Article Text

Abstract
Background Regular intensive physical activity is associated with non-pathological changes in cardiac morphology. Differential diagnosis with arrhythmogenic right ventricular cardiomyopathy (ARVC) constitutes a frequent problem, especially in athletes showing ventricular arrhythmias with left bundle branch block morphology.
Aim of the study To assess the different clinical and non-invasive instrumental features of the subjects affected by ARVC and by athletes.
Methods Three groups of subjects (40 ARVC patients, 40 athletes and 40 controls, mean age 27 (9) years) were examined with family and personal history, physical examination, 12-lead ECG, 24-h ECG, signal-averaged ECG and 2-D and Doppler echocardiography.
Results 12-Lead ECG was abnormal in 62% of ARVC patients versus 7.5% of athletes and 2.5% of controls (p<0.0001). Ventricular arrhythmias and late potentials were present in 70% and 55% of ARVC subjects, respectively (vs 5% of athletes and 7.5% of controls, p<0.0001). Left ventricular parietal wall thickness and left ventricular end-diastolic diameters were significantly higher in athletes. Both athletes and ARVC patients presented a right ventricular (RV) enlargement compared with controls. Moreover, RV outflow tract, measured on parasternal long axis and at the level of aortic root, was significantly larger in ARVC patients (33.6 (4.7) mm vs 29.1 (3.4) mm and 35.6 (6.8) mm vs 30.1 (2.9) mm; p<0.0001), and RV fractional shortening and ejection fraction were significantly lower in ARVC patients compared with athletes (40 (7.9)% vs 44 (10)%; p=0.05 and 52.9 (8)% vs 59.9 (4.5)%; p<0.0001). A thickened moderator band was found to be present in similar percentage in ARVC patients and athletes.
Conclusions An accurate clinical and instrumental non-invasive evaluation including echocardiography as imaging technique allows to distinguish RV alterations typical of ARVC from those detected in athletes as a consequence of intensive physical activity.
Statistics from Altmetric.com
Regular intensive physical activity is associated with non-pathological changes in cardiac morphology, referred to as “athlete’s heart”.1,–,4 The differential diagnosis between this condition and some cardiac diseases potentially at risk of sudden death constitutes an important and frequent problem.
In the past years, many studies focused on left ventricular (LV) morphological adaptations induced by athletic training and on the possible criteria used in distinguishing athlete’s heart from hypertrophic cardiomyopathy.5,–,7 Nonetheless, in athletes’ population, the presence of right-sided chambers adaptations, and in particular, dilatation, were described and have to be considered in the differential diagnosis with arrhythmogenic right ventricular cardiomyopathy (ARVC), which is an important cause of juvenile sudden death.8 9
This is absolutely important when dealing with athletes showing ventricular arrhythmias with left bundle branch block morphology or 12-lead ECG abnormalities such as right ventricular conduction delay or negative T wave in the precordial leads. Nonetheless, although different studies examined the RV modifications induced by physical activity,[10, 11] none pointed out on the differences between athletes’ heart and ARVC.
Even if cardiac magnetic resonance is the ideal tool to evaluate RV features, in the clinical practice, it cannot be used systematically to analyse RV adaptations induced by effort. On the contrary, two-dimensional echocardiography performed with an accurate protocol can play an important role in detecting RV abnormalities, also considering the good acoustic windows usually found in young subjects. Thus, in the present study, we compared the non-invasive clinical and instrumental features detected in subjects affected by ARVC and in athletes, including echocardiography as imaging technique, with the aim to assess the possible differences between these two conditions.
Methods
Study population
Three groups of different subjects were examined (table 1).
Baseline characteristics of the three groups
Group I consisted of 40 consecutive patients affected by ARVC (28 men and 12 women, mean age 28 (8) years; range 14–42 years), fulfilling the established diagnostic criteria.12 ARVC patients with severe dilation of the RV-right ventricular end-diastolic volume (RVEDV) >85 ml m2, RV diastolic area (RVAd) >30 cm2, RV ejection fraction (RVEF) <45%, RV fraction area change (RVFAC) <30% were excluded from the study.13 14 Seventeen ARVC subjects had a family history of ARVC, with cases of juvenile sudden death in five.
Group II was composed of 40 highly trained athletes (28 males and 12 females; mean age 26 (5) years; range 20–38 years). They were engaged in soccer (n=28.70%), volleyball (n=10.25%) and running (n=2.5%). All subjects were competing for 5.2 (4) years (range 2–11 years); the total amount of hours of intensive training averaged 7 (1.7) h week-1 (minimum, 4; maximum 10 h week-1). None of them presented a family history of ARVC and/or of juvenile sudden death related to cardiovascular diseases.
