Article Text

Abstract
Rehabilitation of the patient with glenohumeral impingement requires a complete understanding of the structures involved and the underlying mechanism creating the impingement response. A detailed clinical examination and comprehensive treatment programme including specific interventions to address pain, scapular dysfunction and rotator cuff weakness are recommended. The inclusion of objective testing to quantify range of motion and both muscular strength and balance in addition to the manual orthopaedic clinical tests allows clinicians to design evidencebased rehabilitation programmes as well as measure progression and patient improvement.
Statistics from Altmetric.com
Rehabilitation of the athlete with shoulder impingement is a complex process that requires a comprehensive evaluation and multifactorial treatment programme. The purpose of this article is to present an evidence-based review of the key treatment strategies to rehabilitate and restore shoulder function of the athlete with rotator cuff impingement.
Types of shoulder impingement
Significant advancement in the basic science research in the areas of anatomy and biomechanics of the human shoulder has led to the identification of multiple types of impingement, as well as other causes of rotator cuff pathology, including instability and intrinsic tendon overload. This greater understanding of the cause or causes of impingement can lead to a more specific and non-generalised treatment approach to treat this disorder.
Primary impingement
Primary compressive disease or impingement is a direct result of compression of the rotator cuff tendons between the humeral head and the overlying anterior third of the acromion, coracoacromial ligament, coracoid or acromial clavicular joint.1 2 The physiological space between the inferior acromion and the superior surface of the rotator cuff tendons has been measured using anteroposterior radiographs and found to be 7–13 mm in patients with shoulder pain3 and 6–14 mm in normal shoulders.4
Neer1 2 has outlined three stages of primary impingement as it relates to rotator cuff pathology. These have been extensively reported and referred to in both the surgical and rehabilitative literature, and give the clinician a progressive understanding of the role compressive disease plays in mechanical loading of the rotator cuff. For the sake of space limitations, additional discussion of these three stages will not be undertaken, however, the reader is referred elsewhere for a complete discussion of these stages.1 2
Secondary impingement
In addition to impingement playing a primary role, impingement or compressive symptoms may be secondary to underlying instability of the glenohumeral joint.5,–,7 Attenuation of the static stabilisers of the glenohumeral joint, such as the capsular ligaments and labrum, from the excessive demands incurred in throwing or overhead activities can lead to anterior instability of the glenohumeral joint. Due to the increased humeral head translation, the biceps tendon and rotator cuff can become impinged secondary to the ensuing instability.5 Also, a progressive loss of glenohumeral joint stability may be created when the dynamic stabilising functions of the rotator cuff are diminished from fatigue, intrinsic overload and subsequent tendon injury.5 In addition, rotator cuff impingement can occur secondary to scapular dysfunction. The effects of secondary impingement can lead to rotator cuff tears as the instability and impingement continue.5
Internal impingement
One additional aetiology for rotator impingement in the young athletic shoulder is termed internal, or undersurface, impingement.6 7 This phenomenon was originally identified by Walch et al6 during shoulder arthroscopy with the shoulder placed in the 90/90 position. Placement of the shoulder in a position of 90° of abduction and 90° of external rotation causes the supraspinatus and infraspinatus tendons to rotate posteriorly. This more posterior orientation of the tendons aligns them such that the undersurface of the tendons rub on the posterior-superior glenoid lip, and become pinched or compressed between the humeral head and the posterosuperior glenoid rim.6 Individuals presenting with posterior shoulder pain brought on by positioning of the arm in 90° of abduction and 90° or more of external rotation, typically from overhead positions in sport or industrial situations, may be considered as potential candidates for undersurface impingement.
