Article Text

Abstract
Sudden cardiac death in young competitive athletes is an important public health problem, although a relatively low-event-rate phenomenon. The single most common cardiovascular cause of these unexpected catastrophes is hypertrophic cardiomyopathy (HCM), accounting for about one-third of cases. Since the phenotypic expression of HCM is variable, and not uncommonly includes patients with mild and localised left ventricular hypertrophy, the differential diagnosis with physiological remodelling of athlete’s heart not uncommonly arises. This review discusses those non-invasive strategies that are useful in distinguishing the benign consequences of systematic athletic training from pathological left ventricular hypertrophy with the potential for sudden cardiac death. Preparticipation screening in healthy general athlete populations may raise the suspicion of HCM, and ultimately lead to definitive diagnosis. However, recently controversy has arisen regarding the most effective and practical strategy for the screening of athletes. European investigators have promoted routine 12-lead ECGs as part of a national mandatory programme distinct from the customary practice in the US which is limited to history and physical examinations. Consensus criteria and recommendations for eligibility and disqualification of athletes with HCM (and other cardiovascular abnormalities) have proved useful to the practising community.
Statistics from Altmetric.com
Sudden unexpected deaths of young trained athletes are highly visible events with devastating emotional impact on families, physicians and the community at large.1 2 Once regarded as rare personal and family tragedies, sudden deaths in young athletes have become increasingly integrated into the public discourse. Although a focal point first in the US in the early 1980s,3 this issue has now become one of increasing concern in many parts of the industrialised world, particularly in Europe.4 5 The visibility afforded this medical issue in the US is underscored by the highly publicised sudden deaths of several elite or professional athletes, Hank Gathers2 and Reggie Lewis (with myocarditis), and more recently by three sudden deaths or cardiac arrests which occurred in professional athletes due specifically to hypertrophic cardiomyopathy (HCM): Jason Collier (basketball), Thomas Herrion (football), Jiri Fischer (hockey) and more recently a cluster of several athletes from Europe, South American and Africa including Marc-Vivian Foe (Cameroon; soccer) who died during a televised international match, previously diagnosed as having HCM.6 7
Because of the public visibility generated by athletic field deaths and the potentially adverse consequences of underlying cardiovascular diseases in young athletes, considerable attention has understandably been directed toward the clinical distinction between physiologically based athlete’s heart and HCM,8 9 the most common cause of sudden death in young people.10 This differential diagnosis has critical implications for dedicated athletes (and their physicians) because HCM (and other cardiovascular diseases) may represent the basis for disqualification from most intense competitive sports to reduce the arrhythmic risk for sudden death.11 12 On the other hand, improper overdiagnosis of cardiac disease in an athlete may lead to unnecessary withdrawal from competitive sports, depriving that individual of the varied psychological and sometimes economic benefit of athletic participation. Finally, legal liability incurred by evaluating athletes with cardiovascular disease has raised the general level of anxiety within the practising community, surrounding decision-making in these clinical situations.13
Overall magnitude of the problem
Sudden deaths of young competitive athletes is recognised as an important public health problem.1 While apparently uncommon,14 the absolute frequency with which these catastrophes occur has been controversial. Recently, the number of sudden deaths in US competitive athletes was estimated from the large national Sudden Death in Young Athletes’ registry assembled over a 27-year period (1980–2006), employing systematic identification and tracking strategies.10 A total of 1866 athletes who died suddenly (or survived cardiac arrest) were identified in 38 diverse sports (fig 1). Ages were 19 (SD 6) years, about 90% were male, and 82% of the events occurred during or just following physical exertion.