Group III consisted of 40 volunteer healthy controls age- and sex-matched (30 men and 10 women; mean age 28.5 (12) years; range 20–38 years) who did not practice any physical activity. All subjects had normal physical examination, including blood pressure, and none presented symptoms of underlying cardiovascular diseases or family history for juvenile sudden death.
Study protocol
It included 12-lead ECG, 24 h Holter monitoring, signal-averaged ECG (SAECG) and 2-D and Doppler echocardiography.
Twelve-Lead ECG
The following ECG parameters were analysed: incomplete or complete right bundle branch block, negative T wave in the precordial leads, epsilon wave, mean QRS duration value, ST segment elevation ≥2 mm in V1–2. Moreover, Sokolow voltage criteria (sum of the S wave in V1 and R wave in V5>3.5 mV) were used to identify LV hypertrophy.15 As recommended by the International Society and Federation of Cardiology task force criteria published in 1994, the presence of negative T waves was not considered abnormal in patients with complete right bundle branch block.12 The presence of negative T wave was considered abnormal when present in at least V1–2. The epsilon wave was defined as a distinct wave of low amplitude localised immediately after the QRS complex, usually in the precordial leads.
Ventricular arrhythmias
Ventricular arrhythmias recorded on 24 h Holter ECG or 12-lead ECG (Mortara Rangoni, Italy) were classified into four groups: premature ventricular complexes both isolated and in couplets or triplets, non-sustained ventricular tachycardia (VT), sustained VT (when lasted more than 30 s).
Signal-averaged ECG
SAECG was performed using a MAC 15 system (Marquette Milwaukee, Wisconsin, USA). Time–domain analysis was obtained in each patient using three different filters at 25, 40, 80 Hz. At each filter setting, the following parameters for each filter were obtained: filtered QRS duration (QRSD), high-frequency low-amplitude signal duration in the terminal portion of the QRS (HFLA), root mean square of the voltage in the last 40 ms of the filtered QRS (RMS).For the 80 Hz filter, RMS was automatically calculated from the last 20 ms of the filtered QRS. The average number of analysed beats varied from 250 to 400 with a noise level <0.7 μV. Normal values for our laboratory were established by analysing the recordings of 146 healthy subjects, matched for sex and age, who had a normal ECG and a QRSD<90 ms. The normal values were (95% CI): for the 25 Hz filtered QRSD<120 ms, HFLA<40 ms, RMS>25 μV; for the 40 Hz filtered QRSD<118 ms, HFLA<40 ms, RMS>20 μV; for the 80 Hz filtered QRSD<106 ms, HFLA<34 ms, RMS>12 μV. The SAECG was considered positive when at least two parameters were abnormal at one filter setting.16
Echocardiography
Two-dimensional echocardiography was performed by two experienced operators, using a Hewlett Packard Sonos 5500 (Andover, Massachusetts, USA) with S4 probe. Images of the heart were obtained in the standard parasternal long axis and short axis, apical four-chamber and subcostal view. LV volumes were calculated using an ellipsoid biplane area–length model derived from LV images in the apical four-chamber view.17 The ejection fraction was calculated using the formula: end-diastolic volume minus end-systolic volume divided by end-diastolic volume. End-diastolic and end-systolic RV volumes were calculated using an area–length method derived from orthogonal planes (apical four-chamber and short-axis subcostal views).18 A ratio between RVEDV and LV end-diastolic volume (LVEDV) was also calculated. Moreover, RV cavity dimensions were also obtained according to Foale et al,19 with the evaluation of right ventricular outflow tract (RVOT) and RV inflow tract (RVIT) dimensions (fig. 1). From the outflow tract, we measured RVOT1 (calculated from the anterior RV wall to the RV septum in parasternal long-axis view), RVOT3 (just below the pulmonary valve annulus) and RVOT4 (maximum distance between the anterior aortic wall and the RV free wall in parasternal short axis view). From the inflow tract, we measured RVIT1 (one-third of the distance below the annulus towards the RV apex, parasternal long-axis view), RVIT2 (maximum distance between the right side of the mid-interventricular septum to the RV free wall) and RVIT3 (within one-third of the distance below the tricuspid valve annulus). Moreover, RV long axis (LAX: from the RV apex to the mid-point of the tricuspid annulus) and short axis (SAX: middle third of the RV) from apical four-chamber view were also considered, together with RV end-diastolic area (RVAd) and systolic (RVAs) area and fraction area change (RVFAC).

