Article Text

Abstract
Objective: To study the incidence and nature of injuries at European Championships, to compare training and match injury characteristics and to study differences in injury incidence between tournaments.
Design: Team physicians prospectively recorded individual player exposure and time loss injuries during 12 European Championships (men’s EURO n = 1, men’s Under-21 n = 2, men’s Under-19 n = 3, men’s Under-17 n = 3, women’s Under-19 n = 3) from 2006 to 2008.
Setting: International football tournaments
Participants: 1594 men and 433 women
Main outcome measurement: Injury incidence
Results: 224 injuries (45 training, 179 match play) were registered among 208 (10%) players. No differences in training injury incidence were seen between tournaments (range 1.3–3.9 injuries/1000 hours). The men’s EURO had the highest match injury incidence (41.6 injuries/1000 hours) followed by the men’s Under-21 tournaments (33.9). The lowest match injury incidence was seen in the women’s Under-19 tournaments (20.5). Training injuries constituted 20% of all injuries and caused 26% of all match unavailability. A greater proportion of match injuries were due to trauma (83 vs 47%, p<0.001) and occurred from player contact (75 vs 48%, p = 0.018) compared to training injuries. A higher frequency of re-injury was found among training injuries than match injuries (20 vs 6%, p = 0.009).
Conclusions: Match injury incidence increased with age, indicating greater risk with higher intensity of play. Training injury incidence was relatively low, but training injuries were responsible for a quarter of all match unavailability and may thus have a profound impact on team performance and should be the object of preventive measures.
Statistics from Altmetric.com
Injury registration systems have been implemented as a matter of routine at international football championships during Federation of International Football Associations (FIFA) World Cups and Olympic Games since 19981–5 and at Union of European Football Associations (UEFA) European Championships since 2004.6 Registration shows that the injury risk in international tournament matches (men 29–51 time loss injuries/1000 match hours; women 24–36) is just as high as or even higher than at the elite club level for men (21–35/1000)7–13 and women (14–24/1000).13–16
The incidence, nature and consequences of training injuries at national team level are not equally well described. Training injury incidences at the men’s 2004 EURO, women’s 2005 EURO and the men’s Under-19 2005 European Championship were low (2.1–2.9 injuries/1000 training hours)11 compared to that at men’s (2–12/1000)8–13 and women’s (3–7/1000)13–16 elite club level. This is probably due to the large number of low intensity recovery and tactical training sessions that carry a low risk for injury, during international tournaments. Even though the risk for training injury is relatively low, training injuries represented 15% of all injuries sustained during European Championships 2004–5.6
The purposes of this prospective audit were to study the incidence and nature of injuries at European Championships from 2006 to 2008, to compare training and match injury characteristics, and to study differences in injury incidence between tournaments. Our hypotheses were that the injury incidence would increase with age, that injury characteristics would not differ between training and match injuries, and that the type of training performed during the tournament would influence the injury incidence.
METHODS
Study design and participants
Twelve UEFA European Championships (nine men’s and three women’s, table 1) from 2006 to 2008 were followed prospectively using the same methods as implemented during previous tournaments 2004–5.6 Study design, methods and definitions have been validated for professional club football17 and comply with the consensus statement.18 All players selected to participate in the tournament were included in the audit. Players who were brought into a team during the tournament as replacement for an injured player were included. Data from players who left their team during the study (ie, due to injury or illness) were included for their entire participation in the tournament. All players received information about study purpose and design from their team physician and signed a written informed consent.
Exposure and injury registration
The team physician documented individual player training exposure and time loss injuries that occurred during the tournament on standard forms.6 17 The definitions applied in the study are shown in table 2. Training content was registered according to four categories (table 2). Match exposure was taken from official records. Injuries resulting in the player being unable to fully participate in training or match play were recorded. All injuries were followed until the final day of rehabilitation even if this was after the tournament (three anterior cruciate ligament tears were given an estimated recovery of six months). The information collected for each injury included: player code and team, date of injury, date of return to full participation, training or match injury, injury type and location, diagnosis, traumatic or overuse injury, contact or non-contact, re-injury or not and the referee’s decision.