Identification of underlying joint mobility status
A systematic approach to shoulder and upper extremity evaluation must be undertaken to identify the specific cause or subtle underlying causes of rotator cuff pathology and/or impingement. Special tests to evaluate the underlying mobility status of the glenohumeral joint are key aspects of the evaluation of the patient with rotator cuff pathology. These special tests include the multidirectional instability sulcus sign,8 anterior posterior humeral head translation tests or drawer tests,9 subluxation relocation test10 and Beighton hypermobility index.11 These tests can be used to identify glenohumeral joint hypermobility and the presence of subtle underlying instability of the shoulder. These important tests can provide key insights into one of the potential causes of the rotator cuff injury and guide the clinician in the development of an evaluation-based treatment programme. For example, a positive sulcus sign, increased humeral head translation with anterior posterior testing and a positive Beighton hypermobility index would indicate the presence of underlying instability as a contributing factor to a patients' symptoms. A positive subluxation/relocation test indicates both the presence of subtle anterior instability as well as internal undersurface impingement of the rotator cuff.10 12
The use of glenohumeral joint accessory mobilisation, often a mainstay in the treatment of patients with shoulder pathology, would not be indicated in the patient with these positive instability signs.13 14 However, for patients who present with glenohumeral joint hypomobility, often seen in patients with primary impingement, the inclusion of select joint mobilisation to restore normal joint arthrokinematics and address capsular tightness or restriction would be indicated.15 Failure to identify patients with glenohumeral joint hypermobility and underlying instability properly can result in the inappropriate use of capsular stretching and mobilisation techniques that could further jeopardise shoulder stability and decrease the potential success of the rehabilitation programme, particularly in the overhead athlete.
Rotational ROM adaptation
The measurement of glenohumeral joint internal and external rotation range of motion (ROM) is an important part of the evaluation process, and can guide important interventions in the treatment process. The measurement of glenohumeral internal and external rotation should be done with the joint in 90° of abduction in the coronal plane.16,–,18 Care must be taken to stabilise the scapula with the patient in the supine position, so that the patient's body weight helps to minimise scapular motion. It is recommended that additional stabilisation be provided through the use of a posteriorly directed force by the examiner on the anterior aspect of the coracoid and shoulder during internal rotation ROM measurement (figure 1). This limits scapular compensation and provides a more isolated internal rotation measurement. Bilateral comparison of external and internal rotation ROM should be performed.
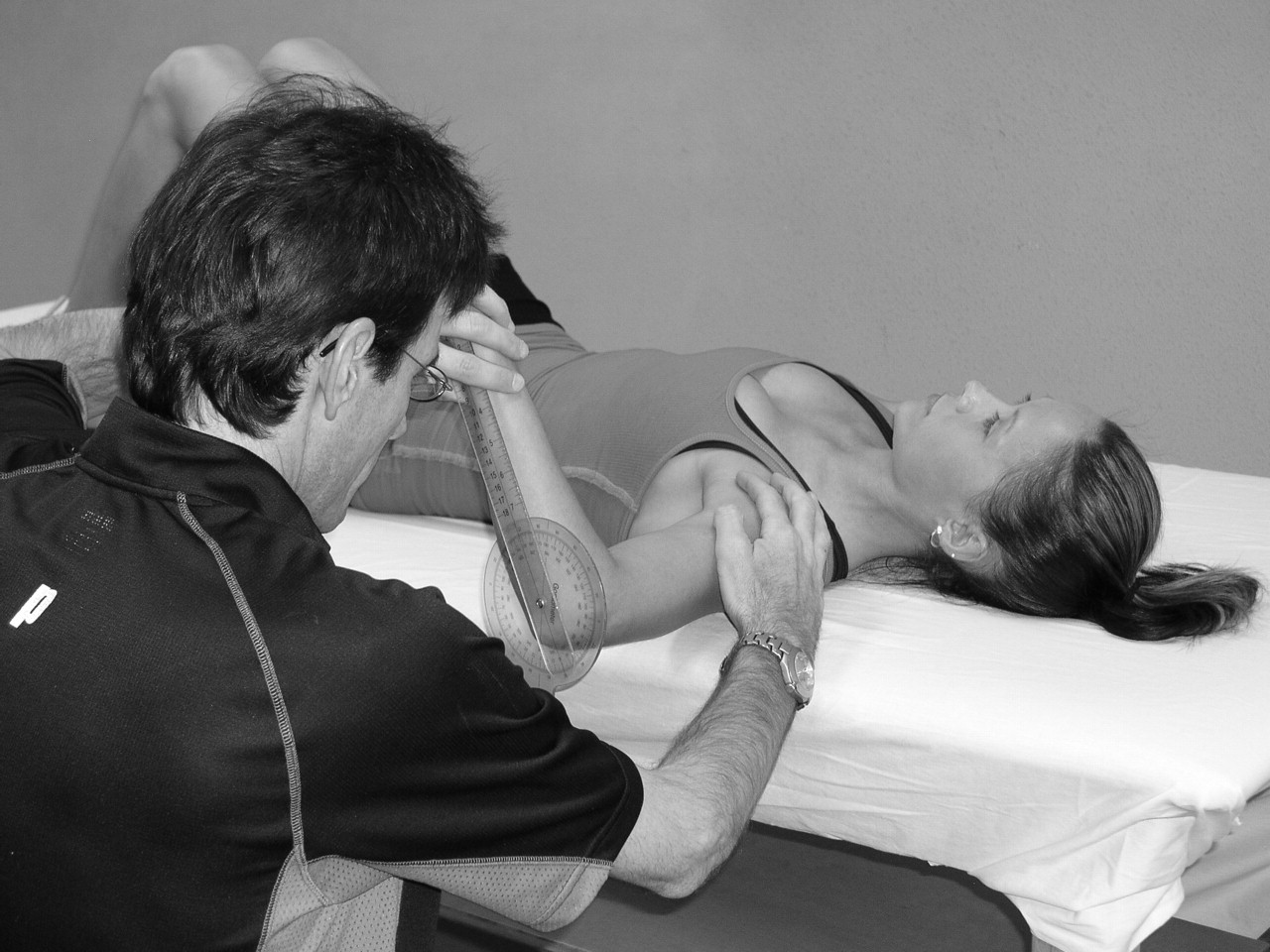
Technique used to measure more isolated glenohumeral joint internal rotation with the shoulder in 90° of abduction in the coronal plane.