Definition of two-dimensional cavities and wall measurements. Right ventricle: RVOT1, right ventricular outflow tract from the anterior RV wall to the RV septum in parasternal long-axis view; RVOT3, distance calculated just below the pulmonary valve annulus; RVOT4, maximum distance between the anterior aortic wall and the RV free wall in parasternal short-axis view; RVIT1, right ventricular inflow tract (one-third of the distance below the annulus, parasternal long-axis view); RVIT2, maximum distance between the right side of the mid-interventricular septum to the RV free wall; RVIT3, inflow measurement calculated one-third of the distance below the tricuspid valve annulus. RV long axis (LAX, form the RV apex to the mid-point of the tricuspid annulus) and short axis (SAX, middle third of the RV) from the apical four chamber. Right atrium: RA1, medial-lateral distance; RA2, superior-inferior distance. Left atrium: LA1, medial-lateral distance; LA2, superior-inferior distance (adapted from Foale et al19).
The possible presence of both global and localised kinetic alterations (akinesia and dyskinesia) was carefully investigated, with particular regard to RV anterior wall, apex and subtricuspid region.
Abnormalities in structure, as a thickened and/or highly reflective moderator band, were carefully analysed. The septomarginal trabecula (moderator band) was defined as “thickened” when it was ≥5 mm and as “highly reflective” if there was a persistence of echogenicity at the time that the RV wall disappeared after the echocardiographic gain had been reduced for at least 50% of baseline level. Left and right atrial dimensions (LA1, LA2, RA1, RA2) were measured from apical four-chamber view, at the end of the ventricular systole (fig 1).
M-mode echocardiography was used for the measurement of LV end-diastolic and end-systolic dimensions (left ventricular end-diastolic diameter and left ventricular end-systolic diameter), interventricular septum and the posterior wall. Measures were obtained basing on the standards of the American Society of Echocardiography.20
Statistical analysis
Statistical analysis was performed using STATISTICA V.5.1 (StatSoft, Tulsa, Oklahoma, USA). Categorical variables were compared using a χ2 test or Fisher exact test. Continuous variables were compared by analysis of variance. Data were expressed as mean (SD). A p value <0.05 was considered significant.
Results
Twelve-lead ECG
Basal ECG was abnormal in 25 (62%) ARVC patients (vs 7.5% of athletes and 2.5% of controls, p<0.0001), with presence of negative T wave in the precordial leads ≥V2 in 18 (45%), incomplete right bundle branch block in 7 (17%), low QRS voltages in 2 (5%), whereas no subject showed ST segment elevation. Moreover, in this group. the Sokolow voltage criteria was 18.9 (8.3) mV. Among athletes, ECG was altered in 3 (7.5%) patients who showed incomplete right bundle branch block (QRS duration<120 ms); in addition, 16 (40%) subjects presented Sokolow voltage criteria for LVH, with the mean value of 33.5 (8.3) mV (ARVC patients vs athletes; p<0.0001). One (2.5%) out 40 control subjects had an incomplete right bundle branch block; the Sokolow voltage criteria was 23.8 (5.3) mV (ARVC patients vs controls; p<0.01; athletes vs controls; p=0.0001). Moreover, no subjects presented an epsilon wave.
Ventricular arrhythmias
They were present in 28 (70%) ARVC patients and consisted in sustained VT in 7 (17.5%), non-sustained VT in 3 (7.5%), repetitive with couplets and triplets in 5 and frequent PVBs (>30/h) in 12 (30%). Moreover, one patient had a cardiac arrest with ventricular fibrillation interrupted with direct current shock. In addition, isolated premature ventricular beats <1000/24 h were found in two athletes (5%, ARVC patients vs athletes; p<0.0001) and in 3 (7.5%) controls.
Signal-averaged ECG
Late potentials were present in 22 (55%) ARVC patients (table 2); among these, in 4 (18%) patients, they were present at 25, 40, 80 Hz, in 14 (63%) at 40–80 Hz and in 4 (18%) at 80 Hz (fig 2B). Moreover, late potentials were found at 40–80 Hz in two athletes (5%, ARVC patients vs athletes; p<0.0001) and in three (7.5%) controls.

