, even by proponents of the “electrolyte depletion” hypothesis.6 23 In the “electrolyte depletion” hypothesis there is no suitable physiological explanation of how a systemic abnormality such as electrolyte depletion could result in localised symptoms that are episodic. Furthermore, the proponents of the “electrolyte depletion” hypothesis indicated that the immediate treatment of acute EAMC is rest, prolonged passive stretching, and oral sodium chloride.6 The “electrolyte depletion” hypothesis does not explain why interventions such as rest and passive stretching are effective and why these are supported.6
In summary, there is evidence that altered serum osmolality and altered serum electrolyte concentrations (notably hypochloraemia, hyponatraemia, and hypocalcaemia) can cause generalised skeletal muscle cramping at rest in specific clinical settings. However, data from well-conducted prospective cohort studies show that athletes with acute EAMC are not hyponatraemic, hypochloraemic, or hypocalcaemic and do not have an abnormal serum osmolality.8 Furthermore, there is no evidence that athletes with a history of EAMC (23 reported cases) have higher sweat sodium concentration than reported sweat sodium concentrations from subjects in a number of other studies. Finally, electrolyte depletion is a systemic abnormality that will affect all the skeletal muscles in the body. Yet, the clinical picture of EAMC in the majority of cases is that of localised cramping in the exercising muscle groups. This clinical observation, also reported by clinicians who are proponents of the electrolyte depletion hypothesis, is not in keeping with the systemic nature of electrolyte depletion.
Scientific evidence in support of the dehydration hypothesis for the aetiology of EAMC
The dehydration hypothesis for the cause of EAMC also has its roots more than 100 years ago, when case series reports linked cramping in mine workers to excessive sweating and presumed dehydration.12 These were anecdotal observations and no actual measures of hydration status were reported in these cases. Dehydration is still commonly cited as a cause for muscle cramps in athletes6 36 and is linked to the “electrolyte depletion” hypothesis,6 22 23 and more recently as part of a “triad” of causes of EAMC.6 22
A careful review of the literature did not identify a single published scientific study showing that athletes with acute EAMC are more dehydrated that control athletes (athletes of the same gender, competing in the same race with similar race finishing times). In contrast, there is evidence from four prospective cohort studies showing that dehydration is not associated with EAMC. In these studies, the relationship between hydration status (indirectly measured as the difference between pre and post-race body weight) and EAMC was carefully documented in cramping athletes and controls.8 9 16(Drew N, MPhil Sports Medicine dissertation, University of Cape Town, 2006) The findings of these studies consistently show that cramping athletes, at the time of acute symptoms, were not more dehydrated than control (non-cramping) athletes. If anything, athletes in the cramping groups were consistently less dehydrated (not significantly so) than the control subjects. The results of these studies do not, therefore, support the hypothesis that there is a direct relationship between dehydration and muscle cramping. The proposed mechanism that “as progressive dehydration occurs, the extracellular fluid compartment becomes increasingly contracted” and that this results in EAMC22 23 is therefore not supported by these findings. Both electrolyte depletion and dehydration are systemic abnormalities, and therefore also do not explain the localised nature of EAMC.
Summary: scientific evidence in support of the electrolyte depletion and the dehydration hypothesis for the aetiology of EAMC
In summary, dehydration and electrolyte depletion are often considered together (and recently together with muscle fatigue) as the “triad” causing EAMC. The key components of this hypothesis (fig 1) are that electrolyte (mainly sodium) depletion through excessive sweat sodium loss together with dehydration causes EAMC. However, results from prospective cohort studies consistently show that athletes suffering from acute EAMC are not dehydrated, neither do they have disturbances in serum osmolality or serum electrolyte (notably sodium) concentrations. Furthermore, sweat sodium concentrations measured during exercise in 23 reported cases with a past history of EAMC are not higher than those reported in many other studies. Both electrolyte depletion and dehydration are systemic abnormalities, and therefore would result in systemic symptoms, as has been observed in other clinical conditions. However, in EAMC, the symptoms classically are local and are confined to the working muscle groups. Thus, the available evidence to date does not support the hypotheses that electrolyte depletion or dehydration cause EAMC — therefore an alternate hypothesis for the aetiology of EAMC has to be considered.