Number of cardiovascular (CV) sudden death events in 1866 US young competitive athletes, tabulated by year from the US national registry, shown in comparison with blunt trauma-related and other causes of these deaths (eg, commotio cordis, heat stroke, illicit drugs, pulmonary disease). Reproduced with permission of American Heart Association; from Maron et al.10
Sudden deaths were predominantly due to cardiovascular disease (56%), most commonly HCM, but also included blunt trauma causing structural bodily damage (22%), commotio cordis (4%) and heart stroke (2%). The highest number of cardiovascular disease-related events in a single year was 76, with an average of 66/year over the most recent 6 year period (fig 1). An estimated one-third of the diseases causing sudden death would not have been reliably identified by preparticipation screening (even with 12-lead ECG incorporated into the screening process). The absolute number of cardiovascular sudden deaths in this Registry was somewhat higher than previously estimated, but nevertheless relatively low (<100/year). The relative infrequency of these cardiovascular deaths unavoidably impacts considerations for mandatory national preparticipation screening programmes, similar to that suggested by Italian investigators12 and others.15
Cardiovascular diseases
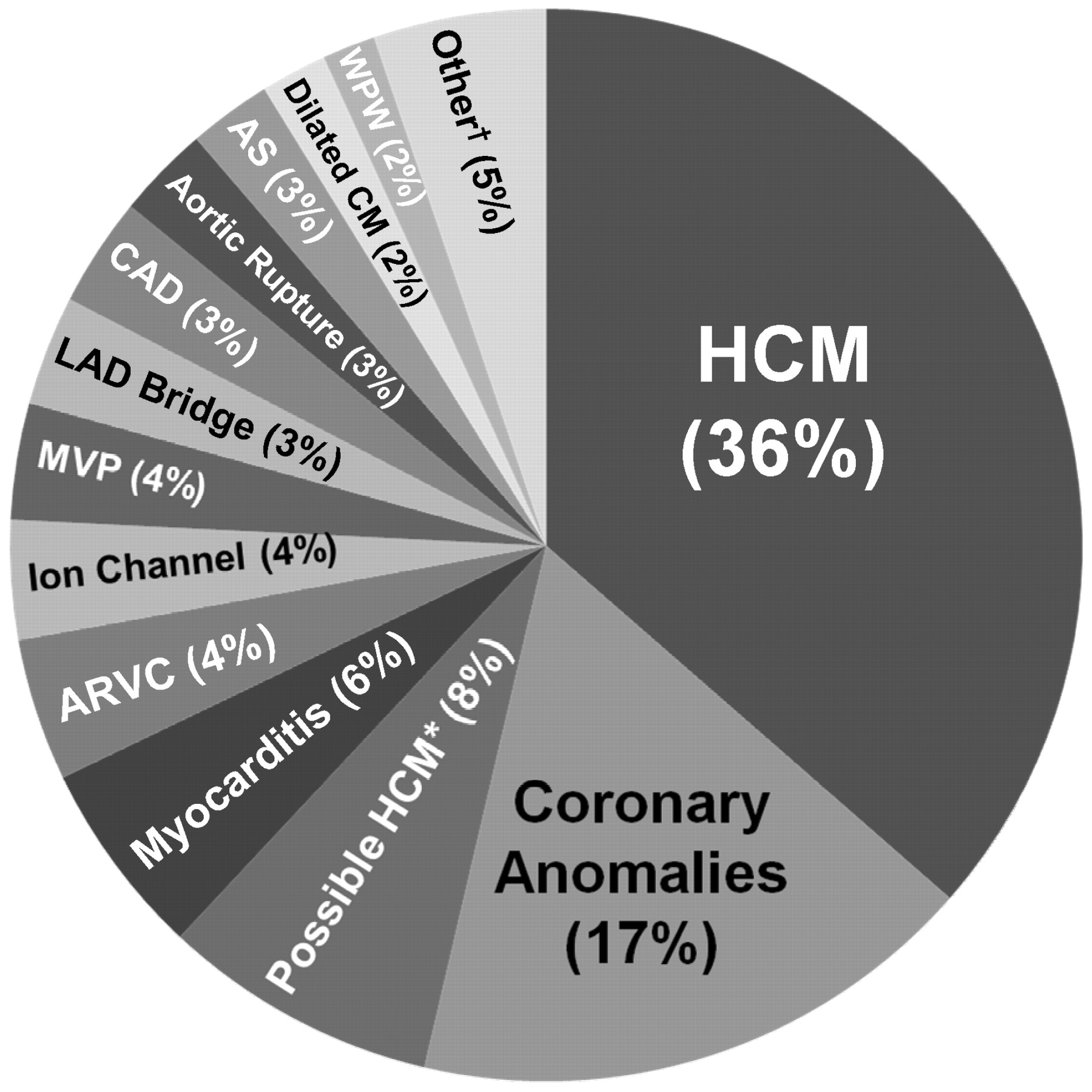