To ensure a high consistency of reporting, all team physicians attended a meeting prior to each tournament where the study purpose and methods were illustrated. Furthermore, they were provided with a study manual including definitions and examples of how to fill in the forms. Exposure and injury forms were collected every third day by a member of the study group on site at each tournament. This procedure allowed direct feedback of the accuracy of reporting and any uncertainties could be clarified immediately.
Statistical analyses
Groups were compared with analysis of variance or the Mann-Whitney U test (for non-normally distributed data) for quantitative variables, and the χ2 test or Fisher exact test for qualitative variables. Injury incidences were compared between groups using z-statistics.19 For comparisons of injury incidences between tournaments data from all tournaments within the same sex and age group were aggregated to increase statistical power. The correlation between team training content and injury incidence was evaluated using Pearson product-moment coefficient and significance tested using a z-test. For these analyses, the two categories of strength training and endurance training were combined due to the small amount (<1%) of endurance training. Group mean values are presented with standard deviations, and injury incidences with 95% confidence intervals. For all analyses, a p value less than 0.05 was considered statistically significant.
The study design was reviewed for ethics and approved by the UEFA Development Division and the UEFA Medical Committee.
RESULTS
The response rate and completeness of exposure and injury forms was 100% for all tournaments.
Exposure and training content
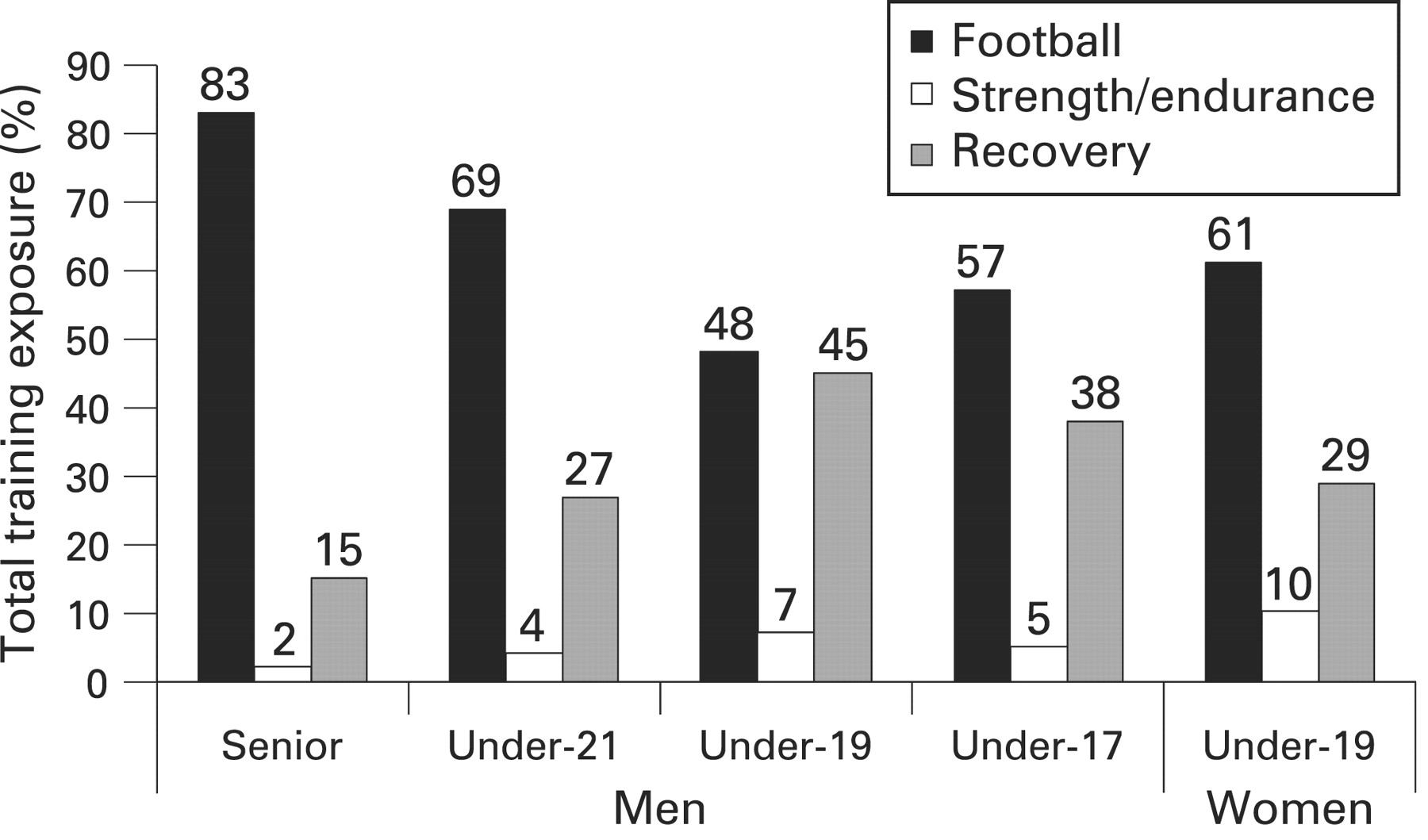
Overall, 772 team training sessions (15 187 training hours) and 199 matches (6542 match hours) were included at the tournaments studied (table 1). Football-specific training dominated the training content (fig 1), being relatively more frequent in the men’s EURO than in the men’s Under-21 (p = 0.069), Under-19 (p<0.001) and Under-17 (p = 0.002) tournaments, and in the women’s Under-19 tournaments (p = 0.002). No significant correlation was found between the degree of football training and total injury incidence (r = −0.044, p = 0.67), training incidence (r = −0.022, p = 0.83) or match incidence (r = 0.064, p = 0.54) during the tournament. Similarly, no correlation was observed between the degree of strength/endurance training (range r = −0.13 to 0.11, all p>0.05) or recovery training (range r = −0.13 to 0.091, all p>0.05) and injury incidence.