SCIENTIFIC EVIDENCE SUPPORTING THE “ALTERED NEUROMUSCULAR CONTROL” HYPOTHESIS FOR THE AETIOLOGY OF EAMC
Introduction and historical background
The development of muscle fatigue resulting in “altered neuromuscular control” as a cause for EAMC was first proposed in March 1996. This was at the time of an international symposium on “Muscle fatigue” which was held in Cape Town, South Africa. The main observation that led to the development of the “altered neuromuscular hypothesis” for EAMC came from results of a descriptive cross-sectional epidemiological study that was conducted in our unit in the early 1990s.37 In this study, 1383 marathon runners responded to a questionnaire on EAMC. Of these runners, 536 (26%) reported a past history of EAMC. The majority (60%) of this group of runners with a past history of EAMC indicated that muscle fatigue was associated with, and preceded, the onset of EAMC. This seemingly incidental finding prompted an in-depth review of the possible mechanism that may link the development of muscle fatigue to EAMC. The results of this review were presented at the meeting that was held in 1996, and the proceedings of the meeting were published in the following year.10 In this review, the possible pathophysiological mechanisms for muscle cramping were explored from the fundamental physiological principle that muscle cramping can be considered as an abnormality of skeletal muscle relaxation.10 38 For the first time, the lack of scientific evidence to support the “electrolyte” and dehydration” hypotheses was also highlighted in this review,10 and evidence that a neurological mechanism resulting from altered reflex control mechanism in response to muscle fatigue was proposed as an alternate hypothesis for the aetiology of EAMC.10
At the same time, a second independent review on the proposed mechanisms of EAMC was published a few months after the 1996 “Muscle fatigue” conference.39 In this review it was also concluded that “disturbances at various levels of the central and peripheral nervous system and skeletal muscle are likely to be involved in the mechanism of cramp.” However, in this review evidence for “electrolyte depletion” or the “dehydration” hypothesis for EAMC was not explored.39
Over the past 10 years, a number of research studies have been conducted to explore possible mechanisms for the development of muscle cramping in general, and EAMC specifically. The findings of these studies form the basis for the current understanding of the “altered neuromuscular control” hypothesis for EAMC. The sequence of physiological events that could explain the development of EAMC has therefore now been refined. The current concepts that link repetitive muscular exercise, the development of muscle fatigue and the possible mechanisms by which muscle fatigue and perhaps other triggers could result in EAMC by altering neuromuscular control are summarised in fig 2. This scientific evidence, including the pathophysiological mechanisms at each step, will now be reviewed.

{kind=link}
{kind=link}
The “altered neuromuscular control” hypothesis for the development of Exercise Associated Muscle Cramping (EAMC).
Scientific evidence supporting an association between factors causing premature muscle fatigue and EAMC
It is well established that, during muscular exercise, there are many factors that can contribute to the development of muscle fatigue. These factors include exercising in hot and humid environmental conditions, increasing exercise intensity, increased exercise duration, and depletion of muscle energy stores. The evidence that some of these known factors are associated with the development of EAMC will now be reviewed.
The observation that EAMC is more common when physical exercise is performed in hot and humid environmental conditions has its roots in case reports dating to over 100 years ago,11 12 and the term “heat cramps” was first used in the medical literature in the 1930s12 and is still used today.6 In considering the possibility that exercising in hot, humid conditions causes cramps, there are two fundamental questions that need to be answered. The first question is whether EAMC is more common when athletes exercise in hot, humid environmental conditions, and the second question relates to the possible mechanism by which exercising in the heat can lead to EAMC.
Historical reports (cases and case series) and clinical anecdotal observations appear to indicate that EAMC does occur more frequently when athletes exercise in hot, humid conditions.11 12 More substantive data to support this observation comes from only one epidemiological study, in which the incidence of EAMC in different environmental conditions has been reported in American Football players.13 In this study it was reported that “heat cramps” were more common when the Heat Index was “high” or “extreme” compared with “low” or “moderate”.13 It must, however, be noted that these hot and humid conditions also occurred during the first 2–3 weeks of training in a season, when players were also likely to be less well conditioned, and were likely not acclimatised to the environmental conditions. In this study, however, acclimatisation and training status were not documented. Therefore, although there is anecdotal evidence that EAMC occurs more frequently when athletes exercise in hot, humid environmental conditions, solid scientific evidence to support this is still lacking.
As indicated, the mechanism by which exercise in hot humid conditions may cause EAMC also requires discussion. Historically, when EAMC occurred in athletes who exercised in hot humid conditions, this has been attributed to dehydration and/or electrolyte disturbances, rather than the possible effects of heat alone. The lack of scientific evidence relating EAMC to dehydration or electrolyte depletion has already been discussed. It appears, therefore, that if exercising in hot and humid conditions does result in EAMC this may not be due to electrolyte depletion or dehydration. Therefore, an alternate mechanism may be responsible for this observation.