The usually clinically silent cardiovascular diseases that predispose athletes to sudden death (largely by virtue of lethal ventricular tachyarrhythmias) have been documented in the autopsy-based US registry (fig 2).10 16 17 HCM is the single most common disease causally linked to athletic field deaths, accounting for about one-third, with congenital coronary artery anomalies (largely those of wrong sinus origin) responsible for 15–20%. A diverse array of 15 other diseases each account for a much smaller proportion of deaths (1–8%) including myocarditis, aortic stenosis, dilated cardiomyopathy and arrhythmogenic cardiomyopathy (ARVC), the most common cause of sudden death in young athletes in the Veneto region of Italy.4 12 18
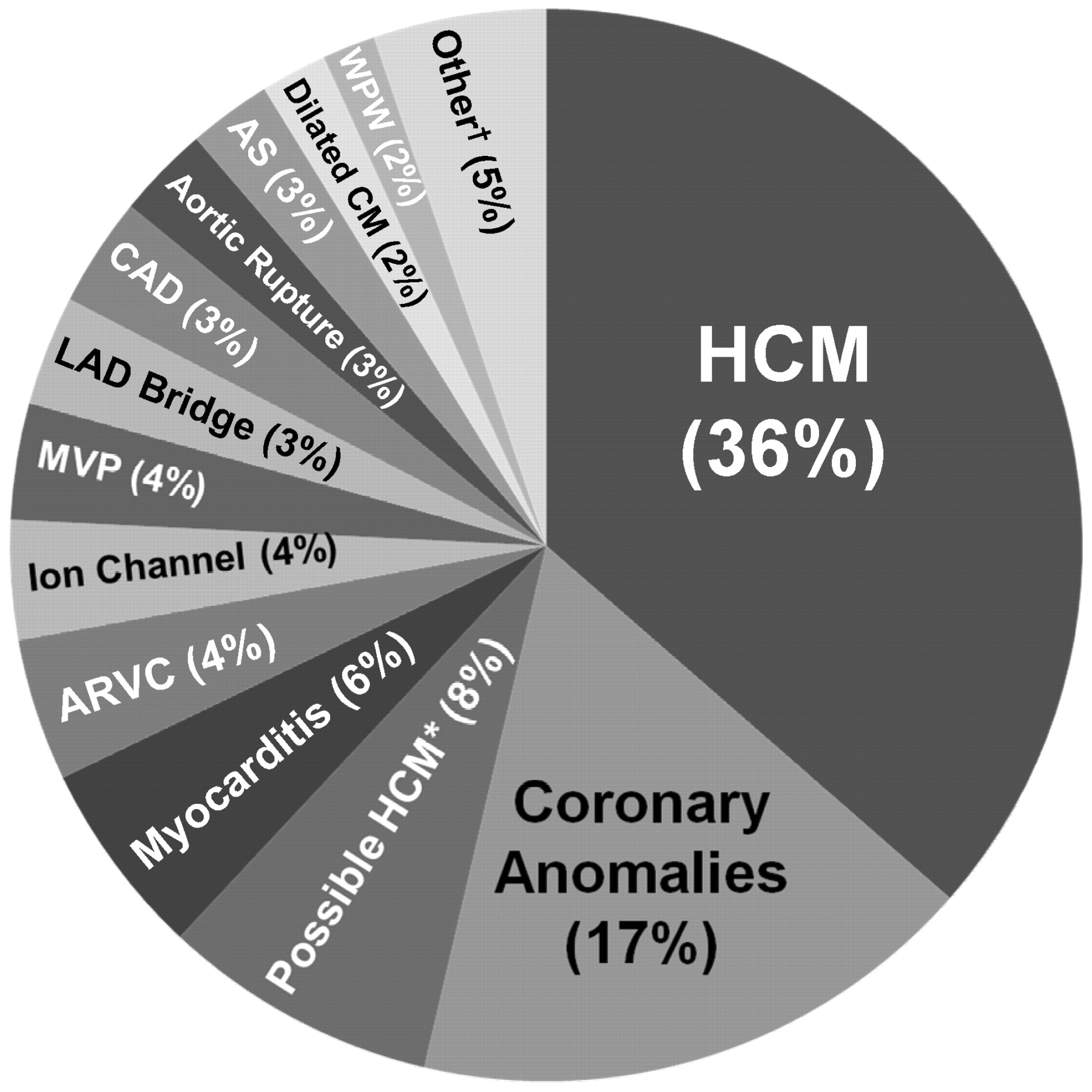
Cardiovascular causes of sudden death in young competitive athletes, taken from US national registry of 1866 athlete deaths.10 †Congenital heart disease (n = 8); myocardial infarction (n = 6); Kawasaki disease or related conditions (n = 5) sickle cell trait (n = 5); sarcoidosis (n = 4); stroke (n = 3); cardiac tumour (n = 1); conduction system disease (n = 2); and miscellaneous ( = 2). *Regarded as possible (not definitive) evidence for hypertrophic cardiomyopathy (HCM) at autopsy with mildly increased left ventricular (LV) wall thickness (18 (SD 4) mm) and heart weight (447 (SD 76) g). Ao, aorta; ARVC, arrhythmogenic right ventricular cardiomyopathy; AS, aortic stenosis; CM, cardiomyopathy; CAD, atherosclerotic coronary artery disease; LAD, left anterior descending; MVP, mitral valve disease; WPW, Wolff–Parkinson–White.