Relative distribution of different training categories (% of the total training exposure) at European Championships according to gender and age. The categories strength training and endurance training have been combined due to the small amount (<1%) of endurance training.
Frequency and nature of injuries
In total, 224 injuries (45 training, 179 match play) were registered among 208 (10%) players. This corresponds to 0.9 injuries/match or one training injury per 17 training sessions (table 1). Injuries resulting from trauma represented 76% of injures, 71% of which were due to player contact, and overuse 24% (table 3). Muscle strain, contusion and ligament sprain were the most common injury types. Match contact injuries were more common in the second (n = 67) than in the first half (n = 46) (p = 0.008), while no statistical difference was observed for non-contact injuries (first half n = 14; second half n = 18, p = 0.45). Thirty-one match injuries (17%) were caused by foul play, 24 due to opponent foul and 7 due to own foul. Foul play injuries were evenly divided between the two halves (n = 14 vs 17).
Twenty re-injuries (9%) were recorded, with 16 early (two index injuries during the tournament) and four late recurrences. Re-injuries comprised seven overuse or muscle strain injury to the groin, five thigh strains, three ankle sprains, two knee sprains, one meniscus lesion, one knee joint synovitis and one shoulder dislocation. Re-injuries tended to cause longer absence than non-re-injuries; mean absence 21.3 (26.9) compared to 12.6 (26.2) days (p = 0.07).
No differences in total injury incidence were seen between teams that were eliminated in the group stage compared to teams that went to the final stage of the tournament; men’s EURO 8.8 versus 11.0 injuries/1000 hours (p = 0.48), Under-21 10.2 versus 13.5 (p = 0.42), Under-19 12.2 versus 10.9 (p = 0.74), Under-17 11.7 versus 13.5 (p = 0.67) and women’s Under-19 12.5 versus 10.3 (p = 0.54). No difference in match injury incidence was seen between matches lost (26.2 injuries/1000 hours), matches won (28.8/1000) and matches tied (26.0/1000) (p = 0.86).
Injury severity
The majority of injuries resulted in absence from football of one week or less, but 15% were severe (table 2). Of the total 224 injuries, 133 (59%) led to the player missing a subsequent match (38/45 training injuries and 95/179 match injuries). The mean injury absence was 13.4 (26.3) days, with 2.8 (2.9) days lost during the tournament. Ninety-one injuries (41%) caused absence after the tournament, resulting in a mean of 26.2 (34.1) days absence after the tournament. The diagnosis and circumstances of 34 severe injuries are listed in table 3. Player-to-player contact was involved in 47% of the severe injuries, and 21% of the severe match injuries resulted from foul play.