Non-invasive evaluation of a 25-year-old woman affected with ARVC, diagnosed during familial screening. (A) 12-lead ECG: low QRS voltages, RV conduction delay, negative T wave in V1–5. (B) SAECG showing the presence of late potentials at 24–40 Hz. (C) Apical four-chamber view, showing a moderate dilation of RV cavity, a thickened moderator band and akinesia of anterior wall.
Signal-averaged ECG data on patients affected by arrhythmogenic right ventricular cardiomyopathy (AVRC) patients, athletes and untrained control subjects
Echocardiography
LV measurements
The interventricular septum and the posterior wall were significantly thicker in the athletes group compared with ARVC and normal subjects (table 3). The LV end-diastolic cavity size, quantified with LVEDV and end-diastolic diameter, was significantly larger in the athletes group when compared with ARVC patients and controls. Seven (17%) patients with ARVC showed also LV kinetic alterations that were never present in any subject belonging to the other groups.
Two-dimensional and M-mode echocardiographic left atrial and left ventricular dimensions on ARVC patients, athletes and untrained control subjects
RV measurements
Both athletes and ARVC patients presented a RV enlargement compared with controls. However, RV cavity size, evaluated with area and volumes and RVIT dimensions, was not significantly larger in ARVC group than in athletes (table 4). In addition, the LVEDV to RVEDV ratio did not differ between athletes and controls, whereas this value was found to be smaller in ARVC patients compared with the other two groups. As far as RVOT diameters, RVOT1 and RVOT4 were found to be significantly larger in ARVC patients compared with athletes, whereas these parameters did not differ between athletes and controls. None of the ARVC patients had global kinetic abnormalities, whereas all presented RV localised kinetic alterations: 10 (25%) in the anterior wall, 28 (70%) in the apex and 30 (75%) in the subtricuspid region; these abnormalities were never detected in athletes and controls. The RV function, evaluated both with RVFAC and RVEF, was significantly depressed in ARVC patients compared with athletes.
Two-dimensional and M-mode echocardiographic right atrial and right ventricular dimensions on ARVC patients, athletes and untrained control subjects
Evaluation of structural abnormalities demonstrated that a thickened or hypereflective moderator band was significantly present in ARVC patients compared with controls (20% vs 10%; p=0.03), whereas no differences were found between ARVC and athletes (20% vs 17%; p=NS) and between athletes and controls (17% vs 10%, p=NS) (figs 2C and 3).

{kind=link}
{kind=link}
{kind=link}
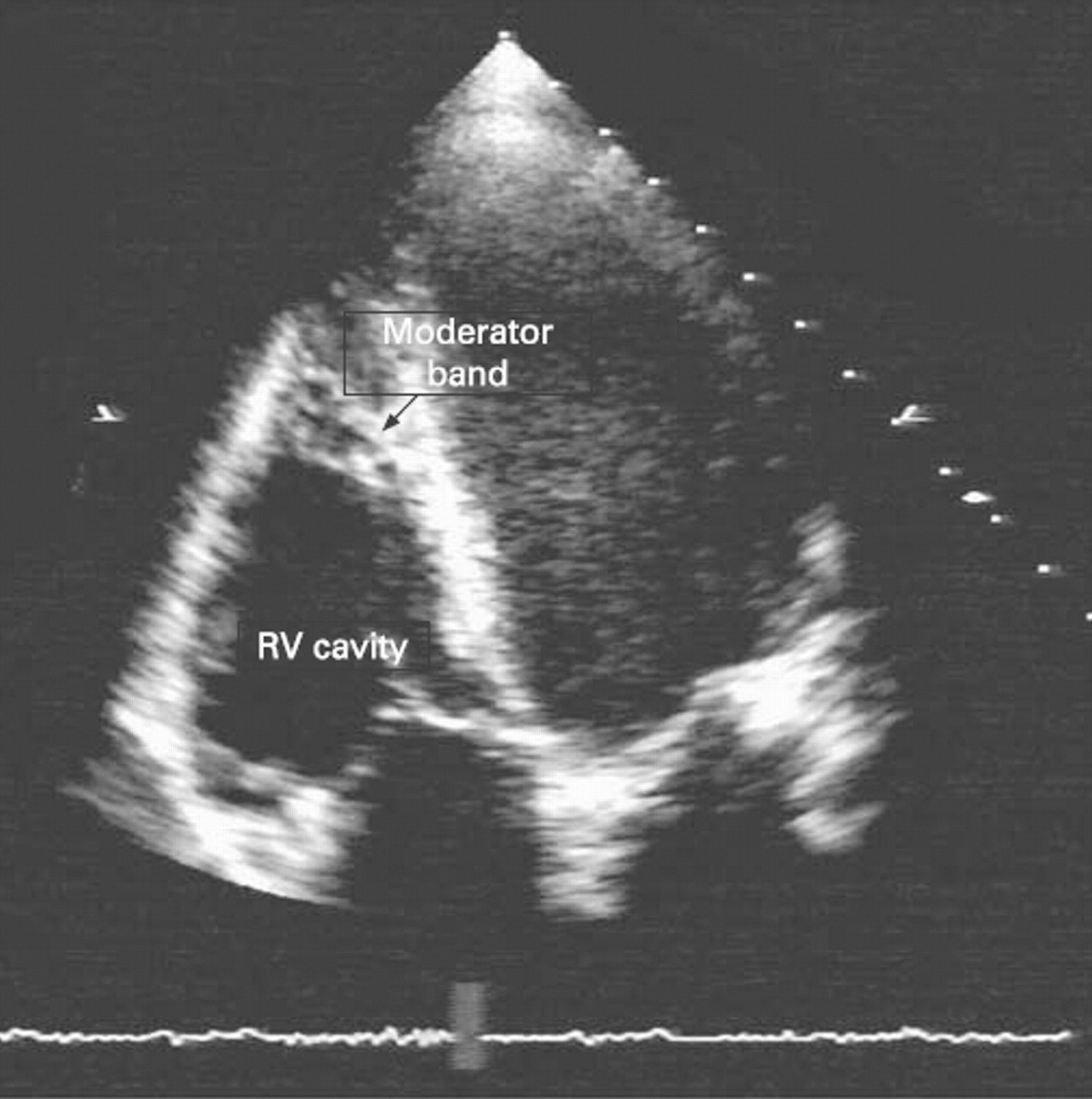
Two-dimensional echocardiogram (apical four-chamber view) of a 22-year-old control subject who showed a thickened moderator band, with normal ECG and negative SAECG.