African–Americans account for a disproportionate number of sports-related sudden death5 owing to previously undiagnosed HCM.17 This contrasts sharply with the under-representation of African–Americans in clinically identified HCM populations, suggesting that socio-economic status and ethnicity may play an important role in determining access to echocardiography and consequently the clinical diagnosis of HCM.17
Circumstantial evidence suggests that vigorous physical exertion as part of sports participation acts as a trigger for lethal ventricular tachyarrhythmias in HCM, given the susceptibility imposed by the underlying (and usually unsuspected) arrhythmogenic substrate. Consequently, differential diagnosis between HCM and physiological (ie, non-pathological) left ventricular (LV) hypertrophy associated with systematic training (“athlete’s heart”) has become an important and not uncommon clinical dilemma.7 8 9 19
Athlete’s heart
Historical perspectives
Recognition that the cardiovascular system of trained athletes differs structurally and functionally from others in the normal general population extends over 100 years.20 During that time, there has also been periodic controversy about the true nature of athlete’s heart, that is, whether the findings are physiologically adapted, benign and related only to training, or alternatively are potentially pathological and the harbinger of disease and disability.
The clinical entity of athlete’s heart has been defined with increasing precision using a variety of techniques. Henschen is credited with the first description (in 1899), using only a basic physical examination with careful percussion to recognise enlargement of the heart caused by athletic activity in cross-country skiers.21 Henschen concluded that both dilatation and hypertrophy were present, involving both the left and right sides of the heart, and that these changes were normal and favourable.
Subsequent investigators used quantitative chest radiography to show that heart size was increased in athletes, particularly those engaged in endurance sports with large aerobic requirements. Some early observers even regarded the heart of the trained athlete to be weakened owing to the “strain” created by continuous and excessively strenuous training and believed that athletes were subject to deteriorating cardiac function and heart failure.20
Physiology
Cardiovascular adaptations to exercise have been systematically defined22 and differ with respect to the type of conditioning: endurance training (sometimes also described as dynamic, isotonic or aerobic) such as long-distance running and swimming; and strength training (also referred to as static, isometric, power or anaerobic) such as wrestling, weightlifting or throwing heavy objects.23 Sports such as cycling and rowing are examples of combined (and intense) endurance and strength exercise.
Long-term cardiovascular adaptation to dynamic training produces increased maximal oxygen uptake due to increased cardiac output and arteriovenous oxygen difference. Strength exercise results in little or no increase in oxygen uptake. Thus, endurance exercise predominantly produces volume load on the left ventricle (LV), and strength exercise causes largely a pressure load.