One rather consistent finding during the examination of the overhead athlete is increased dominant arm external rotation (defined or referred to as external rotation gain) as well as reduced dominant arm glenohumeral joint internal rotation (glenohumeral internal rotation deficiency, GIRD).18,–,21 Ellenbecker et al have identified that this consistent relationship is only identified in a condition in which glenohumeral joint rotation was measured with the scapula stabilised.22 Failure to stabilise the scapula may not reveal the GIRD present as a result of scapular compensation.
Several mechanisms have been proposed to explain this glenohumeral ROM relationship of increased external rotation (external rotation gain) and limited internal rotation (GIRD).19 23 24 Tightness of the posterior capsule and stiffness of the muscle tendon unit of the posterior rotator cuff (thixotrophy) have both been described as factors that limit internal glenohumeral joint rotation.25 In addition, Crockett et al23 and others26 27 have shown unilateral increases in humeral retroversion in throwing athletes, which would explain the increase in external rotation with accompanying internal rotation loss.
Loss of internalrotation ROM is significant for several reasons. The relationship between internal rotation ROM loss (tightness in the posterior capsule of the shoulder) and increased anterior humeral head translation has been documented.28 29 The increase in anterior humeral shear force reported by Harryman et al30 was manifested by a horizontal adduction cross-body manoeuvre, similar to that incurred during the follow-through of the throwing motion or tennis serve. Tightness of the posterior capsule has also been linked to increased superior migration of the humeral head during shoulder elevation.31
Recent research32 33 that studied the effects of posterior capsular tightness in a functional position of 90° of abduction and 90° or more of external rotation found that imbrication of either the inferior aspect of the posterior capsule or of the entire posterior capsule changed humeral head kinematics. In the presence of posterior capsular tightness, the humeral head shifted in an anterior superior direction, as compared with a normal shoulder with normal capsular relationships. With more extensive amounts of posterior capsular tightness, the humeral head was found to shift posterosuperiorly.
Accurate ROM measurement is crucial because a large spectrum of mobility can be encountered when treating the patient with rotator cuff pathology. Figures 2 and 3 show versions of clinical internal rotation stretching positions both of which utilise the scapular plane and can be performed in multiple and varied positions of glenohumeral abduction. Each inherently possesses an anterior hand placement used to give varying degrees of posterior pressure to minimise scapular compensation and also to provide a check rein against anterior humeral head translation during the internal rotation stretch. These stretches can be used in a proprioceptive neuromuscular facilitation contract-relax format or following a low-load prolonged stretch-type paradigm to facilitate the increase in ROM.34 35 Figures 4 and 5 are examples of home stretches given to patients to address internal rotation ROM deficiency. Note the inherent methods of scapular stabilisation (body weight in the sleeper stretch and wall or firm object in the cross-body stretch) in both methods, which are necessary to optimise the value of the stretching procedure.