It is well documented that there are a number of mechanisms by which exercise in the heat will result in the development of muscle fatigue, independent of electrolyte depletion or dehydration.40 Therefore, it is possible that the mechanism by which exercise conducted in hot humid environmental conditions can cause EAMC, not as a result of dehydration or electrolyte depletion, but because of the development of muscle fatigue. The possible mechanisms by which muscle fatigue could result in EAMC will be reviewed in detail in a subsequent section.
Muscle fatigue during exercise can develop if athletes exercise at a high intensity or if exercise is performed for a prolonged time period. In observational studies it has been documented that there is an association between EAMC in athletes and (1) self-reported poor conditioning for an event 37 and (2) exercising at a higher intensity such as during racing and not during training,37 and that development of EAMC is more common in the latter stages of a race (prolonged duration of exercise).16 37 However, stronger evidence linking increased exercise intensity and EAMC comes from a recently completed prospective cohort study in Ironman triathletes. In this study, 210 triathletes competing in the 2006 South African Ironman triathlon acted as subjects. All the subjects were assessed pre-race, and information from a detailed questionnaire included training history, personal best performances and a cramping history. During the race, 44 triathletes developed EAMC (cramp group), while 166 served as a control (non-cramping) group. In a multivariate analysis, the results of this study showed that EAMC was related to a faster overall triathlon racing time and a faster predicted triathlon racing time, despite similarly matched preparation and performance histories to those in the control group. The faster racing time (increased exercise intensity) in the cramp group was an independent risk factor for the development of EAMC in these triathletes (Drew N, MPhil Sports Medicine dissertation, University of Cape Town, 2006).
There are no studies that have explored the relationship between depletion of muscle energy stores (mainly muscle glycogen) and the development of EAMC. However, in a recently published study using a laboratory-based exercise protocol that was specifically designed to cause fatigue of the calf muscles, a high incidence of muscle cramping during exercise was documented.7 In this study of 13 healthy men (91.8 (SD 15.1) kg) the administration of an oral solution containing carbohydrate and electrolytes (given at a rate of 1.0 to 1.5 litres/h), compared with no fluid administration, resulted in a delay in the onset of EAMC (from a mean of 14.6 (SD 5.0) min to a mean of 36.8 (SD 17.3) min). The main limitation in this study was that the intervention consisted of administration of a drink that contained fluid, electrolytes, and carbohydrate. It is therefore not possible to determine whether the act of drinking, the fluid, the electrolytes, the carbohydrate or a combination of these interventions was responsible for the delay in the onset of EAMC. However, as EAMC occurred after a mean of 15 min into the exercise bout, and the mean sweat rate reported in this group was 2.0 litres/h, the mean fluid loss after 15 min can be estimated as 500 ml, which is not enough to result in significant dehydration. Furthermore, if the sweat sodium concentrations in the subjects were in the range reported as “salty sweaters” (mean of ∼50 meq/litre) total sodium loss in the 15 min of exercise would have been ∼25 meq, again not enough to result in significant sodium depletion. Therefore, it is unlikely that either clinically significant dehydration or sodium depletion could occur in this short time period. In contrast, it has been documented that short-duration, intermittent, high-intensity exercise can significantly reduce muscle glycogen stores.41 Although speculative, as measurements of muscle glycogen were not done, the delay in EAMC following the combination drink in the Jung et al study could have been due to the carbohydrate supplementation in the drink, thereby delaying the depletion of muscle energy stores (glycogen).7
In summary, there are some data to support the observations that some factors responsible for the development of muscle fatigue may also be associated with the development of EAMC. There is some evidence that exercising in hot, humid environmental conditions increases the risk of developing EAMC.13 The possible mechanism for this increased risk is not as a result of dehydration or electrolyte depletion, but could be related to the development of muscle fatigue. There is only limited evidence that other factors which can cause muscle fatigue, such as increased exercise duration, poor conditioning and depletion of muscle energy stores, are related to the development of EAMC, and this requires further investigation. However, participating at higher exercise intensity during racing (compared with training) has recently been shown to be an independent risk factor for the development of EAMC.