Chamber morphology
Cardiac dimensional alterations associated with athletic training have been defined over the past 35 years in a number of cross-sectional echocardiographic or cardiovascular magnetic resonance studies, usually performed in highly trained individuals.24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 The responses of individual athletes to systematic conditioning are heterogeneous. In about 50% of athletes, training induces some evidence of cardiac remodelling, which may consist of alterations in ventricular chamber dimensions, including increased LV wall thickness (fig 3) and LV and right ventricular and left atrial cavity size (and volume), associated with normal systolic and diastolic function.
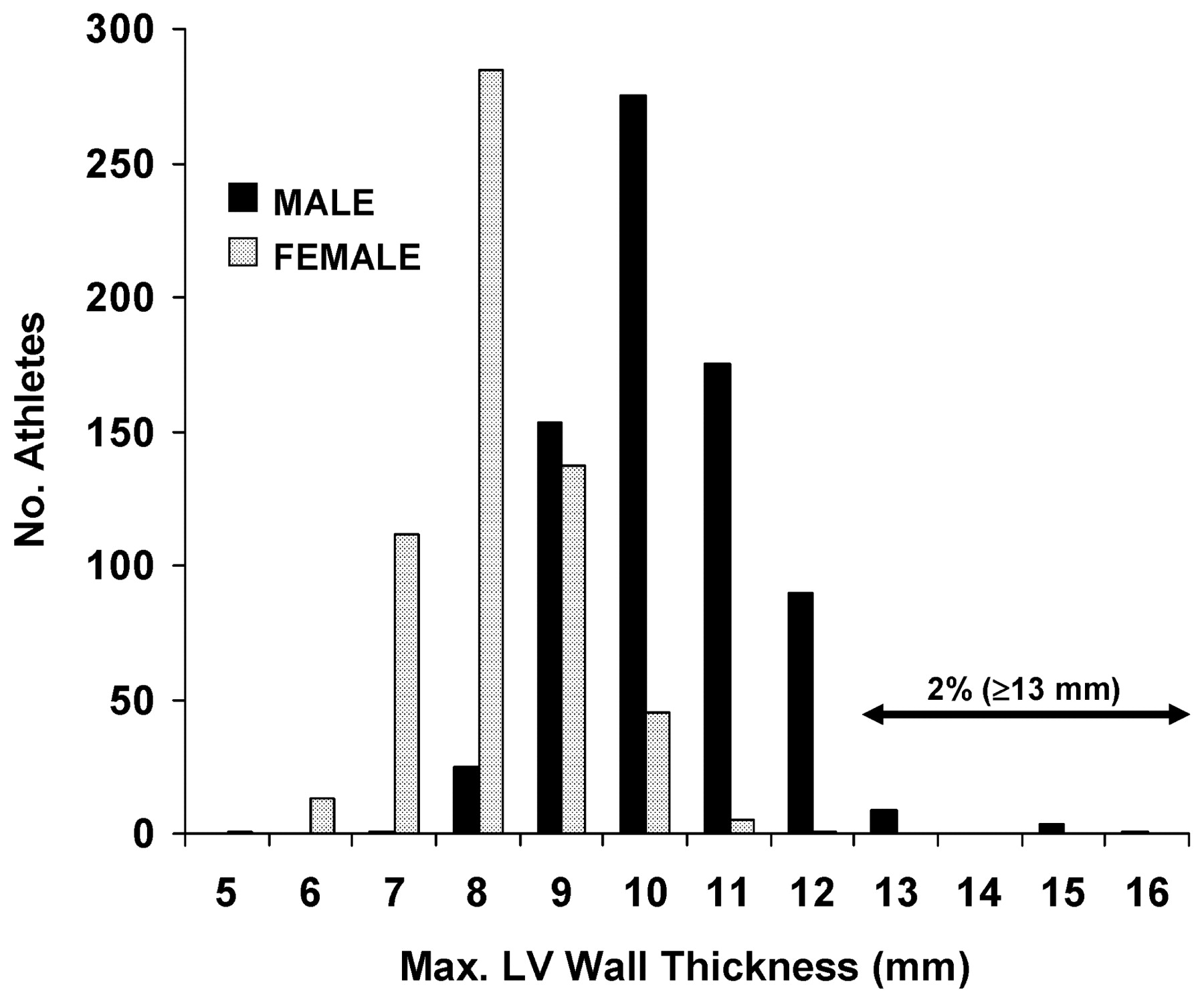
Distribution of maximum left ventricular (LV) wall thicknesses in a large young male and female athletic population. Two per cent of male and 0% of female athletes have a wall thickness ⩾13 mm in the ambiguous “grey-zone” of athlete’s heart versus hypertrophic cardiomyopathy. Reproduced from Pelliccia et al,25 with permission of the Massachusetts Medical Society.
Chamber enlargement is occasionally accompanied by a relatively mild increase in absolute LV wall thickness exceeding upper normal limits (>12 mm) that may mimic HCM.23 Training-related LV remodelling with changes in mass is dynamic and may develop rapidly or more gradually, after the initiation of a vigorous conditioning programme.34 35 36 42 However, it should be underscored that there is considerable overlap in cardiac dimensions between a trained athlete population and age- and sex-matched sedentary controls47 with athletes showing relatively small (but statistically significant) increases of 10–20% for wall thickness (or cavity size), with these values remaining within accepted normal limits in most individual athletes.47
The pattern and magnitude of physiologically increased LV mass may vary with respect to the nature of sports training.29 42 46 One meta-analysis31 and also the large database assembled at the Institute of Sports Medicine and Science (Rome)7 25 26 27 36 37 38 44 46 support an early hypothesis24 that specific morphological adaptations and changes in LV mass result from systematic training in different sports disciplines. The most extreme increases in LV wall thickness have been observed in those elite athletes training in rowing, and cycling (fig 4),7 25 26 27 36 37 38 whereas limited data available in those athletes participating in ultra-endurance sports (such as triathlon) paradoxically show more modest alterations in cardiac dimensions.1 28

Role of type of sport. Effect of specific sports training on maximum end-diastolic left ventricular (LV) wall thickness (and transverse cavity dimension) in elite athletes, representing 27 different sporting disciplines. L.D., long-distance running; X-country, cross-country.