Atrial measurements
Left atrial diameters did not differ significantly in the three groups, whereas ARVC patients and athletes showed a dilation of the right atrium.
Discussion
The need to differentiate cardiac morphological changes induced by physical activity from those due to a structural RV disease is quite common in the clinical practice when dealing with young subjects practising sport. The differential diagnosis becomes mandatory in athletes showing ventricular arrhythmias with left bundle branch block morphology, mild RV abnormalities on echocardiography, those with a family history of ARVC or 12-lead ECG abnormalities that can be present in patients affected by the disease, as RV conduction delay or negative T waves in the precordial leads.
In our study, we examined a series of patients fulfilling the diagnostic criteria of ARVC, and we found several distinctive features when comparing them with a group of highly trained athletes. Moreover, these differences involved distinct instrumental tests. It is noteworthy that athletes rarely presented typical ARVC features at basal 12-lead ECG, whereas the main ECG differences between ARVC patients and athletes consisted of the QRS duration, which was augmented in ARVC in keeping with the high incidence of conduction delay, negative T wave beyond V2 and low QRS voltages that were hardly present in athletes.
On the other hand, it is important to underlie that in our series, about 38% of ARVC patients had a normal ECG because of the lack of severe forms of the disease. Thus, in more than one third of cases, the ECG had no role in the differential diagnosis, with the exception of QRS voltages that were higher in athletes. The different ECG features that are present in athletes and ARVC patients can be explained by the different physiopathology characterising the two conditions: the myocardial hypertrophy that occurs in athletes’ heart and the progressive myocardial atrophy that appears in ARVC and causes a reduction of the electrical signal.
Moreover, the different electrical activation in the two conditions is confirmed by SAECG results that showed late potentials in 65% of the ARVC patients compared with 5% of the athletes and 7.5% of the controls. In addition, all explored SAECG parameters resulted to be significantly different between normal and athlete groups and ARVC group.
As far as ventricular arrhythmias, they were found in 70% of the ARVC patients, in 5% of the athletes and in 7.5% of the controls; this prevalence is similar to the one found by Biffi et al21AU: Biffi et al is reference 22 (originally 23). Please correct the reference to either Pelliccia et al21 or Biffi et al22, in which case, please provide a citation for reference 21. in a large series of athletes. These data confirm that ventricular arrhythmias are present in a limited number of athletes that have to be carefully investigated.