Comparison of injury incidence between tournaments
The highest training injury incidences were seen in the men’s under-21 and the women’s under-19 tournaments (fig 2). No statistical differences were seen, however, in training injury incidence between the men’s tournaments including all time loss injuries (all p>0.05) or only those that led to match absence (all p>0.05). Likewise, no difference was found between the women’s and men’s under-19 tournaments (all time loss p = 0.08; injuries causing match absence p = 0.43).
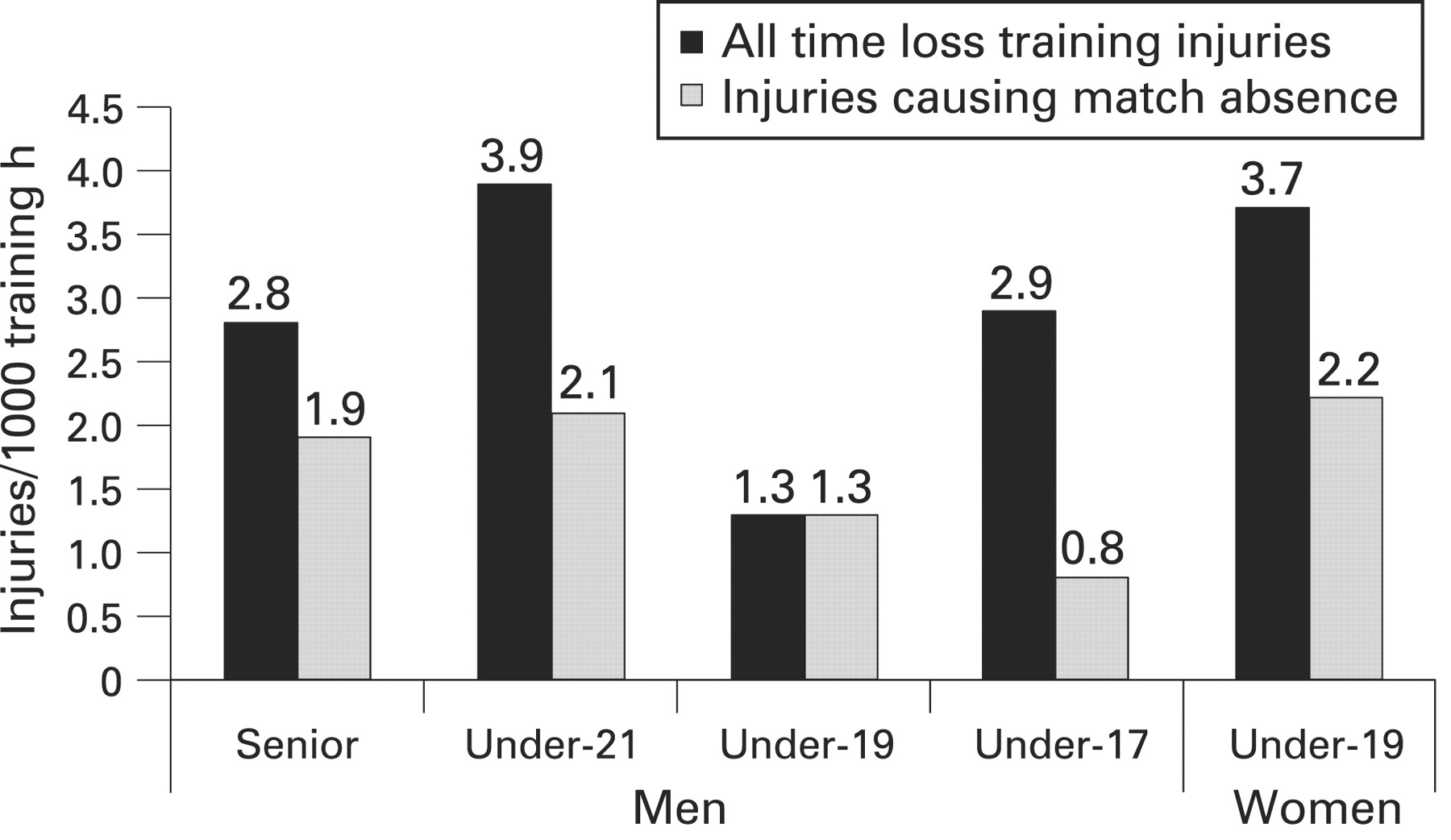
Incidences of all time loss training injuries (black bars) and training injuries that led to a subsequent missed match (shaded bars) at European Championships according to gender and age.