Of note, some misunderstanding persists as to whether strength training (eg, wresting, weight lifting) alone results in LV hypertrophy. Such sports are associated with only mild increase in wall thicknesses (although often disproportionate to cavity size), whereas absolute values uncorrected for body surface area usually remain well within the accepted normal range (⩽12 mm).1 31 43 44 46 47
Twelve-lead ECGs
In cross-sectional analysis, a spectrum of abnormal ECG patterns was present in about 40% of trained athletes, occurring twice as commonly in men than in women, and particularly in those participating in endurance sports.48 Therefore, most athletes have ECGs that are within normal limits or show only minimal alterations. However, the frequency with which these altered ECG patterns occur is highly dependent on the type, intensity and level of training and precise criteria used to define normality, as well as the race of the athletes. This situation underscores the need for more extensive cardiac dimensional data in diverse athlete populations. Indeed, in highly trained American football players, Magalski et al49 found that ECG abnormalities (including distinctly abnormal or bizarre patterns most suggestive of cardiac disease) were twice as common in black than white athletes, with race an independent determinant of the ECG pattern. There is also some evidence that LV wall thicknesses in black athletes exceed those in Caucasians (on average by 1.3 mm) with implications for the clinical diagnosis of HCM.50
The most commonly reported 12-lead ECG pattern alterations in athletes are early repolarisation, increased QRS voltages, diffuse T-wave inversion and deep and narrow Q waves.22 48 51 Distinctly abnormal and bizarre ECG patterns, intuitively suggestive of cardiac disease, are encountered in an important minority of elite athletes without structural disease (about 15%).48
Arrhythmias
Because of the heightened vagal tone that accompanies physical conditioning, trained athletes are known to commonly incur innocent arrhythmias and conduction alterations, such as sinus bradyarrhythmia, junctional rhythm and first-degree or Wenckebach AV block (Mobitz type I).1 41 48 51 However, the application of ambulatory (Holter) ECG monitoring to trained athletes has also commonly documented substantial ectopy with frequent premature beats and complex ventricular tachyarrhythmias (including couplets and bursts of non-sustained ventricular tachycardia), usually unassociated with underlying cardiovascular abnormalities or the magnitude of LV mass.52 53 54 Such arrhythmias appear to be yet another manifestation of the benign athlete’s heart spectrum.
Indeed, most ventricular tachyarrhythmias (including non-sustained ventricular tachycardia) occurring in highly trained athletes are not associated with adverse clinical consequences and are usually abolished or substantially reduced after relatively brief periods of deconditioning. Even in athletes with heart disease, resolution of ventricular tachyarrhythmias with deconditioning is common and may represent a potential mechanism by which sudden death risk is reduced by the withdrawal of such individuals from training and competition,55 56 in accord with consensus panel recommendations.11 12
Although data defining the physiological and morphological adaptations of systemic training are considerable, it is nevertheless unresolved whether the current profile of athlete’s heart can be extrapolated to all subgroups within this physically active and heterogeneous population, including those of different ages, sports disciplines and racial or ethnic origin.25 31 40 49 57 Much (but not all)50 of the available echocardiographic data have been assembled in athletes of white European descent, particularly the large cohort at the Institute of Sports Medicine and Science comprising elite Italian national and international level competitors.25 26 27 36 37 38 44 46 52 53 54 This situation underscores the need for additional cardiac dimensional data in diverse athlete populations.
Strategies for differential diagnosis
HCM is the most common genetic heart disease, caused by mutations in 11 genes encoding proteins of the cardiac sarcomere, with the phenotype characterised by a hypertrophied and non-dilated LV in the absence of another cardiac or systemic diseases capable of producing the degree of hypertrophy evident.58 59 The characteristic echocardiographic marker is increased LV wall thickness, which may range in the clinical arena from mild (13–15 mm) to massive (>50 mm), although any wall thickness is compatible with the presence of the genetic substrate, since both adult and child gene carriers may express normal wall thickness.58 59
An algorithm to resolve the dilemma regarding differential diagnosis between HCM (with mild phenotypic expression)58 59 60 and extreme physiological hypertrophy of athlete’s heart due to LV remodelling adaption has evolved. This issue has particular relevance to trained athletes in whom LV wall thickness falls outside clinically accepted partition values25 (eg, ⩽12 mm at end-diastole; somewhat lower cut-points apply to female27 and adolescent40 athletes) into a “grey zone” of overlap between these two clinical scenarios: ventricular septal thickness of 13–15 mm, which can be expected in about 2% of highly trained male athletes in certain sports (figs 3, 5).7 25 Of note, this clinical distinction is relevant only to HCM with outflow obstruction under resting (basal) conditions, in which mitral valve systolic anterior motion (SAM) is absent, since marked SAM itself is inconsistent with athlete’s heart, and its presence would strongly suggest the diagnosis of HCM.7 8 9 19 34 35 36 56 60 61 62 63 Of note, racial differences in LV wall thicknesses may also impact this differential diagnosis, as the somewhat greater septal dimensions in some black athletes may generate false-positive diagnoses of HCM.50

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Differential diagnosis. Clinical criteria used to distinguish hypertrophic cardiomyopathy (HCM) from athlete’s heart when maximal left ventricular (LV) wall thickness falls within the shaded grey area of overlap, consistent with both diagnoses. Adapted from Maron et al,19 with permission of the American Heart Association. CMR, cardiovascular magnetic resonance.