Considering cardiac morphological features, a RV dilation was found both in athletes and in ARVC subjects, without a significant difference between the two groups; on the contrary, none of the athletes and controls showed kinetic alterations that were present in all affected patients and could explain the lower RV function. Moreover, none of ARVC patients showed global kinetic abnormalities, and this is probably related to the lack of patients with severe forms of the disease, in whom the problem of differential diagnosis with the athletes’ heart usually does not exist. An interesting finding was the ratio between LV and RV end-diastolic volumes, which was similar in athletes and controls, whereas it was significantly smaller in the ARVC group. Echocardiographic studies confirm previous data showing that athletes have increased LV wall thickness and enlarged LV end-diastolic dimensions compared with controls,1,–,7 whereas no differences exist between ARVC subjects and controls. The presence of normal LV dimensions in ARVC patients can be explained with the lack of severe forms of ARVC in our series. Thus, training in athletes induces a biventricular dilation with a maintained ratio between the two chambers, confirming previous studies on heart morphological adaptations in sportsman, evaluated also with cardiac magnetic resonance.11
As far as RVOT diameter is concerned, we found a significant difference between athletes and ARVC subjects, and this could signify that the RV dilation induced by effort prevalently involves the RV main body compared with the RVOT. Thus, evaluation of RVOT diameter in different views (RVOT1–RVOT4) could be important for the diagnosis.14 22
An additional aspect to be considered is the presence of a thickened and/or high reflective moderator band that is commonly considered one of the typical ARVC features. Nonetheless, this aspect was found to be present in a similar percentage in ARVC patients and athletes (20% vs 17%). The presence of similar percentages in athletes and ARVC patients could be explained considering this aspect of the moderator band to be linked to RV dilation, which is present both in athletes and in affected subjects and results in a stretching of the band. As a consequence, it is quite likely that the presence of a thickened moderator band should not be considered a “typical” sign of the disease.
The need to differentiate RV adaptation that is present in athletes from the one that can be found in ARVC patients becomes quite important in the evaluation of subjects involved in competitive sports who belong to ARVC families or who have a family history of juvenile sudden death.
Moreover, the situation becomes still more complicated if we consider that ARVC is a progressive disease that can abruptly progress from a concealed to an overt clinical phase. Thus, in this peculiar group of subjects, the genetic diagnosis, when available, could allow to exclude a priori the presence of an ARVC form. Moreover, it is quite likely that in the future, the recent genetic discoveries in ARVC will provide additional data in differentiating the two conditions.
In conclusion, our data suggest that the athlete’s heart can be differentiated from ARVC through an accurate clinical and instrumental non-invasive evaluation—including 12-lead ECG, SAECG and echocardiography as imaging techniques, if performed with an accurate protocol. ECG findings suggestive of ARVC include the presence of a negative T wave beyond V1 in the precordial leads, incomplete RBBB and low QRS voltage. Both athletes and ARVC patients demonstrate RV enlargement compared with controls; however, RV cavity size is not significantly larger in ARVC patients than in athletes, whereas RVOT diameter is significantly larger in ARVC subjects compared with athletes. Furthermore, all ARVC patients show localised RV kinetic alterations, an abnormality not detected in athletes and controls.
What is already known on this topic
Regular intensive physical activity is associated with non-pathological changes in cardiac morphology, referred to as “athlete’s heart”. Nonetheless, in the athletic population, the presence of right ventricular and atrial adaptations, in particular dilatation, is described and has to be considered in the differential diagnosis with AVRC, which is an important cause of juvenile sudden death.
What this study adds
Our data suggest that athlete’s heart can be differentiated from AVRC through an accurate clinical and instrumental non-invasive evaluation including ECG, signal-averaged ECG and echocardiography, performed with an accurate protocol. ECG findings suggestive of ARVC include the presence of a negative T wave beyond V1 in the precordial leads, incomplete RBBB and low QRS voltage. Both athletes and ARVC patients demonstrate RV enlargement compared with controls; however, RV cavity size is not significantly larger in ARVC patients than in athletes. On the contrary, RV outflow tract is significantly larger in ARVC subjects compared with athletes. Furthermore, all ARVC patients show localised RV kinetic alterations, an abnormality not detected in athletes and controls.
References
Footnotes
-
Funding This study was supported by Telethon (Rome, Italy), Veneto Region (Venice, Italy), MURST (Rome, Italy) and Fondazione Cassa di Risparmio (Padova e Rovigo, Italy).
-
Competing interests None.