Internal rotation stretch using therapist's leg as a stabilising platform to allow both hands to control glenohumeral internal rotation and utilise the scapular plane.

Figure 4 internal rotation stretch. Hand placements allow for containment of humeral translation and scapular compensation.

Sleeper stretch used as a home programme activity for patients with limited internal rotation range of motion.

Cross arm stretch using the wall for additional scapular stabilisation to improve internal rotation range of motion.
Scapular stabilisation
Since the first clinical papers in the literature regarding the role of the scapula in athletic shoulder function and the possible relation to shoulder pain in the overhead athlete,12 36 37 there has been growing interest in scapular kinematics, scapular evaluation and intervention principles and programmes. The association between abnormal scapular positions and motions and glenohumeral joint pathology has been well established in the literature.38,–,45 There is a body of evidence suggesting that patients with impingement symptoms and rotator cuff disease consistently show altered scapular kinematics, which is termed ‘scapular dyskinesis’.
Scapular dyskinesis is generally characterised by a lack of upward rotation, a lack of posterior tilting and increased internal or medial rotation of the scapula.38 39 41,–,44 These changes in scapular kinematics, in the resting position as well as during dynamic arm movements, have been attributed not only to altered recruitment patterns and muscle performance in the scapular stabilising muscles,38 46,–,51 but also to flexibility deficits in the soft tissue surrounding the scapula, possibly restricting normal scapular movement during daily activity and sport-specific movements.12 52,–,55
Several authors have demonstrated altered muscle activity patterns in the scapular muscles in patients with shoulder impingement. These include decreased muscular activity or strength, and changes in the timing properties of the serratus anterior, the lower and middle portions of the trapezius, and increased activity in the upper part of the trapezius.38 46,–,51 Although some of the above-mentioned studies were performed on non-athletic populations,38 43 44 many of the possible causes for scapular dyskinesis have been established in overhead athletes,41 46,–,49 51 and have been suggested to be a contributing and perpetuating factor in the development of impingement symptoms in athletes performing overhead sports.12 56 57
With respect to soft tissue inflexibility, tightness of the pectoralis minor and posterior glenohumeral capsular stiffness have been established in relation to abnormal scapular position. Borstad and Ludewig53 and Borstad54 demonstrated increased scapular internal rotation in subjects with a short pectoralis minor, as well as increased anterior tilting. In a study by Borich et al,52 subjects with posterior shoulder tightness (evaluated by measuring glenohumeral internal rotation ROM) demonstrated greater scapular anterior tilt. However, those studies from both authors were performed on healthy subjects. The association of these flexibility deficits, scapular kinematics and impingement-related shoulder pain should be further explored in overhead athletes with throwing-related shoulder pain. In addition, tightness of other structures possibly altering scapular kinematics and increasing the risk of shoulder impingement, such as the levator scapulae, latissimus dorsi and the rhomboids, have not been quantified in the overhead athlete, but could possibly contribute to motion restriction of the scapula and throwing-related secondary impingement, based on scapular dyskinesis.
In the therapist's decision-making and clinical reasoning process, a thorough clinical examination should precede the choice of treatment goals and appropriate techniques and exercises. In particular, evaluation of scapular dyskinesis should be performed using reliable and valid observation techniques and additional scapular tests. McClure et al58 and Tate et al59 proposed a clinical examination protocol to evaluate scapular dysfunction, easily applicable by the clinician. In addition, scapular tests were developed and validated. The scapular assistance test42 57 58 60 and the scapular retraction/ reposition test61 62 may help the clinician in defining the degree of scapular involvement in the actual shoulder complaints. Kibler et al63 defined three types of scapular dyskinesis, based on the rotational position of the scapula. Type I is increased anterior tilting, type II is increased internal rotation and type III is increased downward rotation. This method of visual observation of scapular evaluation resulted in moderate reliability and validity. A modification of this observational method combining all three types into a ‘yes’ (dyskinesis present)/‘no’ (none of the types seen) method resulted in higher sensitivity and positive predictive value.64 From those studies, we believe that qualitative analysis of scapular malpositioning and classification into subtypes based on observation is relevant from a clinical point of view, helping the therapist in choosing the appropriate treatment goals, based on the particular position and movement disorder. Therefore, we suggest the use of these subtypes in a clinical setting; however, the classification system may have greater limitations in a research setting.
