Article Text

Abstract
Objectives To examine the correction of posture, increase in strength and decrease in shoulder pain and dysfunction in varsity swimmers.
Design and Setting Randomised clinical trial.
Participants Twenty-eight National Collegiate Athletic Association division I varsity swimmers.
Measurements Two testing sessions were conducted before and after an 8-week time period. Posture, strength and shoulder pain and function were assessed. Forward head angle was measured using a digital inclinometer, forward head translation was measured using a ruler and total scapular distance was measured with unmarked string. Average and peak values (N) of strength were measured with the hand-held dynamometer. The intervention subjects then participated in an 8-week exercise training programme to correct posture. The procedures were then repeated in the post-test.
Results Significant group by time interactions (p<0.05) were found in forward head angle and forward shoulder translation indicating a decrease in forward head angle and forward shoulder translation. Significant main effects for time (p<0.05) were found in strength measures for all muscle groups indicating increased strength for shoulder girdle muscles tested.
Conclusions The exercise intervention was successful at decreasing forward head and rounded shoulder postures in elite swimmers. This study supports the theoretical basis for clinical rehabilitation of posture and the shoulder.
Statistics from Altmetric.com
Competitive swimmers practise 6–7 days a week and swim on average 12 000 m each day, rotating the shoulder an estimated 16 000 times.1 It is not surprising that competitive swimmers are plagued by varied levels of shoulder pain, which may or may not limit their regular activity.2 One study has shown that 47% of collegiate swimmers claim to experience shoulder pain persisting for 3 weeks or more, causing eventual alteration or cessation of their normal swimming routines.3 This shoulder pain, termed ‘swimmer's shoulder’, encompasses several pathologies including rotator cuff tendinitis, shoulder instability and shoulder impingement.4 Swimmer's shoulder may be the result of several factors such as postural malalignments, altered scapular kinematics and muscular imbalances surrounding the shoulder and scapula.4 As a result of the high frequency of shoulder pain in swimmers, it is important to understand the factors that may contribute to the development of swimmer's shoulder and to develop effective methods to prevent and to rehabilitate the injury.
Head and shoulder postural malalignments are thought to influence the muscular balances surrounding the shoulder. Forward head posture (FHP) is a forward inclination of the head with cervical spine hyperextension and is associated with shortening of the upper trapezius, the splenuis and semispinalis capitis and cervicis, the cervical erector spinae and the levator scapulae musculature.5 This posture may change the position of the scapula and decrease the ability of the scapula to rotate upwardly,5 a common characteristic found in patients with shoulder impingement.6 Research has shown FHP to be significantly greater in individuals with shoulder pain when compared with a healthy population.7 Rounded shoulder posture (RSP) is a forward deviation of the shoulders associated with a protracted position of the scapula as caused by a muscular imbalance between a shortened pectoralis minor and a lengthened middle trapezius.5 RSP also places the lower trapezius and serratus anterior positions, which are thought to influence scapular tilt negatively.8,–,10 This may be important as increased anterior scapular tilt and scapular internal rotation are associated with shoulder impingement.11 12 These altered scapular mechanics are related to shorter pectoralis minor length13 and decreased serratus anterior and lower trapezius activity.11 14
Exercise interventions aimed at strengthening weak musculature and stretching tight, overdeveloped musculature is thought to improve FHP and RSP.15 16 Strengthening of the scapular stabilisers and stretching of the anterior musculature, namely the pectoralis minor, is thought to be the method to treat RSP.17 Treatment of FHP most often centres on stretching the shortened upper trapezius and levator scapula. Few studies have attempted to correct posture through a training protocol involving flexibility and strength exercises.17 18 These studies suggest that FHP and RSP can improve but have not examined whether changes occur in shoulder girdle muscle performance or clinical outcomes. The purpose of this study was to evaluate the effects of 8 weeks of exercise training on FHP and RSP, shoulder girdle strength and clinical outcomes in division I collegiate swimmers. We hypothesised that measures of FHP and RSP, strength and shoulder pain and function would improve following the intervention.
Methods
Subjects
Subjects were 28 division I varsity swimmers from the National Collegiate Athletic Association, with ages ranging from 17 to 23 years. Subjects were assigned to an exercise group (n=14) or control group (n=14) using a blocked randomised approach in which swimmers were matched by event category, sprint or distance. The block randomised design was used in an effort to equalise the possible effects of training volume. Descriptive statistics for each group are listed in table 1.