Scientific evidence that fatiguing muscular exercise can cause muscle cramping
One of the first studies showing that fatiguing muscle contraction can induce cramping in normal healthy subjects was reported in 1957.42 In this study, among 115 college students, sustained maximal muscle contraction, with the muscle in a shortened position, resulted in muscle cramping in 18% of the subjects before an exercise bout, and in 26% after a 20–30 min exercise (swimming or callisthenics) bout. This was also one of the first studies documenting that these episodes of cramping were electrically active (using electromyography), and that acute cramping could be treated by passive stretching.42 These authors concluded that it was probable that “the motor activity in cramps was originating in the central nervous system”. This observation, that cramping can be induced by voluntary sustained muscle contractions, has now been confirmed by a number of investigators.43–45 Furthermore, there is evidence that muscle cramping can be caused by repetitive electrical stimulation of the nerves supplying the motor input to muscle,45 46 and that this can be used as a reliable laboratory test to induce cramping in humans.47
In these laboratory studies investigating muscle cramping in human subjects, factors that have been shown to increase the likelihood of inducing cramping have also been explored. It has been documented in the voluntary contraction model that contraction of the muscle in a shortened position,42–45 and first performing muscular exercise and then performing the voluntary contraction to induce cramping,42 increases the likelihood of inducing muscle cramping. In the case of the electrical stimulation model, stimulation of the nerve to reach a specific “threshold frequency” of stimulation reliably induces muscle cramping.45 46
In summary, these laboratory-based studies show that, in humans, voluntary muscle contraction and electrical stimulation of the muscle reliably induce muscle cramping. Furthermore, performing muscular exercise, as well as contracting the muscle in a shortened position, increases the likelihood of inducing muscle cramp. These data indicate that the mechanism for muscle cramping is neuromuscular in nature.
Scientific evidence that the mechanism by which fatiguing muscular exercise causes muscle cramping is muscle fatigue resulting in altered neuromuscular control
There is a growing body of evidence to suggest that the mechanism for muscle cramping has a neuromuscular basis. Firstly, as has been discussed, voluntary muscle contraction or stimulation of the motor nerve can reliably cause muscle cramping. Secondly, there is evidence from experimental work in human subjects that stimulation of the 1a afferents through electrical stimulation48 or using the tendon tap (activating the 1a afferents)48 can induce cramping. Thirdly, it has repeatedly been shown that the most effective treatment for cramping induced in this manner is muscle stretching.42 45
An increase in tension in the Golgi tendon organ during stretching, which will result in increased afferent reflex inhibitory input to the α-motor neuron,44 is a plausible mechanism to explain why stretching is an effective treatment of cramping. This mechanism would also support the finding that voluntary contraction of the muscle in a shortened position increases the likelihood of cramping42–45 because the tension in the tendon (and therefore the Golgi tendon organ) would be less. Strong evidence, from a recently published study, supporting this inhibitory mechanism is that electrical stimulation of the tendon afferents has been shown to successfully relieve muscle cramping.44 Collectively, these data indicate that the mechanism responsible for muscle cramping is a result of altered neuromuscular control, whereby increased α-motor neuron activity as well as reduced inhibitory feedback from the tendon both have an important role in generating cramp.44
There is also evidence that the development of muscle fatigue alters spinal neuromuscular control mechanisms that are responsible for muscle activation and inhibition.49 50 In an animal model, muscle fatigue has been shown to disrupt the functioning of the peripheral muscle receptors by causing (1) an increased firing rate of the muscle spindle’s type 1a and II afferents, and (2) a decrease in the type Ib afferent activity from the Golgi tendon organ.49 50 Therefore, as muscle fatigue develops during prolonged intense exercise, it is possible that a combination of the increased excitatory activity of the muscle spindle and a reduced inhibitory effect of the Golgi tendon organ with muscle fatigue would result in a sustained α-motor neuron activity.10 Clinically, and when measuring electromyographic activity, this would initially present as muscle fasciculation (muscle “twitches”) and increased electromyographic (EMG) activity respectively. This has been termed the “cramp prone state”.35 If fatiguing exercise continues, a full-blown muscle cramp will develop.
There is some evidence from a field study in support of this “cramp prone state”. It has been documented that there is increased EMG activity at rest (baseline activity between bouts of acute episodes of EAMC) in athletes who suffer from EAMC.9 In this study, baseline EMG activity in triathletes suffering from EAMC was significantly higher in the cramping muscle than in a non-cramping control muscle in the same athlete.9 This finding indicates that cramping muscles, in between bouts of acute EAMC, exhibit increased neuromuscular excitability — notably in the exercising muscle groups only. In these subjects EAMC was not associated with systemic abnormalities such as electrolyte depletion or dehydration. Although these findings have to be interpreted with caution because of a small sample size,9 the observed heightened neuromuscular excitability (“cramp prone state”) could be explained by the development of muscle fatigue and the resultant changes in spinal neuromuscular control that have already been reviewed.