Figure 6 summarises a clinical reasoning algorithm the clinician may use in the treatment of scapular dyskinesis. Flexibility deficits need to be addressed by stretching and mobilisation techniques, whereas muscle recruitment normalisation is the main goal for the patient who has muscle performance problems.

Treatment algorithm for scapular dysfunction.
Several stretches have been described to increase pectoralis minor length.65,–,67 Borstad and Ludewig67 showed superior effects of the ‘unilateral corner stretch’ (performing passive horizontal abduction with the shoulder in 90° of abduction and external rotation) over ‘sitting manual stretching’ (in which the therapist performs scapular retraction with the shoulder in a neutral position) and ‘supine manual stretch’ (similar to the unilateral corner stretch, but performed by the therapist with the patient in a supine position). However, in our opinion, these stretches (with the exception of the ‘sitting manual stretching’) put the athlete's shoulder into a position, possibly causing pain in the case of subacromial or internal impingement.56 68 69 In addition, it was found in a cadaveric study that performing retraction in a 30° forward flexion position results in the largest changes in pectoralis minor length.66 Therefore, we suggest performing passive retraction and posterior tilting of the scapula with the shoulder in a neutral elevation position and slight external rotation (figure 7).

Cools scapular exercise.
In view of the new insights and research findings on the role of the scapula in shoulder pathology, current exercise protocols emphasise the importance of scapular muscle training as an essential component of shoulder rehabilitation..56 70 In the early stage of scapular training, conscious muscle control of the scapular muscles may be necessary to improve proprioception and to normalise the scapular resting position. In order to activate the lower trapezius selectively, the ‘scapular orientation exercise’ has been described.37 71 This exercise is described as scapular setting in a variety of postures initially with the arm at the side placing the scapula in a mid-range position of upward/downward rotation, internal/external rotation and anterior posterior tilting.37 71 The authors demonstrated in their study71 that it is possible to teach a normal individual consistently to reproduce movements of the scapula into posterior tilt and upward rotation. In addition, this exercise resulted in a significant increase in scapular muscle activity, and a high correlation between assisted and unassisted exercise was established, indicating that an individual is able to perform this exercise in a home programme. Other researchers72,–,74 focused on the use of electromyographic feedback for learning selective activation of the serratus anterior74 and the effect of motor control and movement training on upper limb motor strategies and shoulder function.72 73 Roy and colleagues72 73 showed that conscious movement training with feedback causes immediate, but temporary, effects on motor strategies and upper limb kinematics.73 They also showed that patients with impingement benefit from a 4-week motor control training programme to reduce pain and improve function.72 In summary, there is some preliminary evidence to support the use of conscious muscle control exercises to restore the force-couple activation in the scapular muscles, with special attention to activation of the lower trapezius and serratus anterior.
Depending on the results of the clinical examination, the therapist may decide in the second stage of scapular muscle training to focus more on muscle control (appropriate co-activation of the scapular force couples) or muscle strength (in case, for instance, manual muscle testing or isokinetic testing shows isolated strength deficit in one or more scapular muscles).
Following the scapular orientation exercises, scapular cocontraction may be exercised in basic positions, movements and exercises. Kibler and colleagues75 76 described specific exercises for scapular control in the early phases of shoulder rehabilitation. The ‘low row’, ‘inferior glide’, ‘lawnmower’ and ‘robbery’ exercises, as described in their paper,75 activate the key scapular-stabilising muscles without putting high demands on the shoulder joint, making these exercises appropriate to use in the early stages of non-operative as well as in postoperative rehabilitation. In addition to these basic exercises, the athlete may gradually perform functional diagonals into internal and external rotation with increasing intensity and load and accurate scapular muscle control, in preparation of the third stage of scapular muscle rehabilitation.