Means and SD for subject characteristics (age, height, weight)
Subjects were included based on a demonstration of FHP and RSP as evaluated through the use of a plumbline and the Osteoprint body mapping system. Swimmers whose external auditory meatus and lateral acromion were anterior to a vertical line intersecting the lateral malleolus were allowed for inclusion in the study. Swimmers who had performed at least 6 weeks of formal rehabilitation within the past 3 months for shoulder pain or who had previous shoulder surgery were excluded from the study. Swimmers were also excluded if they missed practice for three consecutive days or more due to shoulder pain. Before initial testing, all subjects signed an informed consent form approved by the University of North Carolina Biomedical Institutional Review Board.
Testing procedure
A pilot study of all dependent variables revealed good to excellent intratrial reliability, with ICC(2,1) values from 0.97 to 0.99. Dependent measures demonstrated good to excellent test–retest reliability with ICC(2,k) values from 0.90 to 0.98. A single examiner performed all measurements. The examiner was not blinded to group assignment; however, pretest results were only recorded and not compared until postintervention assessments were completed.
Posture alignment assessment
Posture was assessed using three methods. The cervical angle was used to quantify FHP and was measured using an inclinometer (Saunders Digital Inclinometer; the Saunders Group, Chaska, Minnesota, USA). Standard instructions were given to subjects in an effort to avoid the Hawthorne effect yielding subject's ‘true’ resting posture. Subjects were instructed to ‘touch their toes three times and then stand in their normal, relaxed posture, with their arms at their sides’. The examiner then palpated and marked the seventh cervical vertebrae (C7) and the external occipital protuberance (inion). The inclinometer was placed over that site and the cervical angle was measured. Before testing, the inclinometer was levelled on a stable surface, using a bubble level and zeroed when level. The most common measure of forward head angle (FHA) is from C7 to the tragus (inner ear) as commonly reported in the literature.19,–,23 During pilot testing the inclinometer FHA was compared against this osteoprint FHA for 10 subjects. Whereas the absolute angles were offset on average 4° (inclinometer yielded a less forward head measure), these angles were not statistically different and yielded a high Pearson r value of 0.68 (p=0.02). These results suggest that the FHA measured by the inclinometer is a reasonable, clinically applicable measure of FHA.
RSP was assessed in two ways: the total scapular distance (TSD) and forward shoulder translation (FST).24 25 The spinous process of the third thoracic vertebrae (T3) and the inferior angle of the acromion were marked. Using a piece of unmarked string, the linear distance from the inferior angle of the acromion to the spinous process of the third thoracic vertebrae was defined as the TSD. The examiner defined the linear length from the inferior angle of the acromion to the medial border of the scapula as the length of the scapula. Values were normalised to account for subject size by dividing the TSD by the length of the scapula.
FST was measured using a levelled metric ruler.26 The subject stood in a relaxed position with their heels against a wall. The posterolateral acromion was marked and the ruler was held square. The ruler measured from the acromion to the wall behind the subject to determine the amount of forward displacement. TSD and FST were assessed for both shoulders.
Strength assessment
The isometric strength of the periscapular muscles of both shoulders was measured using a hand-held dynamometer (CDS 300 strength dynamometer; Chatillon, Largo, Florida, USA) and measured in Newtons (N) of force. The instrument was calibrated before each measurement.
Isometric strength testing of the middle trapezius, lower trapezius and serratus anterior was performed as described by Kendall,27 with the serratus anterior tested in supine. For each testing position, subjects performed one submaximal isometric contraction and one maximal contraction in order to familiarise themselves with the test. Subjects then performed three maximal isometric contractions in each testing position. Each test lasted approximately 5 s. Subjects were instructed to ‘Push up as hard as you can against my resistance’. Throughout the duration of the contraction, repeated verbal encouragement of ‘push, push, push’ was given. The average and peak force (N) for each trial were recorded for each muscle tested. There was a 30-s rest period between trials with one test condition and a 1-minute rest interval between test conditions. Strength assessment was counterbalanced in order to control for an order effect.