Finally, further evidence in support of the “abnormal neuromuscular control” hypothesis for EAMC comes from an analysis of the effective therapeutic approaches to EAMC. As has already been discussed, passive stretching is the most common and effective therapy to relieve acute muscle cramping.42 44 51–53 It is also regarded as effective treatment by those who mainly support the electrolyte depletion and dehydration hypotheses of EAMC.6 As previously discussed, passive stretching increases the tension in a muscle, thereby increasing the Golgi tendon organ’s inhibitory activity,44 50 and this mechanism offers further support for the hypothesis that abnormal neuromuscular control is associated with EAMC.10
In summary, there is growing scientific evidence from studies in human and animal models that muscle cramping occurs with repetitive muscle contraction. As muscle fatigue develops there is evidence that this is associated with increased excitatory and decreased inhibitory signals to the α-motor neuron. If muscle contraction (or electrical stimulation of the muscle) continues, muscle cramping results. Effective immediate treatment of the cramping is by increasing inhibitory input to the muscle, either by stimulating the Golgi tendon organ afferents through stretching or by electrical stimulation of the tendon. Finally, there is some evidence that athletes with acute EAMC exhibit this increased muscular hyperexcitability in between bouts of acute EAMC (“cramp prone state”). These data suggest that altered neuromuscular control during fatiguing muscular exercise is the principal mechanism in the aetiology of acute EAMC.
Other aetiological factors in EAMC that have to be considered in future research
There are other factors that may have to be considered in the aetiology of EAMC. These factors may well also alter neuromuscular control during exercise, but need further investigation. Recently, it has been shown in a prospective cohort study that one of the two independent risk factors associated with EAMC in triathletes (multivariate analysis) was a previous history of EAMC (Drew N, MPhil Sports Medicine dissertation, University of Cape Town, 2006). A positive family history of cramping has also been reported as a risk factor for EAMC in a cross-sectional study.37 Therefore, a genetic predisposition to EAMC cannot be excluded, but the precise mechanism for such a predisposition requires further investigation.
There are other possible mechanisms that could alter neuromuscular control at the spinal cord level, and therefore may contribute to the development of EAMC. The first of these is the possibility that muscle injury or muscle damage, resulting from fatiguing exercise, could cause a reflex “spasm”, and thereby result in a sustained involuntary contraction. The second possibility is that increased or decreased signals from other peripheral receptors (such as chemically sensitive intramuscular afferents, pressure receptors or pain receptors) could elicit a response from the central nervous system that can alter neuromuscular control of the muscles.44 These other mechanisms have not been investigated in athletes with EAMC, but would be important to explore in the future.
SUMMARY
In summary, scientific evidence in support of the “electrolyte depletion” and “dehydration” hypotheses for the aetiology of EAMC comes mainly from anecdotal clinical observations, case series totalling 18 cases, and one small (n = 10) case–control study. Results from four prospective cohort studies do not support these hypotheses. In addition, the “electrolyte depletion” and “dehydration” hypotheses do not offer plausible pathophysiological mechanisms, with supporting scientific evidence that could adequately explain the clinical presentation and management of EAMC.
Scientific evidence for the “altered neuromuscular control” hypothesis is based on evidence from human laboratory models of cramping, animal experimental data on spinal reflex activity during fatigue, and field studies where EMG data were recorded during bouts of acute cramping after fatiguing exercise.34 Whilst it is clear that further evidence to support the “altered neuromuscular control” hypothesis is also required, research data are accumulating that support this as the principal pathophysiological mechanism for the aetiology of EAMC (fig 2).
Acknowledgments
Funding for the studies by the author who contributed to this review came mainly from the University of Cape Town and the Medical Research Council of South Africa. No funding was received from any company that may have benefited from results of the scientific studies conducted by the author.
REFERENCES
Footnotes
Competing interests: The author has been reimbursed by Gatorade, the manufacturer of Gatorade sports drinks, for the costs to attend the “Sodium and Exercise” conference in Vail, Colorado in July 2007 and to produce the original manuscript for the proceedings of this conference.