A tendency towards increasing match injury incidences with age was observed in the men’s tournaments (fig 3). This reached statistically significant levels between the men’s EURO and the Under-19 (p = 0.009) and Under-17 (p = 0.011) tournaments (all time loss injuries; similar results for injuries causing subsequent match absence). No differences in match injury incidences were observed between the men’s and the women’s Under-19 tournaments (all time loss injuries p = 0.60; injuries causing match absence p = 0.54).

{kind=link}
{kind=link}
{kind=link}
Incidences of all time loss match injuries (black bars) and match injuries that led to a subsequent missed match (shaded bars) at European Championships according to gender and age.
Nature and consequences of training injuries versus match injuries
There was no difference in injury severity between injuries sustained during training compared to match injuries (table 3). Traumatic injuries and player contact injuries were more common among match injuries. No significant differences were observed in injury location between training and match injuries, although most head/neck injuries occurred in matches (training: one neck pain, match: seven concussions, two facial fractures, five head contusions). A higher frequency of re-injury was found among training injuries.
In total, injuries led to 457 missed training sessions (on average 2.9% of the squad was absent due to injury) and 148 missed matches (average 1.9% of the squad unavailable for match selection). Injuries sustained during training represented 17% (n = 79) and 26% (n = 39) of unavailability for training sessions and matches respectively. Match injuries accounted for 83% (n = 378) and 74% (n = 109) of the training and match unavailability.
DISCUSSION
The main finding of this study was that training injuries represented 20% of all injuries sustained during international tournaments and were responsible for 26% of squad match unavailability. This means that even though the rate of training injury is low at international tournaments compared to club level football, this could have a profound impact on team performance as well as the medical resources required during international tournaments and should be the object of preventive measures. Another important finding was that match injury incidence increased with age, being highest in the men’s EURO, while no difference was seen between the men’s and women’s Under-19 tournaments. Finally, the incidence of severe injury was substantially greater than that reported at professional club level.9–11 13
Frequency and nature of injuries
Overuse injuries and non-contact traumatic injuries represented 44% of all injuries, with similar findings in senior and youth tournaments. The major European Championships are played shortly after the end of the domestic season and the finals of the Champions League and UEFA Cup, and player fatigue due to a busy match calendar prior to an international tournament could be a contributing factor behind these injuries.3 20 It is thus vital to allow sufficient time for rest and recovery of key players before a tournament. Many young players are not used to playing matches every second or third day, as during international youth tournaments, and this could be a risk factor for overuse and non-contact injury related to fatigue. The mental stress that comes with playing an international tournament is also a factor to consider, and sufficient recuperation should be ensured.
Traumatic injuries due to player contact represented 54% of all injuries overall, and were more frequent among match injuries (63%). No differences were observed between tournaments showing the competitive nature of both youth and senior tournaments. Contact injuries were more common in the second half, possibly because of fatigue and a lack of focus towards the end of a match. It could also be that the intensity and frequency of contact situations is greater towards the end of a match when players increase their efforts to win. Foul play injuries were evenly divided between halves, but it is unknown whether foul play situations occurred more frequently towards the end of matches. If this is the case then stronger sanctions by the referee could help prevent injuries. Overall, relatively few match injuries (17%) were due to foul play. It is not clear whether the remaining 83% of match injuries occurred in situations that complied with the laws of football or whether referees failed to recognise foul play in injury situations. One previous study suggested that many match contact injuries are caused by the players’ failure to comply with the laws of the game, and that referees often fail to award fouls for incidents leading to injury.21
Very few re-injuries (overall 9%, early recurrences 7%) were observed, as in previous European Championships (early recurrence rate 5%).6 Early recurrence rates in professional club football, using a similar definition, is reported to be considerably higher (15–30%)9–11 13 indicating that players with complaints and injuries are generally not selected for the final international tournament squads. The fact that only two injuries resulted in recurrence later on in the tournament suggests that the standard of medical care was high. Re-injuries tended to cause longer absence than non-re-injuries, which stresses the importance of avoiding re-injury.