This diagnostic ambiguity can be resolved by the application of a number of non-invasive parameters, such as reduction in LV mass after short deconditioning periods (most reliably assessed with serial cardiovascular magnetic resonance imaging) or absolute transverse LV end-diastolic dimension ⩾55 mm, both of which are most consistent with athlete’s heart. LV dimensions >55 mm are common in trained athletes but rare in HCM in which cavity size is most often <45 mm and dimensions of >55 mm are usually confined to the end-stage phase with progressive heart failure and systolic dysfunction.64 In contrast, an HCM diagnosis would be favoured by abnormal pulsed and tissue Doppler-derived indices of LV diastolic filling with impaired relaxation (ie, since these parameters are always normal in athlete’s heart),60 62 or by documentation of a family member with HCM. In addition, cardiovascular magnetic resonance may have considerable value in resolving the HCM vs athlete’s heart differential diagnosis in selected athletes by virtue of its superiority over echocardiography in detecting segmental LV hypertrophy diagnostic of HCM present in the anterolateral free wall, posterior ventricular septum, or apex,65 66 67 or the demonstration of delayed enhancement (postgadolinium infusion), indicative of replacement fibrosis.68
Gender differences in cardiac dimension are often relevant to differential diagnosis. Highly trained female athletes rarely show absolute LV wall thicknesses >11 mm. Indeed, of 600 elite woman athletes in one study,27 none had LV thickness in the range compatible with the diagnosis of HCM (⩾13 mm) (fig 3). Therefore, female athletes presenting with “grey zone” LV wall thickness of 13–15 mm (and normal cavity size) are most likely to have HCM.
Rapid commercial laboratory testing is now available for both HCM (and cardiac ion channel mutations), with the potential for achieving a DNA-based diagnosis. If a proband is positive for one of the mutations known to be disease-causing, the result is definitive. On the other hand, genetic testing has certain potential limitations. For example, negative tests are common (about 50%) and non-diagnostic, since they usually represent false-negative results. In addition, commercial testing can be costly, and it is currently unpredictable as to whether the expense will be covered by insurance carriers. However, if the family mutation is known, then all other relatives can be tested definitively, rapidly and inexpensively.
Complex and frequent ventricular tachyarrhythmias evident on ambulatory Holter ECG in trained athletes without cardiovascular abnormalities can raise the possibility of disease states such as myocarditis, for which a high index of clinical suspicion is required for diagnosis. Periods of forced deconditioning may not be useful in resolving the differential diagnosis of myocarditis versus athlete’s heart, since detraining is associated with reduction (and even abolition) of ventricular tachyarrhythmias in athletes with or without underlying pathological substrates.53
Preparticipation screening and HCM
The reliable detection of HCM within general healthy populations, such as with the screening of young athletes for cardiovascular disease, has proved complex. The detection rate of HCM with history and physical examination screening in athlete populations (customary in the US) appears to be relatively low,7 16 largely due to the frequent absence of a loud heart murmur, a family history of the disease, or prior symptoms such as syncope. Nevertheless, it should be underscored that history and physical examination screening do have the capability of raising the suspicion of HCM; indeed, 3% of new referrals to the HCM Center in Minneapolis have been specifically identified de novo by virtue of preparticipation athlete screening.69
Italian investigators have emphasised the capability of mass screening for HCM with routine 12-lead ECGs.5 12 18 56 However, there are a number of considerations and limitations related to the recognition of HCM among large athlete populations. First, there is the issue of false negatives. While the majority of HCM patients show abnormalities on the ECG that may raise suspicion of underlying cardiac disease with screening, an important minority (ranging from 5 to 20%, depending on patient selection) show innocent appearing normal or near-normal ECGs.70 Second, 10 to 20% of screened athletes will have false-positive examinations due largely to ECG alterations.18 71 72 While the vast majority of such ECGs represent only extreme manifestations of physiological athlete’s heart,48 a pattern of marked repolarisation abnormalities with diffusely distributed and deeply inverted T-waves has been associated with the development over time of high-risk cardiac diseases such as HCM (and also ARVC).73 Therefore, markedly abnormal ECGs in young and apparently healthy athletes can occasionally represent the initial expression of underlying cardiomyopathies (including HCM) that may not be evident until years later and can be associated with adverse outcome.73 Athletes with such ECG patterns merit continued clinical surveillance, even after their sports careers have ended.