Self-assessment of shoulder pain and function
The American shoulder and elbow surgeons shoulder assessment (ASES) form was used to record the presence of shoulder pain and function in the subjects. The questionnaire addressed self-evaluation of pain using a visual analogue scale (VAS) and an activities of daily living questionnaire.
The ASES pain subscore was calculated by measuring the VAS, subtracting the patient's mark on the VAS from the maximum score of 10 cm. To convert the pain subscale score, the raw score was multiplied by 5, accounting for 50% of the total score. The function subscore consisted of 10 items, each scored on a three-point Likert scale, with 0 points equalling maximum difficulty. The raw score was multiplied by 5/3 to convert the subscale function score.
The pain and function scores were added and a high point total indicated low perceived pain and a low dysfunction in activities of daily living.
Intervention protocol
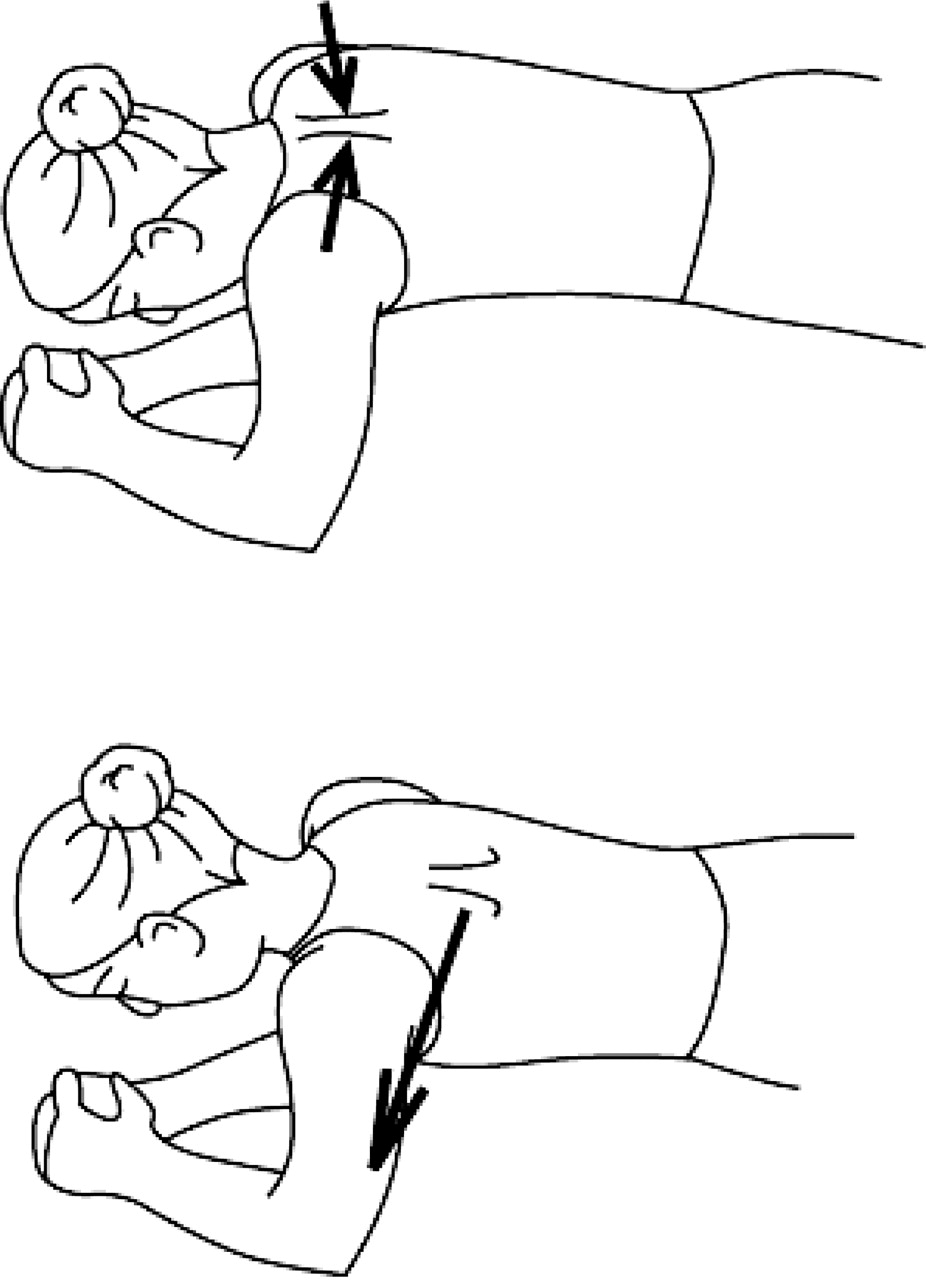
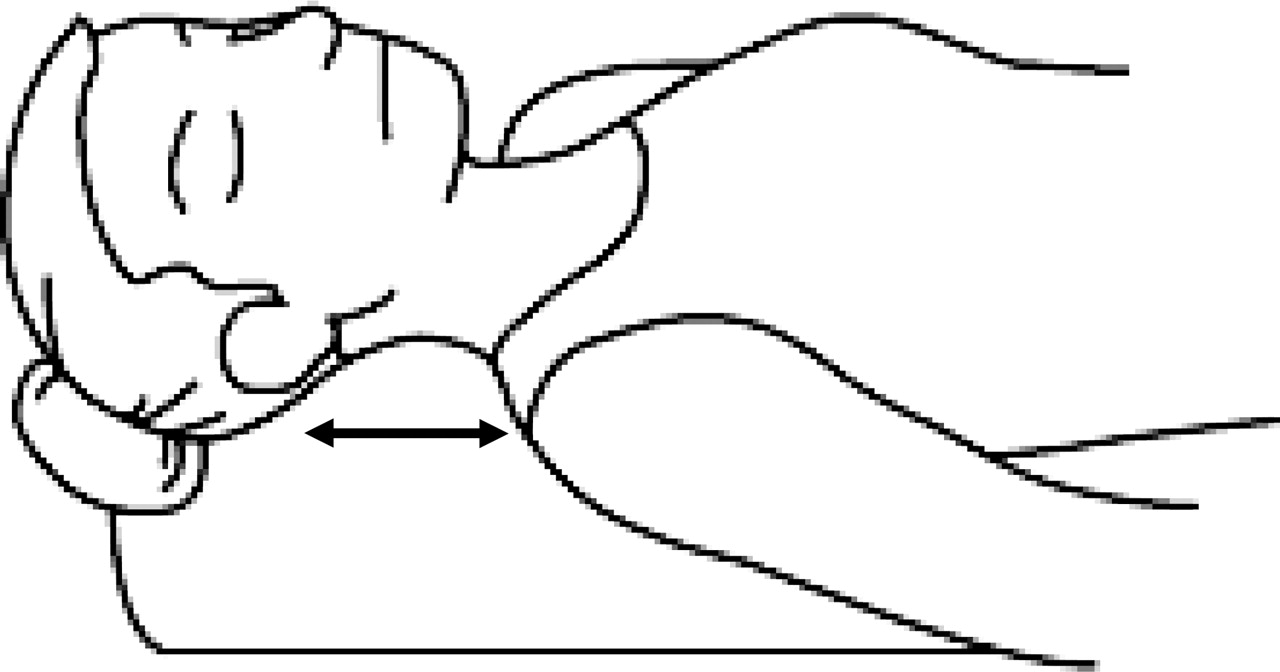
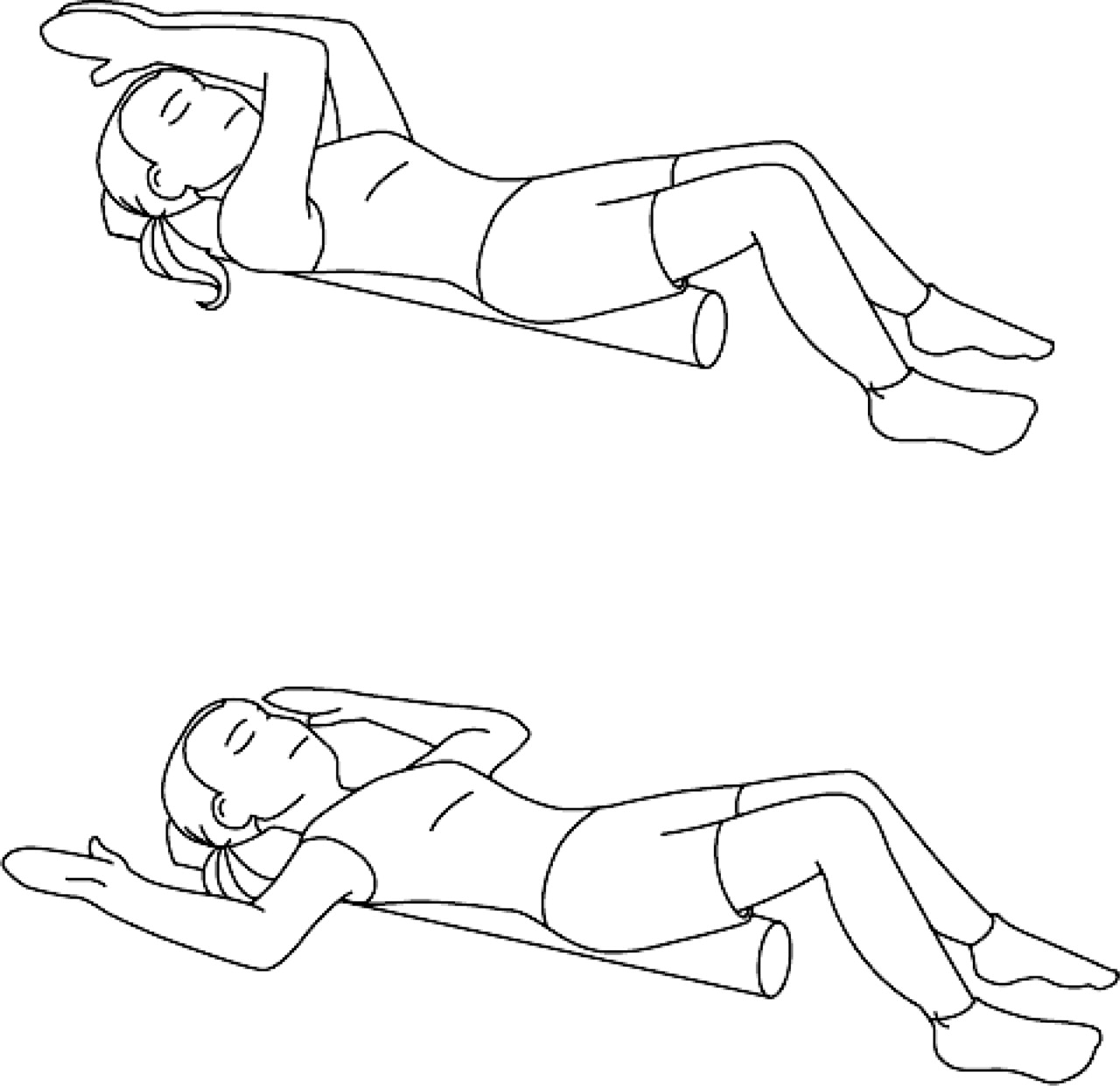
Following the testing protocol, subjects in the intervention group began an 8-week stretching and strengthening programme. Exercises were performed three times a week, scheduled around their regular team practice and strength training sessions. Subjects in the intervention group were trained using an instructional video of the exercises as well as being provided with an illustrated handout. Descriptions of the exercises are shown in tables 2 and 3. Strengthening exercises targeted the periscapular muscles (figures 1–3). Stabilisation of the scapula throughout the exercise routine was emphasised during instruction. Subjects performed three sets of 10 repetitions of all strengthening exercises. The stretching portion of the intervention aimed at increasing the flexibility of the pectoralis muscle group and the cervical neck extensors (figures 4 and 5). Exercises were selected based on literature that suggests selective activation of the lower trapezius/middle trapezius and serratus anterior,9 28,–,31 lengthening of the pectoralis minor32 and improving deep cervical flexor function and improving posture.33,–,35 Subjects logged the number of times the training was performed. Random checks by the investigator were performed to ensure compliance as well as the correct execution of the exercises.

Y to Ws described in table 2.

L to Ws described in table 2.
Scapular protraction described in table 2.