For patients with a strength deficit and muscle imbalance in the scapular muscles, selective activation of the weaker muscle parts with minimal activity of the hyperactive muscles is an important component in the second stage of scapular muscle rehabilitation. Because of the observed lack of activity in the lower trapezius and serratus anterior,38 48 often combined with excessive use of upper trapezius38 47 48 exercises with low upper trapezius/lower trapezius, upper trapezius/middle trapezius and uppper trapezius/serratus anterior ratios are of particular importance. Several studies have been performed identifying exercises that meet this standard of favourable inter and intramuscular activation balance, in open as well as in closed kinetic chain,77,–,84 and several clinical papers extensively describe these exercises.56 85 In a recent study by De Mey et al,78 it was demonstrated that exercises with optimal upper trapezius/middle trapezius and upper trapezius/lower trapezius ratios in terms of activity level77 also guarantee early activation of the lower trapezius and inhibition of the latency of the upper trapezius. Another way to increase muscle activity in the weaker muscles is by integrating kinetic chain components into the exercise. Maenhout et al83 investigated the influence of lower extremity position on muscle activity and balance during push-up variations, and revealed increased activity in the serratus anterior if the ipsilateral leg was extended, whereas extension of the contralateral leg improved lower trapezius activity. Also, in open chain low rowing exercises, unilateral stance on the contralateral leg increased scapular muscle activity and improved the upper trapezius/lower trapezius ratio, whereas sitting positions and bilateral stance seem not to be favourable for optimal scapular muscle balance (De Mey et al, unpublished data).
Once muscle balance is restored, in the third stage of scapular muscle rehabilitation, general scapular strengthening exercises may be used to increase muscle strength. Numerous studies propose optimal strengthening exercises for the scapular muscles,80 85,–,88 and a detailed description of these exercises goes beyond the scope of this paper. In this last stage of scapular rehabilitation, in which the treatment goal is to exercise advanced scapular muscle control and strength during sportspecific movements, special attention is given to integration of the kinetic chain into the exercise programme,56 83 89 implementation of sport-specific demands by performing plyometric exercises90 and eccentric exercises.91 92
Rotator cuff strengthening
The use of specific techniques to quantify muscular strength and most importantly muscular balance in the patient with rotator cuff pathology is indicated. Objective studies using instrumented testing of the rotator cuff consistently show both weakness and muscular imbalance of the external and internal rotator muscles on the injured extremity in patients with rotator cuff impingement and glenohumeral joint instability.93 In a detailed study of electromyographic activity of the rotator cuff and deltoid musculature in normal subjects and patients with shoulder impingement, significant decreases in supraspinatus and infraspinatus activity in subjects with impingement were found.94 Several studies have measured the concentric external rotators/internal rotators ratio using isokinetic dynamometry in healthy uninjured subjects and found this ratio to be approximately 60–70%95,–,99 in most positions of testing, including 0° and 90° of abduction in the scapular plane. Therefore, evaluating the relative strength and/or unilateral muscle strength ratio (ie, concentric external rotators/ internal rotators ratio) will help to direct the emphasis in the rehabilitation resistive exercise programme.95
Resistive exercise progression to promote muscular balance
The primary goals of these programmes are to elicit high levels of rotator cuff and scapular muscular activation using movement patterns and positions that do not create significant subacromial contact or undue stress to the static stabilisers of the glenohumeral joint.
Sidelying external rotation and prone shoulder extension with an externally rotated (thumb out) position are typically utilised first, with progression to the prone horizontal abduction and prone external rotation exercises with scapular retraction following a demonstrated tolerance to the initial two exercises. Prone horizontal abduction is used at 90° of abduction to minimise the effects from subacromial contact. Research has shown this position to create high levels of supraspinatus muscular activation100 101 102 103 making it an alternative to the widely used ‘empty can’ exercise, which can often cause impingement due to the combined inherent movements of internal rotation and elevation.105 The empty can exercise is no longer recommended in the rehabilitation of patients with rotator cuff pathology.
In general, three sets of 15–20 repetitions are recommended to create a fatigue response and target the development of local muscular endurance.105 Moncrief et al106 have demonstrated the efficacy of these exercises in a 4-week training paradigm, and measured 8–10% increases in isokinetically measured internal and external rotation strength in healthy subjects. Niederbracht et al107 also reported significant gains in strength of the rotator cuff, specifically targeting external rotation strengthening to normalise external/internal rotation strength balance in a group of female overhead athletes.