Italian investigators have also attributed a decline in the rate of sudden cardiac death, in athletes in the Veneto region of northeastern Italy, to the longstanding national systematic preparticipation screening programme, which routinely includes a 12-lead ECG.4 5 18 56 They have reported a 90% decline in the annual incidence of sudden cardiovascular death in competitive athletes (owing largely to reduced mortality from cardiomyopathy). However, recent data from the US emphasise that the low mortality rate attributable to cardiovascular diseases (including HCM) in trained athletes over the last decade, has not differed significantly from that in the Veneto region of Italy.74 Such observations as well as numerous practical obstacles impede the adoption and incorporation of a mandatory and national cardiovascular preparticipation screening programme with routine ECGs legally binding into the present US healthcare system.75
Cardiovascular disease and disqualification from sports
Criteria
The devastating impact of even relatively infrequent sudden deaths of young athletes offers justification for restriction from competition to reduce the risk related to silent and unsuspected cardiac disease. For athletes in whom cardiovascular disease has been identified (either by preparticipation screening or under other circumstances), important considerations arise with respect to the appropriate eligibility and disqualification decisions for competitive sports. The American College of Cardiology 36th Bethesda Conference11 and the European Society of Cardiology (ESC)12 consensus documents offer expert panel recommendations and clear benchmarks for clinical practice, largely focused on amateur competitive athletes. Panel recommendations for athletic eligibility are based on the premise that intense sports training and competition increase risk for sudden death or disease progression in susceptible athletes with heart disease, and that conversely this risk can be reduced or minimised by either temporary or permanent withdrawal from sports. Indeed, the US appellate court decision in Knapp v Northwestern University76 supports the use of national association medical guidelines (such as those of the Bethesda Conference) in justifying disqualification decisions in athletes. Therefore, team physicians would be prudent to rely on the Bethesda Conference recommendations in making difficult but important disqualification decisions, because this document will likely play an important role as precedent in resolving future medical-legal disputes. Those athletes disqualified with HCM may become high risk patients eligible for primary prevention implantable cardioverter-defibrillators should risk markers related to their disease be present.77
The recent ESC consensus report assessing eligibility criteria for competitive athletes with cardiovascular disease is modelled after the Bethesda Conference. Although the two guidelines are very similar, the European recommendations are selectively more restrictive in advising disqualification for certain cardiac conditions, including HCM, particularly when diagnostic cardiac findings are not definitive.78
Societal and legal implications
However, decisions to withdraw elite athletes from competitive sports due to the recognition of HCM and other heart diseases are not uncommonly confounded by complex societal considerations and consequently can be difficult to implement, particularly when elite or professional sports careers are involved. Many such athletes are highly motivated to remain in the competitive arena, may not fully appreciate the implications of the relevant medical information presented to them, and are willing to accept risks while at the same time resisting prudent medical recommendations to withdraw.79 80 Also, as a cautionary note, physician judgement in making these medical eligibility/disqualification decisions can be impaired insidiously by extrinsic pressures imposed by relatives, fans, alumni, coaching staff, administrators and other interested parties, particularly when athletes “shop” for multiple medical opinions.1 2 7
The relationship between sports medicine and the law is complex and involves relationships between physicians, athlete-patients, teams and institutions. Indeed, liability issues relevant to the management of competitive athletes with cardiovascular disease have become of increasing concern to the practising medical community, given that several athlete deaths have triggered attempts to hold physicians legally responsible and accountable for alleged grievances.2 An evolving US medicolegal framework13 80 is clarifying the standard of care associated with the practice of eligibility/disqualification decision-making, while upholding the wisdom of withholding selected student-athletes with cardiovascular abnormalities from access to competitive sports programmes in an effort to prevent their exposure to medically unacceptable risks.80
What is already known on this topic
Hypertrophic cardiomyopathy (HCM) is the leading cause of sudden cardiac death in young competitive athletes in the US.
The distinction of physiological remodelling of athlete’s heart from pathological left ventricular (LV) hypertrophy in HCM is challenging with important implications for preparticipation screening.
What this study adds
HCM is caused by mutations in 11 genes encoding proteins of the cardiac sarcomere with variable phenotypic expression, but characterised by a hypertrophied and non-dilated left ventricle.
The distinction of pathological versus physiological hypertrophy in cases of “grey zone” ventricular wall thickness (ie, 13–15 mm) can be resolved by the application of a number of non-invasive parameters such as family history of HCM, but also reduction of LV mass after deconditioning periods (most reliably assessed by serial cardiovascular magnetic resonance imaging) or an absolute transverse LV end-diastolic dimension ⩾55 mm, both of which are most consistent with athlete’s heart.
Cardiovascular magnetic resonance may have considerable value in resolving the HCM versus athlete’s heart differential diagnosis in selected athletes by virtue of its superiority over echocardiography in detecting segmental LV hypertrophy diagnostic of HCM that may be present in the anterolateral free wall, posterior ventricular septum, or apex, or the demonstration of delayed enhancement (post-gadolinium infusion), indicative of replacement fibrosis.
REFERENCES
Footnotes
Competing interests None.
Provenance and peer review Commissioned; not externally peer reviewed.