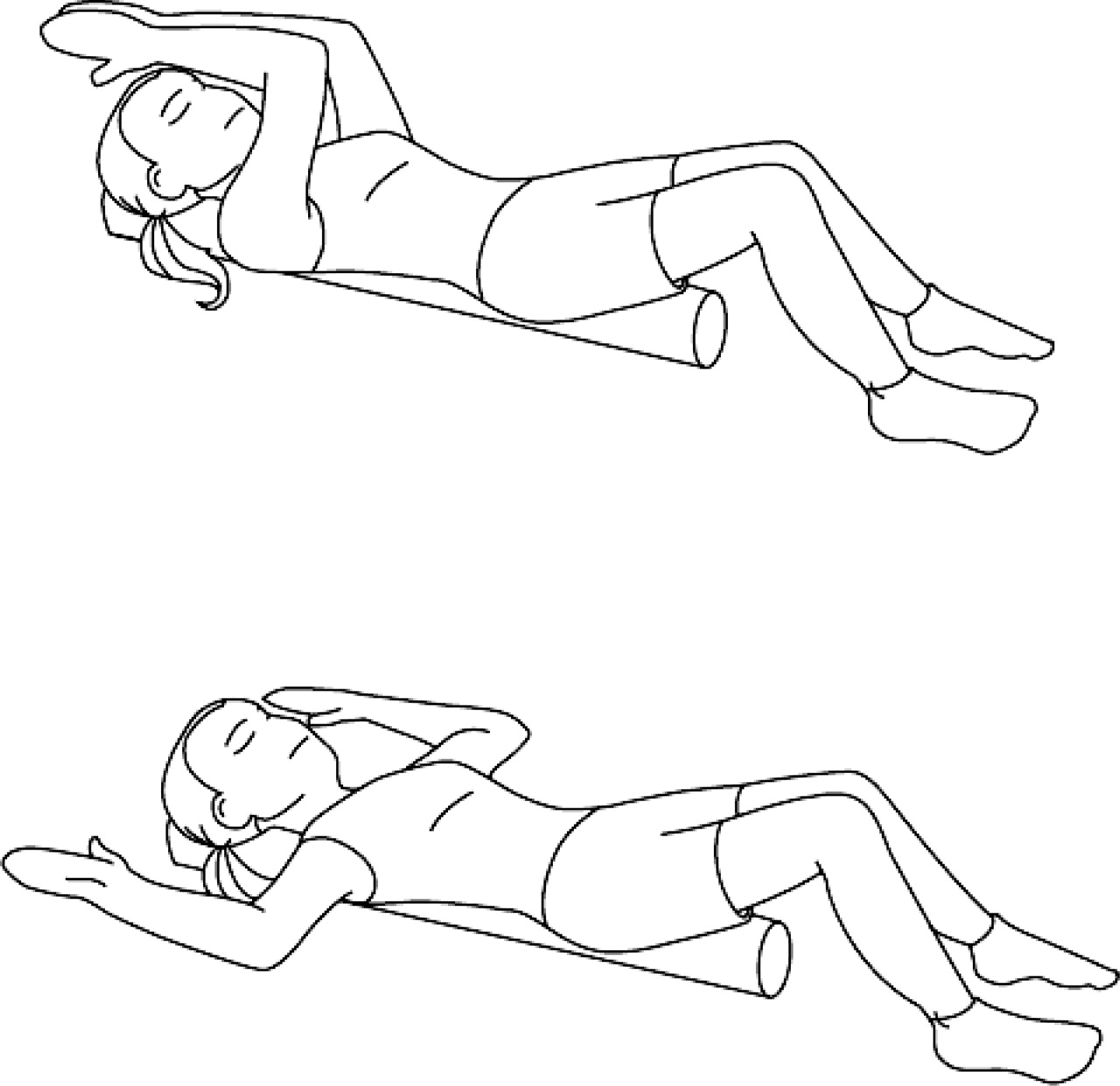
Pectoralis stretch on foam roll described in table 3.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chin tucks described in table 3.
Statistical analysis
A 2×2 (group×time) mixed-model analysis of variance was used to evaluate the within-subjects comparison of pretests and post-tests for both groups as well as to evaluate the between-subjects comparison between groups. An α level of p<0.05 was used for all statistical tests. SPSS statistical software (version 11.0) was used to analyse all data.