These isotonic exercises can be coupled with a standing external rotation exercise with elastic tubing as well as the external rotation oscillation exercise, which uses 30-s sets and elastic resistance to provide a resistance bias to the posterior rotator cuff using an oscillating device (figure 8). All exercises for external rotation strengthening in standing are performed with the addition of a small towel roll placed in the axilla, as pictured. In addition to assisting in the isolation of the exercise and controlling unwanted movements, this position of slight abduction has been shown to elevate muscular activity by 10% in the infraspinatus muscle when compared with identical rotational exercises performed in adduction.102 Other advantages of the use of a towel roll or pillow to place the shoulder in approximately 20–30° of abduction are preventing decreased blood flow in the supraspinatus tendon108 and increasing the subacromial space.109
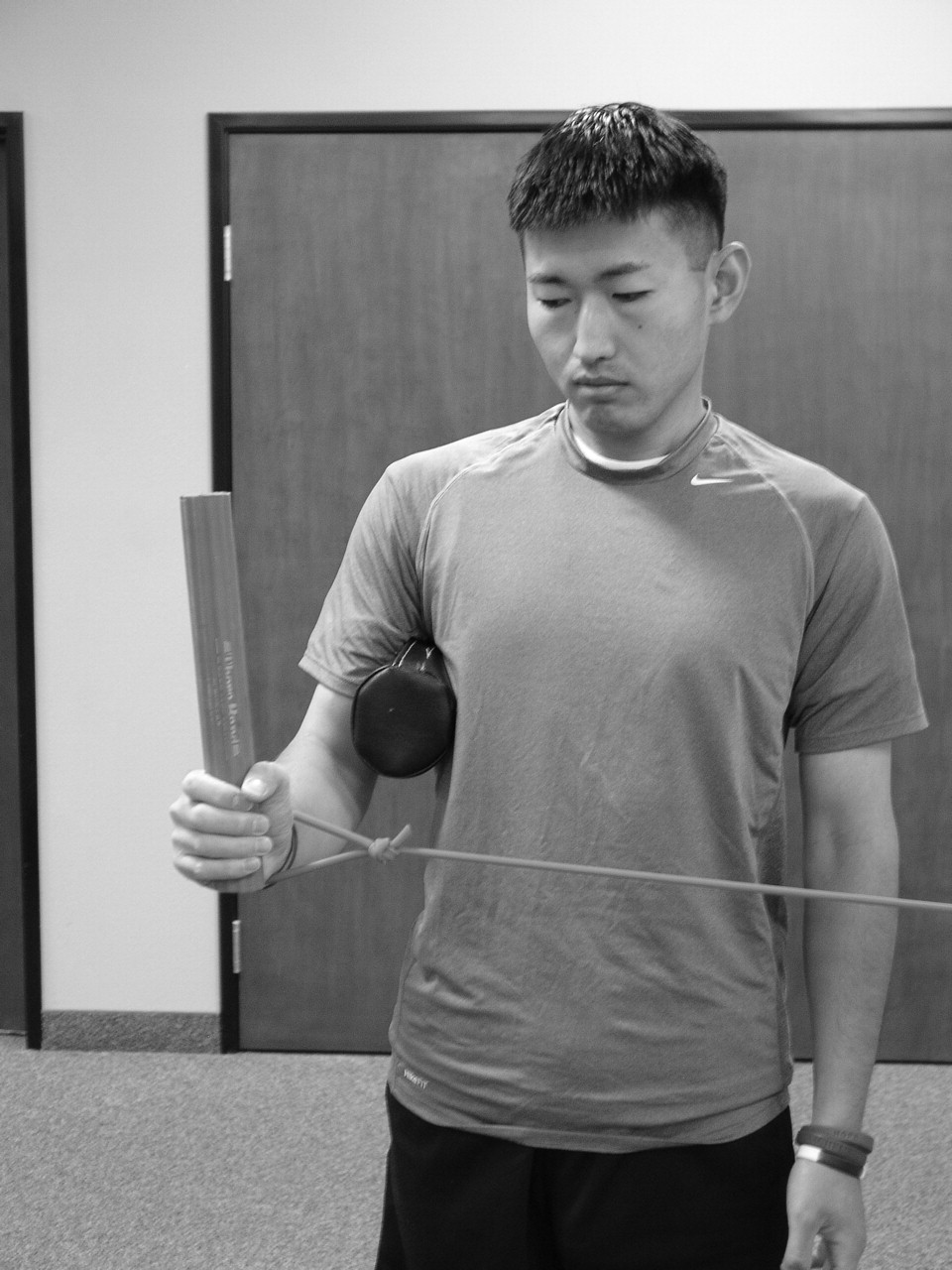
External rotation oscillation.