Injury incidence and severity
Training and match injury incidences were similar to previous European Championships 2004–56 as well as the time loss match injury incidences reported from several FIFA tournaments.1–5 Match injury incidence increased with age in the men’s tournaments, indicating a greater risk with increased intensity of play. No gender-related difference in injury incidence was found when comparing the men’s and women’s Under-19 tournaments. This agrees with previous findings where similar injury rates were seen in the men’s 2004 and women’s 2005 EUROs.6 No obvious differences in training injury incidence were seen between tournaments, and incidences were generally low compared with elite club football.
The rate of severe injury in the men’s EURO 2008 (23%) was similar to the tournament in 2004 (27%)6 and this rate is considerably higher than that reported in men’s professional club football (9–15%) using the same methods.9–11 13 This could reflect the competitive nature of top international football, but it could also be a sign of player fatigue, as discussed previously. Forty-one per cent of injuries sustained in the European Championships 2006–8 resulted in absence after the tournament, with an average of nearly four weeks in rehabilitation after the tournament. This was also seen after tournaments 2004–56 and is a problem since players risk missing a vital part of their pre-season preparation, which may further increase their risk for injury during the regular club season.
Consequences of training injuries
Injuries sustained during training represented one fifth of all injuries, including six severe injuries. Having high player availability for training and matches is vital at top-level international football. The fact that training injuries were responsible for 26% of unavailability for match play shows that the impact of training injuries can be considerable even though the incidence of tournament training injury is low compared to club football. In an attempt to study the association between type of training and injuries at international tournaments we registered four different training categories. We found no correlation, however, between the type of training performed during a tournament and the injury incidence. The most likely explanation is that training exposures recorded as football-specific were also low intensity sessions with few contact situations and thereby no increased risk for injury as one might otherwise have suspected. Suggestions for improvement include adding an intensity measure for each training session, and to add more specific details regarding training content. This would enable the study of training intensity and content during international tournaments and their possible association with occurrence of injuries.
Injuries and performance
In the women’s 2005 EURO it was noted that teams that were eliminated in the group stage had a higher match injury incidence than teams advancing to the semi-finals, suggesting a correlation between injuries and performance.6 Furthermore, in a study of the Swedish national team over a 6-year period, an increased injury incidence during matches lost (52.5 injuries/1000 hours) compared with matches won or tied (22.7/1000) was observed, and it was suggested that injuries may have an impact on the match result due to a forced change in tactics or match strategy.22 We could not confirm these findings in the present study, by neither injuries and match results, nor team injury incidence and performance. This would suggest that tournament squads were rather homogenous as regards player skill, thereby enabling an injured player to be replaced with an equally skilled team mate.
Study strengths and limitations
The UEFA Injury Study has been implemented as a matter of routine in several European Championships starting with the men’s EURO in 2004.6 Some of the strengths of the study design are that team physicians report individual exposure and injuries during both training and match play, thereby providing a complete picture of the injury problem at major international tournaments. All injuries were followed to the final day of rehabilitation (except for three ACL tears) allowing us to evaluate the severity of injuries, and also the impact that injuries might have after the tournament. Exposure forms and injury cards were collected every third day of the tournament by a member of the study group on site. This meant that any uncertainties with data registration could be corrected immediately, thus ensuring high quality data and a high response rate. Since a time loss injury definition was used, minor bruises and overuse complaints without absence were not recorded. It is, however, unlikely that this has affected the inter-tournament comparisons in this study. The major limitation of this study is the small number of injuries, even though 12 European Championships were included. This limited our chances of comparing incidences of specific injury types between tournaments. The variation in injury rates between different years in the same age group was apparent, and in order to increase the power of inter-tournament comparisons, data from all tournaments within the same age group were aggregated for analyses.
What is already known on this topic
The match injury incidence at international tournaments is just as high, or even higher, than at professional club level.
Only limited data has been published on training injuries at tournaments, but this shows that the training injury incidence is slightly lower than at club level.
What this study adds
Training injuries were responsible for a quarter of match unavailability and may thus have a profound impact on team performance and should be the object of preventive measures.
Match injury incidence increased with age at men’s tournaments; no difference was observed between the men’s and women’s Under-19 tournaments.
Acknowledgments
The work of the team physicians who delivered data for the study is gratefully acknowledged. The help of J Diding , H Magnusson and L Sandersson with monitoring the data collection on site during the tournaments is greatly appreciated.
REFERENCES
Footnotes
Funding: The study was funded by UEFA.
Competing interests: None.