Results
Cervical angle, FST and TSD
Descriptive statistics for the postural variables are listed in table 4. Statistical analysis revealed a significant group by time interaction for FHA (F(1,26)=7.51; p=0.005; Cohen's effect size (ES) 1.2). Post-hoc analysis revealed a significant difference within the intervention group from pretest to post-test (minimum significant difference (MSD) 4.17), indicating a decrease in the cervical angle following the intervention. Analysis also revealed a significant difference between the intervention and control groups at post-test (MSD 2.02). The intervention group presented with less cervical angle at post-test compared with the control group at the same time.
Means and SD for FHA, FST and TSD in control and intervention subjects, pretest and post-test
Statistical analysis revealed a significant group by time interaction for FST (F(1,26)=12.89; p=0.001; ES 1.4). Post-hoc analysis revealed a significant difference within the intervention group from pretest to post-test (MSD 1.52), indicating a decrease in FST following the intervention. Analysis also revealed a significant difference between the intervention and control groups at post-test (MSD 1.11). The intervention group presented with a smaller amount of FST at the time of posttest compared with the control group.
Statistical analyses revealed no significant interaction (F(1,26)=0.16; p=0.696; 1–β=0.067; ES 0.15) and no main effects (F(1,26)=2.98; p=0.096; 1–β=0.384; ES 0.68) for TSD.
Middle trapezius, lower trapezius and serratus anterior strength
Descriptive statistics for the strength of the middle and lower trapezius as well as the serratus anterior are listed in table 5. Strength testing was performed on both left and right sides and statistical analysis was performed on each as separate dependent variables. Analysis revealed equivalent statistical outcomes left to right, therefore only analysis of the right side is presented. Analysis revealed no significant group by time interactions for strength in any muscle group. There was a significant main effect of time for mean middle trapezius strength (F(1,26)=9.28; p=0.005; ES 1.19), lower trapezius strength (F(1,26)=22.93; p<0.005; ES 1.88) and serratus anterior strength (F(1,26)=38.30; p<0.005; ES 2.43). There was also a significant main effect of time for peak middle trapezius strength (F(1,26)=9.30; p=0.005; ES 1.2), lower trapezius strength (F(1,26)=21.29; p<0.005; ES 1.81) and serratus anterior strength (F(1,26)=37.43; p<0.005; ES 2.4). The results indicate an increase in strength of each muscle group from pretest to post-test in both the control and intervention groups.
Means and SD of average and peak strength values for control and intervention subjects, pretest and post-test
ASES form
Means and SD for the self-assessment scores for daily function and pain are listed in table 6. Statistical analysis revealed no significant interaction for ASES scores (F(1,26)=0.853; p=0.389; 1–β=0.145; ES 0.34), indicating no significant change in pain and function scores following the intervention. However, the control group demonstrated a trend of average ASES scores, whereas the intervention group was similar from pretest to post-test. Seven out of 14 subjects in the intervention group reported an increase in ASES scores, indicating a decrease in shoulder pain and dysfunction following the intervention. In addition, a total of 11 out of 14 subjects in the intervention group reported either decreases or no change in their pain. In contrast, 10 of 14 subjects in the control group displayed a decrease in their ASES score and nine out of 14 displayed an increase in their pain at post-test compared with pretest.
Shoulder pain and function scores derived from the ASES form for swimmers and non-swimmers
Discussion
Swimmers can be plagued by shoulder pain and dysfunction attributed to several factors including strength imbalances and posture. This study examined the role of posture and the effects of an 8-week exercise intervention in changing posture, scapular muscle strength and shoulder pain and function. Our results indicate that the intervention significantly decreased cervical angle and FST, suggesting that the exercises targeted tissues that contribute to improved posture. However, we did not observe between-group differences for TSD and scapular muscle strength following the intervention.
The flexibility exercises were chosen based on theories that FHP and RSP are caused by tightness in the levator scapulae, the sternocleidomastoid and the pectoralis muscle group, and could be corrected through active stretching of the musculature. Few studies have investigated an intervention specific to the correction of FHP, although it has been indicated as an important factor in the development of several pathologies including craniomandibular pain and shoulder injuries.7 36 Shortening of the levator scapulae as caused by prolonged FHP may change the position of the scapula, decreasing its ability to rotate upwardly and changing the mechanics of the shoulder complex. The strong relationship that exists between the shoulder complex and the spine17 may account for the decrease in the cervical angle as well as the decrease in subjects' perceived shoulder pain.