One of the other key aspects of any resistive exercise programme is exercise load or intensity. Bitter et al110 have reported the inherent advantages of using low-resistance exercise strategies to target the infraspinatus during external rotation exercise. They report specifically on external rotation exercise using a 40% maximal voluntary isometric contraction to be superior to higher loads in preferentially recruiting the infraspinatus muscle over conditions with higher maximal voluntary isometric contraction loading, because increased loading leads to a relative increase in the amount of middle deltoid muscle activation.
Progression to exercises that more appropriately simulate the function of the rotator cuff during overhead activities is warranted upon successful tolerance of the initial rotator cuff exercise programme outlined above.111 Exercises using 90° of glenohumeral joint abduction and the scapular plane serve to apply the specificity principle to middle-stage rehabilitation and prepare the athletic patient for the positions used during a return to both throwing112 and serving based on biomechanical research. In addition to traditional external rotation exercise in the scapular plane elevated position, the use of both oscillation and rhythmic stabilisation or perturbations applied by the clinician can be used to add additional challenges to the exercise and increase the number of repetitions applied in the exercise session (figure 9).

Perturbations applied to the patient's extremity in the 90/90 position using the scapular plane.
Finally, the use of isokinetic exercise, initially in the modified base position, which is characterised by the glenohumeral joint elevated 20–30° in the scapular plane position95 96 and progressing to 90° abducted training, has been shown to increase multiple parameters of muscle function113 114 and also to improve functional performance. Multiple sets of 15–20 repetitions are applied using the isokinetic dynamometer focusing on faster, more functional contractile velocities (speeds) and using load ranges similar to those used during functional activities. Plyometric exercises for the posterior rotator cuff in overhead athletes are also used in the later stages of rehabilitation in the 90/90 position (figure 10). Descriptive reports of electromyographic activity in the rotator cuff and scapular musculature have demonstrated favourable activation of these important muscles using 0.5 and 1 kg medicine balls, with improvements in both concentric and eccentric rotator cuff strength following an 8-week training period of plyometric and elastic-based rotator cuff exercise in baseball players.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prone 90/90 plyometric exercise for posterior rotator cuff and scapular training.
Each of these exercise progressions for the rotator cuff is applied with the goal of improving strength and local muscular endurance. Frequent monitoring of muscular performance with specific emphasis on the muscle balance between the external and internal rotators is recommended and followed to guide the continued evidence-based selection of exercise for the patient undergoing rehabilitation for rotator cuff pathology. Patients ultimately progress towards levels of bilateral symmetry in muscular strength and established muscular strength ratios. The emphasis and relative success of resistive exercise programmes for the rotator cuff and scapular musculature has been outlined in a systematic review of shoulder impingement by Kuhn.115
What is known about this topic
Due to a greater understanding of the anatomy and biomechanics of the shoulder and the impingement process gained through basic science research, clinicians can better understand the key structures involved, and the mechanism by which impingement occurs in the human shoulder.
What this paper adds
This paper provides a summary of key interventions used to treat shoulder impingement. This review details clinical exercises and their inherent objective muscular activity characteristics to guide clinicians in the development of individualised rehabilitation programmes for treatment of the patient with shoulder impingement.
Conclusion
The integration of key physical examination techniques with evidence-driven rehabilitation concepts to restore optimal ROM and rotator cuff and scapular strength and stabilisation forms the basis of clinical rehabilitation of the athlete with rotator cuff impingement. The continued application of basic science research, clinical training and outcomes research will provide additional insight and guidelines for treating impingement in the athletic shoulder.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; not externally peer reviewed.
-
Detail has been removed from these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.