Studies support our results of decreased RSP through active stretching exercises. A study by Kluemper et al37 found decreased RSP following a 6-week intervention including stretching of the anterior shoulder muscles and strengthening of the posterior shoulder muscles. In addition, Roddey et al38 successfully improved RSP following a 2-week pectoralis-stretching programme.
We hypothesised that the isometric strength of the scapular stabilising muscles would improve following the intervention. The results indicated no differences in strength measures of the intervention group compared with the controls after 8 weeks. In fact, the mean and peak output forces increased for both groups. This trend could be due to several reasons, including subject compliance, length of the intervention, type of exercises performed or intensity of subjects' swim training. Compliance was controlled through exercise cards, random checks and reminder e-mails. However, low compliance was still a risk because of the number of intervention subjects and their already lengthy time commitment to training.
The intervention exercises were selected based on electromyography research. Prone horizontal abduction exercises at the shoulder have been shown to illicit high activity in the scapular retractors such as the middle trapezius and lower trapezius.28 39 Prone push-ups with a plus have been shown to illicit high activity in the serratus anterior.40 41 Wang and colleagues18 reported increases in periscapular muscle strength following an 8-week intervention. However, the study incorporated resistance tubing to the strengthening programme, suggesting that the results of our study may be due to an intervention that was not challenging enough to a highly competitive and highly trained athlete.
Measures of strength were tested as peak and average isometric force over a 5-s period. Swimming by nature is a high endurance sport with training that involves 16 000 shoulder revolutions per week. Endurance testing of the scapular muscles may thus be a more effective variable to measure in reference to an overhead athlete of this type. Beach and colleagues42 reported no significant correlation of shoulder pain to shoulder strength measured as peak torque. However, their results indicated a negative correlation between shoulder pain and muscular endurance ratios, suggesting that with decreased muscular endurance, swimmers are more likely to have increased shoulder pain.
Shoulder pain and function
At the time of pretest, 78% of subjects in our study reported some level of shoulder pain consistent with previous reports in the literature.1 43 44 It is important to note, however, that the swimmers denied limiting their training. We hypothesised that subjects in the intervention group would report higher ASES scores, indicating a decrease in shoulder pain and an increase in function following the 8-week intervention. Our results indicated no difference in ASES scores, which may be due to the relatively large minimal detectable change (9.7 points) and minimally clinically important difference (MCID) (6.4 points) as evidenced by only eight out of 28 subjects experiencing a clinically important difference in ASES scores.45 In contrast, a much smaller MCID has been reported for shoulder pain (1.10–2.17 points).46 47 When applying an MCID of 2 points to our data shows, 79% of subjects in the intervention group reported either decreased (greater than the MCID) or reported no pain at post-test. In addition, 50% of subjects in the control reported increased pain scores greater than the MCID. These results suggest that there may be a ceiling effect in the functional portion of the ASES for this high-level population, and that following intervention subjects had decreased pain compared with the control subjects whose complaints remained the same or became worse.
It is important to note the times of the swimming season at which data were collected. Subjects of our study were tested first in September, a point in the season when they swam 8000–14 000 yards per day. At the time of re-test in December, the peak of most competitive swimming seasons, subjects were at times swimming 20 000 yards in one day. This increase in training may account for the increases in muscular strength seen in both control and intervention groups. It may also have masked any effects of the intervention to strengthen the scapular muscles in the intervention group. However, it emphasises the clinical significance of the pain scores reported by the intervention group at post-test; that despite peak intensity of training, swimmers reported decreased pain following the intervention.
Conclusion
Few research studies have examined the effectiveness of intervention exercise often used by clinicians to correct posture through a training protocol involving flexibility and strength exercises.18 37 38 The exercise intervention used in this study improved posture over the course of the season in elite swimmers, as measured by the cervical angle and FST. The results of this study suggest that preventive interventions aimed at improving postural deviations appear to improve posture and decrease the impact of shoulder pain. Shoulder function, as measured by ASES scores, although not statistically different following the intervention, demonstrated a trend towards a decreased level of perceived shoulder pain and dysfunction. This trend suggests that there may be a relationship between the correction of FHP, RSP and shoulder pain.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the University of North Carolina Biomedical Institutional Review Board.
-
Patient consent Obtained.
-
Provenance and peer review Commissioned; externally peer reviewed.